transitioning from… transitioning baby...transitioning baby to the breast ©2015 nancy mohrbacher,...
TRANSCRIPT
Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 1
Transitioning Baby to the Breast
Nancy Mohrbacher,
IBCLC, FILCA
~
Transitioning from…
• Bottle
• Sipping or lapping methods– Cup
– Bowl
– Spoon
– Syringe
• Tube feeding Preterm/ill baby
• Nipple shield
Does It Really Matter
How Baby Gets the Milk?
Rasmussen & Geraghty. Am J
Public Health 2011; 101(8):1356-59
Long-term pumping can be a hardship
• Stressful: “Triple duty” compared to breastfeeding
• Hormonal levels differ from less body contact
Affects breastfeeding duration
• 4 months after preterm birth:
– 72% still breastfeeding
– 10% still pumping Smith, et al. Pediatrics 2003; 111(6 Pt 1):1337-42
• Earlier formula use increases risk of
negative health outcomes Ip, et al. Evid Rep Technol Assess 2007; (153):1-186
Affects milk quality
• After expression, vitamin, antioxidant, immunological levels decrease
• Freezing kills live cells
• Contamination risk
• Leaching from container & effect on components
Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 2
Affects baby’s oral development • Breastfeeding
promotes normal oral development
• Bottle-feeding increases risk of oral malformations
– Cross-bite
– Maxillary atresiaCarrascoza, et al. J Pediatria 2006; 82:395-97 . Kobayashi, et al. Am J Orthod Dentofacial Orthop 2010; 137:54-58
Galán-Gónzalez, et al. Breastfeed Med 2014; 9(1):24-28
Affects feeding volumes, weight gain & obesity risk
• Consistent flow = more milk faster
• Overrides appetite control mechanism
Li, et al. Arch Pediatr Adolesc Med 2012; 166(5):431-36
Affects stress levels in preemies
• Fast milk flow of bottle disrupts organization of suck-swallow-breathing
• Greater incidence of oxygen desaturation, apnea, bradycardia
Photo: The Breastfeeding Atlas
Meier. Nurs Res 1988; 37(1):36-41 Meier & Anderson. MCN Am J Matern Child Nurs 1987; 12(2):97-105
At what age should we lose hope that baby will breastfeed?
Breast-seeking behaviors seen 8 mo to school age
Despite age & other feeding methods, older babies & toddlers do transition to breast
Gribble. Journal of Prenatal & Perinatal Psychology & Health 2005; 19(3):217-35
Babies are hardwired to breastfeed Priorities
1. Feed the baby
2. Protect mother’s milk production
3. Support baby’s transition to breast

Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 3
Our Primary Job: Ooze Confidence
in Breastfeeding
With Any
Transition
Start with
the Basics
• Share positive time together there– Talk
– Smile
– Play
• Don’t let it become a battleground
Keep the Breast a Pleasant Place
Keep the Breast a Pleasant Place
Mother leans back & baby rests hands free,
tummy down on her body
Let Gravity Help
• Videotaped 40 mothers/baby pairs
• 20 primitive neonatal reflexes (PNRs)
• PNRs work for or against breastfeeding, depending on positioning
Colson, et al. Early Hum Dev 2008; 84(7):441-9 Photo: Melanie Ham
Identified 20 Primitive Neonatal Reflexes Colson, et al. Early Hum Dev 2008; 84(7):441-49
• Tongue licking• Arm & leg cycling• Head lifting• Head bobbing• Stepping, crawling
Include:• Rooting• Suck• Swallow• Hand to mouth• Mouth gaping
Found more PNRs led to breastfeeding when
mothers lean back with baby on top (p=<0.0005)
Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 4
Sitting up, PNRs
made latching more difficult
Pull of gravity caused gaps, head-butting, arching away
Photo: Melanie Ham
A newborn’s curved spine
makes her flail like a turtle on its back
Turn baby over & she has much more body control
Start with Positions Easier for Baby Adjust Body, Baby, Breast
www.YouTube.com/NancyMohrbacher
Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 5
Adjust Your Baby
Think Clock
Baby Heads Up
Adjust Your Breast,Think Sandwich
• Compress breast into an oval
• Fingers parallel to baby’s lips
• Like hamburger, not taco
Wiessinger. J Hum Lact 1998; 14(1):51-56
“Breast sandwich”Photo: The Breastfeeding Atlas
“Nipple-Tilting”Photo: Rebecca Glover, RM, IBCLC
Breast Shaping
Keep baby at breast level, less to juggle
Use Sleep
Lowers baby’s resistance to the breast
• Breastfeed while baby sleeps
• Hold baby at breast during sleep
Smillie in Genna, Supporting Sucking Skills in Breastfeeding
Infants, 2013 Photo: Melanie Ham
Cuddle drowsy, sleeping baby in natural feeding positions
• Triggers inborn reflexes
• Blunts reflex response & frustration
Colson. MIDIRS Midwifery Digest 2003; 13(1):92-97
Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 6
Basics Checklist
� If mother lifts her arms, does baby stay in place?
