treatment of persistent corneal epithelial defect with extended wear of a fluid-ventilated...
TRANSCRIPT
Treatment of Persistent Corneal EpithelialDefect With Extended Wear of a Fluid-
ventilated Gas-permeable Scleral Contact Lens
PERRY ROSENTHAL, MD, JANIS M. COTTER, OD, AND JULES BAUM, MD
● PURPOSE: To report treatment of persistent cornealepithelial defects unresponsive to other therapies byextended wear of a fluid-ventilated gas-permeable scleralcontact lens.● METHODS: In this retrospective study, 14 eyes of 13consecutive patients referred for the treatment of persis-tent corneal epithelial defects that failed to heal withconventional therapies or developed epithelial defectsafter penetrating keratoplasty for persistent corneal epi-thelial defects were fitted with an extended-wear gas-permeable scleral lens. These included seven eyes of sixpatients with Stevens-Johnson syndrome and seven eyesof seven patients who did not have Stevens-Johnsonsyndrome. Twelve eyes had undergone recent penetrat-ing keratoplasty. All 14 eyes were fitted with a gas-permeable scleral contact lens designed to avoid theintrusion of air bubbles under its optic. An antibiotic andcorticosteroid were added to the lens fluid reservoir orinstilled before each lens insertion in 12 of 14 eyes. Thelenses were worn continuously except for brief periods ofremoval for purposes of cleaning, replacement of the lensfluid reservoir, and examination and photography of thecornea.● RESULTS: Five of the seven persistent corneal epithe-lial defects associated with Stevens-Johnson syndromehealed. The persistent corneal epithelial defects of four ofthese eyes re-epithelialized within 7 days, and a fifthhealed in 27 days of gas-permeable scleral lens extendedwear. A sixth persistent corneal epithelial defect thatfailed to heal initially re-epithelialized after a subsequentpenetrating keratoplasty and gas-permeable scleral lensextended wear. The seventh eye healed after 3 days of
gas-permeable scleral lens extended wear, but the persis-tent corneal epithelial defect subsequently recurred.Three of seven non–Stevens-Johnson syndrome persis-tent corneal epithelial defects re-epithelialized within 36hours, 6 days, and 36 days, respectively. Of the six (six of14) persistent corneal epithelial defects that failed to healwith a gas-permeable scleral lens extended wear, one sub-sequently healed after multiple amniotic membrane grafts.Microbial keratitis occurred in four eyes (four of 14) andgraft failure in one eye, all of which required repeatpenetrating keratoplasty.● CONCLUSION: Extended wear of an appropriately de-signed gas-permeable scleral contact lens was effective inpromoting the healing of persistent corneal epithelialdefects in some eyes that failed to heal after othertherapeutic measures. Re-epithelialization appears to beaided by a combination of oxygenation, moisture, andprotection of the fragile epithelium afforded by the sclerallens. However, microbial keratitis represents a significantrisk. (Am J Ophthalmol 2000;130:33–41. © 2000 byElsevier Science Inc. All rights reserved.)
A FTER A TYPICAL CORNEAL ABRASION, EPITHELIUM
characteristically resurfaces the defect quickly anduneventfully. However, the coexistence of risk
factors, such as corneal hypesthesia, limbal stem celldeficiency, dry eye conditions, exposure, and diabetes, mayretard the centripetal migration of epithelia adjacent tothe denuded area, thereby resulting in a persistent cornealepithelial defect.1,2 Lacking an intact epithelium, theunderlying cornea is susceptible to inflammation andinfection. Therapeutic modalities available to facilitatere-epithelialization include eyelid patching, soft contactlens extended wear, copious lubrication, and tarsorrhaphy.However, these efforts sometimes fail. In a recent report,only 51% of corneas with severe ocular surface disordersre-epithelialized after epithelial stem cell transplantation.3
Other studies document complete resurfacing of otherwiseintractable persistent corneal epithelial defects after surgi-
Accepted for publication Jan 11, 2000.From The Boston Foundation for Sight (Drs Rosenthal and Cotter);
Boston Eye Associates (Drs Rosenthal, Cotter, and Baum); and theDepartment of Ophthalmology, Harvard Medical School, MassachusettsEye And Ear Infirmary (Dr Rosenthal), Boston, Massachusetts.
This study was sponsored by the Boston Foundation for Sight (Dr.Cotter).
Reprint requests to Perry Rosenthal, MD, 1244 Boylston St, Suite 202,Chestnut Hill, MA 02467; fax: (617) 735-8814; e-mail: [email protected]
© 2000 BY ELSEVIER SCIENCE INC. ALL RIGHTS RESERVED.0002-9394/00/$20.00 33PII S0002-9394(00)00379-2

cal application of an amniotic membrane,4,5 treatmentwith gas-permeable scleral lenses,6 and the use of nervegrowth factor.7
PATIENTS AND METHODS
THIS RETROSPECTIVE CASE STUDY INCLUDED 14 EYES OF 13
consecutive patients with persistent corneal epithelialdefects who were referred because of failure of othertherapeutic measures or who developed a large epithelialdefect after penetrating keratoplasty for persistent cornealepithelial defects that was refractory to other treatment.
