tobacco chewing in english coal miners: a preliminary report
TRANSCRIPT
TOBACCO CHEWING IN ENGLISH COAL MINERS
A Prel iminary Report
W. R. TYLDESLEY, M.Sc., Ph.D., F.D.S.R.C.S.(Ed.) Department of Dental Surgery, University of Liverpool
THE relationship between oral leukoplakia and tobacco smoking and chewing habits has been demonstrated in a number of studies (Mehta et al., I969a; Mehta et al., I969b; Pindborg & Renstrup, I963; Pindborg, Strivastava & Gupta, I964; Von Wyk, I966). Most of these studies have been carried out in India where oral carcinoma constitutes a major problem, representing a high proportion of all cancers diagnosed (Mehta et al., I969a). In much of Asia tobacco chewing in some form is practised. Frequently the tobacco is combined with betel nut and lime, wrapped in a betel leaf to form a small parcel--a pan. In some areas of India the tobacco may be chewed alone or with added lime and, according to the habit of the region, the position of the chew in the mouth varies. Often chewing habits are combined with tobacco smoking habits and any response of the mucosa must be considered to be due to the mixed habit. The prevalence of leukoplakia varies from 1.6 to 8.I per cent. in communities where mixed habits are practiced (Mehta et al., I969a), the figure apparently depending on the precise nature of the habits in each of the areas surveyed.
A similar habit to tobacco chewing is snuff chewing, a practice seen in Scandinavia. The snuff is placed in the oral vestibule--usually repeatedly in the same position. It has been shown (Pindborg & Renstrup, I963) that this habit induces leukoplakia, but without any tendency to malignant change. The question of the premalignant nature of the tobacco-induced leukoplakias is an open one. Although some authorities state without reservation that there is a clear association between the use of all forms of tobacco and oral cancer (Moore, I965), no one has so far demonstrated an established relationship as is the case with leukoplakia. Pindborg and Renstrup (I963) state that 'it is substantiated that tobacco promotes epithelial proliferation of the oral mucosa regardless of the manner in which it is used. The histological response, and probably the carcinogenic effect vary, however, with the different habits.' They also state that of the tobacco habits, chewing is most frequently associated with the development of cancer. Landy and White (I96i) in a survey of snuff chewers found it difficult to distinguish between true malignancy and pseudoepitheliomatous hyperplasia in the snuff- induced leukoplakias. It has been suggested that the development of the lesions towards malignancy may well be influenced by the patients' nutritional status, and it has been shown that in some areas of India a large proportion of subjects with carcinoma of the mouth have previously suffered from oral submucous fibrosis, a condition in which nutritional imbalance has been implicated, (Pindborg, Poulsen & Zachariah, I967). It would certainly appear that a high proportion of tobacco-induced leukoplakias remain as such and do not progress towards malignancy. The modern concept ofleukoplakia as a lesion, of which the prognosis can be assessed only by a study of histological detail, seems to be well substantiated in these tobacco-induced lesions.
2I
22 BRITISH JOURNAL OF ORAL SURGERY
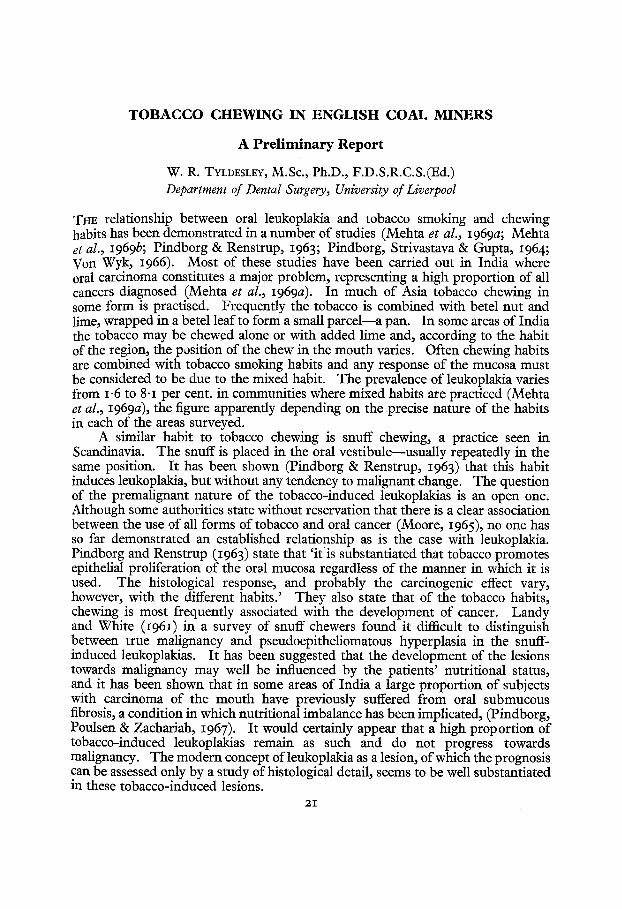
The tobacco chewing habit of English coal miners has not previously been reported. It is carried out 8s a substitute for smoking in the underground conditions where this would be impossible. The tobacco being an excellent sialogogue, there is also the added effect that the mouth is kept moist in the dusty working conditions of the coal mines. The tobacco is placed in the mouth in quantities of from o. 5 g. to I g., is softened by the saliva and is then very gently chewed or kept in the buccal sulcus (Fig. i). In the case of edentulous subjects, the dentures are usually removed before descending the mine and the chewing takes place between edentulous ridges. In some subjects the chew is constantly moved around the mouth. Often (as in Fig. I), where an edentulous area occurs, the tobacco is kept on the ridge.