� Is mother fully relaxed & partly reclined,
not upright or completely flat?
� Is baby tummy down (frog legs) & heads up
(head higher than bottom)?
� Tried varying baby’s lie (clock)?
� Baby’s feet touching mother or something else?
� Tried breast shaping (hamburger not taco)?
� Is baby upset, need to be calmed (arousal state)?
Skin-to-Skin and Body Contact
Without pressure to take breast
If baby becomes unhappy, move away
Chiu, et al. Breastfeed Med 2008; 3(4):231-37
With Severe Latch Problems
• Half were skin-to-skin during breastfeeding tries, half weren’t
• Same % overcame problems
• In STS group, happened twice as fast
Svensson, et al. Int Breastfeed J 2013; 8:1; 103 babies 1-16 wk old
If awake, feed a little so baby’s not ravenously hungry
Will be more open to trying something new
Photo: Kirsten Hedberg Nyqvist, RN, PhD
Feed a Little First
IF BABY STILL BALKS AT THE
BREAST, CONSIDER THE 4 Fs
• FEEL• FLOW• FAMILIARITY• FITNESS to
breastfeed
Target Strategies to the Cause
Glover & Wiessinger. In Supporting Sucking Skills in Breastfeeding
Infants, 2nd ed. by C.W. Genna, 2013, p. 105-48
Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 7
FEEL?• Expectations
altered by artificial nipples?
• Positioned to trigger feeding behaviors?
• Latched deeply enough to trigger active sucking?
FEEL Issues
• Use positioning, body contact, & sleep to release feeding reflexes
• Adjust for a deeper latch
Use tools to evert or firm mother’s nipple (FEEL):
• Inverted syringe
• Nipple everter
• Apply cold
• Breast pump
• Nipple shield
Kesaree, et al. J Hum Lact 1993; 9(1):27-29
FLOW?• Baby used to instant, consistent flow?
• Mother’s milk production low?
To increase flow
• Boost low milk production
• Deliver instant flow at breast
−Spoon
−Eyedropper
−Syringe
−At-breast supplementer
• Negative oral experiences?
• Hair-trigger temperament?
• Used to another feeding method?
FAMILIARITY?
Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 8
FAMILIARITY Issues
When transitioning from another
feeding method, take baby steps
Sipping/Lapping Methods
Muscles used more similar to breastfeeding than bottlefeedingFranca, et al. BMC Pregnancy Childbirth 2014; 14:154
May lead to easier transition to the breastYilmaz, et al. J Hum Lact
2014; 30(2):174-79
Photo: Kirsten Hedberg Nyqvist, RN, PhD
Baby Steps from the Bottle
Make bottle-feeding more like breastfeeding
Kassing. J Hum Lact
2002; 18(1):56-60
Photos: Karl B. Walker
Bottle-feed at breast
• Rest baby’s cheek against exposed breast
• Wrap bottle in cloth so baby can’t touch it
Photo: The Breastfeeding Atlas
’Bait & Switch’
Start bottle-feeding against exposed breast
As baby sucks and swallows, quickly remove bottle and insert breast
Photo: The Breastfeeding Atlas

Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 9
FITNESS to breastfeed
Is baby in pain?
