transverse myelitis in systemic lupus erythematosus filereumatol clin. 2007;3(2):73-7 73 mielitis...
TRANSCRIPT

Reumatol Clin. 2007;3(2):73-7 73
Mielitis transversa en lupus eritematoso sistémico
Objetivo: La mielitis transversa aguda (MTA) es una rara complicación en los pacientes con lupus eritematososistémico (LES). Revisamos nuestra serie de pacientescon LES para determinar la prevalencia de MTA y analizar las características clínicas, las pruebascomplementarias, la evolución y la respuesta altratamiento.Pacientes y método: Se identificó a 6 pacientes con MTAque se sometieron a valoración clínico-neurológica,resonancia magnética y estudio electrofisiológico yrecibieron el mismo tratamiento. Realizamos un estudioestadístico descriptivo.Resultados: Observamos una prevalencia de MTA del0,92% de nuestros pacientes con LES. El 83,3%presentaba anticuerpos antifosfolipídicos y/oanticoagulante lúpico. La resonancia magnética confirmóel diagnóstico en 5 de los 6 casos; 3 de los 5 pacientes conanticuerpos antifosfolipídicos fueron anticoagulados oantiagregados, con buena evolución neurológica; 2 deellos han quedado sin secuelas.Conclusiones: Encontramos una prevalencia similar a laobservada en otras series, en torno al 1%. La altaprevalencia de anticuerpos antifosfolipídicos en lospacientes, con buen resultado en los antiagregados oanticoagulados, indica un importante papel patogénico enel desarrollo de la MTA, y nos hace plantearnos laimportancia de añadir al tratamiento estándar terapiaantiagregante o anticoagulante.
Palabras clave: Mielitis transversa. Lupus eritematososistémico. Anticuerpos antifosfolipídicos.
Introduction
Neuropsychiatric manifestations are present in up to 60%of patients with systemic lupus erythematosus (SLE).Acute transverse myelitis (ATM), a very uncommonneurological manifestation, occurs in 1%-2%. The physiopathologic mechanism of ATM in SLE isunknown, though inflammatory and arterial thromboticphenomena have been proposed. A greater prevalence of
Correspondence: Dra. M.L. Velloso Feijoo.Avda. Ramón Carande, 7, portal 4, 2.o A. 41013 Sevilla. España.E-mail: [email protected]
Manuscript received September 11, 2006; accepted for publication January31, 2007.
Objective: Transverse myelitis (TM) is a rarecomplication in patients with systemic lupuserithematosus (SLE). We reviewed a series of our SLEpatients to determine the prevalence of TM, and evaluatethe clinical characteristics, medical tests, evolution, andresponse to the treatment.Patients and method: Six patients with TM wereidentified and underwent a neurological evaluation, MRI,electrophysiologic study, and were all subjected to thesame treatment. A descriptive statistical study wasconducted.Results: We observed a prevalence of 0.92% in ourpatients with SLE. Eighty-three point three per cent hadantiphospholipid antibodies and/or lupus anticoagulant.The MRI confirmed the diagnosis in 5 cases. Of the 5 patients with antiphospholypid antibodies, 3 wereanticoagulated or took aspirin with a good neurologicaloutcome, leaving 2 of them without posteriorcomplications.Conclusions: We found a prevalence similar to thatobserved in other series, around 1%. The high prevalenceof antiphospholypid antibodies in these patients, withgood outcome in those anticoagulated or treated withantiplatelet agents suggests an important pathogenic rolein the development of TM, and emphasized thepossibility of adding to the standard treatment,antiplatelet agents, or anticoagulation.
Key words: Transverse myelitis. Systemic erithematosuslupus. Antiphospholipid antibodies.
Transverse Myelitis in Systemic Lupus Erythematosus
María Luisa Velloso Feijoo, Francisco García Hernández, Celia Ocaña Medina, Rocío González León,Rocío Garrido Rasco, and Julio Sánchez Román
Unidad de Colagenosis, Servicio de Medicina Interna, Hospital Universitario Virgen del Rocío, Sevilla, Spain
Original Articles
Document downloaded from http://www.elsevier.es, day 30/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from http://www.elsevier.es, day 30/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

antiphospholipid antibodies has been described in patientswith SLE and ATM than in the general population ofpatients with SLE,1-3 something that could have importantimplications to decide whether if these patients are suitablefor anticoagulant treatment or not.Different authors have proposed different treatmentregiments for this entity, based on high-dose steroids,combined or not with immunosuppresants and/orplasmapheresis.The main objective of the present study is to determinethe prevalence of ATM in our series of patients with SLEand to describe their clinical characteristics as well as thefindings of complementary testing as well as the evolutionand the response to treatment.
