time to psychiatric hospitalization in patients with bipolar disorder treated with a mood stabilizer...
TRANSCRIPT

Clinical Therapeutics/Volume 31, Number 4, 2009
836 Volume 31 Number 4
This work was presented at the 60th Annual Institute on Psychiatric Services, October 2–5, 2008, Chicago, Illinois, the Annual European Congress of the International Society for Pharmacoeconomics and Outcomes Research, November 8–11, 2008, Athens, Greece, and the World Psychiatric Association Congress, April 1–4, 2009, Florence, Italy.
Accepted for publication April 17, 2009.doi: 10.1016/j.clinthera.2009.04.0220149-2918/$ - see front matter
© 2009 Excerpta Medica Inc. All rights reserved.
ABSTRACTObjective: This study compared the time to psychi-
atric hospitalization in commercially insured patients with bipolar disorder who were treated with a mood stabilizer plus adjunctive aripiprazole versus adjunctive ziprasidone, olanzapine, quetiapine, or risperidone.
Methods: This was a retrospective, propensity score– matched cohort study using the Ingenix I3/LabRx in-tegrated insurance claims data set. Patients with bipolar disorder were included if they had ≥180 days of pre-index enrollment in the health plan without atypical antipsychotic exposure. Patients received mood stabi-lizers and subsequently received adjunctive atypical antipsychotic agents; they were then monitored for up to 90 days after the index antipsychotic prescription. The primary analysis was a Cox proportional hazards analysis to evaluate the time until psychiatric hospi-talization comparing adjunctive aripiprazole with ziprasidone, olanzapine, quetiapine, or risperidone after adjusting for age, sex, and preindex hospitaliza-tion.
Results: Adjunctive aripiprazole was associated with a longer time until hospitalization than adjunctive ziprasidone, olanzapine, quetiapine, or risperidone (hazard ratios 1.7, 1.6, 1.5, and 1.5, respectively; all, P < 0.05). Mean initial and maximum doses of all drugs were below those recommended by the package insert or clinical practice guidelines. Sensitivity analy-ses suggested the robustness of the results in the gen-eral population of patients with bipolar disorder re- cently treated with atypical antipsychotics.
Conclusions: This retrospective claims-data analy-sis suggests that in these adults with bipolar disorder treated with mood stabilizers, the addition of adjunc-tive aripiprazole was associated with a longer time to
hospitalization than adjunctive ziprasidone, olanza- pine, quetiapine, or risperidone during a 90-day fol-low-up period. (Clin Ther. 2009;31:836–848) © 2009 Excerpta Medica Inc.
Key words: bipolar disorder, adjunctive treatment, aripiprazole.
INTRODUCTIONBipolar disorder is a chronic, recurring disorder asso-ciated with periodic mood swings. The economic bur-den of bipolar disorder is substantial. Treatment costs are estimated at $7200 to $12,100 per year of which 20% is attributable to hospitalizations.1,2 Acute ma-nia is frequently a medical emergency requiring hospi-talization for behavioral control, rapid resolution of irritability and agitation, de-escalation of mood, and a decrease in risk-taking behavior. Patients who present with an acute episode require fast intervention to minimize hospitalization. Despite the availability of multiple efficacious medications, >75% of patients with bipolar disorder report ≥1 lifetime psychiatric hospitalization.3
Medication is an essential part of successful treat-ment for bipolar disorder. Recent prescription data indicate that 42% to 64% of patients with bipolar
Time to Psychiatric Hospitalization in Patients With Bipolar Disorder Treated With a Mood Stabilizer and Adjunctive Atypical Antipsychotics: A Retrospective Claims Database Analysis
Edward Kim, MD, MBA1; Ross Maclean, MD1; Diane Ammerman, PharmD1; Yonghua Jing, PhD1; Andrei Pikalov, MD, PhD2; Min You, MS1; Quynh Van-Tran, PharmD2; and Gilbert L’Italien, PhD3
1Bristol-Myers Squibb, Plainsboro, New Jersey; 2Otsuka America Pharmaceutical, Inc., Rockville, Maryland; and 3Bristol-Myers Squibb, Wallingford, Connecticut

April 2009 837
E. Kim et al.
through December 31, 2006. The data set is a propri-etary sample of individuals receiving health insurance benefits from United Health Care (UHC). UHC data include the inpatient, outpatient, and prescription drug claims of >15 million covered lives across the United States.
Patients were monitored for up to 90 days after the index date for psychiatric hospitalization, medical hospitalization, discontinuation of the index atypical antipsychotic, and prescription of a nonindex atypical antipsychotic during the follow-up period. The index date was the date of the first prescription claim for an adjunctive atypical antipsychotic.
Inclusion CriteriaThe study included outpatients aged 18 to 65 years
with an International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)27 code for bipolar disorder (manic, mixed, or hypomanic [296.0x, 296.1, 296.4x, 296.6x, 296.7x, 296.8x]). Eligible patients were required to have continuous health-plan enrollment for ≥180 days before and ≥90 days after the index date, and a supply of mood stabilizer (lithium carbonate, carbamazepine, lamo- trigine, divalproex sodium, oxcarbazepine, or topira-mate) of ≥30 days before the index date. Patients were included if they were treated with a single atypical antipsychotic.
