timing is everything—colectomy performed on monday decreases length of stay
TRANSCRIPT

The American Journal of Surgery (2013) 206, 340-345
Clinical Science
Timing is everythingdcolectomy performed on Mondaydecreases length of stay
Denis M. Gilmore, M.D., Thomas Curran, M.D., Shiva Gautam, Ph.D.,Deborah Nagle, M.D., Vitaliy Poylin, M.D.*
Department of Surgery, Beth Israel Deaconess Medical Cen
ter, Boston, MA, USAKEYWORDS:Day of week;Colectomy;Length of stay
The authors declare no conflicts of i
* Corresponding author. Tel.: 11-6
2978.
E-mail address: [email protected]
Manuscript received May 22, 2012;
2012
0002-9610/$ - see front matter � 2013
http://dx.doi.org/10.1016/j.amjsurg.20
AbstractBACKGROUND: Perioperative care of patients undergoing colon resection requires a multidisciplin-
ary approach by the operating surgeon, residents, and nurses. Operations performed on Monday takefull advantage of hospital resources throughout the week to meet expected discharge by Friday. In acurrent health care environment of diminishing means, improving the timing of surgery in relationto expected length of stay may play an important role in preserving health care resources.
METHODS: A retrospective review of a prospectively collected colorectal surgical database identi-fied all patients who underwent segmental colon resection at a single tertiary care referral center from2004 to 2010. Length of stay for patients undergoing elective open and minimally invasive segmentalcolectomy was compared for Monday versus Tuesday through the weekend. Patient and surgeon demo-graphics were recorded as well as postoperative outcomes and complications.
RESULTS: A total of 868 segmental colectomies were performed during the study period. Length ofstay was significantly decreased by .73 days (P , .01) for all segmental colectomies performed onMonday compared with those performed Tuesday through Sunday. There was also a significantdecrease in length of stay looking independently at right (.96 days, P , .01) and left or sigmoidcolectomies (.56 days, P, .01). There was no significant difference in patient or surgeon demographicsto account for this difference.
CONCLUSIONS: Segmental colectomies have a significantly decreased length in stay whenperformed on Monday compared with the rest of the week. The decrease is independent of surgeon,comorbidities, and complications. This difference may be the result of patients’ taking full advantageof hospital resources and ancillary support. Cost-effective measures may be evaluated and directed atadjustment of resources available throughout the week to reduce length of stay.� 2013 Elsevier Inc. All rights reserved.
Timing is critical in patient care. Time until intervention,total time of therapy, and the time of day or day of the weeka procedure is performed all affect patient outcomes.1–6
nterest.
17-667-4159; fax: 11-617-667-
revised manuscript October 5,
Elsevier Inc. All rights reserved.
12.11.014
Hospitals function 24 hours per day, but many servicesare curtailed or suspended during evening and weekendhours, with potential detrimental effects. In the currentenvironment of diminishing returns, optimal utilization ofavailable resources is needed to provide excellent yetcost-effective patient care. Multidisciplinary managementof surgical patients has become the current paradigm inmany areas of medicine and surgery.7–9 For each individualmember of the care team, effects of long work days andwork weeks in addition to increases in care transitions

D.M. Gilmore et al. Early Week Surgery Decreases LOS 341
and decreased staffing may result in possible suboptimaland delayed care, leading to increased length of stay. Deci-sions on scheduling and staffing may be altered to accountfor expected postoperative course and potentially improvethe efficiency and effectiveness of postoperative outcomesof surgical patients.
The effect of timing on patient outcomes is welldocumented in both medicine and surgery. Nonemergentsurgical cases and anesthetic procedures performed later inthe day have both increased mortality and adverse eventswhen risk adjusted and compared against first-start cases.Differences in outcomes are attributed to medical caredelivery factors such as case load, fatigue, and care transi-tions.1,2 In addition to the time of day, nonemergent caseshave increased mortality if surgery is performed on Fridayversus Monday through Wednesday.3 The same poor out-comes are noted in patients presenting over the weekendwith acute myocardial infarction4 and stroke.5,6 The authorscollectively conclude that the differences in outcomes maybe secondary to decreased staffing on weekends, leading toinadequate and/or delayed care. Studies of both floor and in-tensive care unit nursing have confirmed that stable staffingand on-site intensivist coverage leads to stability and conti-nuity of care and similar outcomes regardless of time of dayor day of the week.10–12 In addition to ancillary staff short-ages, hospitals have the added pressure of resident work-hour restrictions with which to contend. Consistent, qualitycare is needed for optimal patient outcomes.