The design, manufacture, and fitting protocol of theBoston Scleral Lens are described elsewhere.8
Informed consent was obtained from all patients. Thecontinuous wear of the Boston Scleral Lens was inter-rupted by brief periods of removal once or twice duringeach 24-hour period for cleaning and replacement of thefluid reservoir, except for patient 8, who wore the lenswithout interruption for 1 week. After its removal, the lenswas cleaned with the Boston Cleaner (Polymer Technol-ogy Corporation, Rochester, NY), rinsed with nonpre-served sterile saline, and generously coated with Simplicityconditioning solution (Polymer Technology Corporation).The posterior surface of the lens was again rinsed withsterile saline. In some patients one or two drops of theprescribed medications (Tables 1 and 2) were placed in thelens cup, which was topped off with sterile, nonpreservedsaline before lens reinsertion. In others, the medication(s),
which consisted of an antibiotic and/or corticosteroid,were instilled immediately before lens insertion (Tables 1and 2). The size of the fluorescein-stained persistentcorneal epithelial defect was monitored at each visit byvideo and still photography performed during the briefperiods of lens removal.
In designing the lenses, priority was given to preventingthe intrusion of large air bubbles under the optic of thelenses. Small, mobile bubbles were acceptable.
RESULTS
DETAILS OF CLINICAL FINDINGS, TREATMENTS, AND OUT-
comes before scleral lens wear are listed in Table 3. Previousunsuccessful treatments of the persistent corneal epithelialdefects included tarsorrhaphy (11 eyes), soft contact lensextended wear (11 eyes), patching (12 eyes), buccal mucousmembrane grafts of the tarsal conjunctiva in five of the sevenStevens-Johnson syndrome eyes, and copious lubrication inall eyes. The persistent corneal epithelial defects of 12 of the14 eyes in this study followed penetrating keratoplasty ofwhich seven were in eyes of six patients with Stevens-Johnson syndrome and eight were performed for nonhealingpersistent corneal epithelial defects.
The persistent corneal epithelial defects of five of theseven eyes with Stevens-Johnson syndrome, includingone eye of one patient with toxic epidermal necrolysis,re-epithelialized with gas-permeable scleral lens ex-tended wear (Table 4). Four of these five eyes were
TABLE 1. Ocular Medications Used in Scleral Lens Reservoir: Prophylactic Antibiotics
Ciprofloxacin
0.3%
Ofloxacin
0.3%
Trimethoprim
Polymyxin B
Sulfate
Bacitracin Zinc
Polymyxin B
Ophthalmic Ointment
Polymyxin B
10,000 units/ml
Gramicidin
0.025 mg/ml
Patient 1 2 gtt.*
2 RE 1 gt.
2 LE 1 gt.
3 fourth PK No antibiotic used
3 fifth PK 1 gt.
4 No antibiotic used
5 1 gt.
6 1 gt.
7 Placed on peripheral rim
of lens
8 2 gtt.
9 2 gtt.
10 2 gtt.
11 2 gtt.
12 1 gt.
13 1 gt.
PK 5 penetrating keratoplasty.
* Drops.
AMERICAN JOURNAL OF OPHTHALMOLOGY34 JULY 2000

transitioned to daily wear without recurrence of acorneal epithelial defect. The fifth patient (patient 5),whose corneal epithelial defects had persisted for 60days and healed in 3 days of extended-wear gas-perme-able scleral lens extended wear, discontinued scleral lenswear because of handling difficulties, and the cornealepithelium remained intact 1 year later. The epithelialdefect of patient 1 did not resolve with gas-permeablescleral lens extended wear, but it did heal after asubsequent penetrating keratoplasty that was immedi-ately followed by gas-permeable scleral lens extendedwear.
Of the three non–Stevens-Johnson syndrome cornealepithelial defects that persisted and healed uneventfullywith gas-permeable scleral lens extended wear, two were inneurotrophic corneas secondary to Herpes simplex keratitis(patients 7 and 11), and the defect in patient 8 wasassociated with longstanding ocular cicatricial pemphi-goid.
The persistent corneal epithelial defects of six eyes failedto resurface during the course of this study (Table 4).Epithelial defects in patients 1 and 9 had healed afterpenetrating keratoplasties, but these corneas failed tore-epithelialize after a subsequent penetrating keratoplastywas performed for other reasons.
Four eyes in this study developed microbial keratitis; theeye of patient 10 had three separate episodes. All requiredpenetrating keratoplasty, which resolved the infection. Apersistent corneal epithelial defect was present in all eyesat the time of onset, except for patient 3, in whom thestatus of the corneal epithelium was unknown. All patients
had been wearing the scleral lens for extended periods,except for patient 10, whose third corneal bacterial ulceroccurred during daily wear. The organisms cultured fromthe corneal ulcers are listed in Table 5.