Is there a physical or health issue
affecting breastfeeding?
Photo: The Breastfeeding Atlas
Fitness Issues Genna, Supporting Sucking Skills, 2013
Baby• Unusual oral
anatomy?
• Pain or birth injuries?
• Respiratory issues?
• Preterm?
• Health issues?
• Neurological or tone issues?
Mother• Large
breasts?
• Taut breast tissue?
• Unusual nipple placement?
• Unusual nipple anatomy?
Do What
Works.
Don’t Do
What
Doesn’t
Work.
One Mother’s Story
0
100
200
300
400
500
600
700
800
900
0 1 2 3 4 5 6 7 8 9 10
ml
weeks
Daily average of supplement given to baby
ave MyS
ave F
Transitioning Preterm Babies to the Breast
Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 10
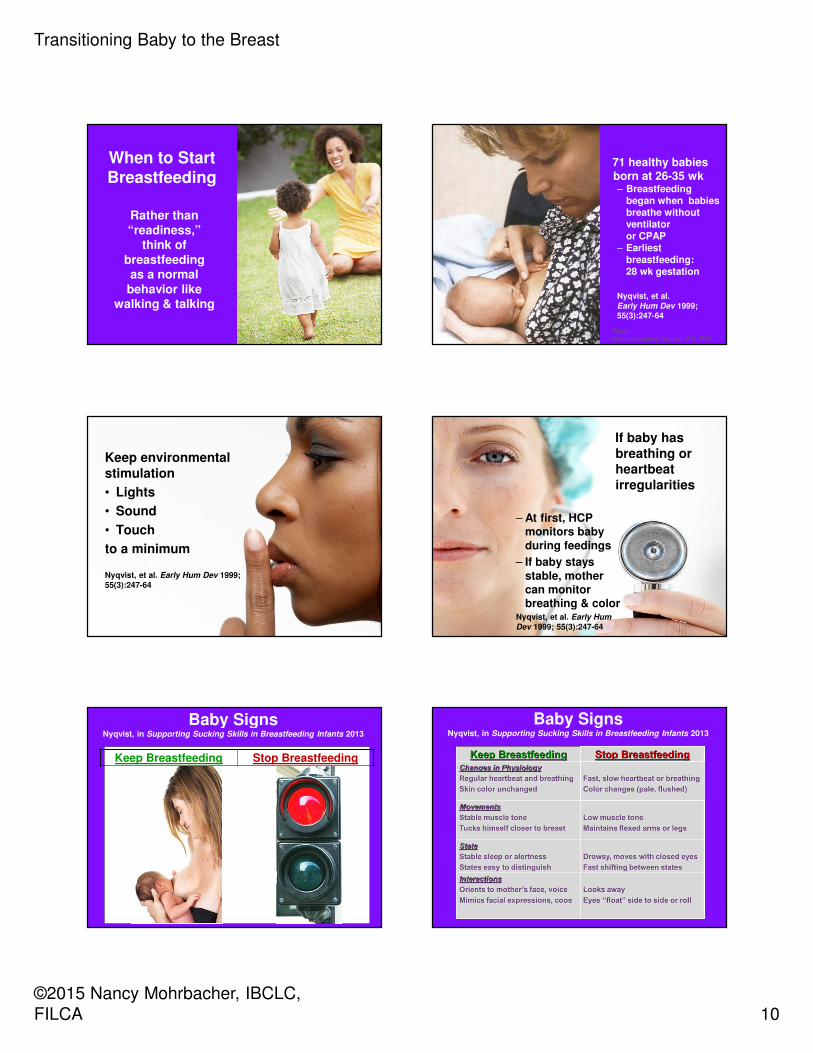
When to Start Breastfeeding
Rather than “readiness,”
think of breastfeeding as a normal
behavior like walking & talking
71 healthy babies born at 26-35 wk– Breastfeeding
began when babies breathe without ventilator or CPAP
– Earliest breastfeeding: 28 wk gestation
Nyqvist, et al. Early Hum Dev 1999; 55(3):247-64
Photo: Kirsten Hedberg Nyqvist, RN, PhD
Keep environmental stimulation
• Lights
• Sound
• Touch
to a minimum
Nyqvist, et al. Early Hum Dev 1999; 55(3):247-64
If baby has breathing or heartbeat irregularities
– At first, HCP monitors baby during feedings
– If baby stays stable, mother can monitor breathing & color
Nyqvist, et al. Early Hum
