training for fluoroscopic peritoneal dialysis catheter ...€¦ · record success of catheter...
TRANSCRIPT
Training for FluoroscopicPeritoneal Dialysis Catheter
Placement
Rajeev Narayan MD
San Antonio Kidney Disease Center
San Antonio, TX

Disclosures
No financial conflicts of interest to disclose.
My comments apply primarily to Nephrologists
Introduction:
1.Why should we promote percutaneous PD catheterplacement, especially amongst Nephrologists?
2.Training requirements and expected outcomes forcertification and for a successful program
3.Suggestions for trainees starting PD insertion (Opinion)
4.Suggestions for trainers to improve success and outcomes(Opinion)
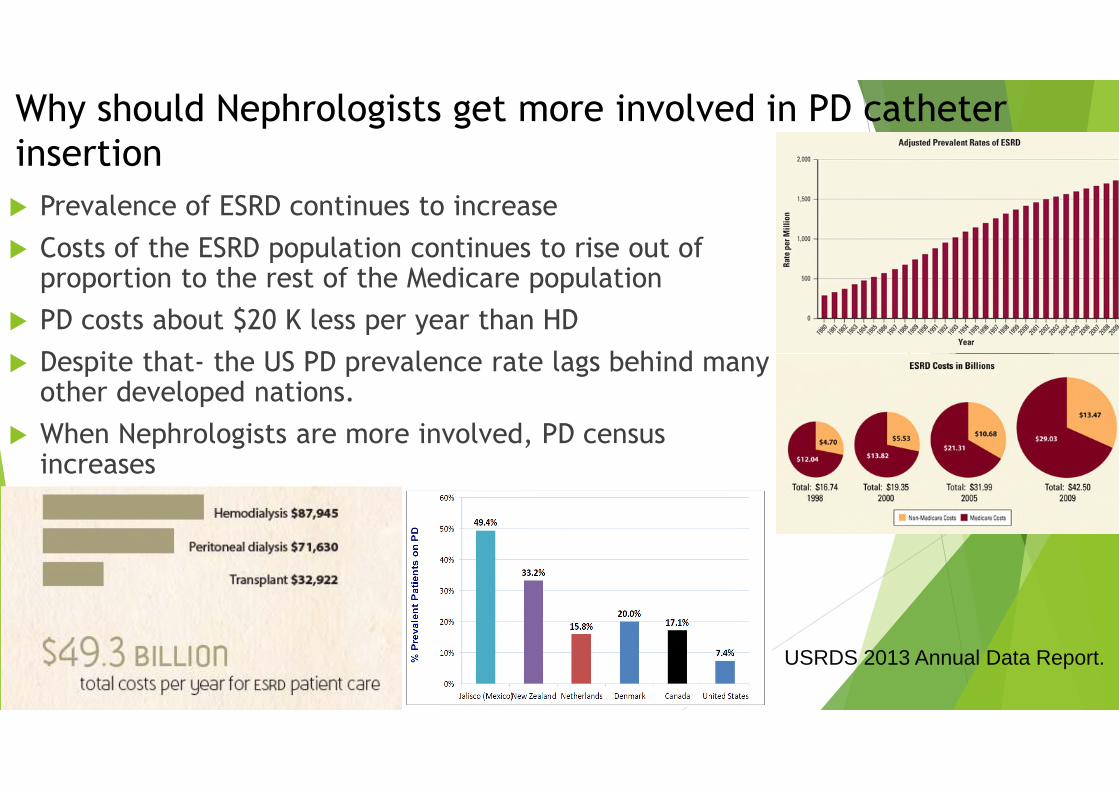
USRDS 2013 Annual Data Report.
Prevalence of ESRD continues to increase
Costs of the ESRD population continues to rise out ofproportion to the rest of the Medicare population
PD costs about $20 K less per year than HD
Despite that- the US PD prevalence rate lags behind manyother developed nations.