FIG. I
Chew of tobacco in place in mouth of subject.
When the chew is exhausted the tobacco is replaced, the tobacco-stained saliva being continually expectorated.
There is some extra significance in the study of this habit since it is carried out in a group in which nutritional deficiency might be expected to be at a minimum. Thus, the resultant lesions should be unaffected by any such deficiency.
MATERIAL AND METHODS
The investigation was carried out in a group of five closely associated coal mines in South Lancashire.
In order to determine the extent of the chewing habit 149o miners, both surface and underground workers, were questioned as to their tobacco habits. This figure represented 91.6 per cent. of the total work force of two collieries. Information available included the location of the subjects' work in the mine (i.e. surface or underground worker) as well as personal details. Detailed information was obtained by the questioning and examination of 402 volunteer subjects from
TOBACCO CHEWING IN ENGLISH COAL MII~EXS 23
the five collieries. Of these 28o were tobacco chewers and 122 non-chewers. The information obtained, apart from personal details, included the quantity of tobacco chewed, the duration of the habit and the location of the tobacco when chewing, together with details of the use of smoking tobacco and snuff.
All mouths were examined in natural light as far as possible, lesions being recorded on charts similar to those suggested by Roed-Petersen and Renstrup (1969). All white lesions of the oral mucosa were charted, the terms leukoplakia, pre-leukoplakia and leukoedema being used to conform to the usage of Pindborg et al. (1968). Thus, leukoplakia was defined as a white patch which could not be rubbed off and which could not be diagnosed as being due to any other disease. Pre-leukoplalda was the term used to describe a lesion similar to that of leukoplakia but less well defined and with a greyish appearance rather than the white of leukoplakia. Leukoedema was the term used to describe the condition where the mucosa was covered by a diffuse, faint grey-white film which could, at least partly, be scraped off.
Incisional biopsy, under local anaesthetic, was carried out on those lesions recorded as leukoplakia when allowed by the subject (8 cases).
RESULTS
The incidence of the habit among 149o miners is shown in Table I. It will be seen that there is an incidence of only 1.7 per cent. chewers amongst the surface workers although a large proportion of these workers have previously worked underground.
TABLE I
Total Chewers
Surface Workers 399 7 = I'7 %
Underground Workers lO91 374 = 34"3 %
TABLE II
Total Smokers
Chewers 195 178 = 91"2%
Non-Chewers 663 243 = 37"5%
The relationship between chewing and smoking in 858 miners is shown in Table II. It will be seen that in 91"2 per cent. of cases the tobacco habit is a mixed one of chewing and smoking.
The consumption of chewing tobacco was found to vary from 3 g. to 15 g. per day, the most usual pattern being the use of one pre-packed daily supply of 45 g. The age range of the chewers examined was wide, from 17 to 64 years.