Reported length of stay after minimally invasive colec-tomy ranges from 3 to 5 days.13–17 On the basis of thesedata, for procedures performed on Monday, Friday shouldbe an expected date of discharge in this cohort. Our studyaim was to determine if the day of the week a procedureis performed has an effect on the length of stay. On thebasis of current literature, we hypothesized that colectomyperformed on Monday avoids the ‘‘weekend effect’’ ofdecreased staffing and should have the benefit of allowingpatients to take advantage of full hospital resourcesthroughout the week of the multidisciplinary team members(nursing, ostomy care, physical therapy, case management,and surgical staff), resulting in shorter length of stay.
Table 1 Total number of cases reviewed in each respectivegroup for Monday compared with the rest of the week
Colectomy Case type Monday Rest of the week
Right All 107 294MIS 63 131Open 44 163
Left All 138 329MIS 92 186Open 47 143
MIS 5 minimally invasive surgery.
Methods
Database
A prospectively collected colorectal database wasreviewed for all elective segmental colectomies performedat a tertiary referral center over the period from 2004 to2010. We compared all right and left or sigmoid colec-tomies performed using open and minimally invasive(single-incision laparoscopic surgery, laparoscopic, andhybrid) approaches performed on Monday versus Tuesdaythrough the weekend. Patient age, sex, and comorbiditieswere recorded. A total of 25 surgeons were included in thisstudy. Excluded were rectal cases, emergent cases, and
those with incomplete data. Outcomes measured includedlength of stay and complications of wound infection,anastomotic leak, deep venous thrombosis, urinary tractinfection, urinary retention, ileus, pneumonia, acute renalfailure, return to the operating room, and death.
Statistical analysis
All analysis was performed using SAS (SAS InstituteInc, Cary, NC). We performed univariate and multivariateanalyses. In the univariate and multivariate analyses, thosefactors with P values ..15 were not considered for furtheranalysis. The associations between the cofactors and lengthof stay were evaluated using Wilcoxon’s rank-sum tests forcontinuous variables and Fisher’s exact tests or chi-squaretests for categorical variables, individually. Length of staywas log transformed and then compared for Monday versusthe rest of the week using a 2-sample t test. To adjust for theeffect of covariates found to be significant in the univariateanalysis, we used a linear regression approach. Even afteradjusting for these factors, day of the week was found tobe a significant predictor of length of stay. The effect ofday of the week on several outcomes was evaluated usinglogistic regression approach.
Results
In total, 868 segmental colectomies were reviewed,including 401 right and 467 left or sigmoid colectomies.Colectomies were also broken down by surgical approach,including open and minimally invasive (single-incisionlaparoscopic surgery, laparoscopic, and hybrid). For rightcolectomy, minimally invasive (n 5 194) and open(n 5 207) approaches were compared. Similarly, for leftcolectomy, minimally invasive (n 5 277) and open(n 5 190) approaches were reviewed. Differences in lengthof stay among all, left, and right colectomies were exam-ined, as well as by approach (Table 1).
Patient demographics were collected for all cases. Theaverage ages were 59.4 and 60.1 years in the Monday cohortand those who had surgery performed later in the week,respectively. The ratio of male to female patients was notstatistically significant (1.3 vs 1.1). Rates of comorbidities,

Figure 1 Length of stay for all segmental colectomies performedon Monday compared with the rest of the week. There was a sig-nificant decrease in length of stay for procedures performed onMonday, driven mostly by minimally invasive procedures.
342 The American Journal of Surgery, Vol 206, No 3, September 2013
including inflammatory bowel disease, coronary arterydisease, diabetes, congestive heart failure, chronic obstruc-tive pulmonary disease, atrial fibrillation, cirrhosis, andother cancers, were compared for patients who underwentelective segmental colectomy and were not statisticallysignificant (Table 2). There was no significant statistical dif-ference in the 2 patient groups with regard to age, sex, orrates of comorbidities, and therefore, differences in lengthof stay cannot be attributed to patient qualities.