Exclusion CriteriaPatients were excluded from the analysis if they re-
sided in a nursing home, hospice, or another type of long-term care facility; received mail-order prescrip-tions; or were diagnosed with a schizophrenia spectrum disorder (295.xx) during the pre- or postindex study period. Patients were also excluded if they used any atypical antipsychotic during the 180-day preindex period or were hospitalized at the time of index pre-scription or within 7 days after the index prescription.
Assessments and Statistical AnalysesThe primary outcome of interest was the time to
first psychiatric hospitalization during the 90-day postindex follow-up period. Patients were censored for the following events: psychiatric hospitalization, medical hospitalization, discontinuation of the index antipsychotic (>15 days of gap in coverage), or pre-scription of a different antipsychotic during the follow- up period.
disorder receive traditional mood stabilizers, such as lithium, valproate, or carbamazepine, and 44% to 60% receive antipsychotic augmentation therapy.4–6 Antipsychotics are used increasingly in the treatment of bipolar disorder because of their properties as anti-manic or mood-stabilizing agents, coupled with favor-able tolerability profiles, compared with conventional agents.4,5 Updated treatment guidelines reflect this expanded role for atypical antipsychotics in the treat-ment of bipolar disorder.7,8 Severe manic episodes are typically treated with mood stabilizers in combination with atypical antipsychotics as a first-line treatment.7–11 For patients with milder symptoms, combination therapies are a second-line approach, but mood stabi-lizers augmented with atypical antipsychotics are com- monly used.7,12 Few data are available on the com-parative effectiveness of combined treatments with a mood stabilizer and atypical antipsychotic for the prevention of hospitalization in patients with bipolar disorder.13
Aripiprazole is an atypical antipsychotic with par-tial agonist activity at dopamine D2 and D3 recep-tors14–17 and serotonin 5-hydroxytryptamine (HT)1A receptors, and antagonist activity at 5-HT2A recep- tors.18,19 Aripiprazole has been approved for the treat-ment of manic and mixed episodes associated with bipolar I disorder, with or without psychotic features, in adults and in pediatric patients aged 10 to 17 years, as both monotherapy and adjunctive therapy to either lithium or valproate.20 In patients with an inadequate response to lithium or valproate, adjunctive aripipra-zole provided a greater improvement in mania symp-toms from week 1 to study end (week 6) compared with lithium or valproate alone.21 The safety and tolerabili- ty profile of adjunctive aripiprazole was similar to that observed in previous studies of aripiprazole mono- therapy in patients with bipolar mania.22–26
The objective of the present study was to compare the time to psychiatric hospitalization in commercially insured patients with bipolar disorder who were treated with a mood stabilizer plus adjunctive aripiprazole versus adjunctive ziprasidone, olanzapine, quetiapine, or risperidone.
PATIENTS AND METHODSStudy Design
This was a retrospective cohort study using the Ingenix I3/LabRx (Ingenix Health Intelligence, Salt Lake City, Utah) claims data set from January 1, 2003

838 Volume 31 Number 4
Clinical Therapeutics
and limited evidence of titration to maximum dose. Mean starting and maximum doses were as follows: ziprasidone, 90.3 and 100.2 mg/d; olanzapine, 9.3 and 10.2 mg/d; quetiapine, 147.0 and 169.8 mg/d; and risperidone, 1.6 and 1.8 mg/d. The mean starting and maximum daily doses of atypical antipsychotics after propensity score matching are presented in Table V. After matching, a lower postindex hospitalization rate was observed with aripiprazole (6.5% [28/431]) than with any of the other atypical antipsychotics (ziprasi-done, 10.2% [44/431]; olanzapine, 8.7% [60/690]; quetiapine, 8.5% [71/840]; and risperidone, 8.6% [71/829]) (Table VI).
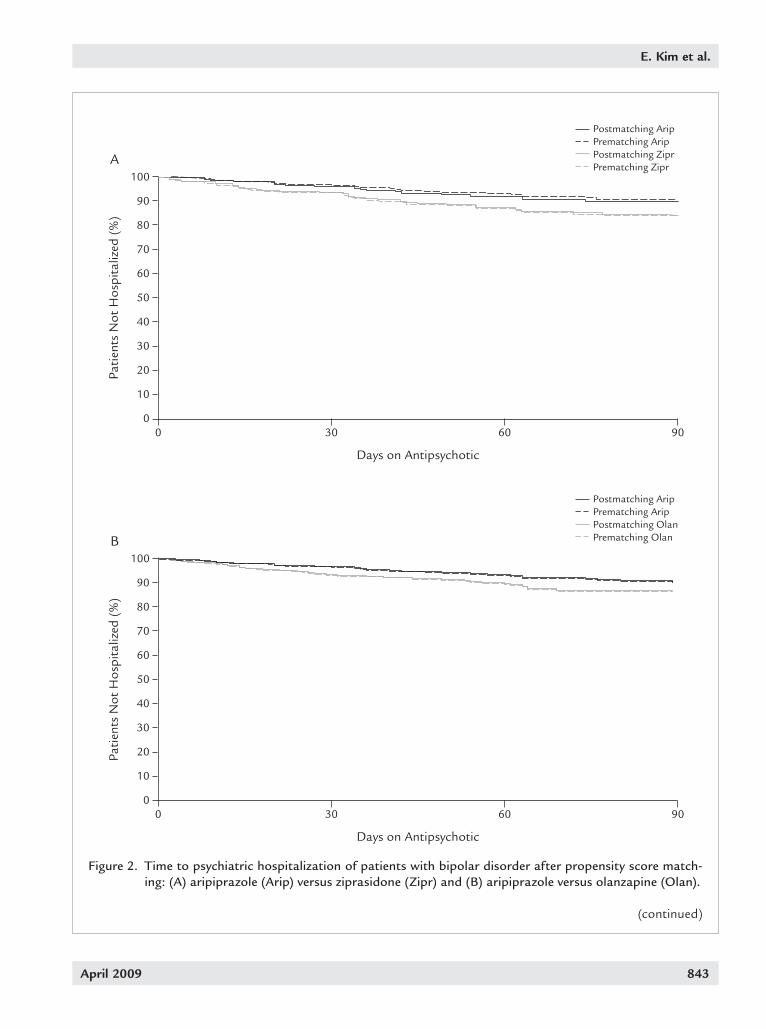
Regression AnalysesResults of the Cox proportional hazards regression
analyses indicated that, compared with aripiprazole, all the other atypical antipsychotics were associated with significantly shorter time to hospitalization (zip-rasidone: hazard ratio [HR] = 1.7; P = 0.04; olanza- pine: HR = 1.6; P = 0.03; quetiapine: HR = 1.5; P = 0.04; and risperidone: HR = 1.5; P = 0.04). Kaplan-Meier survival curves in Figure 2 demonstrate that adjunc-tive aripiprazole was associated with a longer time until hospitalization than adjunctive ziprasidone, olanza- pine, quetiapine, and risperidone.