24 BRITISH JOURNAL OF ORAL SURGERY
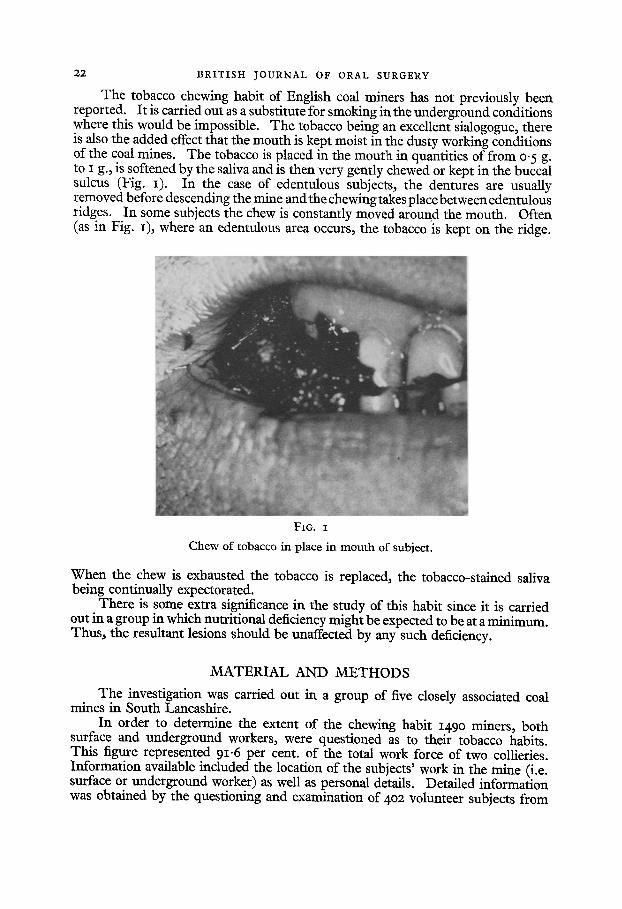
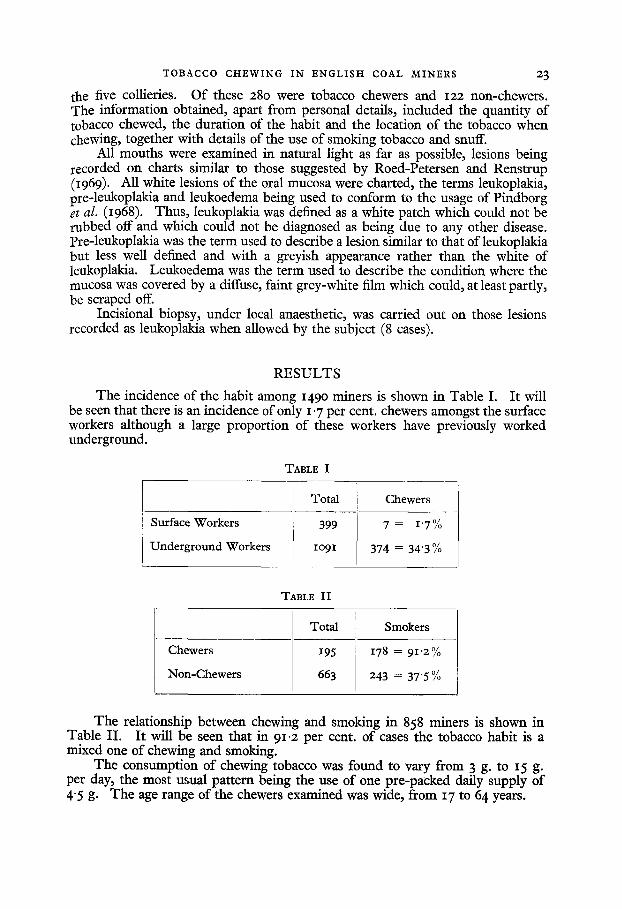
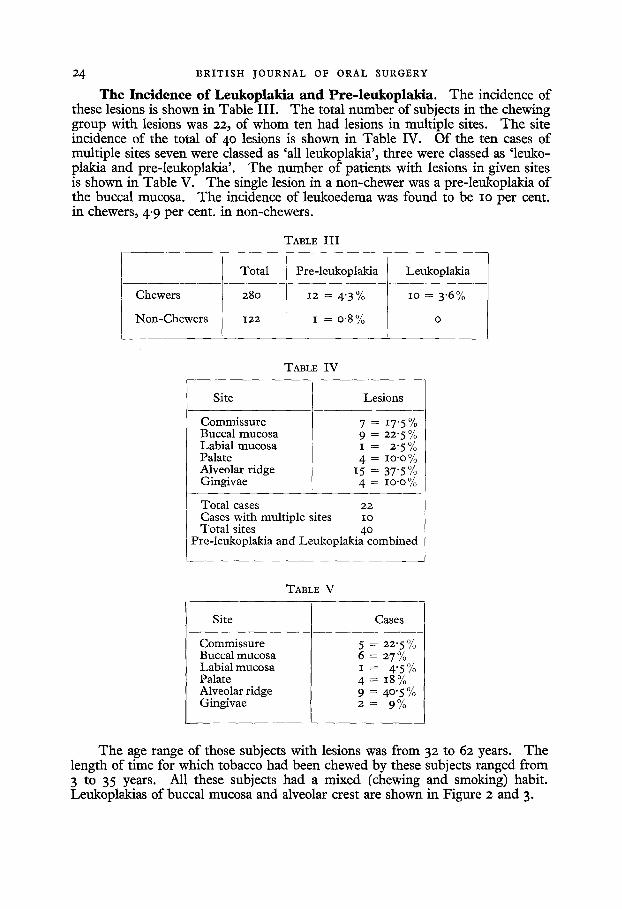
The Incidence of Leukoplakia and Pre-leukoplakia. T h e inc idence o f these les ions is shown in T a b l e I I I . T h e to ta l n u m b e r o f subjects in t he chewing g r o u p w i t h lesions was 22, o f w h o m t en h a d les ions in m u l t i p l e sites. T h e s i te i nc idence o f t he to ta l o f 40 lesions is s h o w n in T a b l e IV. O f t h e t en cases o f m u l t i p l e si tes seven were c lassed as 'a l l l eukop lak ia ' , t h r ee were c lassed as ' l e uko - p lak ia a n d p r e - l eukop l ak i a ' . T h e n u m b e r o f pa t