treatment of mercury vapor toxicity by combining deferasirox and deferiprone in rats
TRANSCRIPT

Treatment of mercury vapor toxicity by combiningdeferasirox and deferiprone in rats
Marzieh Iranmanesh • S. Jamil A. Fatemi •
Mohammad Reza Golbafan •
Faezeh Dahooee Balooch
Received: 17 May 2013 / Accepted: 5 July 2013
� Springer Science+Business Media New York 2013
Abstract The hypothesis that combination of
deferasirox and deferiprone chelators might be more
efficient as combined therapy than single therapy in
removing mercury from the body was considered.
Male Wistar rats were exposed to mercury vapor for
2 weeks. After mercury administration some abnormal
clinical signs such as red staining around the eyes,
greenish mottling on the liver, weakness, loss of hair
and weight, were observed in animals. Chelators were
given orally after mercury vapor application for
2 weeks. Mercury toxicity symptoms in rats decreased
after drug administration. After chelation therapy,
these rats were anesthetized with ether vapor and
immobilized by cervical dislocation and then their
heart, liver, kidneys, intestine, spleen and testicles
were sampled for determination of mercury and iron
concentration. The combined chelation therapy results
showed that these chelators are able to remove mercury
from the body and toxicity symptoms decreased.
Keywords Deferasirox � Deferiprone �Mercury toxicity � Chelation therapy � Rats
Introduction
Mercury is a serious environmental pollutant with
toxic effects in all living organisms. Gold mining
emits elemental mercury vapor that is inhaled and
absorbed into the bloodstream (Grandjean et al. 1999).
Human exposure to inorganic mercury is mainly
occupational, which is often related to mining and
industrial activities. In addition, inorganic mercury is
believed to be the toxic species produced in tissues
after inhalation of mercury vapor. Because mercury
vapor generated from metallic mercury (Hg0) is highly
diffusible and lipid soluble, Hg0 vapor is absorbed
quickly and efficiently through the alveolar membrane
from inhaled air in the lung. Most inhaled Hg0 vapor is
oxidized rapidly to bivalent ionic mercury by catalase
in the blood and is distributed via the blood to various
organs (Magos et al. 1978). One way to remove toxic
elements from the body is chelation therapy. Chelation
therapy involves the use of ligating drugs that bind
metal for the treatment of potentially fatal conditions.
These ligands promote the excretion and subsequent
depletion of this transition metal in biological systems.
These chelating agents consist of a range of bidentate,
tridentate and hexadentate ligands in which two, three
or six atoms are able to coordinate, respectively
(Clarke and Martell 1992; Gomez et al. 1988). In this
procedure, chelators are administered orally in order to
remove toxic element. Deferasirox (4-[3,5-bis(2-
hydroxyphenyl)-1,2,4-triazol-1-yl]-benzoic acid, or
ICL670; Fig. 1a is a tri-dentate chelator with high
M. Iranmanesh (&) � S. J. A. Fatemi �M. R. Golbafan � F. Dahooee Balooch
Department of Chemistry, Shahid Bahonar University
of Kerman, 22 Bahman Blvd, Kerman, P.O. Box 76961,
Iran
e-mail: [email protected]
S. J. A. Fatemi
e-mail: [email protected]
123
Biometals
DOI 10.1007/s10534-013-9656-9

selectivity for Fe3?. It selectively binds Fe3? over Fe2
? and shows little affinity for other divalent ions such
as Zn2? or Cu2? (Steinhauser et al. 2004). In vivo, this
selectivity is demonstrated by conserved plasma Zn
and Cu levels in patients taking deferasirox, and while
its efficacy is rather low for inducing negative iron
balance, it is effective and well tolerated (Nisbet-
Brown et al. 2003). In 2005 deferasirox became the
first FDA-approved oral alternative for treatment of
iron overload and was subsequently approved in the
EU in 2006 (Yang et al. 2007). Deferasirox possesses a
pFe3? value of 22.5 and can penetrate membranes
easily and possesses good oral availability. Indeed,
when orally administered to hypertransfused rats,
deferasirox promotes the excretion of chelatable iron
from hepatocellular iron stores four to five times more
effectively than desferrioxamine (Hershko et al.