For colectomies performed on Monday, anticipateddischarge is on Friday, thus minimizing any potentialweekend effect. Therefore, length of stay was comparedfor procedures performed on Monday versus the rest of theweek. When all colectomy cases were compared, there wasa significant decrease in length of stay of .73 days (5.04 vs5.77 days, P , .01). Surgical approaches were compared toevaluate for bias due to the potential influence of minimallyinvasive procedures. For all colectomies performed using aminimally invasive approach, there was a significant de-crease of .4 days (4.4 vs 4.8 days, P 5 .02). The open ap-proach led to a decrease of .8 days, but it did not reachstatistical significance (5.9 vs 6.7 days, P 5 .12). A de-crease in length of stay was demonstrated for all segmentalcolectomies performed on Monday compared with the restof the week, although this difference reached significanceonly when comparing all colectomies combined and theminimally invasive approach (Fig. 1). Looking specificallyat right colectomies, again, there was a decrease in lengthof stay, powered mostly by the minimally invasive ap-proach. For all right colectomies, there was a significant de-crease in length of stay of .96 days (4.57 vs 5.53 days,P , .01). Although they did not reach statistical signifi-cance, decreases of 1.0 day (3.9 vs 4.9 days, P 5 .08)and .6 days (5.4 vs 6.0 days, P 5 .46) for minimally inva-sive and open approaches, respectively, were observed(Fig. 2). Last, left or sigmoid colectomies were analyzedfor effect of day of the week of surgery on length of stay.
Table 2 Patient demographics for both Monday and rest-of-the-week populations
Variable Monday Rest of the week
Age (y) 59.4 60.1Ratio of men to women 1.3 1.1IBD 16.8% 14.1%CAD 11.6% 13.5%DM 8.44% 11.9%CHF 5.8% 7.1%COPD 5.5% 5.5%Atrial fibrillation 7.0% 7.7%Other cancer 10.8% 12.8%Cirrhosis 2.7% 5.6%
Groups were not significantly different from each other when age,
sex ratio, and comorbidities were analyzed.
CAD 5 coronary artery disease; CHF 5 congestive heart failure;
COPD 5 chronic obstructive pulmonary disease; DM 5 diabetes
mellitus; IBD 5 inflammatory bowel disease.
All P values ..05.
There was a significant decrease in length of stay of .56days (5.1 vs 5.66 days, P , .01) when all left colectomieswere analyzed. Although there was a minimal difference inlength of stay for minimally invasive left or sigmoid colec-tomies (4.7 vs 4.6 days, P 5 .14), open left colectomies hada considerable decrease of 1.2 days (5.8 vs 7.0 days,P 5 .12) (Fig. 3).
Complications are known to significantly increase lengthof stay. We compared the complication rates in the 2 groupsto ensure that decreases in length of stay were not attributedto this difference (Table 3). There was no statistical differ-ence in complication rates in the 2 groups, and althoughdeep venous thrombosis rates were higher in the rest ofthe week, the total number of was small (n 5 3).
Although the Monday and rest-of-the-week cohorts weresimilar in both comorbidities and complication rates,certain factors were independently associated with anincrease in the length of stay. Using linear regressionanalysis to identify significant effects of covariates onlength of stay, comorbidities of congestive heart failure(1.90 days), cirrhosis (1.02 days), and atrial fibrillation(1.88 days) were identified as independent risk factors forincreased length of stay. Similarly, complications of post-operative wound infection (1.35 days), deep venous throm-bosis (.33 days), anastomotic leak (1.16 days), acute renalfailure (1.00 days), ileus (.46 days), and return to theoperating room (1.24 days) were identified as independent
Figure 2 Length of stay for right colectomies performed onMonday compared with the rest of the week. Overall, there wasa decrease in length of stay for all approaches, although statisticalsignificance was reached only when all colectomies wereanalyzed.