Given the significant disparities between observed and label-recommended dosing, we conducted analy-ses within each treatment arm to compare “subthera-peutic” dosing (below the label-recommended dose) with “therapeutic” dosing (at or above the label- recommended dose). Because the labels of quetiapine, risperidone, and ziprasidone recommend either a start-ing dose and targeted dose for titration, or a dosing range, we compared the index dose with the recom-mended starting dose, and the maximum dose with the targeted dose, if applicable. For olanzapine and que-tiapine, a therapeutic starting dose was associated with a higher risk of hospitalization than a subthera-peutic starting dose (olanzapine: HR = 1.730; P = 0.01; quetiapine: HR = 1.371; P = 0.03). For risperidone, a therapeutic maximum dose was associated with a higher risk of hospitalization than a subtherapeutic maximum dose (HR = 1.780; P < 0.01) (Table VII). Subtherapeutic doses were not associated with higher risks of hospitalization in any treatment arm.
To assess the generalizability of the results, we con-ducted a sensitivity analysis beyond the prespecified propensity score–matched study sample. Cox propor-
The primary analysis was a Cox proportional haz-ards analysis assessing the time until postindex psy-chiatric hospitalization. Covariates for adjustment in the model included age, sex, diagnosis or treatment of diabetes or hyperlipidemia, preindex psychiatric hos-pitalization, preindex lipid or glucose laboratory claims, choice of preindex mood stabilizer, and Charl-son comorbidity index.
To control for treatment selection bias, we used propensity score matching to construct comparison groups that shared similar demographic and clinical characteristics. Propensity scores were calculated for every patient using logistic regression, with indepen-dent variables of age, sex, region, preindex diagnosis or treatment of diabetes or hyperlipidemia, preindex psychiatric hospitalization, preindex lipid or glucose laboratory claims, choice of preindex mood stabilizer, and Charlson comorbidity index. The propensity score was the predicted probability of treatment calculated for each patient in the regression model. Patients in comparison treatment groups were matched if their propensity scores were within 0.25 SD of the logit of the propensity score.
RESULTSPatient Disposition and Characteristics
Of 198,919 patients with at least 1 prescription for an atypical antipsychotic, 13,774 had bipolar dis- order, of whom 6162 met the full inclusion criteria (Figure 1). Of these, 840 patients were taking aripip-razole, 446 ziprasidone, 1101 olanzapine, 2501 que-tiapine, and 1274 risperidone. Propensity score match-ing allowed the matching of 431 aripiprazole and ziprasidone patients, 690 aripiprazole and olanzapine patients, 840 aripiprazole and quetiapine patients, and 829 aripiprazole and risperidone patients. Base-line characteristics before and after matching are shown in Tables I to IV. The results demonstrate that propensity score matching successfully eliminated significant baseline and preindex differences in all variables.
Duration of therapy with atypical antipsychotics was generally comparable across treatment groups, except that patients taking aripiprazole had longer therapy than those taking olanzapine (49.0 vs 43.4 days; P < 0.001) (Table V). Before propensity score match-ing, the mean starting dose of aripiprazole was 11.2 mg/d; the mean maximum dose was 12.4 mg/d. Most of the other atypical antipsychotics had low starting doses

April 2009 839
E. Kim et al.
Patients treated with atypical antipsychotics from 2003 through 2006 (the first episode of atypical antipsychotic treatment was used for the analysis)
(N = 198,919)
Patients(1) aged 18–65 years;
(2) not treated with clozapine;(3) without mail-order prescription; and
(4) 6 months preindex and 3 months postindex with continuous enrollment(n = 61,901)
Patients(1) without long-term care (nursing home or hospice); and
(2) without psychiatric hospitalization at index date or 7 days after index (n = 59,755)
Patients(1) with bipolar disorder; and
(2) without schizophrenia(n = 13,774)
Study Sample(1) total preindex mood stabilizer supply ≥30 days; and
(2) mood stabilizer claim during atypical antipsychotic treatment or within 30 days before atypical antipsychotic index date
(n = 6162)
Aripiprazole(n = 840)
Ziprasidone(n = 446)
Olanzapine(n = 1101)
Quetiapine(n = 2501)
Risperidone(n = 1274)
Figure 1. Flow of patients through the study of mood stabilizer plus atypical antipsychotics for bipolar disorder.