CASE REPORTS
● PATIENT 2: This woman developed Stevens-Johnsonsyndrome in 1992 at age 18, 2 months after treatmentwas initiated for acute leukemia. In the same year, 4months after a depleted bone marrow graft was per-formed, she developed bilateral persistent corneal epi-thelial defects. The cornea in her right eye perforatedafter two glue and bandage lens procedures. The subse-quent penetrating keratoplasty perforated, as did thelamellar keratoplasty that followed. A second lamellarkeratoplasty developed a persistent corneal epithelialdefect that persisted despite a 75% tarsorrhaphy whichwas extended to over 90%. Sixteen months later, thetarsorrhaphy was reversed, and gas-permeable sclerallens extended wear was initiated on an intact corneaand resumed immediately after a stem cell allograft wasperformed 1 month later. Four months later this eyeunderwent a penetrating keratoplasty, cataract extrac-tion, and posterior chamber implant, after which a largeepithelial defect developed that promptly healed onresuming gas-permeable scleral lens extended wear. Thiseye was transitioned to daily wear and has 20/301vision through the lens 2 years later
The cornea of the left eye perforated, as did the
TABLE 2. Ocular Medications Used in Scleral Lens Reservoir: Topical Corticosteroid Drops
Prednisolone Acetate 1%
Prednisolone Sodium
Phosphate 1%
Rimexolone Ophthalmic
Suspension 1%
Patient 1 2 gtt.
2 RE Not used in lens reservoir*
2 LE Not used in lens reservoir*
3 fourth PK No steroid used
3 fifth PK 1 gt.
4 2 gtt.
5 Not used in lens reservoir*
6 1 gt.
7 No steroid used
8 Not used in lens reservoir*
9 2 gtt.
10 2 gtt.
11 Not used in lens reservoir*
12 2 gtt.
13 1 gt.
PK 5 penetrating keratoplasty.
* Corticosteroid drop instilled just before scleral lens insertion.
TREATMENT OF PERSISTENT EPITHELIAL DEFECT WITH SCLERAL CONTACT LENSVOL. 130, NO. 1 35

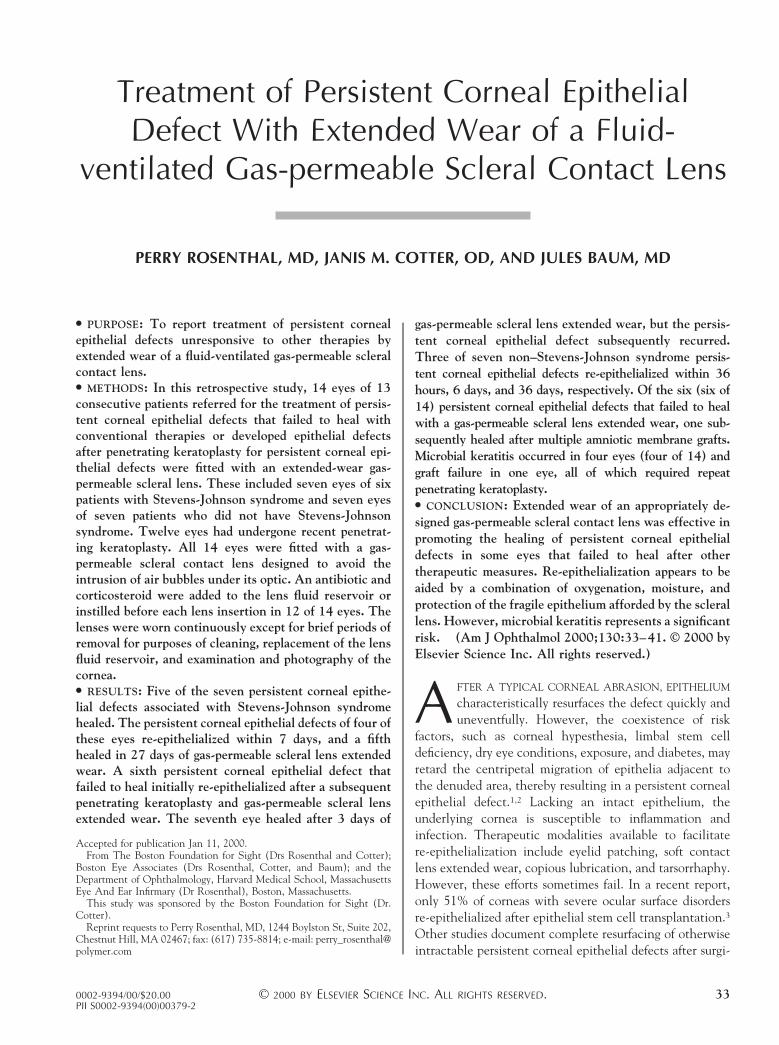
subsequent Gunderson flap. The penetrating keratoplastythat followed developed a persistent corneal epithelialdefect 8 months postoperatively which persisted for 5months, despite a 75% tarsorrhaphy. Extended-wear usegas-permeable scleral lens was then initiated, and thepersistent corneal epithelial defect healed in 6 days (Figure1). This eye was subsequently transitioned to daily wearand has been free of an epithelial defect during thesubsequent 4 years.