Patients and Methods
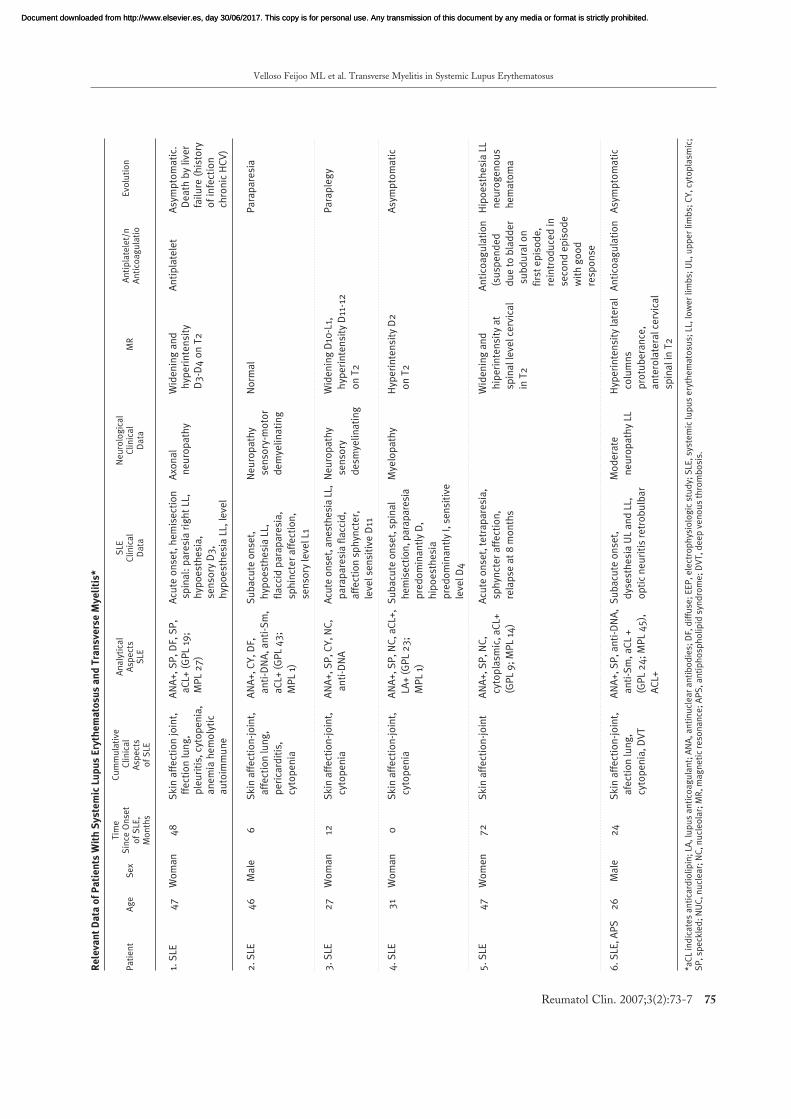
From a total population of 650 patients with SLE,classified according to the ACR criteria and attended atthe Unit of Collagenosis of the Hospital Virgen del Rocíoin Sevilla, 6 patients with ATM were identified in thelast 10 years.The diagnosis of ATM was done according to the clinicalcharacteristics that reflected spinal cord lesion, such assensory and/or motor sphincter dysfunction, documentedwith the magnetic resonance imaging (MR) findings, andother tests. Patients were studied through a clinical and neurologicalevaluation, MR and an electrophysiologic study. ELISA(enzyme-linked immunosorbent assay) was employed for thedetermination of anticardiolipin antibodies and normalvalues were 0 to 20 and 0 to 10 units GPL and MPL forIgG and IgM isotypes, respectively. All patients weretreated using the same therapeutic scheme. A descriptive statistical analysis was carried out, takinginto account numerical and qualitative variables, expressedas means ± standard deviations and expressed throughTables and percentages. The most relevant patient data reviewed is presented in Table 1.