2001). The other chelator for iron overload is deferi-
prone (1,2-dimethyl-3-hydroxypyrid-4-one) Fig. 1b.
Deferiprone is water soluble and can be given orally
(Hider et al. 1984; Kontoghiorghes et al. 1987;
Gyparaki et al. 1987). It possesses a pFe3? value of
20.5 and its important property is its ability to
penetrate cells, coordinate iron, forming a neutral
complex, which is also capable of permeating mem-
branes (Glickstein et al. 2006). At present, combina-
tion therapy with deferiprone and desferrioxamine,
that is highly selective for iron(III) under biological
conditions (pFe?3 = 26.6), is reported to be the most
effective treatment for many patients (Galanello et al.
2010). The combined therapy procedure is likely to
enhance iron excretion, target specific iron compart-
ments, minimize side-effects (by virtue of the use of
lower doses), facilitate individualization of therapy
and improve compliance (Ma et al. 2012). Desferri-
oxamine with a higher pFe?3 value acting as a sink.
Presumably deferasirox, also possessing a higher
pFe?3 value than deferiprone, behaves in a similar
manner. Recently successful chelation therapy using
both deferasirox and deferiprone has been reported
(Voskaridou et al. 2011). This kind of therapy by
combining two chelators is based on the assumption
that various chelating agents mobilize toxic elements
from different tissue compartments and therefore
better results are expected (Flora et al. 1995). Results
of this kind of combined chelation therapy have been
confirmed by (Amiri et al. 2007; Fatemi et al. 2007,
2009; Tubafard and Fatemi 2008). The aim of the
present research was to test the chelation potency of
deferasirox and deferiprone in combination, given to
animals after mercury loading. Testing was performed
by using a chronic poisoning model on rats with
individual and combined chelators given shortly after
mercury application.
Experimental
Apparatus
A Varian atomic absorption spectrometer (FAAS) was
used for measurement of mercury and iron concentrations
in various organs, respectively. Also a Mettler analytical
balance Model AE 160 was used in this research.
Maintenance of the animals
Male Wistar rats were obtained from Razi Institute
(Karaj, Iran). They were bred in animal house at
Kerman Neuroscience Research Center, Iran. The rats
were maintained under a controlled light:dark
(12:12 h) schedule at 23 ± 1 �C and the humidity of
55 %. The animals were assigned to control and
treated groups and were kept in well cleaned sterilized
cages. The rat food was purchased from Razi Institute.
This study was approved by the ethics committee of
Shahid Bahonar University of Kerman, Iran and
Kerman Neuroscience Research Center, Iran.
Materials
Mercury, deferiprone and other materials were pur-
chased from Merck Chemicals Co. and deferasirox was
purchased from Novartis Co. (Basel, Switzerland).
Fig. 1 Chemical structures of deferasirox (a) and deferiprone (b)
Biometals
123

Experimental design
In our research, the rats were classified as two groups:
control group and treated group. In control group,
inhalation of fresh air was carried out and in treated
group: they were exposed to mercury vapor. Exper-
iments were performed on 7-weeks-old Wistar male
rats.
There were slight differences between the groups in
the initial body weight of the rats (mean 225 g), but at
the end of mercury administration experiment, those
given mercury in their diet had significant weight loss
(Table 1). Comparison of the weights in this experi-
ment showed that dietary treatment affected the food
intake, whereby animals that were given normal diet
consumed more food than those given mercury. Also
because of the slight (but significant) differences in
body weight of rats at the start of the research, the
results can be influenced by the initial classification
and assignment of rats to treated groups. Therefore,
the day 1 groups’ body weights are notable and they
must be considered. Consequently after acclimatiza-
tion of the animals, we assigned them randomly to
control and treated groups.
Treated groups were exposed to mercury vapor for
2 weeks. Chelation therapy was carried out after
mercury application.
In this part of the research, treated groups were
divided into five groups: before chelation therapy,
without chelation therapy, chelation therapy with
deferasirox, chelation therapy with deferiprone and
chelation therapy with deferasirox ? deferiprone
(Table 2). Chelators (deferasirox and deferiprone)
were given orally after mercury application during
2 weeks. Doses of deferasirox and deferiprone were
140 and 300 mg/kg body weight, respectively.