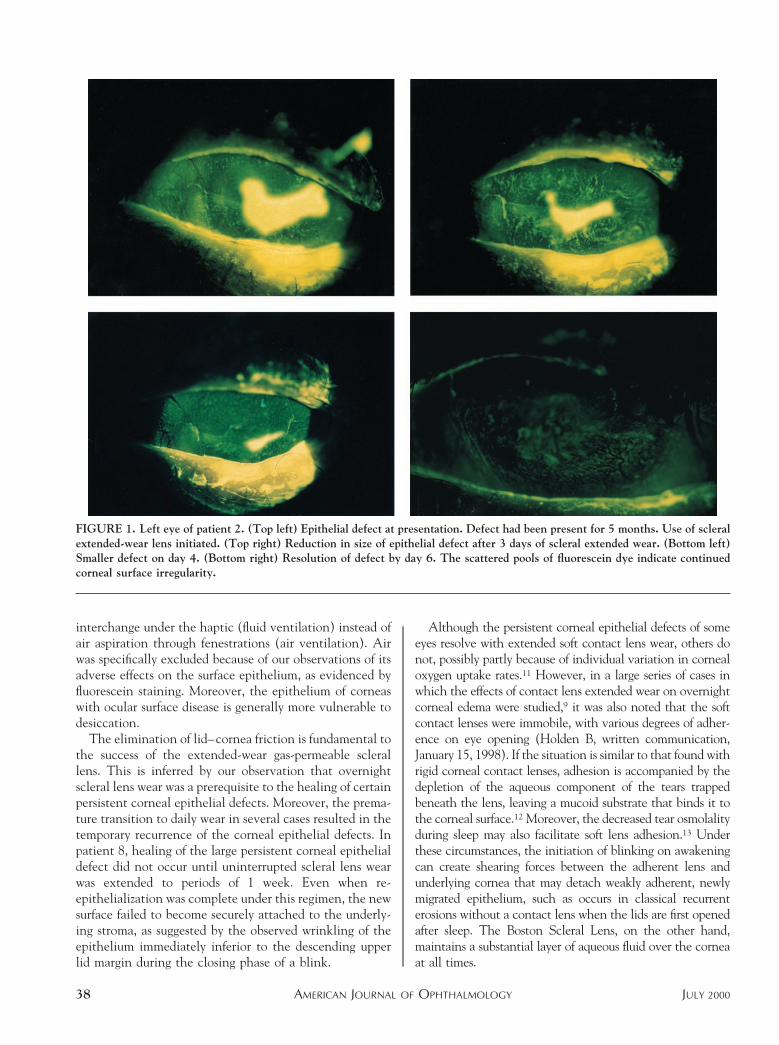
● PATIENT 4: This woman developed Stevens-Johnsonsyndrome in 1992 at age 15. Her right cornea perforatedshortly thereafter and was treated with glue and bandagelens. Four years later this eye underwent a penetratingkeratoplasty, cataract extraction, posterior chamber lensimplantation, and anterior segment reconstruction. Apersistent corneal epithelial defect developed postopera-tively and persisted for 21 days until gas-permeable sclerallens extended wear was initiated and the defect healed in
6 days (Figure 2). This eye, which was transitioned to dailywear, has been free of an epithelial defect during theinterim 3 years, and the patient has 20/30 visual acuitythrough the lens.
● PATIENT 11: This 56-year-old man developed a persis-tent corneal epithelial defect in his left eye secondary tochronic herpes simplex keratitis. His first penetratingkeratoplasty in 1996 was followed by a persistent cornealepithelial defect that persisted until his second penetratingkeratoplasty, cataract extraction, and posterior chamberimplant 1 year later. A persistent corneal epithelial defectdeveloped immediately after surgery and persisted for 5months. The epithelial defect healed in 36 hours after theinitiation of gas-permeable scleral lens extended wear, atwhich time the schedule was changed to daily wear. Thepersistent corneal epithelial defect promptly reappearedand resolved when extended wear was resumed for anadditional 24 hours. This eye has been free of an epithelial
TABLE 3. Patient Profiles Before Scleral Lens Fitting for Persistent Corneal Epithelial Defect
Patient Age Gender Eye Diagnosis
Penetrating
Keratoplasty Duration of PCED
Prior Treatment
for PCED*
1 16 M LE Stevens-Johnson syndrome Yes 12 months 1,2,3,4,5,6,8(2)
2 18 F RE Stevens-Johnson syndrome Yes 2 days† 1,2,4,5,6,8(1)
2 LE Yes 5 months 2,3,4,5,6,8(1)
3 26 M LE Toxic epidermal necrolysis Yes 21 days 3,4,5,6,8(3)
4 19 F RE Stevens-Johnson syndrome Yes 21 days 3,4,5,6
5 M LE Stevens-Johnson syndrome Yes 60 days 1,2,3,4,5,6,7
6 74 F RE Neurotrophic keratitis
Keratoconjunctivitis sicca
Rheumatoid arthritis
Diabetes
Yes 0‡ 2,4,6,7
7 69 F RE Neurotrophic keratitis
Herpes simplex
No 5 months 2,5,6
8 68 F RE Ocular cicatricial pemphigoid No 1 month 2,4,5,6
9 66 M LE Neurotrophic keratitis
Herpes zoster
Keratoconjunctivitis sicca
Yes 0‡ 2,6
10 57 F RE Sjogren syndrome
Mooren ulcer
Yes 0‡ 2,4,5,6,8(3)
11 56 M LE Neurotrophic keratitis
Herpes simplex
HIV 1
Yes 5 months 4,5,6,8(2)
12 49 F LE Neurotrophic keratitis
Herpetic corneal disease
Atopic keratoconjunctivitis
Yes 4 months 2,4,6,8(2)
13 20 M LE Stevens-Johnson syndrome Yes 3 days† 1,2,4,5,6,7,8(7)
HIV 5 human immunodeficiency virus; PCED 5 persistent corneal epithelial defect.
