transesophageal echocardiographic guidance of transcatheter closure of atrial septal defect
TRANSCRIPT

CONGENITAL HEART DISEASE
Transesophageal Echocardiographic Guidanceof Transcatheter Closure of Atrial Septal Defect
William E. Hellenbrand, MD, JohnT. Fahey, MD, Francis X. McGowan, MD,Gregory G. Weltin, MD, and Charles S. Kleinman, MD
Transcatheter closure of atrial septal defect (ASD)was accomplished in 10 of 11 patients aged 13months to 46 years (weight range 11 to 77 kg).Transesophageal echocardiography (TEE) wasused simultaneously with fluoroscopic imaging in 4of these patients aged 4.5 to 46 years (weightrange 19 to 77 kg). TEE was used to ascertain defect size, position and number of defects and to ascertain appropriate seating of the defect occluderwithin the atrial defect. In 2 patients TEE-assistedtranscatheter ASD closure was accomplished afterprevious attempts at transcatheter ASD closure,unaided by TEE, had been unsuccessful. The onlyunsucc:euful ASD closure procedure occurred inthe smallest patient in the series (an U-kg 13month-old), a child who was too small to undergoTEE using our ll-mm diameter endoscopic probe.The concomitant use of TEE with fluoroscopic imaging provides information that is unique and completnentary and may improve the efficacy and safety of the transcatheter technique for ASD closure.The recent availability of a 7-mm diameter TEEprobe will extend the use of TEE into the infant agegroup and may decrease the discomfort and potential morbidity of TEE in olderpatients.
(Am J Cardioll990;66:207-213)
From the Departments of Pediatrics, Diagnostic Imaging and Anesthesiology, Yale University School of Medicine, New Haven, Connecticut.Manuscript received December 22, 1989; revised manuscript receivedand accepted March 6, 1990.
Address for reprints: William E. Hellenbrand, MD, Yale University School of Medicine, Section of Pediatric Cardiology, 333 CedarStreet, New Haven, Connecticut 06510.
Transcatheter therapy for many different types ofcongenital heart disease has been well describedover the past 8 years.l'? Recently, a double um
brella with a clamshell configuration was developed fortranscatheter closure of atrial septal defect (ASD) allowing spring tension rather than hooks or lockingscrews to attach the umbrella to the atrial septum. II Inthe present study, the technique for double umbrellaclosure of ASD in children and adults as recently described by Lock et al12,13 was used. This technique relied on fluoroscopic imaging alone to place the device.
The relatively recent development of transesophageal echocardiography (TEE) imaging tranducers interfaced with steerable endoscopes has altered the natureof echocardiography. These "semiinvasive" studies provide high-quality tomographic images of the heart andgreat vessels, unaffected by superimposed lung tissueand body habitus. The use of TEE during cardiac surgery, in the intensive care unit and in outpatients,in whom precordial echocardiographic studies havebeen inadequate for diagnostic purposes, has beenwell described.I'
This report describes the combined application ofTEE and fluoroscopic imaging for monitoring the transcatheter closure of ostium secundum ASD. These 2 imaging modalities, used simultaneously, are complementary and represent a unique approach. We believe thatTEE provides information that makes this interventional catheterization procedure easier, safer and more effective than using fluoroscopic guidance alone.
METHODSStudy patients: Between March 1 and October 31,
1989, 11 patients, aged 1 to 46 years (median 4.6),ranging in weight from 11 to 77 kg (median 19.3) haveundergone attempted transcatheter closure of ASDs atthe Yale-New Haven Medical Center (Table I). Theseprocedures were performed under a protocol for humaninvestigation approved by our institutional review boardas part of a multicenter study using an investigationaldevice being evaluated under the approval of the Foodand Drug Administration (IDE approved).
Four of these patients, ranging in age from 45 to 46years and in weight from 19 to 77 kg, underwent TEEmonitoring and guidance of placement of the atrial defect occluder device.