Dev 1999; 55(3):247-64
Baby Signs Nyqvist, in Supporting Sucking Skills in Breastfeeding Infants 2013
Keep Breastfeeding Stop Breastfeeding
Baby Signs Nyqvist, in Supporting Sucking Skills in Breastfeeding Infants 2013
Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 11
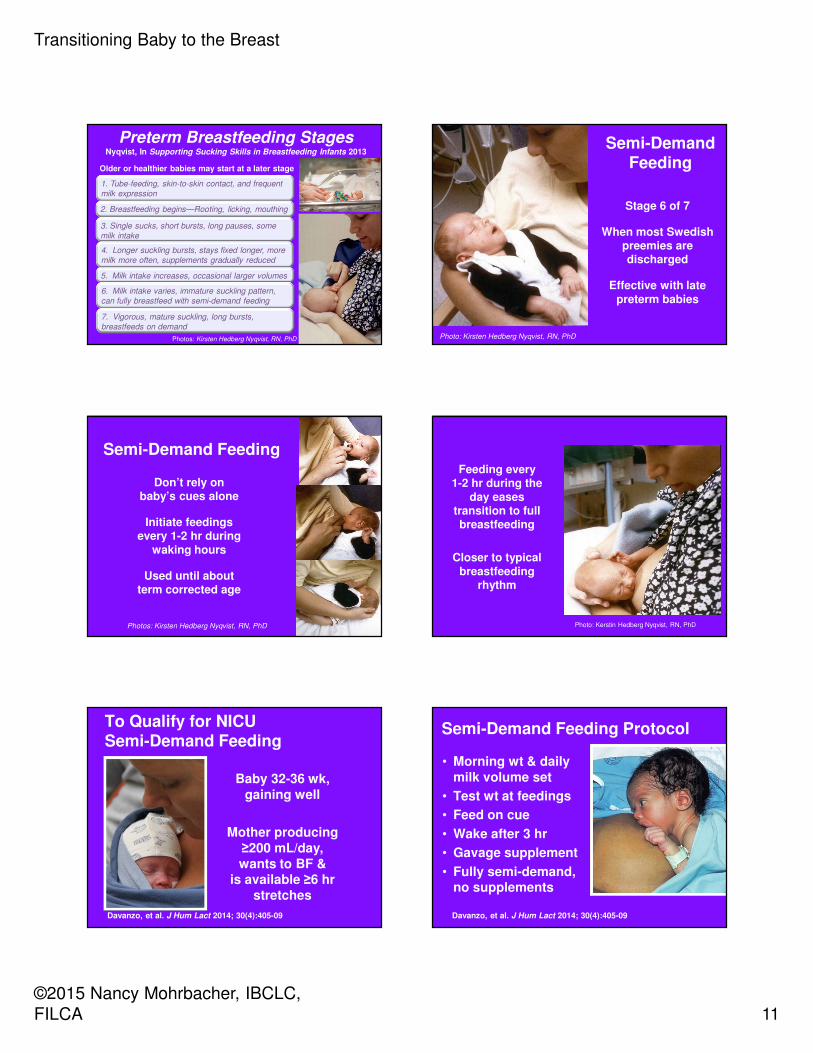
Preterm Breastfeeding StagesNyqvist, In Supporting Sucking Skills in Breastfeeding Infants 2013
1. Tube-feeding, skin-to-skin contact, and frequent
milk expression
2. Breastfeeding begins—Rooting, licking, mouthing
3. Single sucks, short bursts, long pauses, some
milk intake
4. Longer suckling bursts, stays fixed longer, more
milk more often, supplements gradually reduced
5. Milk intake increases, occasional larger volumes
6. Milk intake varies, immature suckling pattern,
can fully breastfeed with semi-demand feeding
7. Vigorous, mature suckling, long bursts,
breastfeeds on demand
Photos: Kirsten Hedberg Nyqvist, RN, PhD
Older or healthier babies may start at a later stage
Semi-Demand Feeding
Stage 6 of 7
When most Swedish preemies are discharged
Effective with late preterm babies
Photo: Kirsten Hedberg Nyqvist, RN, PhD
Semi-Demand Feeding
Don’t rely on baby’s cues alone
Initiate feedings every 1-2 hr during
waking hours
Used until about term corrected age
Photos: Kirsten Hedberg Nyqvist, RN, PhD
Feeding every 1-2 hr during the