When Nephrologists are more involved, PD censusincreases
Why should Nephrologists get more involved in PD catheterinsertion
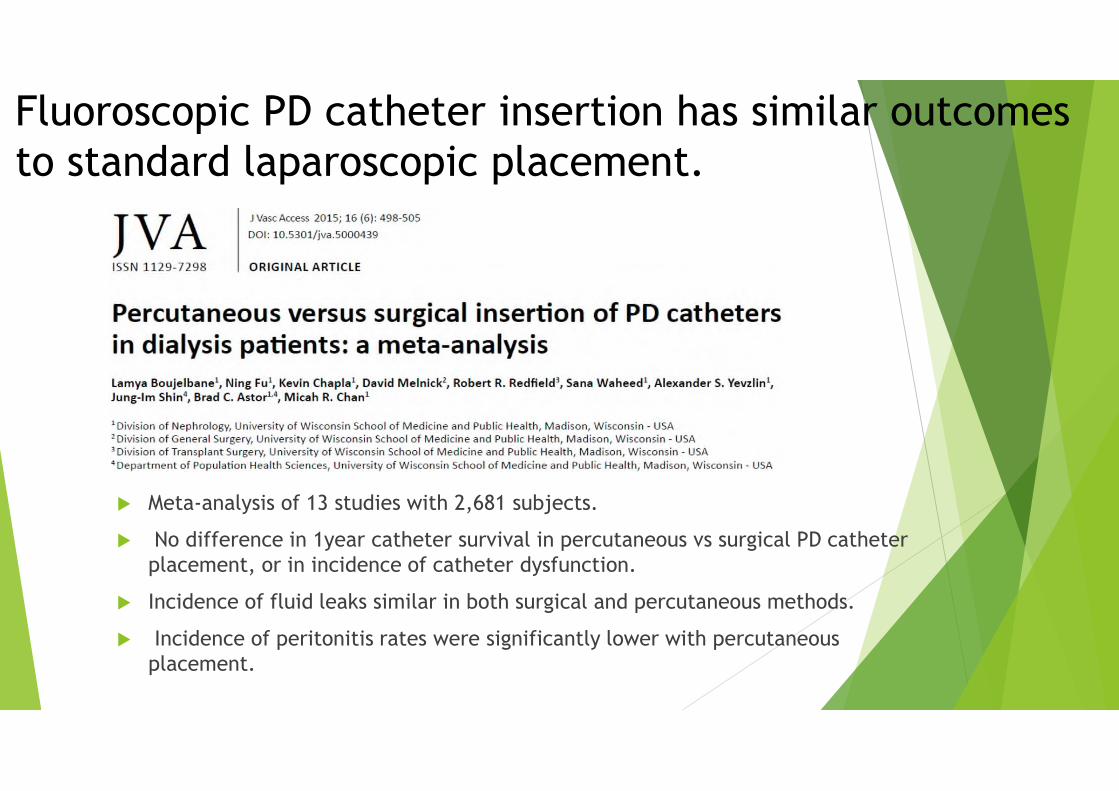
Meta-analysis of 13 studies with 2,681 subjects.
No difference in 1year catheter survival in percutaneous vs surgical PD catheterplacement, or in incidence of catheter dysfunction.
Incidence of fluid leaks similar in both surgical and percutaneous methods.
Incidence of peritonitis rates were significantly lower with percutaneousplacement.
Fluoroscopic PD catheter insertion has similar outcomesto standard laparoscopic placement.