In 3 pediatric patients, ranging from 4.5 to 11 yearsof age, the procedure was performed under general an-
THE AMERICAN JOURNAL OFCARDIOLOGY JULY 15, 1990 207
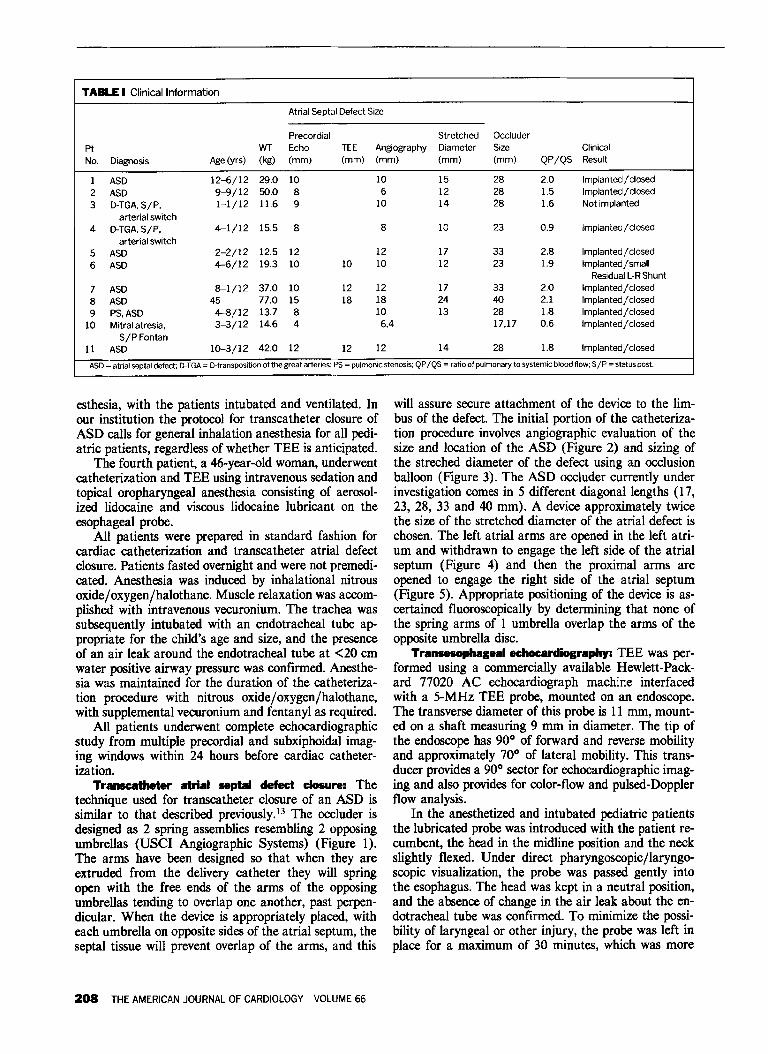
TABLE I Clinical Information
Atrial Septal Defect Size
Precordial Stretched OccluderPt WT Echo TEE Angiography Diameter Size ClinicalNo. Diagnosis Age(yrs) (kg) (mm) (mm) (mm) (mm) (mm) QP/QS Result
1 ASD 12-6/12 29.0 10 10 15 28 2.0 Implanted / closed2 ASD 9-9/12 50.0 8 6 12 28 1.5 Implanted / closed3 D-TGA,S/P. 1-1/12 11.6 9 10 14 28 1.6 Not implanted
arterial switch4 D-TGA,S/P. 4--1/12 15.5 8 8 10 23 0.9 Implanted/closed
arterial switch5 ASD 2-2/12 12.5 12 12 17 33 2.8 Implanted / closed6 ASD 4-6/12 19.3 10 10 10 12 23 1.9 Implanted/small
ResidualL-RShunt7 ASD 8-1/12 37.0 10 12 12 17 33 2.0 Implanted/closed8 ASD 45 77.0 15 18 18 24 40 2.1 Implanted / closed9 PS,ASD 4--8/12 13.7 8 10 13 28 1.8 Implanted/closed
10 Mitral atresia, 3-3/12 14.6 4 6,4 17,17 0.6 Implanted/closedSIP Fontan
11 ASD 10-3/12 42.0 12 12 12 14 28 1.8 Implanted / closed
ASD = atrial septal defect; D-TGA - D-transposition ofthe great arteries; PS - pulmoruc stenosis; QP/QS - ratio of pulmonary to systemic blood flow; S/P - status post.
esthesia, with the patients intubated and ventilated. Inour institution the protocol for transcatheter closure ofASD calls for general inhalation anesthesia for all pediatric patients, regardless of whether TEE is anticipated.
The fourth patient, a 46-year-old woman, underwentcatheterization and TEE using intravenous sedation andtopical oropharyngeal anesthesia consisting of aerosolized lidocaine and viscous lidocaine lubricant on theesophageal probe.