day eases transition to full breastfeeding
Closer to typical breastfeeding
rhythm
Photo: Kerstin Hedberg Nyqvist, RN, PhD
To Qualify for NICU Semi-Demand Feeding
Baby 32-36 wk, gaining well
Mother producing ≥200 mL/day, wants to BF &
is available ≥6 hr stretches
Davanzo, et al. J Hum Lact 2014; 30(4):405-09
Semi-Demand Feeding Protocol
• Morning wt & daily milk volume set
• Test wt at feedings
• Feed on cue
• Wake after 3 hr
• Gavage supplement
• Fully semi-demand, no supplements
Davanzo, et al. J Hum Lact 2014; 30(4):405-09
Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 12
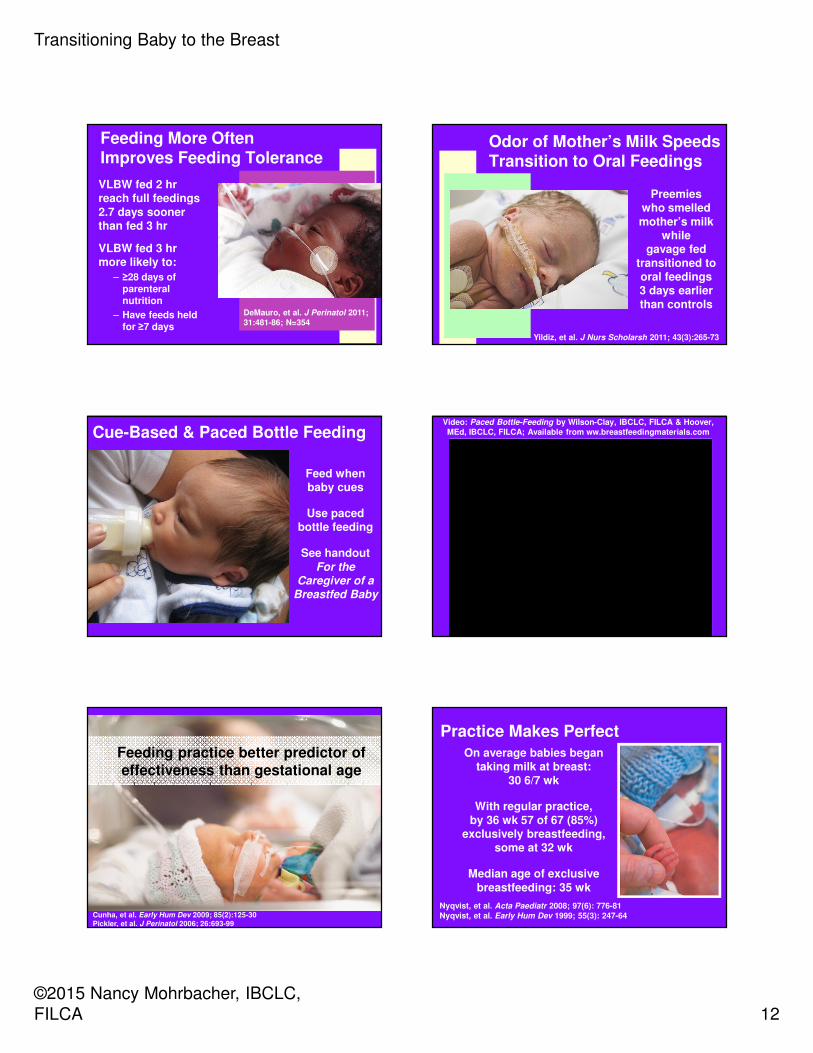
Feeding More Often Improves Feeding Tolerance
VLBW fed 2 hr reach full feedings 2.7 days sooner than fed 3 hr
VLBW fed 3 hr more likely to:
– ≥28 days of parenteral nutrition
– Have feeds held for ≥7 days
DeMauro, et al. J Perinatol 2011; 31:481-86; N=354
Odor of Mother’s Milk Speeds Transition to Oral Feedings
Preemies who smelled mother’s milk
while gavage fed
transitioned to oral feedings 3 days earlier than controls
Yildiz, et al. J Nurs Scholarsh 2011; 43(3):265-73
Cue-Based & Paced Bottle Feeding
Feed when baby cues
Use paced bottle feeding
See handout For the
Caregiver of a Breastfed Baby
Video: Paced Bottle-Feeding by Wilson-Clay, IBCLC, FILCA & Hoover, MEd, IBCLC, FILCA; Available from ww.breastfeedingmaterials.com