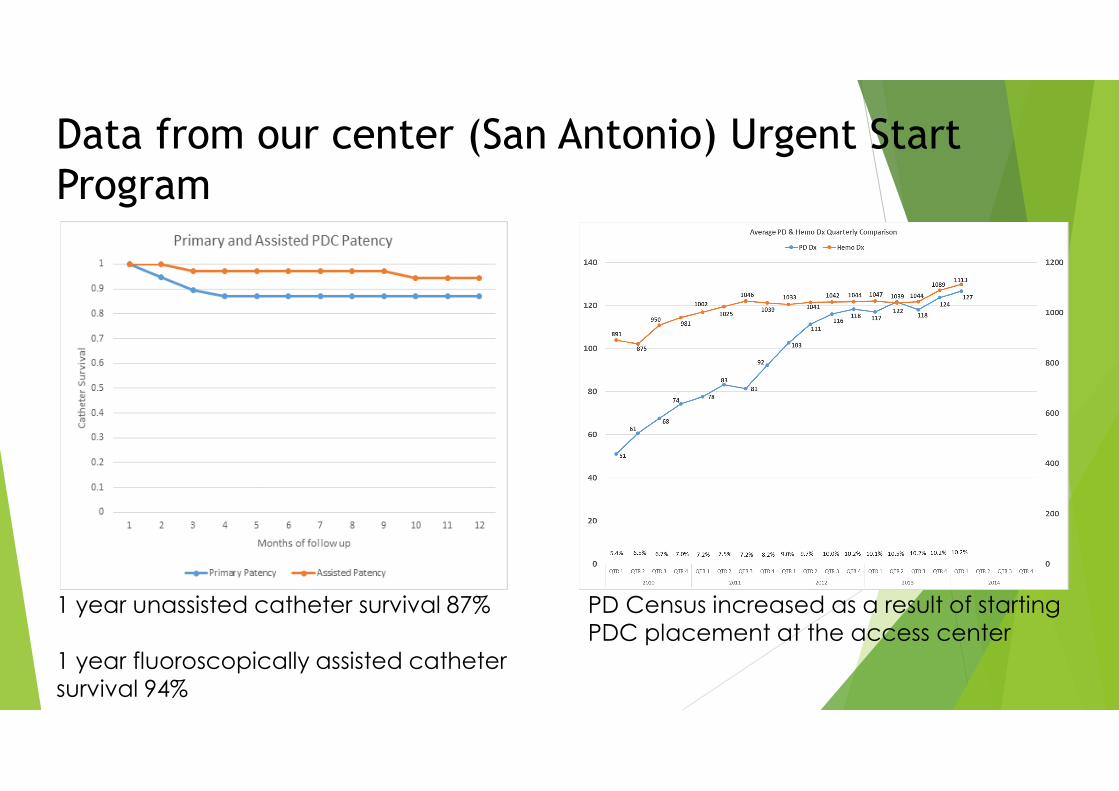
Data from our center (San Antonio) Urgent StartProgram
1 year unassisted catheter survival 87%
1 year fluoroscopically assisted cathetersurvival 94%
PD Census increased as a result of startingPDC placement at the access center
Summary
There is a clinical and economic need for greater PDprevalence
Non-surgeons can readily learn to and performpercutaneous fluoroscopic PD catheter insertion
Nephrologists getting more involved in PD catheterinsertion can increase PD census
If my program can do it and be successful, so can yours.
Outcomes/Goals (ISPD):
Goal to have 1 year catheter survival > or equal to 80%
Fewer than 20% of catheters removed per year for anycomplication including hydraulic failure, failure of deep orsubcutaneous cuffs, or infection.
Peritonitis rate should not exceed 1 episode every 18months (0.67 per year at risk). (Depends on both insertingfacility and PD units)
Fewer than 10% of catheters a year should be removed forinfectious complications.
Bowel puncture rate < 1%
ASDIN Certification Guidelines Currently certified by ABIM in Nephrology or American Osteopathic Board of Int
Med in Nephrology, American board of Radiology, or American Board of Surgery
Completed the following:
Study of written or audio-visual materials related to the procedure, It is recommendedbut not required that the apprentice should spend 2 hours in practice of the procedureusing a standard permanent PD catheters. At least 2 catheters be placed in a DummyTummy model or anesthetized dog or pig or human cadaver
Observe placement of 2 PD catheters performed by physician trainers
Performance of 6 placements in the presence of a physician (certified, if possible) intraining . Should be done in 1 year, within the US healthcare system
Documentation and outcome measurement:
Log outcomes at 1 week, one month
Record success of catheter function and occurrence of any catheter dysfunction
Agree to the Monitoring of the Next 10 PD catheter placements for 30 days. If there aremore than two procedure related complications or more than three catheter failures byone month, an additional three placement procedures should be monitored.