All patients were prepared in standard fashion forcardiac catheterization and transcatheter atrial defectclosure. Patients fasted overnight and were not premedicated. Anesthesia was induced by inhalational nitrousoxide/oxygen/halothane. Muscle relaxation was accomplished with intravenous vecuronium. The trachea wassubsequently intubated with an endotracheal tube appropriate for the child's age and size, and the presenceof an air leak around the endotracheal tube at <20 emwater positive airway pressure was confirmed. Anesthesia was maintained for the duration of the catheterization procedure with nitrous oxide/oxygen/halothane,with supplemental vecuronium and fentanyl as required.
All patients underwent complete echocardiographicstudy from multiple precordial and subxiphoidal imaging windows within 24 hours before cardiac catheterization.
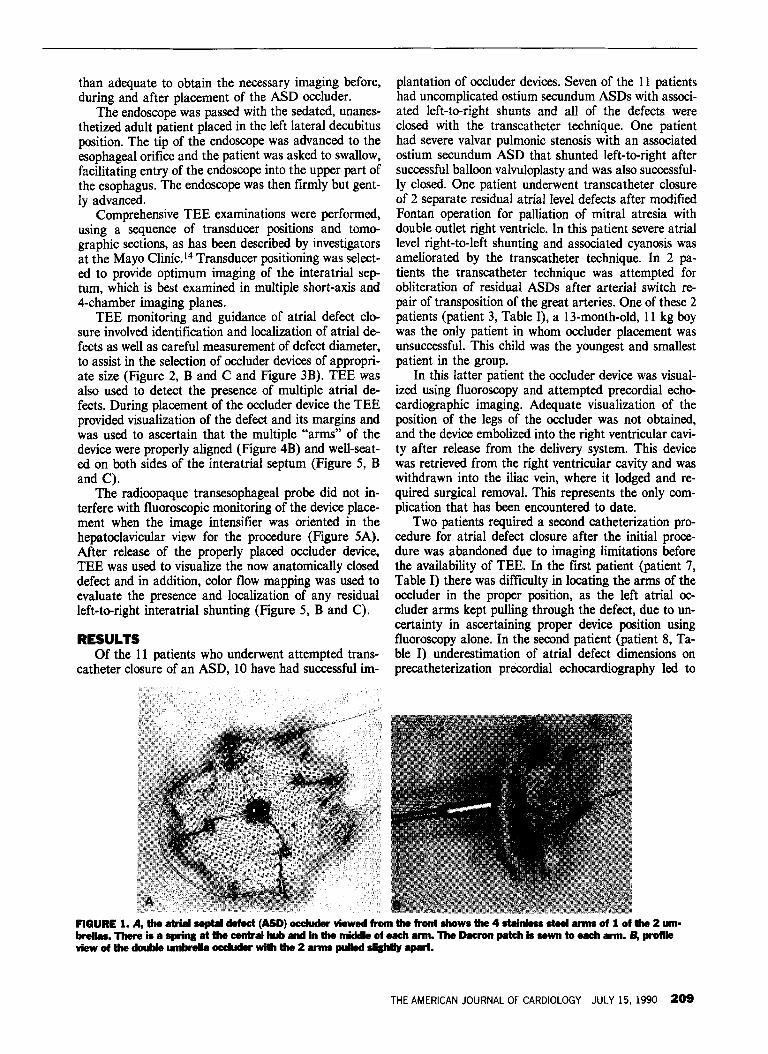
Transcatheter atrial septal defect closure: Thetechnique used for transcatheter closure of an ASD issimilar to that described previously.P The occluder isdesigned as 2 spring assemblies resembling 2 opposingumbrellas (USCI Angiographic Systems) (Figure 1).The arms have been designed so that when they areextruded from the delivery catheter they will springopen with the free ends of the arms of the opposingumbrellas tending to overlap one another, past perpendicular. When the device is appropriately placed, witheach umbrella on opposite sides of the atrial septum, theseptal tissue will prevent overlap of the arms, and this
208 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 66
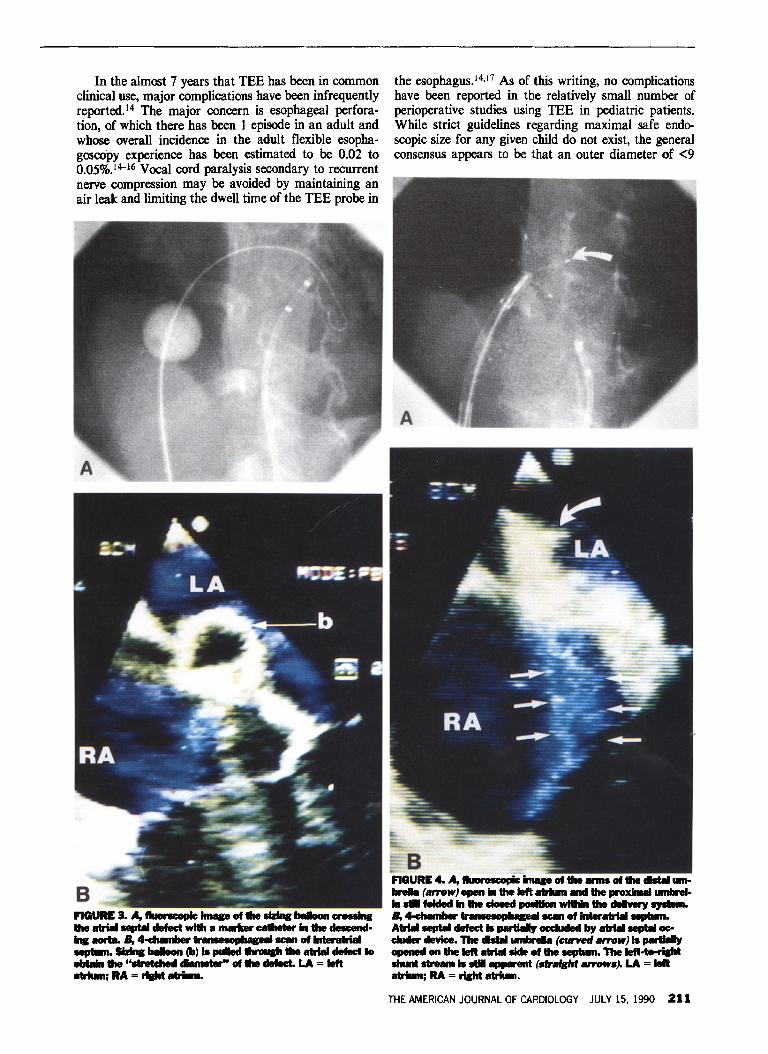
will assure secure attachment of the device to the limbus of the defect. The initial portion of the catheterization procedure involves angiographic evaluation of thesize and location of the ASD (Figure 2) and sizing ofthe streched diameter of the defect using an occlusionballoon (Figure 3). The ASD occluder currently underinvestigation comes in 5 different diagonal lengths (17,23, 28, 33 and 40 mm). A device approximately twicethe size of the stretched diameter of the atrial defect ischosen. The left atrial arms are opened in the left atrium and