Observed mercury toxicity symptoms in rats were
removed in short term after drug administration. After
chelation therapy, these rats were anesthetized with
ether vapor and immobilized by cervical dislocation
and their heart, liver, kidneys, intestine, spleen and
testicles samples were collected, weighed and dried
for determination of their mercury contents. The
samples were placed in an oven at 60 �C for 3 days.
They were then digested by 1.5 ml of HNO3 per 1 g of
dry weight tissues. After digestion, the solutions were
evaporated with the addition of 1.0 ml of H2O2 under
the hood. Then, the residue was diluted with water to
10 ml volume.
Statistical analysis
Determination of mercury and iron in samples were
carried out by FAAS. The values are expressed as
mean values (at least three separate determina-
tions) ± standard error of the mean. The data were
subjected to statistical analysis by Student’s t test;
P \ 0.05 was considered significant.
Results
Results of mercury raising and iron reduction in
organs of treated groups were statistically different.
A significant difference between control and treated
groups was observed. The general symptoms of
toxicity appeared after 2 weeks of mercury vapor
administration. Abnormal clinical signs in animals
were appeared as follows: darkening of the eyes,
yellowish discoloration of hair, flaccid, hypotonic
muscles, irritability, weakness and loss of hair. Also
the body weights of all animals in treated groups were
significantly decreased. The highest amount of
Table 1 Body weights over 2 weeks for the rats in different
groups (values are mean for the number of observation in
parentheses)
Group Control group Treated group
Initial body
weighta (g)
230 ± 6 (5) (day 1) 220 ± 4 (5) (day 1)
Final body
weighta (g)
245 ± 5 (5) (day 14) 225 ± 5 (5) (day 28)
a Mean of five determination ± standard deviation
Table 2 Classification of animals
All rats
Control
group
Treated group
Before chelation therapy
Without chelation therapy
Chelation therapy with deferasirox (140 mg/kg
body weight)
Chelation therapy with deferiprone (300 mg/kg
body weight)
Chelation therapy with deferasirox (70 mg/kg
body weight) ? deferiprone (150 mg/kg body
weight)
Biometals
123
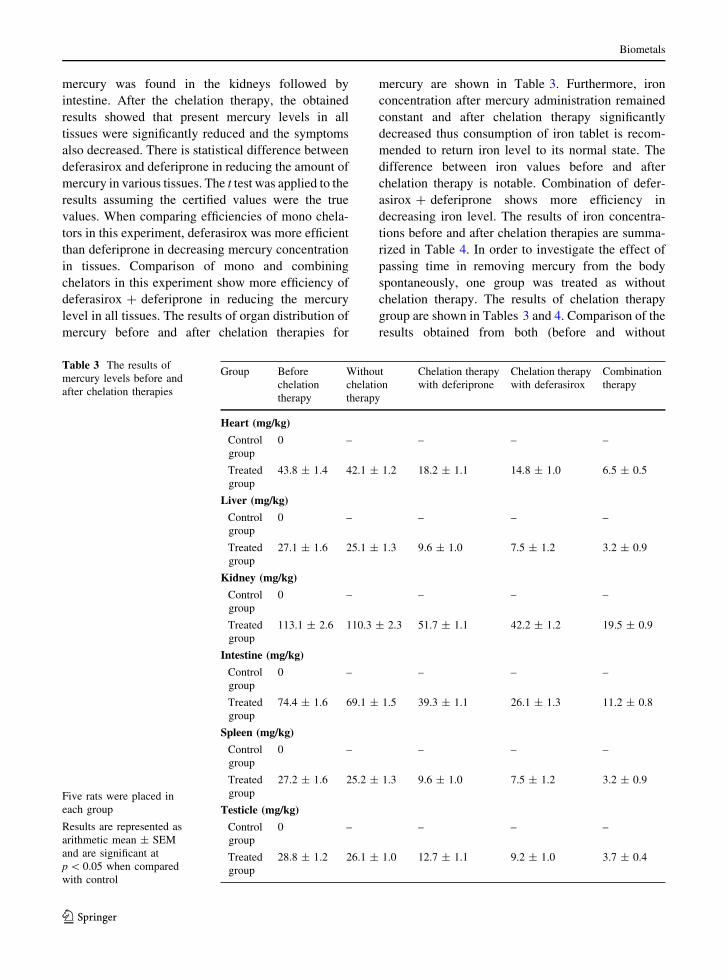
mercury was found in the kidneys followed by
intestine. After the chelation therapy, the obtained
results showed that present mercury levels in all
tissues were significantly reduced and the symptoms
also decreased. There is statistical difference between
deferasirox and deferiprone in reducing the amount of
mercury in various tissues. The t test was applied to the
results assuming the certified values were the true
values. When comparing efficiencies of mono chela-