* 1) Limbal allograft, 2) tarsorrhaphy, 3) mucous membrane grafting, 4) pressure patching, 5) therapeutic soft lens, 6) copious lubrication,
7) amniotic membrane grafting, 8) penetrating keratoplasty (number of penetrating keratoplasties before scleral lens fitting).† History of previous persistent epithelial defects.‡ Scleral lens inserted prophylactically at close of penetrating keratoplasty.
AMERICAN JOURNAL OF OPHTHALMOLOGY36 JULY 2000

defect during the subsequent 18 months, except for onetransient episode that followed the patient’s failure to tapethe lids closed at night.
DISCUSSION
ALTHOUGH THIS UNCONTROLLED RETROSPECTIVE CASE
series study lacks a previous and subsequent treatmentprotocol, the history and outcomes before referral suggestthat continuous wear of a fluid-ventilated gas-permeablescleral lens enhances the healing of persistent corneal
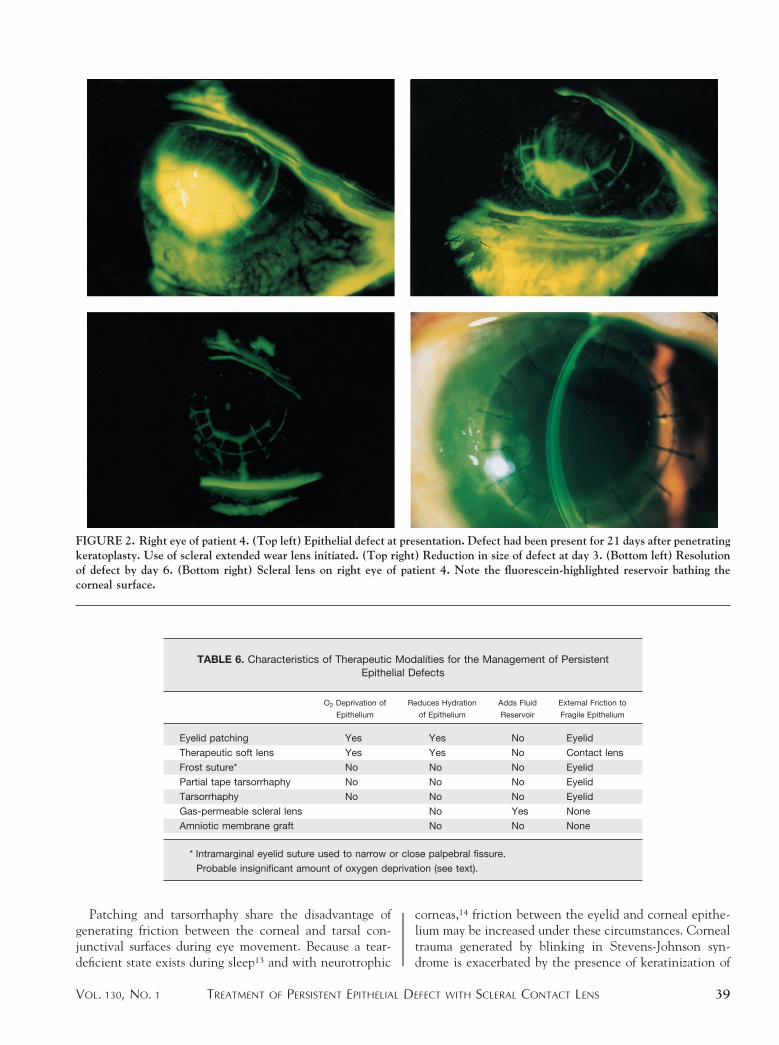
epithelial defects that are refractory to other treatmentmodalities. We believe this to be the result of the uniqueenvironment these lenses create for the corneal epithe-lium, an environment consisting of three salient features:an adequate supply of oxygen, a constant aqueous inter-face, and the absence of friction or shearing forces gener-ated by the movement of the lids over the cornea as occursduring blinking, or the movement of the cornea under thelids, as occurs in patching and tarsorrhaphy (Table 6).
A continuing supply of oxygen is necessary to sustainthe health and repair of the corneal epithelium. It has beensuggested that partial tarsorrhaphy is more effective thanpatching in treating epithelial defects, because it causesless corneal oxygen deprivation.1 The oxygen content ofthe reservoir fluid of the Boston Scleral Lens is maintainedprincipally by its diffusion through the matrix of the lens,although some is also supplied through tear-fluid exchange.During sleep, the driving partial pressure of oxygen at thefront surface of a contact lens is greatly reduced, and theamount that reaches the corneal surface is further attenu-ated as it passes through the matrix of the lens and the fluidcompartment.9,10 Nevertheless, our results suggest that thecorneal oxygen supply under the Boston Scleral Lens issufficient to maintain the viability of regenerating epithe-lium during sleep.
One of the principal design features of the BostonScleral Lens is its ability to avoid suction through fluid-tear
TABLE 4. Clinical Outcomes After Onset of Extended-wear Scleral Lenses for PersistentCorneal Epithelial Defects
Patient
Diagnosis
SJS vs
Non-SJS Defect Healed Time to Heal Complications
1 SJS No Microbial keratitis
2 RE SJS Yes 4 days
2 LE Yes 6 days
3 SJS Yes 27 days Microbial keratitis (4th PK)
Suture abscess (5th PK)
4 SJS Yes 6 days
5 SJS Yes 3 days
6 Non-SJS No Graft failure, repeat penetrating
keratoplasty
7 Non-SJS Yes 6 days
8 Non-SJS Yes 36 days
9 Non-SJS No Repeat penetrating keratoplasty
with limbal autograft, Amniotic
membrane grafting
10 Non-SJS No Microbial keratitis 3 3
11 Non-SJS Yes 36 hours
12 Non-SJS No Microbial keratitis
13 SJS No Graft rejection
Defect recurred and failed to heal
Non-SJS 5 non–Stevens-Johnson syndrome; PK 5 penetrating keratoplasty; SJS 5 Stevens-
Johnson syndrome.