i en t s w i th les ions in g iven si tes is s h o w n in T a b l e V. T h e s ingle les ion in a n o n - c h e w e r was a p r e - l e u k o p l a k i a o f t he bucca l mucosa . T h e inc idence o f l e u k o e d e m a was f o u n d to b e i o p e r cent . in chewers , 4"9 p e r cent . in non -chewer s .
TABLE I I I
Total Pre-leukoplakia Leukoplakia
Chewers 280 12 = 4"3% io = 3"6%
Non-Chewers 122 I = o-8 % o
TABLE IV
Site Lesions
Commissure Buccal mucosa Labial mucosa Palate Alveolar ridge Gingivae
7 = 17"5% 9 -- 22"5% I = 2"5% 4 = lO'O%
15 = 37'5% 4 = lO"O%
Total cases 22 Cases with multiple sites io Total sites 4o
Pre-leukoplakia and Leukoplakia combined
TABLE V
Site Cases
Commissure Buccal mucosa Labial mucosa Palate Alveolar ridge Gingivae
5 = 22"5% 6 = 27% I-- - 4"5% 4 = 18% 9 = 40"5% 2 = 9%
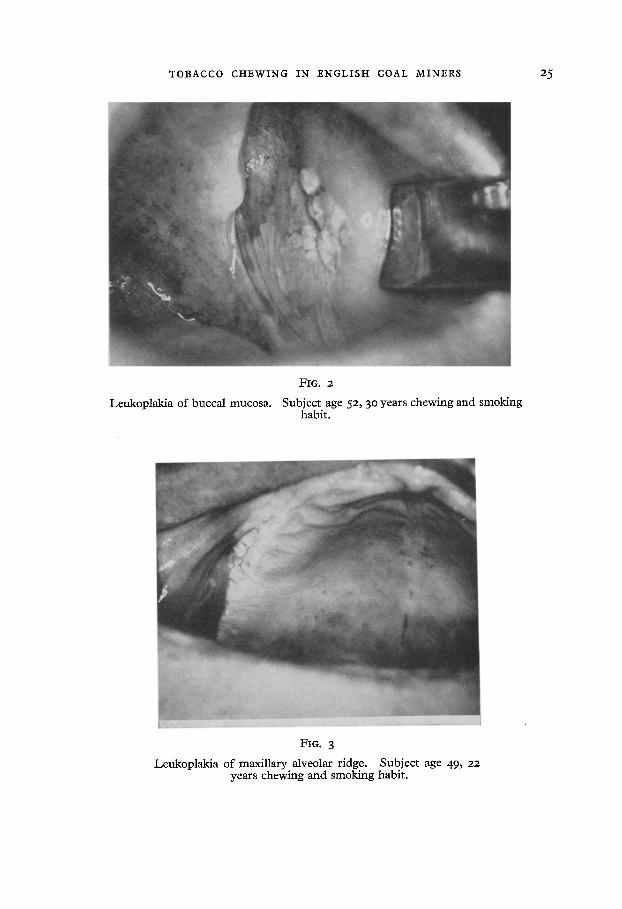
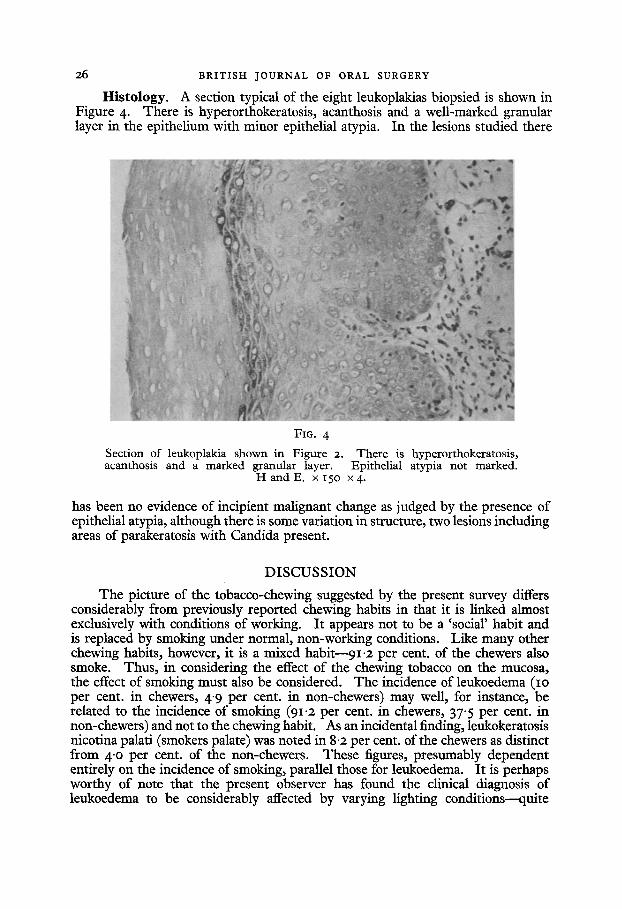
The age range of those subjects with lesions was from 32 to 62 years. The length of time for which tobacco had been chewed by these subjects ranged from 3 to 35 years. All these subjects had a mixed (chewing and smoking) habit. Leukoplakias of buccal mucosa and alveolar crest are shown in Figure 2 and 3.
TOBACCO CHEWING IN ENGLISH COAL MINERS 25
Leukoplakia of buccal mucosa.
FIG. 2
Subject age 52, 30 years chewing and smoking habit.
FIG. 3
Leukoplakia of maxillary alveolar ridge. Subject age 49~ 22 years chewing and smoking habit.
