threshold tracking pacing based on beat by beat evoked response detection: clinical benefits and...
TRANSCRIPT

Journal of Interventional Cardiac Electrophysiology 4, 511±522(2000)
#2000 Kluwer Academic Publishers. Manufactured in The Netherlands.
Threshold Tracking Pacing Based on Beat by Beat EvokedResponse Detection: Clinical Bene®ts and Potential Problems
Fi�rat Duru1, Urs Bauersfeld2, Hans SchuÈ ller3, andReto Candinas1
1Cardiac Arrhythmia Unit, University Hospital of Zurich;2University Children's Hospital, Zurich, Switzerland;3University of Lund, Sweden
Abstract. Continuous monitoring of pacemaker stimu-lation thresholds and automatic adjustment of pace-maker outputs were among the longstanding goals ofthe pacing community. The ®rst clinically successfulimplementation of threshold tracking pacing was theAutocapture feature which has accomplished auto-matic ventricular capture veri®cation for every singlestimulus by monitoring the Evoked Response (ER)signal resulting from myocardial depolarization. TheAutocapture feature not only decreases energyconsumption by keeping the stimulation outputslightly above the actual threshold, but also increasespatient safety by access to high-output back-up pulsesif there is loss of capture. Furthermore, it providesvaluable documentation of stimulation thresholdsover time and serves as a valuable research tool.Current limitations for its widespread use include therequirements for implantation of bipolar low polariza-tion leads and unipolar pacing in the ventricle.Fusion=pseudofusion beats with resultant insuf®cientor even non-existent ER signal amplitudes followed byunnecessary delivery of back-up pulses and a possibleincrease in pacemaker output is not an uncommonobservation unique to the Autocapture feature. Therecent incorporation of the Autocapture algorithm indual chamber pacemakers has been challengingbecause of more frequent occurrence of fusion=pseudo-fusion beats in the presence of normal AV conduction.Along with a review of the previously published studiesand our clinical experience, this article discusses theclinical advantages and potential problems of Autocap-ture.
Key Words. pacemaker, threshold tracking, Auto-capture, evoked response, threshold search
Introduction
Since the introduction of permanent pacing in1958, a pacemaker output setting that providesconsistent capture with an adequate safetymargin remains to be the most importantelement of pacemaker treatment. Ideally, a pace-maker should run at the minimum output thatwill provide maximum pulse generator longevity
without compromising safety. To reach this goal,the issue of threshold tracking pacemakers wasraised by Funke, Preston and Mugica in the1970s [1±5]. Following these early attempts,several techniques have been described in aneffort to identify ventricular capture or its conse-quences [6±12]. However, the ®rst clinicallysuccessful implementation of threshold trackingpacing was the Autocapture feature (PacesetterMicrony, Solna, Sweden) in 1994. The thresholdtracking feature present in this world's smallestpulse generator (12.8 grams) has enabled captureveri®cation on a beat-by-beat basis by sensing thepaced Evoked Response (ER) signal with apredicted mean service life-span of approximatelyseven years. This energy saving feature was laterincorporated into the Regency family of pace-makers (VVIR) which provided many clinicalbene®ts [13±16]. More recently, Autocapture hasbecome available in a dual chamber pacemakersystem (Af®nity DR, and a subsequent modelÐentity) and its clinical feasibility has beendemonstrated [17].
Evoked Response and Polarization SignalsThreshold tracking pacing is based on an accu-rate detection of the ER signal to determinewhether or not a pacemaker stimulus hascaptured the myocardium [18]. The ER signaloccurs as a result of cardiac depolarization andits peak amplitude can be in the range of 5±30 mVfollowing the pacing stimulus [12]. Detection ofan ER signal requires a special sensing windowthat has a different set of ®lters as compared tothe usual sensing circuit for the intrinsic ventri-cular depolarization.
511
Address for correspondence: Firat Duru, M.D., CardiacArrhythmia Unit, University Hospital of Zurich, RaÈmistr.100, Zurich, CH-8091, Switzerland. E-mail: ®[email protected]
Received 25 February 2000; accepted 21 June 2000
Following a pacemaker stimulus, polarizationsignals always occur, even in the absence ofmyocardial depolarization, due to charging ofthe Helmholtz capacitor at the lead-myocardiuminterface. Accurate detection of the ER signalwhile precluding detection of polarization signalsafter the pacemaker stimulus is a prerequisite forappropriate function of Autocapture pacingsystems [19]. Occasionally, the amplitude of thepolarization signal may be very high, approach-ing or even extending above the amplitude of theER signal and persist for a considerable timeafter the pacemaker stimulus, resulting in falseER detection (Polarization oversensing). The useof a low polarization lead and the blanking periodfollowing the ventricular output should effec-tively preclude the detection of the polarizationsignal.