Suggestion for trainees
Invest in a electrocautery unit (try not to rely on pen thermalcautery devices)
Invest in good ultrasound equipment- that will allow you toscreen patients well, look for vessels and assist in cannulation ifneeded.
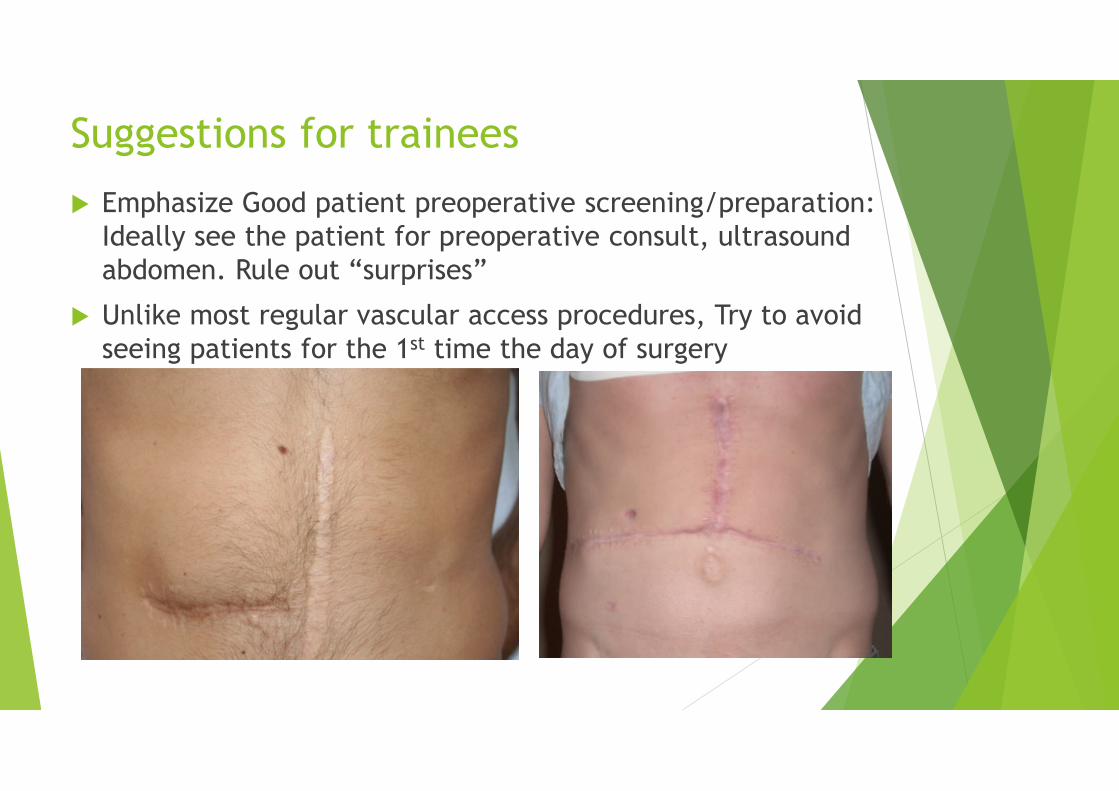
Suggestions for trainees
Emphasize Good patient preoperative screening/preparation:Ideally see the patient for preoperative consult, ultrasoundabdomen. Rule out “surprises”
Unlike most regular vascular access procedures, Try to avoidseeing patients for the 1st time the day of surgery
Involve PD nurses, invite them to watchcases, give them your cell phone number andhave their number.
Be interested in what goes on in the PD unit
Work with the nurses and fellow physiciansto establish protocols for referral, PDcatheter dysfunction, make the PD nurses andthe Access center part of the same team.