tors in this experiment, deferasirox was more efficient
than deferiprone in decreasing mercury concentration
in tissues. Comparison of mono and combining
chelators in this experiment show more efficiency of
deferasirox ? deferiprone in reducing the mercury
level in all tissues. The results of organ distribution of
mercury before and after chelation therapies for
mercury are shown in Table 3. Furthermore, iron
concentration after mercury administration remained
constant and after chelation therapy significantly
decreased thus consumption of iron tablet is recom-
mended to return iron level to its normal state. The
difference between iron values before and after
chelation therapy is notable. Combination of defer-
asirox ? deferiprone shows more efficiency in
decreasing iron level. The results of iron concentra-
tions before and after chelation therapies are summa-
rized in Table 4. In order to investigate the effect of
passing time in removing mercury from the body
spontaneously, one group was treated as without
chelation therapy. The results of chelation therapy
group are shown in Tables 3 and 4. Comparison of the
results obtained from both (before and without
Table 3 The results of
mercury levels before and
after chelation therapies
Five rats were placed in
each group
Results are represented as
arithmetic mean ± SEM
and are significant at
p \ 0.05 when compared
with control
Group Before
chelation
therapy
Without
chelation
therapy
Chelation therapy
with deferiprone
Chelation therapy
with deferasirox
Combination
therapy
Heart (mg/kg)
Control
group
0 – – – –
Treated
group
43.8 ± 1.4 42.1 ± 1.2 18.2 ± 1.1 14.8 ± 1.0 6.5 ± 0.5
Liver (mg/kg)
Control
group
0 – – – –
Treated
group
27.1 ± 1.6 25.1 ± 1.3 9.6 ± 1.0 7.5 ± 1.2 3.2 ± 0.9
Kidney (mg/kg)
Control
group
0 – – – –
Treated
group
113.1 ± 2.6 110.3 ± 2.3 51.7 ± 1.1 42.2 ± 1.2 19.5 ± 0.9
Intestine (mg/kg)
Control
group
0 – – – –
Treated
group
74.4 ± 1.6 69.1 ± 1.5 39.3 ± 1.1 26.1 ± 1.3 11.2 ± 0.8
Spleen (mg/kg)
Control
group
0 – – – –
Treated
group
27.2 ± 1.6 25.2 ± 1.3 9.6 ± 1.0 7.5 ± 1.2 3.2 ± 0.9
Testicle (mg/kg)
Control
group
0 – – – –
Treated
group
28.8 ± 1.2 26.1 ± 1.0 12.7 ± 1.1 9.2 ± 1.0 3.7 ± 0.4
Biometals
123

chelation therapy) groups indicate that the passing of
time has no significant effect on the removal of
mercury.
Discussion
The aim of the present research was to evaluate the
ability of deferasirox ? deferiprone in removing
mercury from rat organs. Many studies have now
reported the high absorption, distribution, long-term
efficacy and safety of deferasirox and deferiprone in
removing some toxic metal ions and treating iron
overload in patients with b-thalassaemia major (Cap-
pellini 2008; Neufeld 2006).