withdrawn to engage the left side of the atrialseptum (Figure 4) and then the proximal arms areopened to engage the right side of the atrial septum(Figure 5). Appropriate positioning of the device is ascertained fluoroscopically by determining that none ofthe spring arms of 1 umbrella overlap the arms of theopposite umbrella disc.
Transesophageal echocardiography: TEE was performed using a commercially available Hewlett-Packard 77020 AC echocardiograph machine interfacedwith a 5-MHz TEE probe, mounted on an endoscope.The transverse diameter of this probe is 11 mm, mounted on a shaft measuring 9 mm in diameter. The tip ofthe endoscope has 90° of forward and reverse mobilityand approximately 70° of lateral mobility. This transducer providesa 90° sector for echocardiographic imaging and also provides for color-flow and pulsed-Dopplerflow analysis.
In the anesthetized and intubated pediatric patientsthe lubricated probe was introduced with the patient recumbent, the head in the midline position and the neckslightly flexed. Under direct pharyngoscopicjlaryngoscopic visualization, the probe was passed gently intothe esophagus. The head was kept in a neutral position,and the absence of change in the air leak about the endotracheal tube was confirmed. To minimize the possibility of laryngeal or other injury, the probe was left inplace for a maximum of 30 minutes, which was more
than adequate to obtain the necessary imaging before,during and after placement of the ASD occluder.
The endoscope was passed with the sedated, unanesthetized adult patient placed in the left lateral decubitusposition. The tip of the endoscope was advanced to theesophageal orifice and the patient was asked to swallow,facilitating entry of the endoscope into the upper part ofthe esophagus. The endoscope was then firmly but gently advanced.
Comprehensive TEE examinations were performed,using a sequence of transducer positions and tomographic sections, as has been described by investigatorsat the Mayo Clinic." Transducer positioning was selected to provide optimum imaging of the interatrial septum, which is best examined in multiple short-axis and4-chamber imaging planes.