Feeding practice better predictor of effectiveness than gestational age
Cunha, et al. Early Hum Dev 2009; 85(2):125-30 Pickler, et al. J Perinatol 2006; 26:693-99
Practice Makes PerfectOn average babies began
taking milk at breast: 30 6/7 wk
With regular practice, by 36 wk 57 of 67 (85%)
exclusively breastfeeding, some at 32 wk
Median age of exclusive breastfeeding: 35 wk
Nyqvist, et al. Acta Paediatr 2008; 97(6): 776-81Nyqvist, et al. Early Hum Dev 1999; 55(3): 247-64
Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 13
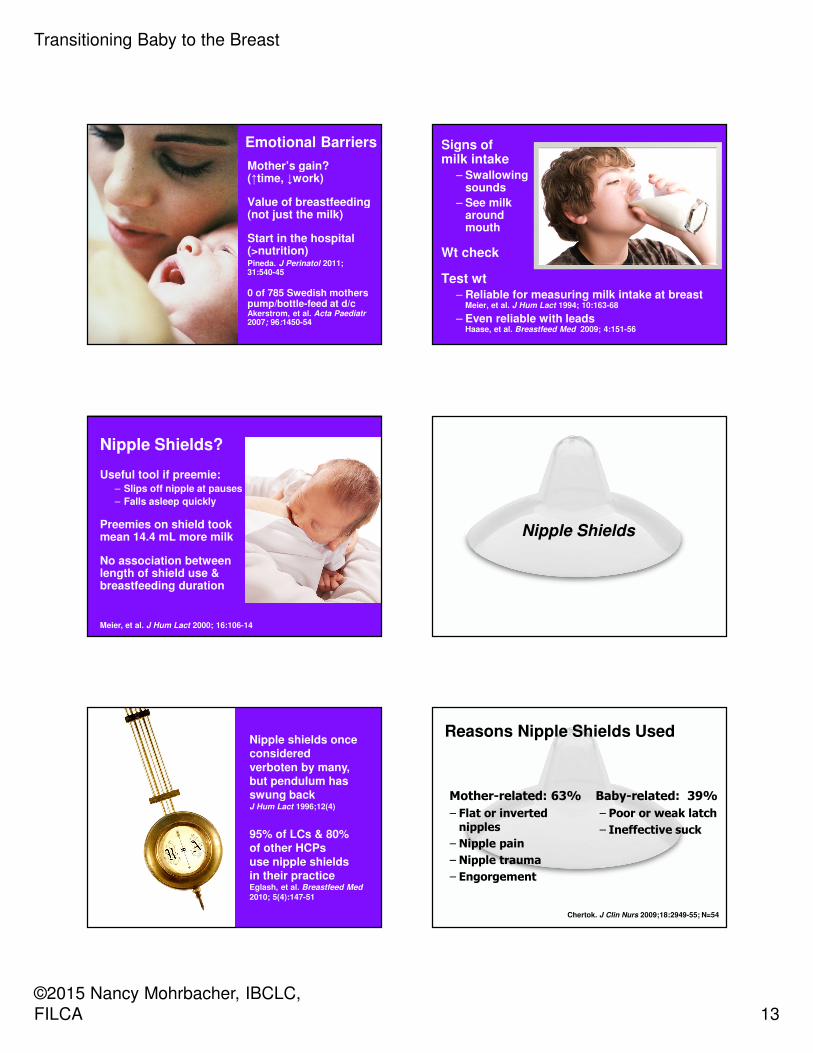
Emotional Barriers
Mother’s gain? (↑time, ↓work)
Value of breastfeeding (not just the milk)
Start in the hospital (>nutrition)Pineda. J Perinatol 2011; 31:540-45
0 of 785 Swedish mothers pump/bottle-feed at d/cAkerstrom, et al. Acta Paediatr2007; 96:1450-54
Signs of milk intake
– Swallowing sounds
– See milk around mouth
Wt check
Test wt– Reliable for measuring milk intake at breast
Meier, et al. J Hum Lact 1994; 10:163-68
– Even reliable with leads Haase, et al. Breastfeed Med 2009; 4:151-56
Nipple Shields?
Useful tool if preemie:– Slips off nipple at pauses
– Falls asleep quickly
Preemies on shield took mean 14.4 mL more milk
No association between length of shield use & breastfeeding duration
Meier, et al. J Hum Lact 2000; 16:106-14
Nipple Shields