Suggestions for trainees
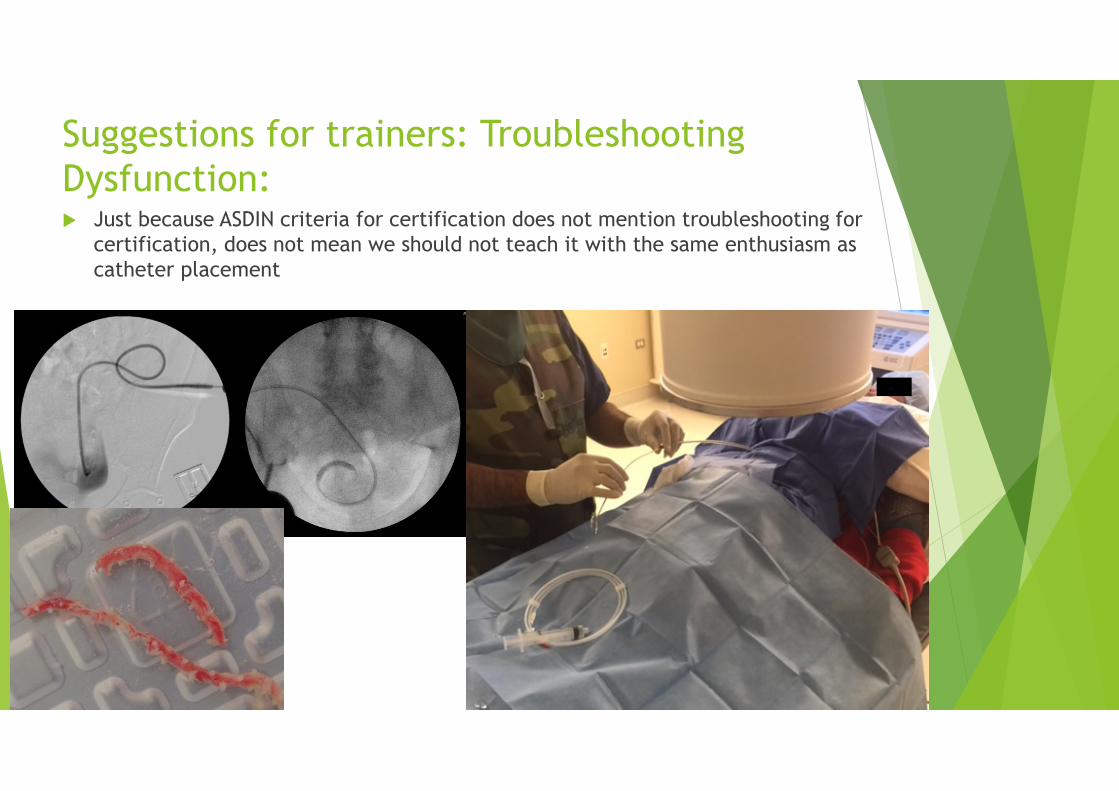
Suggestions for trainers: TroubleshootingDysfunction: Just because ASDIN criteria for certification does not mention troubleshooting for
certification, does not mean we should not teach it with the same enthusiasm ascatheter placement
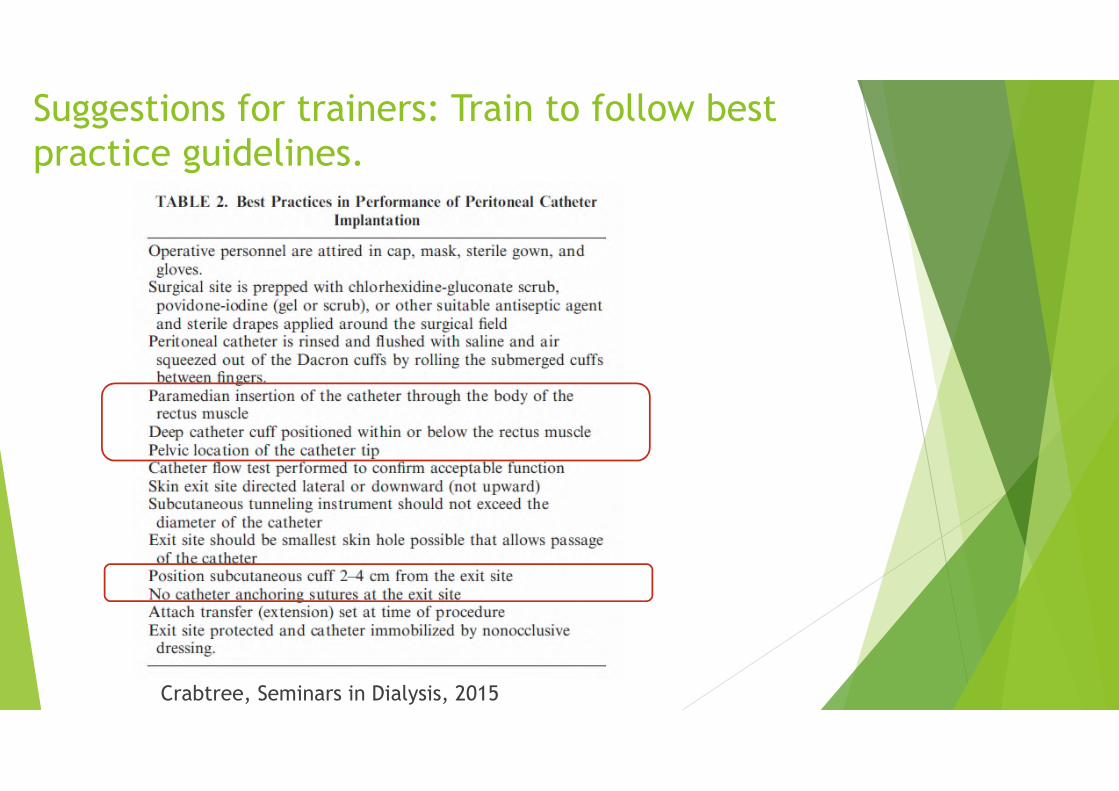