840 Volume 31 Number 4
Clinical Therapeutics
Table I. Baseline characteristics before and after propensity score matching for aripiprazole versus ziprasidone among patients being treated for bipolar disorder. Values are no. (%) unless otherwise indicated.
Before Propensity Score Match* After Propensity Score Match
Aripiprazole Ziprasidone Aripiprazole Ziprasidone Variable (n = 840) (n = 446) P (n = 431) (n = 431) P
Age, mean (SD), y 37.9 (11.5) 37.5 (10.9) 0.61 37.8 (11.5) 37.5 (11.0) 0.64Men 557 (66.3) 328 (73.5) 0.01 325 (75.4) 313 (72.6) 0.35Psychiatric hospitalization 232 (27.6) 193 (43.3) <0.01 178 (41.3) 179 (41.5) 0.95Preindex mood stabilizer exposure† Carbamazepine 44 (5.2) 32 (7.2) 0.16 26 (6.0) 28 (6.5) 0.80 Lamotrigine 300 (35.7) 143 (32.1) 0.19 147 (34.1) 142 (32.9) 0.72 Lithium 220 (26.2) 129 (28.9) 0.29 113 (26.2) 121 (28.1) 0.54 Oxcarbazepine 129 (15.4) 61 (13.7) 0.42 58 (13.5) 61 (14.2) 0.77 Topiramate 135 (16.1) 70 (15.7) 0.86 76 (17.6) 68 (15.8) 0.47 Valproate 285 (33.9) 143 (32.1) 0.50 146 (33.9) 142 (32.9) 0.77Charlson comorbidity index, mean (SD) 0.3 (0.8) 0.3 (0.8) 0.28 0.4 (0.9) 0.3 (0.8) 0.82
* Patients with ≥30 days of total mood stabilizer supply during the preindex time period and ≥1 mood stabilizer claim from 30 days before the index atypical antipsychotic date to hospitalization or the end of follow-up.
† Mood stabilizer claims were found during 30 days before the index date of atypical antipsychotic to hospitalization or the end of follow-up.
Table II. Baseline characteristics before and after propensity score matching for aripiprazole versus olanza- pine among patients being treated for bipolar disorder. Values are no. (%) unless otherwise indicated.
Before Propensity Score Match* After Propensity Score Match
Aripiprazole Olanzapine Aripiprazole Olanzapine Variable (n = 840) (n = 1101) P (n = 690) (n = 690) P
Age, mean (SD), y 37.9 (11.5) 38.7 (11.6) 0.13 38.5 (11.5) 38.6 (11.8) 0.98Men 557 (66.3) 606 (55.0) <0.01 431 (62.5) 409 (59.3) 0.23Psychiatric hospitalization 232 (27.6) 449 (40.8) <0.01 215 (31.2) 216 (31.3) 0.95Preindex mood stabilizer exposure†
Carbamazepine 44 (5.2) 65 (5.9) 0.53 41 (5.9) 45 (6.5) 0.66 Lamotrigine 300 (35.7) 205 (18.6) <0.01 189 (27.4) 196 (28.4) 0.67 Lithium 220 (26.2) 370 (33.6) <0.01 197 (28.6) 209 (30.3) 0.48 Oxcarbazepine 129 (15.4) 104 (9.4) <0.01 93 (13.5) 95 (13.8) 0.88 Topiramate 135 (16.1) 117 (10.6) <0.01 102 (14.8) 101 (14.6) 0.94 Valproate 285 (33.9) 502 (45.6) <0.01 270 (39.1) 250 (36.2) 0.27Charlson comorbidity index, mean (SD) 0.3 (0.8) 0.3 (0.9) 0.98 0.3 (0.8) 0.3 (0.8) 1.00
* Patients with ≥30 days of total mood stabilizer supply during the preindex time period and ≥1 mood stabilizer claim from 30 days before the index atypical antipsychotic date to hospitalization or the end of follow-up.
† Mood stabilizer claims were found during 30 days before the index date of atypical antipsychotic to hospitalization or the end of follow-up.

April 2009 841
E. Kim et al.
Table III. Baseline characteristics before and after propensity score matching for aripiprazole versus quetia- pine among patients being treated for bipolar disorder. Values are no. (%) unless otherwise indicated.