Results
In our series of patients with SLE, ATM was seen witha frequency of 0.92%; 66.6% of patients were women;mean age at the onset of ATM was 37.33±10.367 years.The clinical characteristics related to lupus were varied.All patients had skin and joint affection; 50% had lunginvolvement; 33.3% had presented serositis in somemoment of their evolution; 83.3% had some typo ofcytopenia and 16.7% had presented autoimmune hemolyticanemia.We proved the presence of antinuclear antibodies (ANA)in all patients, with diverse immunofluoresence patterns:
Velloso Feijoo ML et al. Transverse Myelitis in Systemic Lupus Erythematosus
74 Reumatol Clin. 2007;3(2):73-7
speckled (present in 83.3%), diffuse (66.7%), cytoplasmic(50%), nucleolar (50%), anti-Sm antibodies (33.3%), andnuclear (16.7%). Anti-DNA antibodies were positive in50%. As for the presence of antihospholipid antibodies, 83.3%(5 of 6 patients) had positive results for anticardiolipinantibodies and/or lupus anticoagulant: IgG anticardiolipinantibodies in 60% and IgM in 40% and lupus anticoagulant(elongated partial thromboplastin time without correctionafter the addition of normal plasma) in 33.3%. Only 1patient had presented a previous thrombotic event, namelya deep venous thrombosis. The time since onset of SLE, when ATM appeared, was27±27,821 months; it was the first manifestation of SLEin 1 of the 6 patients. The start of the manifestation was acute in 50% of casesand subacute in the rest. In 33.3%, ATM was manifestedas a Brown-Sequard syndrome. In the majority ofpatients (5 out of 6) a sensitive level was present: 4 inthe dorsal spine and 1 in the lumbar spine. Sphincterdysfunction was present in 50% and 1 patient had acase of optic neuritis; 33.3% of cases were associatedto fever. RM confirmed the diagnosis in 83.3% of cases, showingwidening and an increase in signal of the spinal cord tissue,on T2 (Figure 1). An electrophysiologic study was carriedout in 5 of 6 patients; they all showed alterations compatiblewith sensorymotor demyelinating axonal neuropathy. As mentioned, the same therapeutic scheme was employedin all patients, consisting in 3 bolus doses of 1 gmethylprednisolone on 3 consecutive days when startingwith the manifestations and 6 bolus doses ofcyclophosphamide at 15 mg/kg, monthly during the first6 months and 6 trimestral doses during the following 18months. After the pulse therapy, patients received oralsteroids at a dose of 0.5-1 mg/kg/day of prednisone orthe equivalent, in a descending pattern until a maintenancedose of 10-15 mg/day was reached; 16.7% of the patientsreceived antiplatelet therapy and 33.3% receivedanticoagulation. One of the latter presented a subduralhematoma that forced the suspension of oral anticoagulants.The evolution of the hematoma was favorable, but a newbout of ATM developed (the only patient that presentedrecurrence) 8 months later; anticoagulation was restored,with a good response. Response to treatment was favorablein 83.3% of cases, with a very heterogeneous time ofrecuperation; 50% of patients remained asymptomatic andwithout sequelae. The mean follow-up time of thesepatients up until currently was 8 years. A patient withchronic hepatitis C infection died as a consequence of theprogressive deterioration of liver function. Apart fromstandard therapy, 3 of the 5 patients positive forantiphospholipid antibodies received antiplatelet ofanticoagulant therapy, with a favorable evolution of theneurological clinical signs and symptoms; 2 of themremained without sequelae.