Suggestions for trainers: Train to follow bestpractice guidelines.
Crabtree, Seminars in Dialysis, 2015

Suggestion for trainers: emphasize safety:
Consider using a blunt needle to enter the peritoneaum.
Consider doing a pull back peritoneogram and wire-retraction andre-insertion upon entry into the peritoneum.
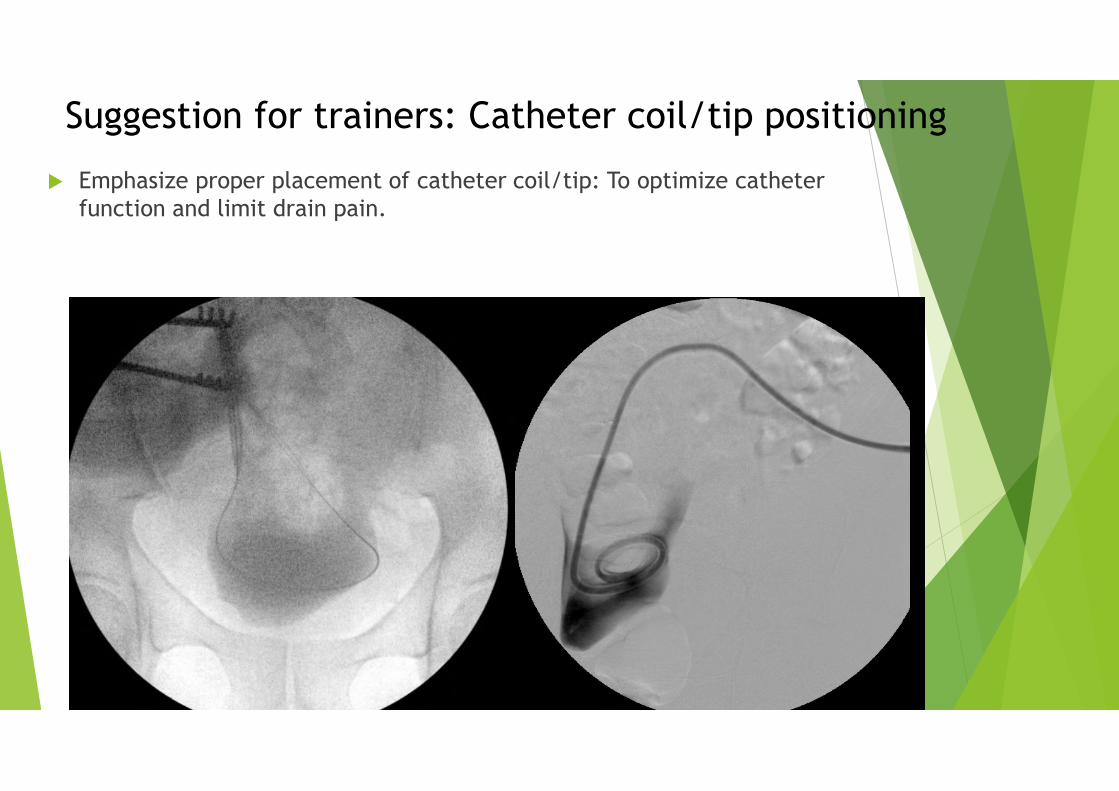
Suggestion for trainers: Catheter coil/tip positioning
Emphasize proper placement of catheter coil/tip: To optimize catheterfunction and limit drain pain.
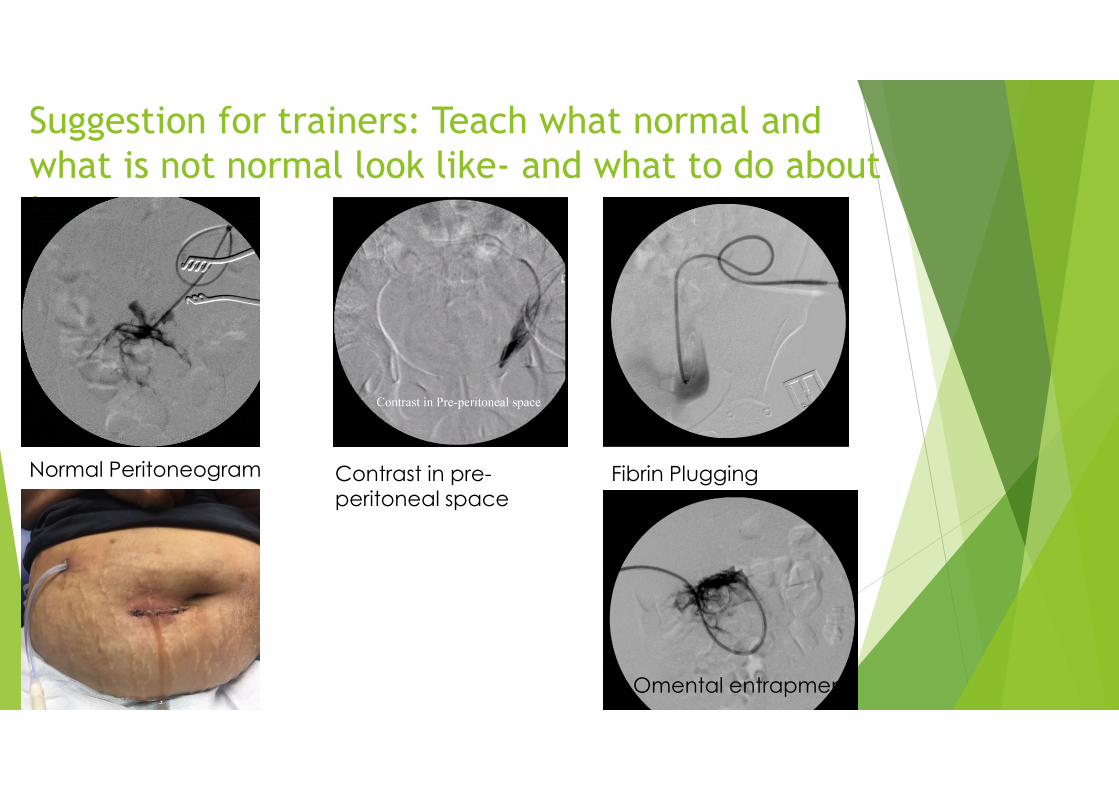
Suggestion for trainers: Teach what normal andwhat is not normal look like- and what to do aboutit..