TABLE 5. Microbial Keratitis in Patients With Scleral LensExtended Wear
Patient Organism Cultured
1 Mycobacterium abscessus
3 Streptococcus pneumoniae
10 (fourth penetrating keratoplasty) Alpha-hemolytic streptococcus
10 (fifth penetrating keratoplasty) Staphylococcus epidermidis
10 (sixth penetrating keratoplasty)* Staphylococcus epidermidis
12 Staphylococcus epidermidis
* Microbial keratitis developed with daily wear of a scleral lens
after penetrating keratoplasty and amniotic membrane grafting.
TREATMENT OF PERSISTENT EPITHELIAL DEFECT WITH SCLERAL CONTACT LENSVOL. 130, NO. 1 37
interchange under the haptic (fluid ventilation) instead ofair aspiration through fenestrations (air ventilation). Airwas specifically excluded because of our observations of itsadverse effects on the surface epithelium, as evidenced byfluorescein staining. Moreover, the epithelium of corneaswith ocular surface disease is generally more vulnerable todesiccation.
The elimination of lid–cornea friction is fundamental tothe success of the extended-wear gas-permeable sclerallens. This is inferred by our observation that overnightscleral lens wear was a prerequisite to the healing of certainpersistent corneal epithelial defects. Moreover, the prema-ture transition to daily wear in several cases resulted in thetemporary recurrence of the corneal epithelial defects. Inpatient 8, healing of the large persistent corneal epithelialdefect did not occur until uninterrupted scleral lens wearwas extended to periods of 1 week. Even when re-epithelialization was complete under this regimen, the newsurface failed to become securely attached to the underly-ing stroma, as suggested by the observed wrinkling of theepithelium immediately inferior to the descending upperlid margin during the closing phase of a blink.
Although the persistent corneal epithelial defects of someeyes resolve with extended soft contact lens wear, others donot, possibly partly because of individual variation in cornealoxygen uptake rates.11 However, in a large series of cases inwhich the effects of contact lens extended wear on overnightcorneal edema were studied,9 it was also noted that the softcontact lenses were immobile, with various degrees of adher-ence on eye opening (Holden B, written communication,January 15, 1998). If the situation is similar to that found withrigid corneal contact lenses, adhesion is accompanied by thedepletion of the aqueous component of the tears trappedbeneath the lens, leaving a mucoid substrate that binds it tothe corneal surface.12 Moreover, the decreased tear osmolalityduring sleep may also facilitate soft lens adhesion.13 Underthese circumstances, the initiation of blinking on awakeningcan create shearing forces between the adherent lens andunderlying cornea that may detach weakly adherent, newlymigrated epithelium, such as occurs in classical recurrenterosions without a contact lens when the lids are first openedafter sleep. The Boston Scleral Lens, on the other hand,maintains a substantial layer of aqueous fluid over the corneaat all times.
FIGURE 1. Left eye of patient 2. (Top left) Epithelial defect at presentation. Defect had been present for 5 months. Use of scleralextended-wear lens initiated. (Top right) Reduction in size of epithelial defect after 3 days of scleral extended wear. (Bottom left)Smaller defect on day 4. (Bottom right) Resolution of defect by day 6. The scattered pools of fluorescein dye indicate continuedcorneal surface irregularity.
AMERICAN JOURNAL OF OPHTHALMOLOGY38 JULY 2000
Patching and tarsorrhaphy share the disadvantage ofgenerating friction between the corneal and tarsal con-junctival surfaces during eye movement. Because a tear-deficient state exists during sleep13 and with neurotrophic
corneas,14 friction between the eyelid and corneal epithe-lium may be increased under these circumstances. Cornealtrauma generated by blinking in Stevens-Johnson syn-drome is exacerbated by the presence of keratinization of
FIGURE 2. Right eye of patient 4. (Top left) Epithelial defect at presentation. Defect had been present for 21 days after penetratingkeratoplasty. Use of scleral extended wear lens initiated. (Top right) Reduction in size of defect at day 3. (Bottom left) Resolutionof defect by day 6. (Bottom right) Scleral lens on right eye of patient 4. Note the fluorescein-highlighted reservoir bathing thecorneal surface.
TABLE 6. Characteristics of Therapeutic Modalities for the Management of PersistentEpithelial Defects
O2 Deprivation of
Epithelium
Reduces Hydration
of Epithelium
Adds Fluid
Reservoir
External Friction to
Fragile Epithelium
Eyelid patching Yes Yes No Eyelid
Therapeutic soft lens Yes Yes No Contact lens
Frost suture* No No No Eyelid
Partial tape tarsorrhaphy No No No Eyelid
Tarsorrhaphy No No No Eyelid
Gas-permeable scleral lens † No Yes None
Amniotic membrane graft † No No None
* Intramarginal eyelid suture used to narrow or close palpebral fissure.† Probable insignificant amount of oxygen deprivation (see text).