In this investigation, a short-term experimental
model was used in order to speed up the preliminary
testing procedure. The effects of these chelators on
mercury and iron levels were remarkable. It has been
reported that the chelating agents having higher
stability constants with a metal in aqueous solution
may also prove successful in reducing the body burden
of the metal (Kaur et al. 1984). Inhalation of mercury
vapor after exposure showed that the accumulation of
mercury in various tissues. In order to understand the
abilities of mentioned chelators, we have done the
distribution of mercury and observed accumulation of
direct toxic effect of mercury in rat organs. After the
administration of chelating agents, the mercury con-
tent reduced. A comparison of the results obtained
Table 4 The results of iron
levels before and after
chelation therapies
Five rats were placed in
each group
Results are represented as
arithmetic mean ± SEM
and are significant at
p \ 0.05 when compared
with control
Group Before
chelation
therapy
Without
chelation
therapy
Chelation therapy
with deferiprone
Chelation therapy
with deferasirox
Combination
therapy
Heart (mg/kg)
Control
group
6.5 ± 0.3 – – – –
Treated
group
6.5 ± 0.2 6.5 ± 0.4 5.1 ± 0.3 5.1 ± 0.2 4.7 ± 0.5
Liver (mg/kg)
Control
group
6.5 ± 0.2 – – – –
Treated
group
6.5 ± 0.1 6.5 ± 0.3 5.5 ± 0.2 5.1 ± 0.3 4.6 ± 0.4
Kidney (mg/kg)
Control
group
4.9 ± 0.2 – – – -
Treated
group
4.9 ± 0.1 4.9 ± 0.3 4.3 ± 0.2 4.1 ± 0.3 3.8 ± 0.4
Intestine (mg/kg)
Control
group
4.0 ± 0.2 – – – –
Treated
group
4.0 ± 0.1 4.0 ± 0.3 3.6 ± 0.2 3.5 ± 0.3 3.1 ± 0.4
Spleen (mg/kg)
Control
group
4.2 ± 0.2 – – – –
Treated
group
4.2 ± 0.1 4.2 ± 0.3 3.7 ± 0.2 3.6 ± 0.3 3.2 ± 0.4
Testicle (mg/kg)
Control
group
3.5 ± 0.2 – – – –
Treated
group
3.5 ± 0.1 3.5 ± 0.3 3.0 ± 0.2 2.6 ± 0.3 2.4 ± 0.4
Biometals
123

from with and without chelation therapies indicate
that combined (deferasirox ? deferiprone) therapy
increases the elimination of mercury from rat organs
effectively. Also toxicity and side-effects of deferasi-
rox and deferiprone are very low, therefore after basic
preclinical research, they could be recommended for
human administration. The important finding that
deferiprone leaves tissue iron levels close to normal is
fundamental and would suggest that the proposed use
of this chelator will not be highly toxic. The reason for
this important observation is that deferiprone is able to
redistribute iron in mammals (Evans et al. 2012).
In comparison to the results obtained by (Fatemi
et al. 2007, 2009; Amiri et al. 2007; Tubafard and
Fatemi, 2008) it can be also concluded that the two
chelators (deferasirox ? deferiprone) are more effi-
cient as combined therapy than single therapy in
removing mercury from rat organs. Therefore com-
bined therapy could eliminate mercury from rat organs
and treat side-effects and the general symptoms of
toxicity caused by mercury. Thus combination of
deferasirox ? deferiprone represent a promising drug
of mercury-mobilizing agent and could be recom-
mended for human administration.
References
Amiri A, Fatemi SJ, Fatemi SN (2007) Removal of thallium by
combining desferrioxamine and deferiprone chelators in
rats. Biometals 20:159–163
Cappellini MD (2008) Long-term efficacy and safety of defer-
asirox. Blood Rev 2:35–41
Clarke ET, Martell AE (1992) Stabilities of 1,2-dimethyl-3-
hydroxypyrid-4-one chelates of divalent and trivalent
metal ions. Inorg Chim Acta 19:57–63
Evans RW, Kong X, Hider RC (2012) Iron mobilization from
transferrin by therapeutic iron chelating agents. Biochim
Biophys Acta 1820:282–290
Fatemi SJ, Amiri A, Bazargan MH, Tubafard S, Fatemi SN
(2007) Clinical evaluation of desferrioxamine (DFO) for
removal of thallium ions in rat. Int J Artif Organs
30:902–905
Fatemi SJ, Tubafard S, Nadi B (2009) Evaluation of the effect of
cadmium on rat organs and investigation of diethyl car-
bamate as an oral drug in treatment of cadmium toxicity.