Document downloaded from http://www.elsevier.es, day 30/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from http://www.elsevier.es, day 30/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Velloso Feijoo ML et al. Transverse Myelitis in Systemic Lupus Erythematosus
Reumatol Clin. 2007;3(2):73-7 75
Re
leva
nt
Da
ta o
f P
ati
en
ts W
ith
Sy
ste
mic
Lu
pu
s E
ryth
em
ato
sus
an
d T
ran
sve
rse
My
eli
tis*
Tim
e
Cu
mm
ula
tive
An
aly
tica
l S
LE
Ne
uro
log
ica
lP
ati
en
tA
ge
Se
xS
ince
On
set
Cli
nic
al
Asp
ect
s C
lin
ica
l C
lin
ica
l M
RA
nti
pla
tele
t/n
Evo
luti
on
of
SLE
, A
spe
cts
SLE
Da
taD
ata
An
tico
ag
ula
tio
Mo
nth
so
f S
LE
1. S
LE4
7W
om
an
48
Sk
in a
ffe
ctio
n j
oin
t,
AN
A+
, S
P,
DF,
SP
,A
cute
on
set,
he
mis
ect
ion
Axo
na
lW
ide
nin
g a
nd
A
nti
pla
tele
tA
sym
pto
ma
tic.
ffe
ctio
n l
un
g,
aC
L+ (
GP
L 19
;sp
ina
l: p
are
sia
rig
ht
LL,
ne
uro
pa
thy
hyp
eri
nte
nsi
tyD
ea
th b
y li
ver
ple
uri
tis,
cyt
op
en
ia,
MP
L 2
7)
hyp
oe
sth
esi
a,
D3
-D4
on
T2
fail
ure
(h
isto
rya
ne
mia
he
mo
lyti
c se
nso
ry D
3,
of
infe
ctio
na
uto
imm
un
eh
ypo
est
he
sia
LL,
le
vel
chro
nic
HC
V)
2.
SLE
46
Ma
le6
Sk
in a
ffe
ctio
n-j
oin
t,
AN
A+
, C
Y,
DF,
Su
ba
cute
on
set,
N
eu
rop
ath
yN
orm
al
Pa
rap
are
sia
aff
ect
ion
lun
g,
an
ti-D
NA
, a
nti
-Sm
,h
ypo
est
he
sia
LL,
sen
sory
-mo
tor
pe
rica
rdit
is,
aC
L+ (
GP
L 4
3;
fla
ccid
pa
rap
are
sia
,d
em
yeli
na
tin
g
cyto
pe
nia
MP
L 1)
sph
inct
er
aff
ect
ion
,
sen
sory
leve
l L1
3.
SLE
27
Wo
ma
n12
Sk
in a
ffe
ctio
n-j
oin
t,
AN
A+
, S
P,
CY
, N
C,
Acu
te o
nse
t, a
ne
sth
esi
a L
L,N
eu
rop
ath
yW
ide
nin
g D
10-L
1,P
ara
ple
gy
cyto
pe
nia
an
ti-D
NA
pa
rap
are
sia
fla
ccid
, se
nso
ry
hyp
eri
nte
nsi
ty D
11-1
2
aff
ect
ion
sp
hyn
cte
r,
de
smye
lin
ati
ng
on
T2
leve
l se
nsi
tive
D11
4.
SLE
31
Wo
ma
n0
Sk
in a
ffe
ctio
n-j
oin
t,
AN
A+
, S
P,
NC
, a
CL+
,S
ub
acu
te o
nse
t, s
pin
al
Mye
lop
ath
yH
ype
rin
ten
sity
D2
Asy
mp
tom
ati
c
cyto
pe
nia
LA+
(G
PL
23
; h
em
ise
ctio
n, p
ara
pa
resi
ao
n T
2
MP
L 1)
pre
do
min
an
tly
D,
hip
oe
sth
esi
a
pre
do
min
an
tly
I, s
en
siti
ve
leve
l D4
5.
SLE
47
Wo
me
n7
2S
kin
aff
ect
ion
-jo
int
AN
A+
, S
P,
NC
, A
cute
on
set,
te
tra
pa
resi
a,
Wid
en
ing
an
dA
nti
coa
gu
lati
on
Hip
oe
sth
esi
a L
L
cyto
pla
smic
, a
CL+
sph
ynct
er
aff
ect
ion
,h
ipe
rin
ten
sity
at
(su
spe
nd
ed
ne
uro
ge
no
us
(GP
L 9
; M
PL
14)
rela
pse
at
8 m
on
ths
spin
al l
eve
l ce
rvic
al
du
e t
o b
lad
de
rh
em
ato
ma
in T
2su
bd
ura
l on
firs
t e
pis
od
e,
rein
tro
du
ced
in
seco
nd
ep
iso
de
wit
h g
oo
d
resp
on
se
6.