Nipple shields once considered verboten by many, but pendulum has swung back J Hum Lact 1996;12(4)
95% of LCs & 80% of other HCPs use nipple shields in their practiceEglash, et al. Breastfeed Med
2010; 5(4):147-51
Reasons Nipple Shields Used
Mother-related: 63%
– Flat or inverted nipples
– Nipple pain
– Nipple trauma
– Engorgement
Baby-related: 39%
– Poor or weak latch
– Ineffective suck
Chertok. J Clin Nurs 2009;18:2949-55; N=54
Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 14
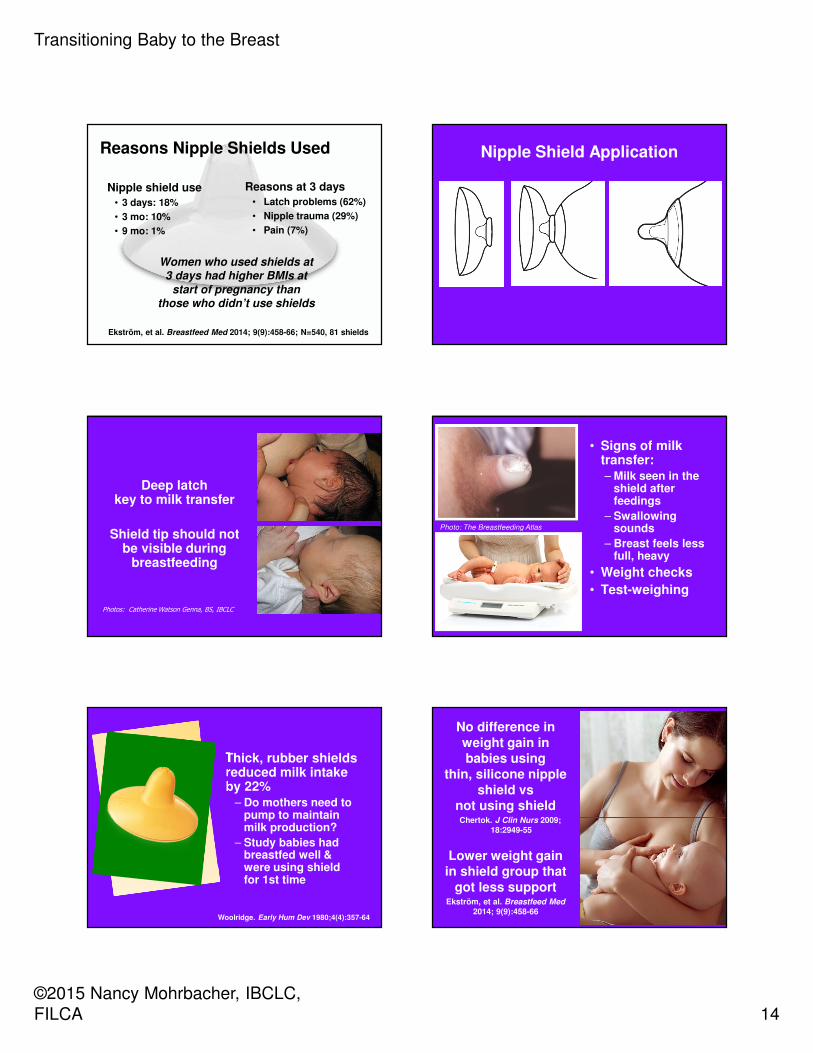
Reasons Nipple Shields Used
Ekström, et al. Breastfeed Med 2014; 9(9):458-66; N=540, 81 shields
Reasons at 3 days
• Latch problems (62%)
• Nipple trauma (29%)
• Pain (7%)
Nipple shield use
• 3 days: 18%
• 3 mo: 10%
• 9 mo: 1%
Women who used shields at 3 days had higher BMIs at
start of pregnancy than those who didn’t use shields
Nipple Shield Application
Deep latch key to milk transfer
Shield tip should not be visible during
breastfeeding
Photos: Catherine Watson Genna, BS, IBCLC
• Signs of milk transfer:– Milk seen in the
shield after feedings
– Swallowing sounds
– Breast feels less full, heavy
• Weight checks
• Test-weighing
Photo: The Breastfeeding Atlas
Thick, rubber shields reduced milk intake by 22%
– Do mothers need to pump to maintain milk production?
– Study babies had breastfed well & were using shield for 1st time