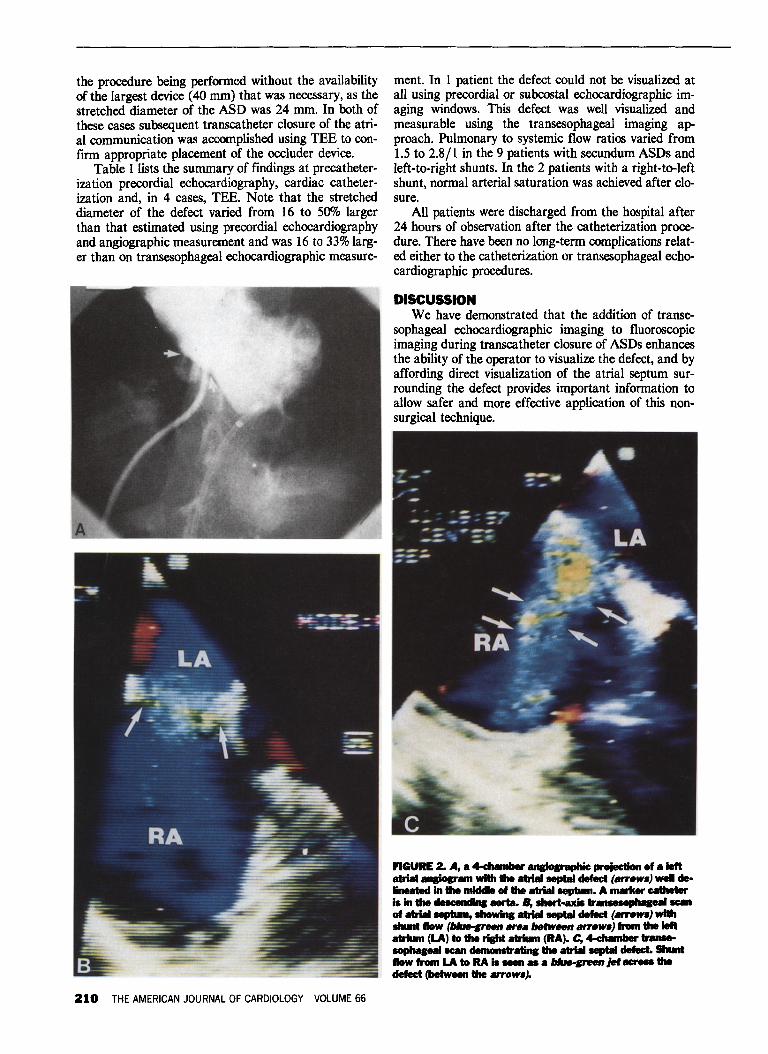
TEE monitoring and guidance of atrial defect closure involved identification and localization of atrial defects as well as careful measurement of defect diameter,to assist in the selection of occluder devices of appropriate size (Figure 2, Band C and Figure 3B). TEE wasalso used to detect the presence of multiple atrial defects. During placement of the occluder device the TEEprovided visualization of the defect and its margins andwas used to ascertain that the multiple "arms" of thedevice were properly aligned (Figure 4B) and well-seated on both sides of the interatrial septum (Figure 5, Band C).
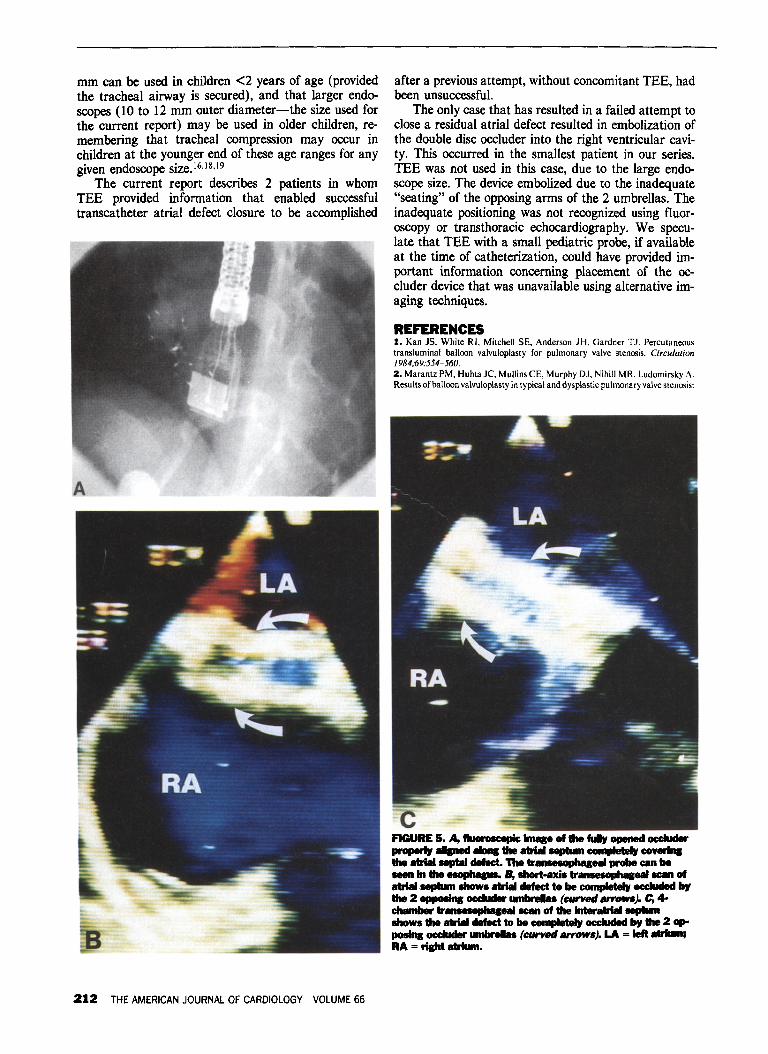
The radioopaque transesophageal probe did not interfere with fluoroscopic monitoring of the device placement when the image intensifier was oriented in thehepatoclavicular view for the procedure (Figure SA).After release of the properly placed occluder device,TEE was used to visualize the now anatomically closeddefect and in addition, color flow mapping was used toevaluate the presence and localization of any residualleft-to-right interatrial shunting (Figure 5, B and C).
RESULTSOf the 11 patients who underwent attempted trans
catheter closure of an ASD, 10 have had successful im-
plantation of occluder devices. Seven of the 11 patientshad uncomplicated ostium secundum ASDs with associated left-to-right shunts and all of the defects wereclosed with the transcatheter technique. One patienthad severe valvar pulmonic stenosis with an associatedostium secundum ASD that shunted left-to-right aftersuccessful balloon valvuloplasty and was also successfully closed. One patient underwent transcatheter closureof 2 separate residual atrial level defects after modifiedFontan operation for palliation of mitral atresia withdouble outlet right ventricle. In this patient severe atriallevel right-to-left shunting and associated cyanosis wasameliorated by the transcatheter technique. In 2 patients the transcatheter technique was attempted forobliteration of residual ASDs after arterial switch repair of transposition of the great arteries. One of these 2patients (patient 3, Table I), a 13-month-old, 11 kg boywas the only patient in whom occluder placement wasunsuccessful. This child was the youngest and smallestpatient in the group.