SLE
, A
PS
26
Ma
le2
4S
kin
aff
ect
ion
-jo
int,
A
NA
+,
SP
, a
nti
-DN
A,
Su
ba
cute
on
set,
Mo
de
rate
Hyp
eri
nte
nsi
ty la
tera
lA
nti
coa
gu
lati
on
Asy
mp
tom
ati
c
afe
ctio
n lu
ng
, a
nti
-Sm
, a
CL
+d
yse
sth
esi
a U
L a
nd
LL,
n
eu
rop
ath
y LL
colu
mn
s
cyto
pe
nia
, D
VT
(GP
L 2
4;
MP
L 4
5),
o
pti
c n
eu
riti
s re
tro
bu
lba
rp
rotu
be
ran
ce,
AC
L+a
nte
rola
tera
l ce
rvic
al
spin
al i
n T
2
*aC
L in
dic
ate
s a
nti
card
ioli
pin
; LA
, lu
pu
s a
nti
coa
gu
lan
t; A
NA
, a
nti
nu
cle
ar
an
tib
od
ies;
DF,
dif
fuse
; E
EP
, e
lect
rop
hys
iolo
gic
stu
dy;
SLE
, sy
ste
mic
lup
us
ery
the
ma
tosu
s; L
L, lo
we
r li
mb
s; U
L, u
pp
er
lim
bs;
CY
, cy
top
lasm
ic;
SP
, sp
eck
led
; N
UC
, n
ucl
ea
r; N
C,
nu
cle
ola
r; M
R,
ma
gn
eti
c re
son
an
ce;
AP
S,
an
tip
ho
sph
oli
pid
syn
dro
me
; D
VT
, d
ee
p v
en
ou
s th
rom
bo
sis.
Document downloaded from http://www.elsevier.es, day 30/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from http://www.elsevier.es, day 30/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

Discussion
ATM is a rare but serious complication in patients withSLE. Its low prevalence is estimated approximately 1%-2% of this patient population, and this is confirmedonce more in our series of patients, which was around1%. Our patients developed it in the first 6 years since diseasediagnosis, coinciding with the start of the disease in oneof them, circumstance that has been mentioned in somestudies in which it is communicated in up to 39% ofcases in which ATM was the initial manifestation ofSLE.1,2
The clinical spectrum of the disease is varied4 and wefound no trace of the underlying disease associated in acharacteristic manner to ATM. The case of the patient with chronic hepatitis C infection,who died due to liver dysfunction, a special mention isdeserved because it is the first communicated case in themedical literature of interferon-alpha induced SLE inpatients with hepatitis C.5
One of our patients developed optic neuromyelitis,described by Devic in 1894 and related to the presence ofantiphospholipid antibodies.6
Through MR, considered the best imaging technique forATM,7 the diagnosis was confirmed in 5 of 6 patients.Nonetheless, in close to 40% of ATM there are nodemonstrable alterations through MR: Mok et al8 observedMR alterations in 56%, Kovacs et al2 in 70%, and D´Cruzet al1 in 93%. There is no consensus for the treatment of thismanifestation of SLE, probably due to its scarce incidence,though the majority of the authors coincide in theimportance of its early installation.9 The use of steroidsat a high dose is recommended, associated to the use ofimmunosuppressants. Kovacs et al2 observed that theclinical manifestations of ATM improve with theadministration of intravenous methylprednisolone, butthe results are better if pulse cyclophosphamide is added.In a clinical trial published by Barile et al10 in patientswith SLE and neurological manifestations,cyclophosphamide is more efficacious than the use ofmethylprednisolone, used in a dose of 0.75 g/m2 bodysurface monthly during 1 year and every 3 months foranother year. Mok et al8 pointed out that cyclophosphamideseems to be more effective than azathioprine regardingthe remaining functional situation. Several authors have shown the that the strong associationbetween ATM and the presence of antiphospholipidantibodies,1-3,9 larger than in the general population ofSLE patients (estimated in 30%-50%). It seems veryprobable that they have an important role in thepathogenesis of this disease, through their interactionwith the spinal phospholipids.11 Thrombosis of the spineblood vessel would explain a larger dorsal affection becausethe vessels are smaller but, in the few autopsy studies
published, necrosis of the spine has been shown, but nothrombosis of the spinal vessels. In any case, it is difficultto precise if it is a thrombotic phenomenon or aninflammatory one, or a combination of both. The role of anticoagulation is a controversial topic, stillnot having been resolved in the ATM associated toSLE. It seems reasonable to install it in patients withantiphospholipid antibodies due to their prothromboticpower. The high prevalence of antiphospholipidantibodies in our patients (83.3%), with a good outcomein those that underwent anticoagulant or antiplatelettherapy, indicating the important role these antibodiesplay in the pathogenesis and development of ATM andforces us to consider adding anticoagulant or antiplatelettherapy to the standard therapy with steroids andimmunosuppresants.Controlled studies are needed to approach the developmentof therapeutic strategies, attending specially the need foanticoagulation and antiplatelet therapy.