Before Propensity Score Match* After Propensity Score Match
Aripiprazole Quetiapine Aripiprazole Quetiapine Variable (n = 840) (n = 2501) P (n = 840) (n = 840) P
Age, mean (SD), y 37.9 (11.5) 37.4 (11.0) 0.26 37.9 (11.5) 37.8 (11.0) 0.87Men 557 (66.3) 1691 (67.6) 0.49 557 (66.3) 542 (64.5) 0.44Psychiatric hospitalization 232 (27.6) 895 (35.8) <0.01 232 (27.6) 233 (27.7) 0.96Preindex mood stabilizer exposure† Carbamazepine 44 (5.2) 136 (5.4) 0.82 44 (5.2) 53 (6.3) 0.35 Lamotrigine 300 (35.7) 773 (30.9) 0.01 300 (35.7) 297 (35.4) 0.88 Lithium 220 (26.2) 700 (28.0) 0.31 220 (26.2) 208 (24.8) 0.50 Oxcarbazepine 129 (15.4) 318 (12.7) 0.05 129 (15.4) 129 (15.4) 0.59 Topiramate 135 (16.1) 303 (12.1) <0.01 135 (16.1) 135 (16.1) 0.64 Valproate 285 (33.9) 928 (37.1) 0.10 285 (33.9) 285 (33.9) 0.84Charlson comorbidity index, mean (SD) 0.3 (0.8) 0.3 (0.8) 0.48 0.3 (0.8) 0.3 (0.7) 0.63
* Patients with ≥30 days of total mood stabilizer supply during the preindex time period and ≥1 mood stabilizer claim from 30 days before the index atypical antipsychotic date to hospitalization or the end of follow-up.
† Mood stabilizer claims were found during 30 days before the index date of atypical antipsychotic to hospitalization or the end of follow-up.
Table IV. Baseline characteristics before and after propensity score matching for aripiprazole versus risperi-done among patients being treated for bipolar disorder. Values are no. (%) unless otherwise indicated.
Before Propensity Score Match* After Propensity Score Match
Aripiprazole Risperidone Aripiprazole Risperidone Variable (n = 840) (n = 1274) P (n = 829) (n = 829) P
Age, mean (SD), y 37.9 (11.5) 37.1 (11.5) 0.15 37.8 (11.4) 37.6 (11.4) 0.69Men 557 (66.3) 800 (62.8) 0.10 550 (66.3) 546 (65.9) 0.84Psychiatric hospitalization 232 (27.6) 442 (34.7) <0.01 232 (28.0) 236 (28.5) 0.83Preindex mood stabilizer exposure† Carbamazepine 44 (5.2) 62 (4.9) 0.70 43 (5.2) 40 (4.8) 0.74 Lamotrigine 300 (35.7) 318 (25.0) <0.01 290 (35.0) 295 (35.6) 0.80 Lithium 220 (26.2) 359 (28.2) 0.32 218 (26.3) 227 (27.4) 0.62 Oxcarbazepine 129 (15.4) 165 (13.0) 0.12 127 (15.3) 132 (15.9) 0.74 Topiramate 135 (16.1) 152 (11.9) 0.01 132 (15.9) 132 (15.9) 1.00 Valproate 285 (33.9) 550 (43.2) <0.01 284 (34.3) 271 (32.7) 0.50Charlson comorbidity index, mean (SD) 0.3 (0.8) 0.3 (0.9) 0.51 0.3 (0.8) 0.3 (0.8) 0.81
* Patients with ≥30 days of total mood stabilizer supply during the preindex time period and ≥1 mood stabilizer claim from 30 days before the index atypical antipsychotic date to hospitalization or the end of follow-up.
† Mood stabilizer claims were found during 30 days before the index date of atypical antipsychotic to hospitalization or the end of follow-up.

842 Volume 31 Number 4
Clinical Therapeutics
cantly different. In the excluded sample and the total sample of patients with bipolar disorder receiving atypi-cal antipsychotics, aripiprazole was associated with a significantly lower risk of hospitalization in the follow-up period than all comparators.
To assess the impact of censoring based on discon-tinuation of the index antipsychotic, we conducted an intention-to-treat analysis that eliminated gaps in therapy as a censoring event. This analysis indicated that, compared with aripiprazole, all the other anti- psychotics were associated with a significantly greater risk of hospitalization (ziprasidone: HR = 1.6; P = 0.05; olanzapine: HR = 1.7; P = 0.01; quetiapine: HR = 1.4;
tional hazards regression models were fitted using the same covariates for adjustment as were used in the original propensity score matching. We conducted these analyses on the entire study sample (n = 6162), the bipolar sample that was excluded (n = 7612), and all bipolar patients receiving atypical antipsychotics who met the diagnostic and enrollment inclusion criteria, regardless of whether they were or were not receiving concomitant mood stabilizers (n = 13,774). The re-sults, summarized in Table VIII, indicate consistent directional relationships favoring aripiprazole across all samples. In the unmatched study sample, compari-sons with olanzapine and quetiapine were not signifi-
Table V. Duration of therapy and dosing of atypical antipsychotics after propensity score matching among patients being treated for bipolar disorder Data are expressed as mean (SD).
Match Days on Therapy Starting Dose Maximum Dose
Ziprasidone vs aripiprazole (n = 431) Ziprasidone 46.2 (27.6) 89.6 (54.0) 99.7 (55.6) Aripiprazole 47.1 (27.6) 11.7 (7.4) 13.1 (7.9)
Olanzapine vs aripiprazole (n = 690) Olanzapine 43.4 (25.9) 8.7 (6.1) 9.8 (8.3) Aripiprazole 49.0 (28.0)* 11.4 (6.9) 12.7 (7.5)
Quetiapine vs aripiprazole (n = 840) Quetiapine 47.5 (28.2) 138.9 (147.5) 161.3 (166.9) Aripiprazole 48.3 (27.7) 11.2 (7.0) 12.4 (7.4)
Risperidone vs aripiprazole (n = 829) Risperidone 48.6 (28.0) 1.5 (1.3) 1.7 (1.4) Aripiprazole 48.3 (27.7) 11.2 (7.0) 12.4 (7.5)
*P < 0.001.