26 BRITISH JOURNAL OF ORAL SURGERY
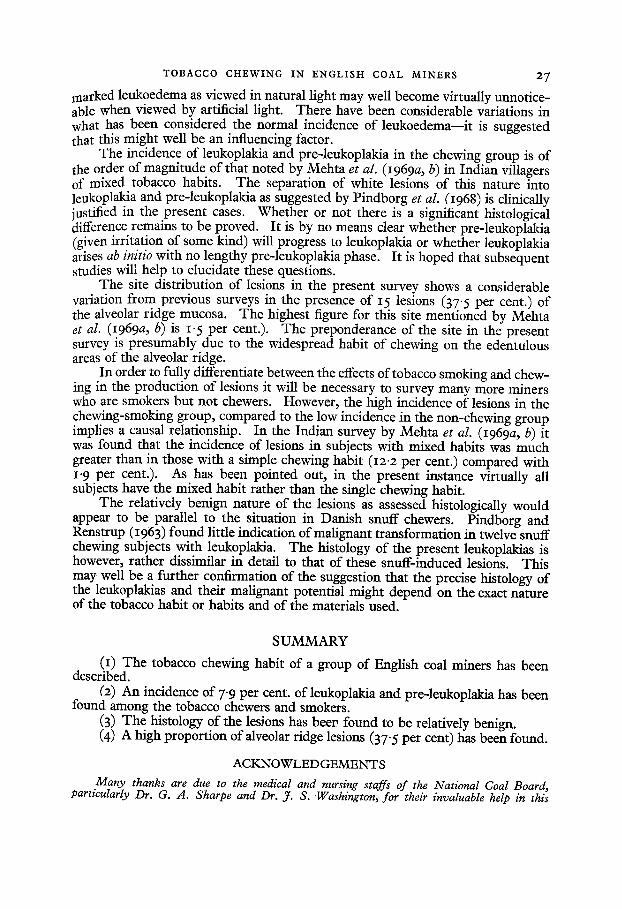
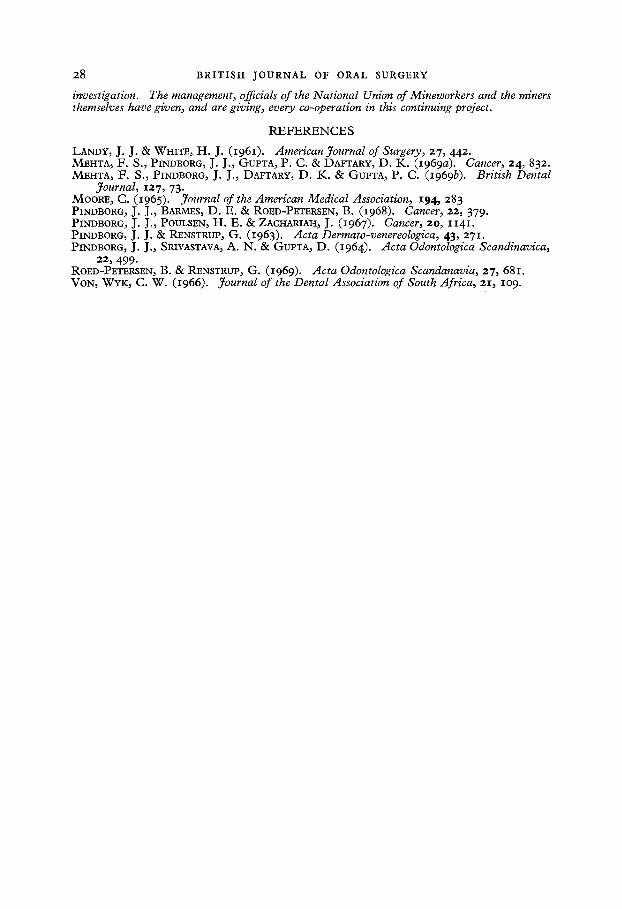
Histology. A section typical of the eight leukoplakias biopsied is shown in Figure 4. There is hyperorthokeratosis, acanthosis and a well-marked granular layer in the epithelium with minor epithelial atypia. In the lesions studied there
FIG. 4
Section of leukoplakia shown in Figure 2. There is hyperorthokeratosis, acanthosis and a marked granular layer. Epithelial atypia not marked.
HandE. xlSO x4.
has been no evidence of incipient malignant change as judged by the presence of epithelial atypia, although there is some variation in structure, two lesions including areas of parakeratosis with Candida present.
DISCUSSION
The picture of the tobacco-chewing suggested by the present survey differs considerably from previously reported chewing habits in that it is linked almost exclusively with conditions of working. It appears not to be a 'social' habit and is replaced by smoking under normal, non-working conditions. Like many other chewing habits, however, it is a mixed habit--91.2 per cent. of the chewers also smoke. Thus, in considering the effect of the chewing tobacco on the mucosa, the effect of smoking must also be considered. The incidence of leukoedema (IO per cent. in chewers, 4"9 per cent. in non-chewers) may well, for instance, be related to the incidence of smoking (91"2 per cent. in chewers, 37"5 per cent. in non-chewers) and not to the chewing habit. As an incidental finding, leukokeratosis nicotina palati (smokers palate) was noted in 8.2 per cent. of the chewers as distinct from 4.o per cent. of the non-chewers. These figures, presumably dependent entirely on the incidence of smoking, parallel those for leukoedema. It is perhaps worthy of note that the present observer has found the clinical diagnosis of leukoedema to be considerably affected by varying lighting conditions--quite
TOBACCO CHEWING IN ENGLISH COAL MINERS 27
marked lcukoedcma as viewed in natural light may well become virtually unnotice- able when viewed by artificial light. There have been considerable variations in what has been considered the normal incidence of lcukocdcma--it is suggested that this might well be an influencing factor.