TREATMENT OF PERSISTENT EPITHELIAL DEFECT WITH SCLERAL CONTACT LENSVOL. 130, NO. 1 39

the lid margins, trichiasis, and dystichiasis. Pressure patch-ing can exacerbate this abrasive effect. Moreover, tarsor-rhaphy does not eliminate lid–cornea friction, and partialtarsorrhaphy does not completely avoid the effects ofcorneal drying.
In patient 13 the size of the persistent corneal epithelialdefect had not changed significantly when observed afterthe first overnight wear, but it rapidly decreased over thecourse of the following day and resolved by the followingmorning. It was apparent in this case that the major periodof healing occurred during waking hours when the lidswere open.
The Boston Scleral Lens also served as a vehicle fordelivering prophylactic and therapeutic topical ocularmedications to the cornea. The low rate of reservoir fluidturnover is reflected by the observed slow seepage offluorescein-stained tears into the postlens fluid reservoirand the fact that the dye can be observed under the lens forup to 24 hours after its introduction. This slow rate ofturnover would also apply to drugs placed in the lensreservoir.
Four eyes developed microbial keratitis with the extend-ed-wear gas-permeable scleral lens and required penetrat-ing keratoplasty. A Mycobacterium abscessus keratitis andendophthalmitis developed in patient 1, 4 months after anextruding Ahmed prosthesis was removed and after 45months of gas-permeable scleral lens extended wear. Thiseye was eventually lost because of a nonreparable retinaldetachment. Patient 3 developed a Streptococcus pneu-moniae keratitis while continuing the extended-wear gas-permeable scleral lens 2 months after the resolution of thepersistent corneal epithelial defect. This was successfullytreated with a penetrating keratoplasty, and the persistentcorneal epithelial defect has not recurred on a scleral lensdaily wear schedule during a follow-up period of 24months. The only eye of patient 10 developed an astreptococcus keratitis 2 months after the extended-weargas-permeable scleral lens was initiated after the fourthpenetrating keratoplasty. Two months after a fifth pene-trating keratoplasty and an extended-wear gas-permeablescleral lens for a persistent corneal epithelial defect, theeye again developed a bacterial keratitis from whichStreptococcus epidermidis was recovered. A subsequent pen-etrating keratoplasty and amniotic membrane graft wereperformed. The amniotic membrane was removed at 1 week,and scleral lens daily wear was started. A large epithelialdefect developed. One month later, a third bacterial keratitisoccurred; S. epidermidis was again cultured.
These cases illustrate the high risk of bacterial keratitisthat exists when contact lenses are worn for extendedperiods,15 especially in the presence of an epithelial defect.The fact that the fluid compartment of the lenses on threeof the four eyes that developed bacterial keratitis con-tained both an antibiotic and a steroid may be significant.Based on this experience, our current strategy is to convertpatients to daily wear as soon as possible after the resolu-
tion of the persistent corneal epithelial defect. The deci-sion when to convert to daily wear is determined bybalancing the risk of developing a bacterial keratitisagainst the benefit of resolving the otherwise intractablepersistent corneal epithelial defect for the individual pa-tient. The risk of keratitis resulting from opportunisticorganisms is not eliminated by the use of prophylacticantibiotics. One of the four eyes developed three episodesof infectious keratitis during scleral lens wear, suggestingthat the occurrence of a bacterial keratitis may be apredictive marker for a future infection. A second eyedeveloped a suture abscess while on scleral lens daily wearafter a persistent corneal epithelial defect, which devel-oped after a therapeutic penetrating keratoplasty for mi-crobial keratitis had resolved.
These results suggest that conversion from extended todaily wear should commence as soon as possible afterresolution of the persistent corneal epithelial defect andafter the epithelium has remained intact for a minimum of24 hours. The risk of infectious keratitis associated withprolonging gas-permeable scleral lens extended wear mustbe balanced against the risk of the recurrence of thepersistent corneal epithelial defect if the transition to dailywear is premature. However, the treatment of both intrac-table persistent corneal epithelial defects and infectiouskeratitis complicating the use of the extended-wear gas-permeable scleral lens is the same, namely, penetratingkeratoplasty. In contrast, in our population with nonper-sistent corneal epithelial defects using scleral lenses, whichis not included in this study, bacterial keratitis occurred infour of 300 eyes of 208 patients, and three of the fourresolved on medical treatment.
The more difficult question is when to discontinue theextended-wear gas-permeable scleral lens in the face of anunresolved persistent corneal epithelial defect. Althoughsix persistent corneal epithelial defects cleared within 1week of this treatment, two eyes required periods of 27 and36 days. If the extended-wear gas-permeable scleral lenshad been aborted in the two cases that required longerextended wear, the likely outcome would have been arepeat penetrating keratoplasty complicated by a recur-rence of the persistent corneal epithelial defects and theneed for the resumption of the extended-wear gas-perme-able scleral lens use.