Table VI. Hospitalization rates after treatment with atypical antipsychotics among patients with bipolar disorder.
Before Match After Match
Atypical Patients, Hospitalizations, Patients, Hospitalizations, Treatment Antipsychotic No. (%) No. (%) No. (%) No. (%) to Match
Aripiprazole 840 49 (5.8) 431 28 (6.5) ZiprasidoneZiprasidone 446 47 (10.5) 431 44 (10.2) AripiprazoleOlanzapine 1101 102 (9.3) 690 60 (8.7) AripiprazoleQuetiapine 2501 219 (8.8) 840 71 (8.5) AripiprazoleRisperidone 1274 124 (9.7) 829 71 (8.6) Aripiprazole
April 2009 843
E. Kim et al.
0
Patie
nts
Not
Hos
pita
lized
(%
)
30 600 90
Days on Antipsychotic
Postmatching AripPrematching AripPostmatching ZiprPrematching Zipr
100
50
40
30
20
10
60
70
80
90
A
Postmatching AripPrematching AripPostmatching OlanPrematching Olan
0
Patie
nts
Not
Hos
pita
lized
(%
)
30 600 90
Days on Antipsychotic
100
50
40
30
20
10
60
70
80
90
B
Figure 2. Time to psychiatric hospitalization of patients with bipolar disorder after propensity score match-ing: (A) aripiprazole (Arip) versus ziprasidone (Zipr) and (B) aripiprazole versus olanzapine (Olan).
(continued)

844 Volume 31 Number 4
Clinical Therapeutics
Postmatching AripPrematching AripPostmatching QuetPrematching Quet
0
Patie
nts
Not
Hos
pita
lized
(%
)
30 600 90
Days on Antipsychotic
100
50
40
30
20
10
60
70
80
90
C
Postmatching AripPrematching AripPostmatching RispPrematching Risp
0
Patie
nts
Not
Hos
pita
lized
(%
)
30 600 90
Days on Antipsychotic
100
50
40
30
20
10
60
70
80
90
D
Figure 2 (continued). Time to psychiatric hospitalization of patients with bipolar disorder after propensity score matching: (C) aripiprazole versus quetiapine (Quet) and (D) aripiprazole versus risperidone (Risp).

April 2009 845
E. Kim et al.
In this retrospective cohort study of patients with bipolar disorder initially treated with mood stabiliz-ers, adjunctive aripiprazole was associated with a longer time until and lower risk of hospitalization than adjunctive ziprasidone, olanzapine, quetiapine, or risperidone. Duration of therapy was generally comparable across all atypical antipsychotics in this study, except for the comparison of aripiprazole ver-sus olanzapine. However, the doses of atypical anti- psychotics used tended to be lower than the recom-mended doses. The mean starting dose of aripiprazole was 11.2 mg/d, and the mean maximum dose was 12.4 mg/d. These doses of aripiprazole are lower than the 15- and 30-mg doses used in an outpatient clinical trial of aripiprazole as adjunctive therapy to lithium or valproate.21 Most of the other atypical antipsy-
P = 0.05; and risperidone: HR = 1.6; P = 0.01). The results of this sensitivity analysis are consistent with our primary findings.
DISCUSSIONIn patients with bipolar disorder, manic and mixed episodes are disruptive and may necessitate hospitali-zation when impulsive behaviors may be dangerous to the patient or to others.28 Thus, in outpatient settings, physicians must initiate treatments that are rapid and effective to decrease the risk of hospitalization. Com-binations of an atypical antipsychotic and mood sta-bilizer are recommended as first-line treatment for severe manic or mixed episodes, or as second-line treatment in patients with an inadequate response to a mood stabilizer alone.7
Table VII. Cox regression results for time to hospitalization by antipsychotic dose within treatment arm among patients being treated for bipolar disorder.*
Therapeutic vs Subtherapeutic (Starting Dose; Targeted Dose) HR P HR P
Aripiprazole (≥15 mg; NA) 1.157 0.64 NA NAZiprasidone (≥80 mg; ≥160 mg) 0.666 0.20 1.451 0.30Olanzapine (≥10 mg; NA) 1.730 0.01 NA NAQuetiapine (≥100 mg; ≥400 mg) 1.371 0.03 0.860 0.47Risperidone (≥2 mg; ≥3 mg) 1.230 0.27 1.780 <0.01
HR = hazard ratio; NA = not applicable.*A subtherapeutic dose is the reference.
Starting Dose Maximum Dose
Table VIII. Cox regression of sensitivity analysis for time to hospitalization in unmatched cohorts of patients with bipolar disorder receiving antipsychotic treatment.*
Study Sample Excluded Sample Total Sample (n = 6162) (n = 7612) (n = 13,774)
Comparator HR P HR P HR P
Ziprasidone 1.589 0.03 2.156 <0.00 1.877 <0.01Olanzapine 1.458 >0.05 1.911 <0.01 1.739 <0.01Quetiapine 1.340 0.07 2.138 <0.01 1.714 <0.01Risperidone 1.602 <0.01 1.999 <0.01 1.812 <0.01
HR = hazard ratio. *Aripiprazole is the reference.