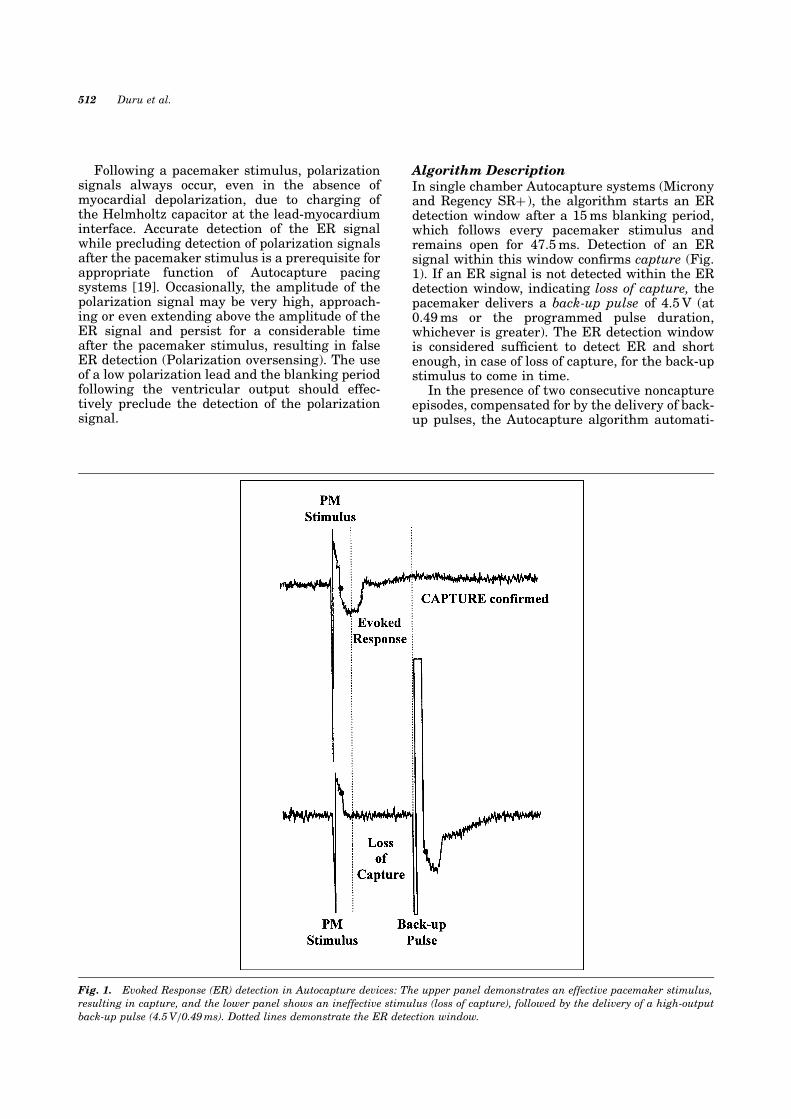
Algorithm DescriptionIn single chamber Autocapture systems (Micronyand Regency SR� ), the algorithm starts an ERdetection window after a 15 ms blanking period,which follows every pacemaker stimulus andremains open for 47.5 ms. Detection of an ERsignal within this window con®rms capture (Fig.1). If an ER signal is not detected within the ERdetection window, indicating loss of capture, thepacemaker delivers a back-up pulse of 4.5 V (at0.49 ms or the programmed pulse duration,whichever is greater). The ER detection windowis considered suf®cient to detect ER and shortenough, in case of loss of capture, for the back-upstimulus to come in time.
In the presence of two consecutive noncaptureepisodes, compensated for by the delivery of back-up pulses, the Autocapture algorithm automati-
Fig. 1. Evoked Response (ER) detection in Autocapture devices: The upper panel demonstrates an effective pacemaker stimulus,resulting in capture, and the lower panel shows an ineffective stimulus (loss of capture), followed by the delivery of a high-outputback-up pulse (4.5 V=0.49 ms). Dotted lines demonstrate the ER detection window.
512 Duru et al.
cally starts a stimulation threshold search. Thelowest output level that results in two consecu-tive captures is considered to be the stimulationthreshold. Then, the pacemaker increases theoutput by 0.3 V (working margin) above themeasured threshold. A single ineffective pacingstimulus does not initiate a threshold search,since it is considered to be an intermittentcapture loss without need for permanent outputadjustment. In order to adapt to dynamic stimu-lation thresholds, and hence to avoid unnecessaryhigher outputs, the pacemaker automaticallyperforms threshold measurements every eighthours. When initiated, the device decreases theautomatic pulse amplitude by 0.3 V until twoconsecutive losses of capture occur. The auto-matic pulse amplitude is then increased by 0.3 Vuntil two consecutive captures are con®rmed. Thedevice ®nally sets the pulse amplitude at themeasured capture threshold plus a 0.3 V workingmargin to allow for minor threshold ¯uctuations.A stimulation threshold test can also be enabledby applying a magnet over the pacemaker or viathe programmer as a test sequence.