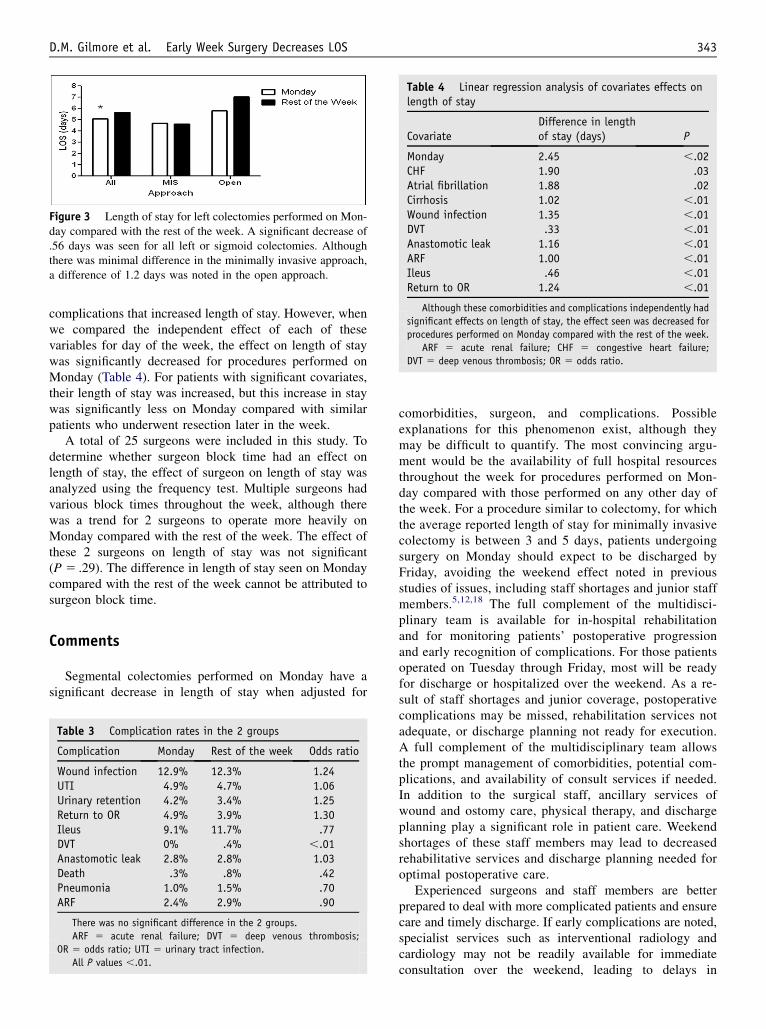
Figure 3 Length of stay for left colectomies performed on Mon-day compared with the rest of the week. A significant decrease of.56 days was seen for all left or sigmoid colectomies. Althoughthere was minimal difference in the minimally invasive approach,a difference of 1.2 days was noted in the open approach.
Table 4 Linear regression analysis of covariates effects onlength of stay
CovariateDifference in lengthof stay (days) P
Monday 2.45 ,.02CHF 1.90 .03Atrial fibrillation 1.88 .02Cirrhosis 1.02 ,.01Wound infection 1.35 ,.01DVT .33 ,.01Anastomotic leak 1.16 ,.01ARF 1.00 ,.01Ileus .46 ,.01Return to OR 1.24 ,.01
Although these comorbidities and complications independently had
significant effects on length of stay, the effect seen was decreased for
procedures performed on Monday compared with the rest of the week.
ARF 5 acute renal failure; CHF 5 congestive heart failure;
DVT 5 deep venous thrombosis; OR 5 odds ratio.
D.M. Gilmore et al. Early Week Surgery Decreases LOS 343
complications that increased length of stay. However, whenwe compared the independent effect of each of thesevariables for day of the week, the effect on length of staywas significantly decreased for procedures performed onMonday (Table 4). For patients with significant covariates,their length of stay was increased, but this increase in staywas significantly less on Monday compared with similarpatients who underwent resection later in the week.
A total of 25 surgeons were included in this study. Todetermine whether surgeon block time had an effect onlength of stay, the effect of surgeon on length of stay wasanalyzed using the frequency test. Multiple surgeons hadvarious block times throughout the week, although therewas a trend for 2 surgeons to operate more heavily onMonday compared with the rest of the week. The effect ofthese 2 surgeons on length of stay was not significant(P 5 .29). The difference in length of stay seen on Mondaycompared with the rest of the week cannot be attributed tosurgeon block time.
Comments
Segmental colectomies performed on Monday have asignificant decrease in length of stay when adjusted for
Table 3 Complication rates in the 2 groups
Complication Monday Rest of the week Odds ratio
Wound infection 12.9% 12.3% 1.24UTI 4.9% 4.7% 1.06Urinary retention 4.2% 3.4% 1.25Return to OR 4.9% 3.9% 1.30Ileus 9.1% 11.7% .77DVT 0% .4% ,.01Anastomotic leak 2.8% 2.8% 1.03Death .3% .8% .42Pneumonia 1.0% 1.5% .70ARF 2.4% 2.9% .90
There was no significant difference in the 2 groups.
ARF 5 acute renal failure; DVT 5 deep venous thrombosis;
OR 5 odds ratio; UTI 5 urinary tract infection.