In this latter patient the occluder device was visualized using fluoroscopy and attempted precordial echocardiographic imaging. Adequate visualization of theposition of the legs of the occluder was not obtained,and the device embolized into the right ventricular cavity after release from the delivery system. This devicewas retrieved from the right ventricular cavity and waswithdrawn into the iliac vein, where it lodged and required surgical removal. This represents the only complication that has been encountered to date.
Two patients required a second catheterization procedure for atrial defect closure after the initial procedure was abandoned due to imaging limitations beforethe availability of TEE. In the first patient (patient 7,Table I) there was difficulty in locating the arms of theoccluder in the proper position, as the left atrial DC
cluder arms kept pulling through the defect, due to uncertainty in ascertaining proper device position usingfluoroscopy alone. In the second patient (patient 8, Table I) underestimation of atrial defect dimensions onprecatheterization precordial echocardiography led to
FIGURE I. A, the atrial septal defect (ASD) occIuder viewed fnIm the front shows the 4 stainless steel anns of 1 of the 2 .....brelas. There is a spring at the central huband in the mickIe of eachann. T11e Dacron patch is sewn to eachann. B, profileview of the double ....breIa ocduderwith the 2 anns pulled sIiIhtIJ apart.
THE AMERICAN JOURNAL OF CARDIOLOGY JULY 15, 1990 209
the procedure being performed without the availabilityof the largest device (40 mm) that was necessary, as thestretched diameter of the ASD was 24 mm. In both ofthese cases subsequent transcatheter closure of the atrial communication was accomplished using TEE to confirm appropriate placement of the occluder device.
Table I lists the summary of findings at precatheterization precordial echocardiography, cardiac catheterization and, in 4 cases, TEE. Note that the stretcheddiameter of the defect varied from 16 to 500/0 largerthan that estimated using precordial echocardiographyand angiographic measurement and was 16 to 33%larger than on transesophageal echocardiographic measure-
210 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 66
ment. In 1 patient the defect could not be visualized atall using precordial or subcostal echocardiographic imaging windows. This defect was well visualized andmeasurable using the transesophageal imaging approach. Pulmonary to systemic flow ratios varied from1.5 to 2.8/1 in the 9 patients with secundum ASDs andleft-to-right shunts. In the 2 patients with a right-to-leftshunt, normal arterial saturation was achieved after closure.