In dual chamber Autocapture systems (Af®nityDR), the algorithm functions similarly. However,in order to override intrinsic AV conductionduring capture veri®cation and thresholdsearch, a shortened AV delay (paced AV interval)of 50 ms and a shortened PV delay (sensed AVinterval) of 25 ms are used. Programmed AV=PVdelays are restored after the search is complete.In Af®nity DR, automatic pulse amplitudesdecrements are 0.25 V and increments are0.125 V. The working margin is 0.25 V above the
measured stimulation threshold, while the safetymargin is 4.5 V at 0.5 ms pulse duration (orgreater of previously programmed). Figure 2demonstrates an automatic threshold search inAf®nity DR pacemakers.
When the time indicates that a thresholdsearch should be initiated but the ventricularchannel is inhibited by intrinsic activity, thesearch is not performed in the VVI mode butremains pending and the eight-hour clock isreset. In the DDD mode, however, the thresholdsearch usually proceeds as scheduled sincepacing of the ventricle is assured by using ashortened AV=PV delay. If the intrinsic heartrate increases during a threshold search andoverrides the pacing rate, the threshold searchis suspended and resumes upon return of pacingactivity.
Implantation and Follow-upAt implantation, physicians should adhere to theuse of low polarization leads in combination withAutocapture devices. This also applies to existingchronic leads in case of pacemaker replacementdue to end-of-life. Other pacing and sensing para-meters are similar as in the implantation of otherconventional pacemakers. It is recommended notto handle the lead tip during implant, sincetouching the lead tip may result in higher polar-ization signals. Device-based testing is the onlyway to measure the ER and polarization signals.In the presence of a very low ER signal, reposi-tioning of the lead to a new position within theventricle may result in improved ER detection
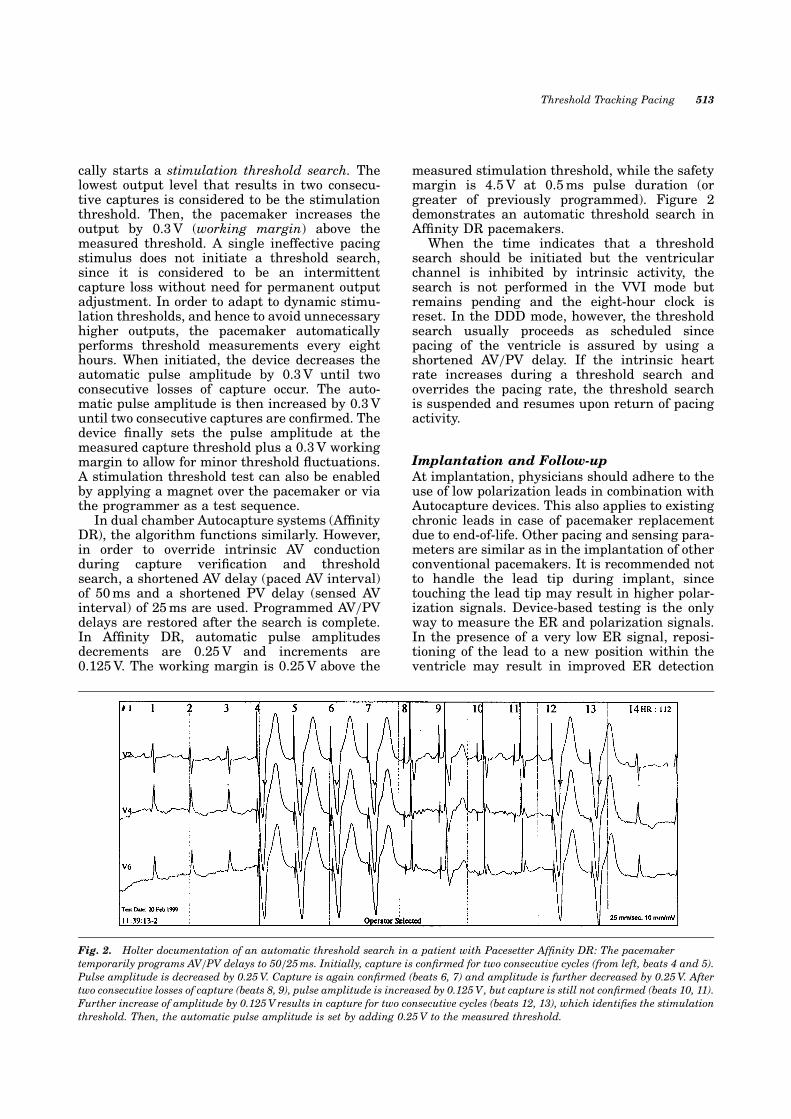
Fig. 2. Holter documentation of an automatic threshold search in a patient with Pacesetter Af®nity DR: The pacemakertemporarily programs AV=PV delays to 50=25 ms. Initially, capture is con®rmed for two consecutive cycles (from left, beats 4 and 5).Pulse amplitude is decreased by 0.25 V. Capture is again con®rmed (beats 6, 7) and amplitude is further decreased by 0.25 V. Aftertwo consecutive losses of capture (beats 8, 9), pulse amplitude is increased by 0.125 V, but capture is still not con®rmed (beats 10, 11).Further increase of amplitude by 0.125 V results in capture for two consecutive cycles (beats 12, 13), which identi®es the stimulationthreshold. Then, the automatic pulse amplitude is set by adding 0.25 V to the measured threshold.