Our current strategy is to examine these patients dailywithout exception and transition them to daily wear 24hours after the persistent corneal epithelial defect hasresolved. The epithelial defect must show improvementwithin the first 24 to 48 hours to continue the extended-wear gas-permeable scleral lens regimen. Once the persis-tent corneal epithelial defect has resolved, the patients areinstructed to remove the lens just before retiring andimmediately instill a lubricating ointment and tape the lidsclosed to minimize eyelid friction during the night. Thelens is reinserted as soon as possible after awakening.
It might be argued that, in some cases, the role of the
AMERICAN JOURNAL OF OPHTHALMOLOGY40 JULY 2000

scleral lens in the healing of the persistent corneal epithe-lial defects was unclear. This is especially true of thosepatients in whom the Boston Scleral Lens was inserted atthe close of surgery or shortly thereafter. However, inpatients 2, 4, 5, 7, 8 and 11, the time frames, histories, anddisease processes strongly support the pivotal role of theextended-wear gas-permeable scleral lens in the resolutionof their persistent corneal epithelial defects. Moreover, theexperience of patients 1, 6, and 9 suggests that the failureof the extended-wear gas-permeable scleral lens to heal apersistent corneal epithelial defect does not preclude it frombeing successful after a subsequent penetrating keratoplasty.
The composition of the fluid in the lens reservoirwarrants further study to improve its biocompatibility andperhaps further improve the healing environment of thecorneal epithelium. The incorporation of autologous se-rum4 and nerve growth factor7 may optimize their sug-gested benefits, because of the small rate of turnover of thefluid compartment and the significantly greater cornealcontact time. More rapid healing and earlier conversion todaily wear has the potential of reducing the risk ofmicrobial keratitis significantly.
The recently introduced amniotic membrane5 also ap-pears to aid in resurfacing the cornea after a persistentcorneal epithelial defect. Its mechanism of action may besimilar to that of the extended-wear gas-permeable sclerallens in that it is permeable to oxygen, moist, and protectsthe regenerating corneal epithelium from lid friction.
Further long-term studies are required to determinewhether the continuation of daily gas-permeable sclerallens wear subsequent to the healing of a persistent cornealepithelial defect prevents or reduces their recurrence invulnerable eyes.
ACKNOWLEDGMENTS
The authors are grateful to The Boston Foundation ForSight and the Thomas Anthony Pappas Charitable Foun-dation for their financial support of this project, to Bausch& Lomb, which manufactured and donated the specialpolymer blanks and provided the lathe required for thefabrication of the scleral lenses, and to C. Stephen Foster,MD, for his support and guidance in the care of many ofthese patients.
REFERENCES
1. Baum J. Prolonged eyelid closure is a risk to the cornea.Cornea 1997;16:602–611.
2. Foulks GN, Thoft RA, Perry HD, et al. Factors related tocorneal epithelial complications after closed vitrectomy indiabetics. Arch Ophthalmol 1979;97:1076–1078.
3. Tsubota K, Satake Y, Kaido M, et al. Treatment of severeocular surface disorders with corneal epithelial stem-celltransplantation. N Engl J Med 1999;340:1697–1703.
4. Tsubota K, Satake Y, Ohyama M, et al. Surgical reconstruc-tion of the ocular surface in advanced ocular cicatricialpemphigoid and Stevens-Johnson syndrome. Am J Ophthal-mol 1996;122:38–52.
5. Lee S, Tseng SCG. Amniotic membrane transplantation forpersistent epithelial defects with ulceration. Am J Ophthal-mol 1997;123:303–312.
6. Cotter JM, Rosenthal P, Baum J. Gas permeable sclerallenses in the management of non-healing corneal epithelialdefects. Ophthalmol Vis Sci 1997;38:S137.
7. Lambiase A, Rama P, Bonini G, et al. Topical treatmentwith nerve growth factor for corneal neurotrophic ulcers. NEngl J Med 1998;338:1174–1180.
8. Romero-Rangel T, Stavrou P, Cotter J, et al. Gas permeablescleral lens therapy in ocular surface disease. Am J Ophthal-mol 1999;130:25–32.
9. La Hood D, Sweeney DF, Holden BA. Overnight cornealedema with hydrogel, rigid gas-permeable and silicone elas-tomer contact lenses. Int Contact Lens Clin 1988;15:149–154.
10. Pullum KW, Hobley AJ, Davison C. 1001: Does thicknessmake much difference? J Br Contact Lens Assoc 1991;14:17–19.
11. Larke JR, Parrish ST, Wigham CG. Apparent human cornealoxygen uptake rate. Am J Optom Physiol Op 1981;58:803–805.
12. Swarbrick HA, Holden BA. Rigid gas-permeable binding:significance and contributing factors. Optom Physiol Optics1987:64:815.
13. Gilbard JP, Cohen GR, Baum J. Decreased tear osmolarityand absence of the inferior marginal tear strip after sleep.Cornea 1992;11:231–233.
14. Heigle TH, Pflugfelder SC. Aqueous tear production inpatients with neurotrophic keratitis. Cornea 1996;15:135–138.
15. Schein OD, Glynn RJ, Poggio ED, et al. The relative riskof ulcerative keratitis among users of daily wear andextended-wear soft contact lenses. N Engl J Med1989;321:773–778.
The full-text of AJO is now available online at www.ajo.com. AuthorsInteractivet, currently available in limited form, is undergoing an upgrade.
TREATMENT OF PERSISTENT EPITHELIAL DEFECT WITH SCLERAL CONTACT LENSVOL. 130, NO. 1 41