All P values ,.01.
comorbidities, surgeon, and complications. Possibleexplanations for this phenomenon exist, although theymay be difficult to quantify. The most convincing argu-ment would be the availability of full hospital resourcesthroughout the week for procedures performed on Mon-day compared with those performed on any other day ofthe week. For a procedure similar to colectomy, for whichthe average reported length of stay for minimally invasivecolectomy is between 3 and 5 days, patients undergoingsurgery on Monday should expect to be discharged byFriday, avoiding the weekend effect noted in previousstudies of issues, including staff shortages and junior staffmembers.5,12,18 The full complement of the multidisci-plinary team is available for in-hospital rehabilitationand for monitoring patients’ postoperative progressionand early recognition of complications. For those patientsoperated on Tuesday through Friday, most will be readyfor discharge or hospitalized over the weekend. As a re-sult of staff shortages and junior coverage, postoperativecomplications may be missed, rehabilitation services notadequate, or discharge planning not ready for execution.A full complement of the multidisciplinary team allowsthe prompt management of comorbidities, potential com-plications, and availability of consult services if needed.In addition to the surgical staff, ancillary services ofwound and ostomy care, physical therapy, and dischargeplanning play a significant role in patient care. Weekendshortages of these staff members may lead to decreasedrehabilitative services and discharge planning needed foroptimal postoperative care.
Experienced surgeons and staff members are betterprepared to deal with more complicated patients and ensurecare and timely discharge. If early complications are noted,specialist services such as interventional radiology andcardiology may not be readily available for immediateconsultation over the weekend, leading to delays in

344 The American Journal of Surgery, Vol 206, No 3, September 2013
treatment. This is evident in the fact that multiple comor-bidities and complications noted in this study had asignificantly shorter increased length of stay for surgeryperformed on Monday compared with the rest of the week.The more trained health care professionals involved havethe ability to aid in recovery and also the early recognitionof postoperative complications normally seen on postoper-ative days 2 to 5. For cases performed on Monday, thisallows more experienced staff members to discover thecomplications. For patients undergoing procedures later inthe week, complications may occur over the weekend,leading to delays in both recognition and treatment sec-ondary to junior staffing and decreased staffing of consultservices.
Each member of the multidisciplinary team is subject tothe effects of sleep deprivation and fatigue as the workweek progresses, potentially affecting patient outcomes.Multiple studies have reported the detrimental effect ofcase load and fatigue on patient outcomes.1,2 These reportshave led to the adoption of work-hour restrictions by theAccreditation Council for Graduate Medical Educa-tion.19,20 Increasing work-hour restrictions have, in turn, in-creased the number of transitions of care, leading tocommunication errors and inadequate clinical care, necessi-tating the need for structured care transitions.21–26 Morefrequent care transitions have the potential of delayed pa-tient care, leading to increased length of stay. Althoughthis phenomenon was not directly examined in this study,previous studies21–26 have demonstrated this effect andmay have contributed to our results. For patients in the re-covery period, the effects of fatigue, sleep deprivation, andincreased transitions may lead to suboptimal care as earlypostoperative complications are missed and proper rehabil-itation is underused. As a result, patient care may becompromised.
Reviewing the results of this study, we can concludesurgery on Monday is an independent predictive factor fordecreased length of stay. This difference may be due to thefull availability of multidisciplinary resources for patientsundergoing surgery early in the week. Our data supportpreviously published data in surgical, anesthesia, and med-ical journals regarding timing effects of patient care. Each ofthese previously reported studies identified a number ofpotential influences on patient outcomes, including sleepdeprivation, fatigue, case load, time of day, and day of theweek. Weekend effects of staffing shortages and juniormembers of the teammay account for some of the disparitiesseen in patient outcomes. For colectomies performed onMonday, limiting weekend hospitalization may decreaselength of stay by concentrating resources in the immediatepostoperative period. A similar decrease in length of staymay not be seen on any other day, because of delayeddischarge home over the weekend or suboptimal delivery ofhospital resources as the week progresses secondary tofatigue or weekend shortages of all hospital staff members.In an era of diminishing means, hospital resources becomefinite budgets not immune to the economic uncertainties of
society. In the future, our goal will be to identify theresources that influence length of stay so that they can beevenly applied throughout the week.
References
1. Kelz RR, Tran TT, Hosokawa P, et al. Time-of-day effects on surgical
outcomes in the private sector: a retrospective cohort study. J Am Coll
Surg 2009;209:434–45.
2. Wright MC, Phillips-Bute B, Mark JB, et al. Time of day effects on the
incidence of anesthesic adverse events. Qual Saf Health Care 2006;15:
258–63.