Med Chem Res 18:179–186
Flora SJS, Bhattacharyan R, Vijayaraghavan R (1995) Com-
bined therapeutic potential of meso dimercaptosuccinic
acid and calcium edentate on the mobilization and distri-
bution of lead in experimental lead intoxication in rats.
Fundam Appl Toxicol 25:233–240
Galanello R, Agus A, Campus S, Danjou F, Giardina PJ, Grady
RW (2010) Combined iron chelation therapy. Ann N Y
Acad Sci 1202:79–86
Glickstein H, BenEl R, Link G, Breuer W, Konijn AM,
Hershko C, Nick H, Cabantchik ZI (2006) Action of chelators
in iron-loaded cardiac cells: accessibility to intracellular labile
iron and functional consequences. Blood 108:3195–3203
Gomez W, Esparza JL, Domingo JL, Singha PK, Jones MM
(1988) Comparative aluminium mobilizing action of des-
ferrioxamine and four 3-hydroxypyrid-4-ones in alumin-
ium-loaded rats. Toxicology 130:175–181
Grandjean P, White RF, Nielsen A, Cleary D, de Oliveira Santos
EC (1999) Methylmercury neurotoxicity in Amazonian
children downstream from gold mining. Environ Health
Perspect 107:587–591
Gyparaki M, Porter JB, Hirani S, Streater M, Hider RC,
Huehns ER (1987) In vivo evaluation of hydroxypyridone
iron chelators in a mouse model. Acta Haematol 78:217–221
Hershko C, Konijn AM, Nick HP, Breuer W, Cabantchik ZI, Link
G (2001) ICL670A: a new synthetic oral chelator: evaluation
in hypertransfused rats with selective radioiron probes of
hepatocellular and reticuloendothelial iron stores and in iron-
loaded rat heart cells in culture. Blood 97:1115–1122
Hider RC, Kontoghiorghes G and Silver J (1984) Pharmaceu-
tical compositions. GB patent 2118176 A
Kaur G, Srivastava UC, Dwivedi RS, Srivastava RC (1984)
Influence of polyaminocarboxylic acids on the removal of
manganese-54 from the body organs of sham-operated and
partially hepatectomized rats. Toxicol Lett 22:1–6
Kontoghiorghes GJ, Aldouri MA, Hoffbrand AV, Barr J, Wonke
B, Kourouclaris T, Sheppard L (1987) Effective chelation
of iron in beta thalassaemia with the oral chelator 1,2-
dimethyl-3-hydroxypyrid-4-one. Br Med J 295:1509–1512
Ma Y, Zhou T, Kong X, Hider RC (2012) Chelating agents for
the treatment of systemic iron overload. Curr Med Chem
19:2816–2827
Magos L, Halbach S, Clarkson TW (1978) Role of catalase in
the oxidation of mercury vapor. Biochem Pharmacol
27:1373–1377
Neufeld EJ (2006) Oral chelators deferasirox and deferiprone
for transfusional iron overload in thalassemia major: new
data, new questions. Blood 107(9):3436–3441
Nisbet-Brown E, Olivieri NF, Giardina PJ, Grady RW, Neufeld
EJ, Sechaud R (2003) Effectiveness and safety of ICL670
in iron-loaded patients with thalassaemia: a placebo-con-
trolled, dose-escalation trial. Lancet 361:1597–1602
Steinhauser S, Heinz U, Bartholoma M, Weyhermuller T, Nick
H, Hegetschweiler K (2004) Complex formation of
ICL670 and related ligands with Fe(III) and Fe(II). Eur J
Inorg Chem 21:4177–4192
Tubafard S, Fatemi SJ (2008) Chelation of bismuth by com-
bining desferrioxamine and deferiprone in rats. Toxicol Ind
Health 24:235–240
Voskaridou E, Christoulas D, Terpos E (2011) Successful che-
lation therapy with the combination of deferasirox and
deferiprone in a patient with thalassaemia major and per-
sisting severe iron overload after single-agent chelation
therapies. Br J Haematol 154:654–656
Yang LPH, Keam SJ, Keating GM (2007) Deferasirox: a review
of its use in the management of transfusional chronic iron
overload. Drugs 67:2211–2230
Biometals
123