Normal Peritoneogram Contrast in pre-peritoneal space
Fibrin Plugging
Omental entrapment
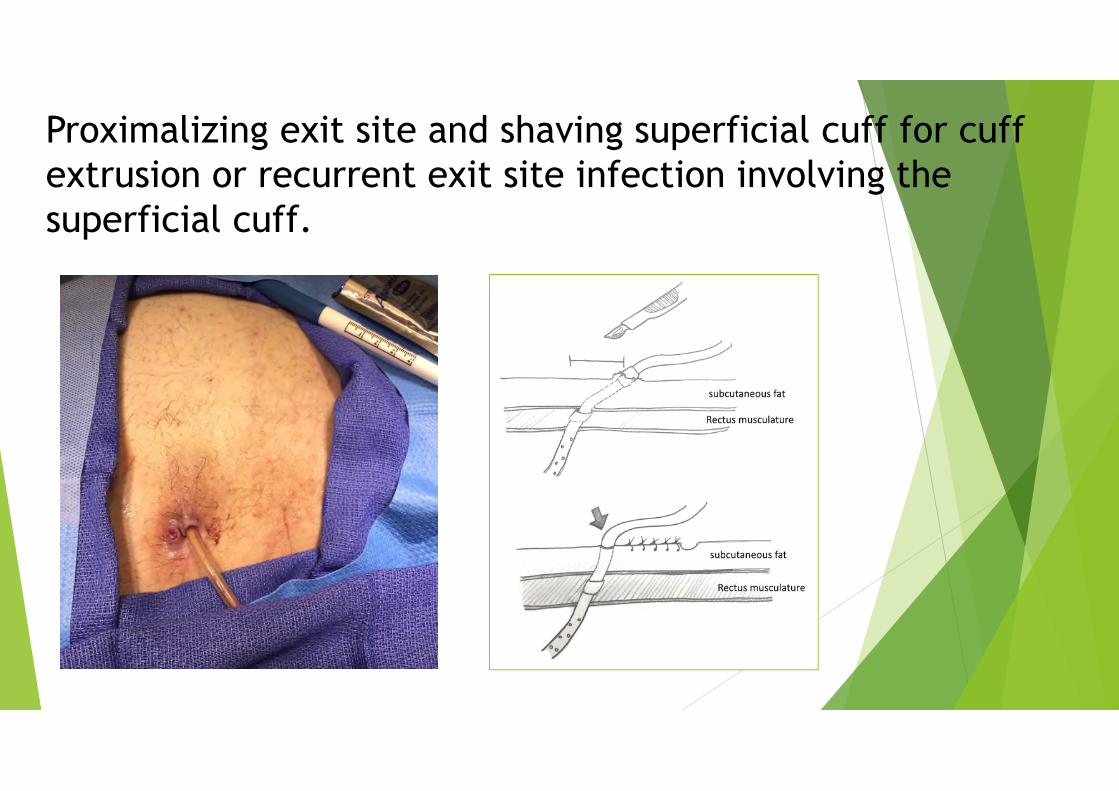
Proximalizing exit site and shaving superficial cuff for cuffextrusion or recurrent exit site infection involving thesuperficial cuff.
Conclusions:
In many areas there is a clinical and economical need fornephrologists and non-surgeons to start placing PD catheters,and this can be done with similar good outcomes as standardlaparoscopic methods.
Trainees to should be mindful of ISPD goals as they start theirprograms, and also be closely involved with the PDunits/nurses to maximize success
Trainers should train to emphasize best practice guidelines,and safety
Trainers should emphasize not just insertion techniques butalso troubleshooting and dealing with complications.