All patients were discharged from the hospital after24 hours of observation after the catheterization procedure. There have been no long-term complicationsrelated either to the catheterization or transesophageal echocardiographic procedures.
DISCUSSIONWe have demonstrated that the addition of transe
sophageal echocardiographic imaging to fluoroscopicimaging during transcatheter closure of ASDs enhancesthe ability of the operator to visualize the defect, and byaffording direct visualization of the atrial septum surrounding the defect provides important information toallow safer and more effective application of this nonsurgical technique.
FIGURE 2. A, a 4-chamberancIo&raphic projection of a leftatrial anPIIram with the atrial septal defect (aITOWI) wei de·Iineated In the midlIe of the atrial septum. A marker catheteris in the deleellell..s aorta. B, short-axil ................ scanof atriaIlNlPlum, IhowIn8 atrial septal defect (atTOWI) willi...... flow (blw-green area between aITOWI) from the leftatrium (LA) to the right atrium (RA). C, 4-ehamber .............eaIscan demoIlIIratins the atrial septal defect. Shuntflow from LA to RA is ..... _ a blue-green Jetacross thedefect (between the .aITOWlj.
In the almost 7 years that TEE has been in commonclinical use, major complications have been infrequentlyreported." The major concern is esophageal perforation, of which there has been 1 episode in an adult andwhose overall incidence in the adult flexible esophagoscopy experience has been estimated to be 0.02 to0.05%.14--16 Vocal cord paralysis secondary to recurrentnerve compression may be avoided by maintaining anair leak and limiting the dwell time of the TEE probe in
FIGURE 3. A, fIuoncopIc of IIzIncINIIoon CI'OSIinI... atrW sept8I defect with C8Iheter In deIcend-... eorta. B, 4-eh8mber tr seen of ................-n 1NIIoon (b) Is puled defect toGbI8In "sb etched cI8meter" of defect. LA = leftetrIunIj RA =......1Itrium.
the esophagus.14,17 As of this writing, no complicationshave been reported in the relatively small number ofperioperative studies using TEE in pediatric patients.While strict guidelines regarding maximal safe endoscopic size for any given child do not exist, the generalconsensus appears to be that an outer diameter of <9
FIGURE 4. A, tIuoI oscepic .... of ....... of ... cht8I um....... (arrow) open in the left 8IrIum end the proxinull umbreIIe .. folded In the doled ..... wiIhin Ihe deIvery aydIm.B,~ tr.....upIupeI seen of inter .AIrilII sept8I defect Is pertIeIy occluded by sIrilII oc-duder device. The ...... umbreII8 (f:UrVed arrow) is~opened on the left atrW..of the ....-n. The Ieft-to-rilhlIhunt ......... Is ... .....-em (.sIght IIrrOWSj. LA = leftetrIum; RA = riIht atrium.
THE AMERICAN JOURNAL OF CARDIOLOGY JULY 15, 1990 211
mm can be used in children <2 years of age (providedthe tracheal airway is secured), and that larger endoscopes (10 to 12 mm outer diameter-the size used forthe current report) may be used in older children, remembering that tracheal compression may occur inchildren at the younger end of these age ranges for anygiven endoscope size.16,J8,19
The current report describes 2 patients in whomTEE provided information that enabled successfultranscatheter atrial defect closure to be accomplished
212 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 66
after a previous attempt, without concomitant TEE, hadbeen unsuccessful.
The only case that has resulted in a failed attempt toclose a residual atrial defect resulted in embolization ofthe double disc occluder into the right ventricular cavity. This occurred in the smallest patient in our series.TEE was not used in this case, due to the large endoscope size. The device embolized due to the inadequate"seating" of the opposing arms of the 2 umbrellas. Theinadequate positioning was not recognized using fluoroscopy or transthoracic echocardiography. We speculate that TEE with a small pediatric probe, if availableat the time of catheterization, could have provided important information concerning placement of the occluder device that was unavailable using alternative imaging techniques.