846 Volume 31 Number 4
Clinical Therapeutics
lipid testing. However, if such colinearity resulted in model overspecification, the results would be biased toward the null hypothesis and would, at worst, reduce the estimate of aripiprazole’s effect on time to hospitali-zation. Finally, the study sample consisted of less than half of all patients with bipolar disorder taking atypical antipsychotics. Our intent was to study a population at high risk of hospitalization. Guo et al13 noted that, compared with patients taking mood stabilizers alone, those taking atypical antipsychotics were 44% more likely to be hospitalized, whereas those taking combi-nations of mood stabilizers and atypical antipsychotics were 61% more likely to be hospitalized. Thus, these observations suggest that the patient population in this study receiving adjunctive atypical antipsychotics and mood stabilizers had a high risk of hospitalization. However, our sensitivity analysis indicated similar re-sults for the entire population of bipolar patients taking atypical antipsychotics with or without mood stabiliz-ers, which may indicate that atypical antipsychotics are prescribed for patients with a more severe symptom profile. We did not perform propensity score matching or dosing analyses for those samples because that was beyond the scope of this study, but the results suggest that the differential acute benefits of aripiprazole in delaying hospitalization appear robust and consistent.
CONCLUSIONSIn these adults with bipolar disorder treated with mood stabilizers, the addition of adjunctive aripiprazole was associated with a longer time to hospitalization than adjunctive treatment with ziprasidone, olanzapine, que-tiapine, or risperidone during a 90-day follow-up peri-od. The results of the sensitivity analysis suggest that this effect may be generalizable to patients with bipolar disorder newly started on atypical antipsychotics with or without adjunctive pharmacotherapy.
ACKNOWLEDGMENTSThis study was supported by Bristol-Myers Squibb (Princeton, New Jersey) and Otsuka Pharmaceutical Co., Ltd. (Tokyo, Japan). Editorial support for the preparation of this manuscript was provided by Ogilvy Healthworld Medical Education; funding was provided by Bristol-Myers Squibb.
REFERENCES 1. Simon GE, Unützer J. Health care utilization and costs
among patients treated for bipolar disorder in an insured
chotics also had low mean starting doses and limited evidence of titration. These observations suggest that in real-world clinical practice, dosing of atypical an-tipsychotics may differ from that recommended in the product labels. This possibility is supported by other reports on the use of atypical antipsychotics to treat both schizophrenia and bipolar disorder.29 The find-ings from the present analysis may reflect differences in tolerability of antipsychotics among patients with bipolar disorder in a commercially insured popula-tion. Moreover, the observation that higher doses were associated with a greater risk of shorter time to hospitalization in some comparator arms suggests that these higher doses were used for more severely ill patients. Although we are not able to determine the reasons for these observations, it is possible that phy-sicians had concerns about tolerability or safety and were therefore reluctant to start patients on doses that were more efficacious unless those patients were ex-tremely unstable, in which case they already had a very high risk of hospitalization.
Observational studies such as ours provide an im-portant source of information on potential outcomes with specific therapies in settings where dosing, titra-tion, and concomitant medications are not constrained by trial protocols. Such studies evaluate the effective-ness of treatments that physicians have selected, wheth-er or not those treatments are deemed appropriate with respect to dosing or titration.
This short-term study has several limitations. Be-cause the analysis was based on a claims database, in-formation on adverse events was not available. As a nonrandomized retrospective study of observational data, it is possible that despite the use of propensity score matching, unobserved treatment selection bias may have contributed to the outcomes. In addition, the data set consists of patients from a single commercial health plan, and the results may not be generalizable to patients with more chronic psychiatric illness that are more likely to be covered by public-sector payers. Dos-ing of study medications was not consistent with the ranges recommended by the product labels or clinical guidelines, and that may have contributed to the re-sults. We decided to allow the full range of adjunctive dosing because we assumed that, once physicians have selected a treatment, they also selected what they be-lieved was the most appropriate dosing and titration for that medication. Some of the covariates might be highly correlated, such as hyperlipidemia and preindex

April 2009 847
E. Kim et al.
man 5-HT1A receptor. Eur J Phar- macol. 2002;441:137–140.
20. Abilify (aripiprazole) [prescribing information]. Princeton, NJ: Bristol-Myers Squibb/Otsuka America Phar- maceutical Inc; 2008. http://www.abilify.com/pdf/pi.aspx. Accessed April 4, 2009.
21. Vieta E, T’joen C, McQuade RD, et al. Efficacy of adjunctive aripiprazole to either valproate or lithium in bipolar mania patients partially nonrespon-sive to valproate/lithium monothera-py: A placebo-controlled study. Am J Psychiatry. 2008;165:1316–1325.
22. Vieta E, Bourin M, Sanchez R, et al, for the Aripiprazole Study Group. Effectiveness of aripiprazole v. halo-peridol in acute bipolar mania: Double-blind, randomised, com-parative 12-week trial. Br J Psychia-try. 2005;187:235–242.
23. Keck PE Jr, Marcus R, Tourkodimi-tris S, et al, for the Aripiprazole Study Group. A placebo-controlled, double-blind study of the efficacy and safety of aripiprazole in pa-tients with acute bipolar mania. Am J Psychiatry. 2003;160:1651–1658.
24. Sachs G, Sanchez R, Marcus R, et al, for the Aripiprazole Study Group. Aripiprazole in the treatment of acute manic or mixed episodes in patients with bipolar I disorder: A 3-week placebo-controlled study. J Psychopharmacol. 2006;20:536–546.