3. Zare MM, Itani KM, Schiffiner TL, et al. Mortality after nonemergent
major surgery performed on Friday versus Monday through Wednes-
day. Ann Surg 2007;246:866–74.
4. Magid DJ, Wang Y, Herrin J, et al. Relationship between time of day,
day of week, timeliness of reperfusion, and in-hospital mortality for
patients with acute ST-segment elevation myocardial infarction.
JAMA 2005;294:803–12.
5. Saposnik G, Baibergenova A, Bayer N, et al. Weekends: a dangerous
time for having a stroke? Stroke 2007;38:1211–5.
6. Fogelholm R, Murros K, Rissnaen A, et al. Factors delaying hospital
admission after acute stroke. Stroke 1996;27:398–400.
7. O’Leary KJ, Sehgal NL, Terrell G, et al, for the High Performance
Teams and the Hospital of the Future Project Team. Interdisciplinary
teamwork in hospitals: A review and practical recommendations for
improvement. J Hosp Med. http://dx.doi.org/10.1002/jhm.970. [Epub
ahead of print].
8. Meterko M, Mohr DC, Young GJ. Teamwork culture and patient sat-
isfaction in hospitals. Med Care 2004;42:492–8.
9. Curtis JR, Cook DJ, Wall RJ, et al. Intensive care unit quality improve-
ment: a ‘‘how-to’’ guide for the interdisciplinary team. Crit Care Med
2006;34:211–8.
10. Needleman J, Buerhaus PB, Mattke S, et al. Nurse-staffing levels and
the quality of care in hospitals. N Engl J Med 2002;346:1715–22.
11. Wunsch H, Mapstone J, Brady T, et al. Hospital mortality associated
with day and time of admission to intensive care units. Intensive
Care Med 2004;30:895–901.
12. Arabi Y, Alshimemeri A, Taher S. Weekend and weeknight admissions
have the same outcome of weekday admissions to an intensive care
unit with onsite intensivist coverage. Crit Care Med 2006;34:605–11.
13. Remzi FH, Kirat HT, Kaouk JH, et al. Single-port laparoscopy in co-
lorectal disease. Colorectal Dis 2008;10:823–6.
14. Boni L, Dionigi G, Cassinotti E, et al. Single incision laparoscopic
right colectomy. Surg Endosc 2010;24:3233–6.
15. Merchant AM, Lin E. Single-incision laparoscopic right hemicolec-
tomy for a colon mass. Dis Colon Rectum 2009;52:1021–4.
16. Law W, Fan J, Poon J. Single-incision laparoscopic colectomy: early
experience. Dis Colon Rectum 2010;53:284–8.
17. Ramos-Valadez DI, Patel CB, Ragupathi M, et al. Single-incision lap-
aroscopic right hemicolectomy: safety and feasibility in a series of
consecutive cases. Surg Endosc 2010;24:2613–6.
18. Thompson JS, Baxter BT, Allison JG, et al. Temporal patterns of post-
operative complications. Arch Surg 2003;138:596–603.
19. Biller CK, Antonacci AC, Pelletier S, et al. The 80-hour work guide-
lines and resident survey perceptions of quality. J Surg Res 2006;135:
275–81.
20. Accreditation Council for Graduate Medical Education. Common pro-
gram requirements. Available at: http://www.acgme-2010standards.
org/pdf/Common_Program_Requirements_07012011.pdf. Accessed
March 20, 2012.
21. Manjunath A, Srirangam SJ. Risks of working time directive. Shorter
shifts and more frequent handover. BMJ 2010;341:c4858.
22. Taubert M, Nelson A. Out-of-hours GPs and palliative careda quali-
tative study exploring information exchange and communication
issues. BMC Palliat Care 2010;9:18.

D.M. Gilmore et al. Early Week Surgery Decreases LOS 345
23. Pezzolesi C, Schifano F, Pickles J, et al. Clinical handover incident re-
porting in one UK general hospital. Int J Qual Health Care 2010;22:
396–401.
24. Sabir N, Yentis SM, Holdcroft A. A national survey of obstetric anaes-
thetic handovers. Anaesthesia 2006;61:376–80.
25. Ye K, McD Taylor D, Knott JC, et al. Handover in the emergency de-
partment: deficiencies and adverse effects. Emerg Med Australas
2007;19:433–41.
26. Adamski P. Implement a handoff communications approach. Nurs
Manage 2007;38:12.