REFERENCES1. Kan J5, White RI. Mitchell 5E, Anderson JH, Gardner TJ. Percutaneoustransluminal balloon valvuloplasty for pulmonary valve stenosis. Circulation1984;69:554-560.2. Marantz PM, Huhta JC, Mullins CE, Murphy DJ, Nihill MR, Ludornirsky A.Results of balloon valvuloplasty in typical and dysplastic pulmonary valve stenosis:
FIGURE 5. A, tIuoroscapic lm8ge of the fuIy opened occIuderproperIr ............. the atrial septum cempIeteIr coverInathe atrial septal defect. The tr.....ophq'" ..... can be.... in the 8, short·axi. tranIeIophaJealllC8I'I ofatrial septum W. atrial defect to be compIeteIr occluded bythe 2 opposIns occIuderumbreIaI (euned ."...). Co ...chamber ........OPo....... scan of the Intwatrial .............w. the atrial defect to be completely occluded It, the 2 op........ occIuder umbreIIu (curved ."..w.j. LA = left ........;RA = ri&ht atrium.

Doppler echocardiographic follow-up. JACC 1988;12:476-491.3. Rao PS. Balloon pulmonary valvuloplasty: a review. Clinical Cardiology1989;/2:55-74.4. Choy M, Beekman RH, Rocchini AP, Crowley DC, Snider AR, Dick M,Rosenthal A. Percutaneous balloon valvuloplasty for valvar aortic stenosis ininfants and children. Am J Cardiol /987;59:/010-1013.5. Lababidi Z, Wu J, Walls JT. Percutaneous balloon aortic valvuloplasty: resultsin 23 patients. Am J Cardiol /984;53:/94-197.6. Beekman RH, Rocchini AP, Dick M, Snider AR, Crowley DC, Serwer GA,Spicer RL, Rosenthal A. Percutaneous balloon angioplasty for native coarctationof the aorta. lACe 198UO:J078-/084.7. Delezo lS, Sancho M, Pan M, Romero M, Olivera C, Luque M. Angiographicfollow-up after balloon angioplasty for coarctation of the aorta. 1ACC1989;13:689-695.8. Kan JS, White RI, Mitchell SE, Farmlett EJ, Donahoo rs, Gardner TJ.Treatment of restenosis of coarctation by transluminal angioplasty. Circulation1983;68:/087-/094.9. Rashkind WJ, Mullins CE, Hellenbrand WE, Tait MA. Nonsurgical closure ofpatent ductus arteriosus: clinical application of the Rashkind PDA occluder system. Circulation /987;75:583-592.10. Hellenbrand WE, Mullins CEoCatheter closure of congenital cardiac defects.Cardiol Clinics /989;7:35/-368.11. LockJE, Rome JJ, Davis R, Van Praagh S, PerrySB, Van Praagh R, KeaneIF. Transcatheter closure of atrial septal defects: experimental studies. Circulation /989;79:/09/-/099.12. Lock JE, Hellenbrand WE, Latson L, Mullins CE, Benson L, Rome JJ.Clamshell umbrella closure of atrial septal defects: initial experience (abstr).
Circulation 1989;80://-592.13. Rome JJ, Keane JF, Perry SB, Spevak PJ, Lock lE. Double umbrella closureof atrial defects: initial clinical applications. Circulation, in press.14. Seward lB, Khandheria BK, Oh lK,Abel MD, Hughes RW, Edwards WD,Nichols BA, Freeman WK, Tajik AJ. Transesophageal echocardiography: technique, anatomic correlations, implementations and clinical applications. Mayocu« Proc 1988;63:649-680.15. Dawson J, Cockel R. Oesophageal perforation at fiberoptic gastroscopy. DrMed 1 198/;283:583-587.16. Byrne WJ. Endoscopy in the diagnosis and treatment of disorders in theproximal gastrointestinal tract. Gastrointest Res 1989;/5:14-26.17. Cucchiara RF, Nugent M, Seward JB, Messick J M_Air embolism in uprightneurosurgical patients: detection and localization by two-dimensional transesophageal echocardiography. Anesthesiology 1984;60:353~355_
18. Caulfield M, Wyllie R, Sivak M, Michener W, Steffen R. Upper intestinaltract endoscopy in the pediatric patient. 1 Pediatr /989;1 I5:339-345.19. Ament ME, Berquist WE, Vargas J, Perisic V. Fiberoptic upper intestinalendoscopy in infants and children. Pediatr Clin North Am 1988;35:/41-/55.
Addendum: Since submission of this article, patientnumber 3 (Table I) has undergone successful transcatheter closure of the ASD with a 33-mm device at 2 yearsof age using TEE.
THE AMERICAN JOURNAL OFCARDIOLOGY JULY 15.1990 213