The incidence of leukoplakia and pre-leukoplakia in the chewing group is of the order of magnitude of that noted by Mehta et al. (I969a, b) in Indian villagers of mixed tobacco habits. The separation of white lesions of this nature into leukoplakia and pre-leukoplakia as suggested by Pindborg et al. (1968) is clinically justified in the present cases. Whether or not there is a significant histological diffcrencc remains to be proved. It is by no means clear whether pre-leukoplakia (given irritation of some kind) will progress to leukoplakia or whether leukoplakia arises ab initio with no lengthy pre-leukoplakia phase. It is hoped that subsequent studies will help to elucidate these questions.
The site distribution of lesions in the present survey shows a considerable variation from previous surveys in the presence of 15 lesions (37"5 per cent.) of the alveolar ridge mucosa. The highest figure for this site mentioned by Mehta et al. (I969a, b) is 1. 5 per cent.). The preponderance of the site in the present survey is presumably due to the widespread habit of chewing on the edentulous areas of the alveolar ridge.
In order to fully differentiate between the effects of tobacco smoking and chew- ing in the production of lesions it will bc necessary to survey many more miners who are smokers but not chewers. However, the high incidence of lesions in the chewing-smoking group, compared to the low incidence in the non-chewing group implies a causal relationship. In the Indian survey by Mehta et al. (I969a, b) it was found that the incidence of lesions in subjects with mixed habits was much greater than in those with a simple chewing habit (I2"2 per cent.) compared with I'9 per cent.). As has been pointed out, in the present instance virtually all subjects have the mixed habit rather than the single chewing habit.
The relatively benign nature of the lesions as assessed histologically would appear to be parallel to the situation in Danish snuff chewers. Pindborg and Renstrup (I963) found little indication of malignant transformation in twelve snuff chewing subjects with leukoplakia. The histology of the present leukoplakias is however, rather dissimilar in detail to that of these snuff-induced lesions. This may well be a further confirmation of the suggestion that the precise histology of the leukoplakias and their malignant potential might depend on the exact nature of the tobacco habit or habits and of the materials used.
SUMMARY
(1) The tobacco chewing habit of a group of English coal miners has been described.
(2) An incidence of 7"9 per cent. of leukoplakia and pre-leukoplakia has been found among the tobacco chewers and smokers.
(3) The histology of the lesions has beep found to be relatively benign. (4) A high proportion of alveolar ridge lesions (37"5 per cent) has been found.
ACKNOWLEDGEMENTS
Many thanks are due to the medical and nursing staffs of the National Goal Board, particularly Dr. G. A. Sharpe and Dr. ft. S. Washington, for their invaluable help in this
28 BRITISH JOURNAL OF ORAL SURGERY
investigation. The management, officials of the National Union of Mineworkers and the miners themselves have given, and are giving, every co-operation in this continuing project.
REFERENCES
LANDY, J. J. & WHITE, H. J. (1961). American Journal of Surgery, 27, 442. MEHTA, F. S., PINDBORG, J. J., GUPTA, P. C. & DAFTARY, D. K. (I969a). Cancer, 24, 832. MEHTA, F. S., PINDBORG, J. J., DAFTARY, D. K. & GUPTA, P. C. (19693). British Dental
Journal, 127, 73. MOORE, C. (1965). Journal of the American Medical Association, 194, 283 PINDBORG, J. J., BARMES, D. E. & ROED-PETERSEN, B. (I968). Cancer, 22, 379. PINDBORG, J. J., POIYLSEN, H. E. & ZACHARIAH, J. (1967). Cancer, 20, 1141. PINDBORG, J. J. & RENSTRUP, G. (1963). Acta Dermato-venereologica, 43, 271. PINDBORG, J. J., SRIVASTAVA, A. N. & GUPTA, D. (1964). Aeta Odomologica Scandinavica,
22, 499. ROED-PETERSEN, B. & RENSTRUP, G. (I969). Acta Odontologica Scandanavia, 27, 681. VON, WYK, C. W. (1966). Journal of the DentalAssociation of South Africa, 2I, lO 9.