Woolridge. Early Hum Dev 1980;4(4):357-64
No difference in weight gain in babies using
thin, silicone nipple shield vs
not using shield Chertok. J Clin Nurs 2009;
18:2949-55
Lower weight gain in shield group that
got less supportEkström, et al. Breastfeed Med
2014; 9(9):458-66
Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 15
Weaning from a Nipple Shield
• Start with shield on
• When swallowing, slip off shield, slip in breast
• If not, try again at a relaxed time
• Not every day
Cutting the shield no longer
recommended
Was safe with latex shields
With silicone shields, creates
sharp edges
• 67% eventually weaned from shield
• 33% used it throughout
– 11% could have nursed without it
– Continued using it for greater comfort
Powers, et al. J Hum Lact 2004;20(3):327-34; N=202
Priorities
1. Feed the baby
2. Protect mother’s milk production
3. Support baby’s transition to breast
• Is it a fitness issue?
• Use feel, flow & familiarity to help baby take the breast
When the basics don’t work, think “Four Fs”
Target tools & strategies to the problem’s cause

Transitioning Baby to the Breast
©2015 Nancy Mohrbacher, IBCLC,
FILCA 16
Babies are hardwired to breastfeed
Choose strategies that make
the most of baby’s hardwiring
www.NancyMohrbacher.com Facebook.com/NancyMohrbacherIBCLC
Pinterest.com/nancymohrbacher@BFReporter
www.YouTube.com/NancyMohrbacher
~