References
1. D´Cruz DP, Mellor-Pita S, Joven B, Sana G, Allason J, Taylor J, et al.Transverse myelitis as the first manifestation of systemic lupus erithematosusor lupus-like disease: good functional outcome and releance of antiphospholipidantibodies. J Rheumatol. 2004;31:280-5.
2. Kovacs B, Lafferty Brent LH, deHoratius RJ. Transverse myelopathy insystemic lupus erythematosus: an analisis of 14 cases and review of theliterature. Ann Rheum Dis. 2000;59:120-4.
3. Lavalle C, Pizarro S, Drenkard C, Sánchez-Guerrero J, Alarcón-Segovia D.Transverse myelitis: a manifestation of systemic lupus erythematosus stronglyasociated with antiphospholipid antibodies. J Rheumatol. 1990; 17:34-7.
4. Chan KF, Boey ML. Transverse myelopathiy in SLE: clinical features andfunctional outcomes. Lupus. 1996;5:294-9.
5. Sánchez Román J, Castillo Palma MJ, García Díaz E, Ferrer Ordínez JA.Lupus eritematoso sistémico inducido por interferón alfarrecombinante. MedClin (Barc). 1994;102:198.
6. Ferreira S, Marquez P, Carneiro E, D’Cruz D, Gama G. Devic´s syndromeand probable antiphospholipid syndrome. Rheumatology. 2005;44:693-5.
7. Boumpas DT, Patronas NJ, Dalakas MC, Hakim CA, Klippel JH, BalowJE. Acute transverse myelitis in systemic lupus erythematosus: magnetic
Velloso Feijoo ML et al. Transverse Myelitis in Systemic Lupus Erythematosus
76 Reumatol Clin. 2007;3(2):73-7
Figure. Magnetic resonance indicating a widening and increase inintensity of signal in the cervical spinal cord on T2.
Document downloaded from http://www.elsevier.es, day 30/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from http://www.elsevier.es, day 30/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

resonance imaging and review of the literature. J Rheumatol. 1990;17:89-92.
8. Mok CC, Lau CS, Chan EY, Wong RW. Acute transverse myelopathy insystemic lupus erythematosus: clinical presentation, treatment and outcome.J Rheumatol. 1998;25:467-73.
9. Sherer Y, Hassin S, Shoenfeld Y, Levy Y, Lionel A, Ohry A, et al. Transversemyelitis in patients with antiphospholipid antobodies, the importance ofearly diagnosis and treatment. Clin Rheumatol. 2002;21:207-10.
10. Barile-Fabris L, Ariza-Andraca R, Olquin-Ortega L, Jara LJ, Fraga MouretA, Miranda-Limon JM, et al. Controlled clinical trial of IV cyclophosphamide versus IV methylprednisolone in severe neurologicalmanifestations in systemic lupus erythematosus. Ann Rheum Dis.2005;64:620-5.
11. Chapman J, Cohen-Armon M, Shoenfeld Y, Korczyn AD. Antiphospholipidantibodies permeabilize and depolarize brain synaptoneurosomes. Lupus.1999;8:127-33.
Velloso Feijoo ML et al. Transverse Myelitis in Systemic Lupus Erythematosus
Reumatol Clin. 2007;3(2):73-7 77
Document downloaded from http://www.elsevier.es, day 30/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from http://www.elsevier.es, day 30/06/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.