25. Keck PE Jr, Calabrese JR, McQuade RD, et al, for the Aripiprazole Study Group. A randomized, double-blind, placebo-controlled 26-week trial of aripiprazole in recently man-ic patients with bipolar I disorder. J Clin Psychiatry. 2006;67:626–637.
26. Keck PE Jr, Calabrese JR, McIntyre RS, et al, for the Aripiprazole Study Group. Aripiprazole monotherapy for maintenance therapy in bipolar I disorder: A 100-week, double-blind study versus placebo. J Clin Psychia-try. 2007;68:1480–1491.
27. International Classification of Diseases, Ninth Revision, Clinical Modification. http://icd9cm.chrisendres.com/
10. Grunze H, Kasper S, Goodwin G, et al, for the WFSBP Task Force on Treatment Guidelines for Bipolar Disorders. The World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for the Biologi-cal Treatment of Bipolar Disorders, Part II: Treatment of Mania. World J Biol Psychiatry. 2003;4:5–13.
11. Yatham LN. Atypical antipsychotics for bipolar disorder. Psychiatr Clin North Am. 2005;28:325–347.
12. Bowden CL. Making optimal use of combination pharmacotherapy in bipolar disorder. J Clin Psychiatry. 2004;65(Suppl 15):21–24.
13. Guo JJ, Keck PE Jr, Li H, et al. Treat-ment costs and health care utiliza-tion for patients with bipolar dis- order in a large managed care population. Value Health. 2008;11: 416–423.
14. Shapiro DA, Renock S, Arrington E, et al. Aripiprazole, a novel atypical antipsychotic drug with a unique and robust pharmacology. Neuro- psychopharmacology. 2003;28:1400– 1411.
15. Burris KD, Molski TF, Xu C, et al. Aripiprazole, a novel antipsychotic, is a high-affinity partial agonist at human dopamine D2 receptors. J Pharmacol Exp Ther. 2002;302:381– 389.
16. Tadori Y, Miwa T, Tottori K, et al. Aripiprazole’s low intrinsic activities at human dopamine D2L and D2S receptors render it a unique anti- psychotic. Eur J Pharmacol. 2005;515: 10–19.
17. Tadori Y, Forbes RA, McQuade RD, Kikuchi T. Characterization of ari- piprazole partial agonist activity at human dopamine D3 receptors. Eur J Pharmacol. 2008;597:27–33.
18. Jordan S, Koprivica V, Dunn R, et al. In vivo effects of aripiprazole on cortical and striatal dopaminergic and serotonergic function. Eur J Pharmacol. 2004;483:45–53.
19. Jordan S, Koprivica V, Chen R, et al. The antipsychotic aripiprazole is a potent, partial agonist at the hu-
population. Psychiatr Serv. 1999;50:1303–1308.
2. Stender M, Bryant-Comstock L, Phillips S. Medical resource use among patients treated for bipolar disorder: A retrospective, cross- sectional, descriptive analysis. Clin Ther. 2002;24:1668–1676.
3. Lish JD, Dime-Meenan S, Whybrow PC, et al. The National Depressive and Manic-depressive Association (DMDA) survey of bipolar mem-bers. J Affect Disord. 1994;31:281– 294.
4. Li J, McCombs JS, Stimmel GL. Cost of treating bipolar disorder in the California Medicaid (Medi-Cal) program. J Affect Disord. 2002;71: 131–139.
5. Blanco C, Laje G, Olfson M, et al. Trends in the treatment of bipolar disorder by outpatient psychiatrists. Am J Psychiatry. 2002;159:1005– 1010.
6. Guo JJ, Keck PE Jr, Corey-Lisle PK, et al. Risk of diabetes mellitus associ-ated with atypical antipsychotic use among patients with bipolar disor-der: A retrospective, population-based, case-control study. J Clin Psychiatry. 2006;67:1055–1061.
7. American Psychiatric Association. Practice guideline for the treatment of patients with bipolar disorder (revision). Am J Psychiatry. 2002;159 (Suppl):1–50.
8. Suppes T, Dennehy EB, Hirschfeld RM, et al, for the Texas Consensus Conference Panel on Medication Treatment of Bipolar Disorder. The Texas implementation of medica-tion algorithms: Update to the al-gorithms for treatment of bipolar I disorder. J Clin Psychiatry. 2005;66: 870–886.
9. Goodwin GM, for the Consensus Group of the British Association for Psychopharmacology. Evidence-based guidelines for treating bipo-lar disorder: Recommendations from the British Association for Psycho- pharmacology. J Psychopharmacol. 2003; 17:149–173; discussion 147.

848 Volume 31 Number 4
Clinical Therapeutics
icd9cm/index.php. Accessed April 17, 2009.
28. Najt P, Perez J, Sanches M, et al. Impulsivity and bipolar disorder. Eur Neuropsychopharmacol. 2007;17: 313–320.
29. Citrome L, Reist C, Palmer L, et al. Dose trends for second-generation antipsychotic treatment of schizo-phrenia and bipolar disorder. Schizophr Res. 2009;108:238–244.
Address correspondence to: Edward Kim, MD, MBA, Health Economic and Outcomes Research, Bristol-Myers Squibb, 777 Scudders Mill Road, Plainsboro, NJ 08536. E-mail: [email protected]