Threshold Tracking Pacing 513

and possibly lower polarization signals. However,routine measurement of Autocapture parametersis not mandatory during implantation, providedrecommended low polarization leads are used.Our clinical experience during the past yearshas shown a slight increase in ER signal ampli-tude during the immediate post-operative period,while the polarization signal often decreases tosome extent within the ®rst couple hours afterimplantation. However, reasonable ER and polar-ization signal measurements can be done one dayafter implantation or prior to discharge and theAutocapture feature can be activated thereafter,provided that the measured parameters aresuitable.
The pacemaker programmer documents theER signal and the polarization signal amplitudes,% ratio of the ER signal to the polarization signal,and informs the user if it is suitable to activatethe feature and proposes ER sensitivity settings(Fig. 3). Autocapture is not recommended if theER amplitude is below 2.5 mV, the ER safetymargin is below 1.8 : 1 (80% safety margin), or ifthe polarization signal is> 60% of the proposedER sensitivity setting. When programmed on, theAutocapture function automatically adjusts thestimulation outputs. If the measured variablesare not suitable, the programmer automaticallyturns off the Autocapture feature and restoresnormal stimulation output settings. It must benoted that, while the ER signal is not affected byvoltage and pulse duration of the stimulus, thepolarization signal can be affected.
At follow-up, the ER amplitudes are usuallystable, but they do not correlate with the indivi-
dual R wave amplitudes, for any given patient[20]. There may be considerable variations in ERamplitude between patients. The occurrence of alate substantial decrease of the ER signal ampli-tude most likely indicates a lead problem. Regu-lar follow-up visits are mandatory to assure anappropriate function of the Autocapture feature.Clinical studies have shown that there has beenan excellent correlation of the Autocapturethreshold test results with the capture thresholdmeasured with the Vario feature (available inMicrony and Regency) at the time of routineevaluation [21].
Clinical Bene®ts of Autocapture
The Autocapture feature increases patient safety,decreases energy consumption and prolongs pace-maker longevity, provides documentation ofstimulation thresholds, and offers a unique toolfor research applications [22].
A. Patient SafetyThe most important bene®cial effect of the Auto-capture feature is its impact on patient safety. Itis well known that early after pacemaker implan-tation, the stimulation threshold increases, as aresult of the maturation process around the elec-trode tip (in response to endocardial thickening,®brosis, and other factors) [23]. Typically, stimu-lation threshold then decreases and reaches aplateau after 8±12 weeks. The peak and durationof the threshold increase are highly variable.Infrequently, a very high and prolonged thresh-old elevation can be experienced or major thresh-
Fig. 3. Programmer print-out showing the measured ER and polarization amplitudes and indicating that the safety margins areacceptable for Autocapture.
514 Duru et al.
old ¯uctuations may occur. In addition, and moreimportantly, an unpredicted late threshold risemay occur at any time despite implantation ofmodern leads with excellent overall performancerecords. Some ¯uctuations in stimulation thresh-old are also known to occur in response to variousphysiologic and pharmacological factors (e.g.,antiarrhythmic drugs) [24±26]. Therefore, therecommended 2 : 1 safety margin based on acutethreshold data obtained during a routine follow-up may not be adequate in rare patients, result-ing in loss of capture [21].
Provided no complete lead dislodgment orstructural lead failure is present, the Autocap-ture function has proven to be safe and reliable inthe long-term [20], because it assures appropriatecapture after every single beat. Numeroussurface ECG and Holter registrations did notyield a single event of loss of capture without aback-up pulse (European Microny evaluationstudy) [21].
B. Energy ConsumptionThe Autocapture feature provides adequatepacing with a minimal working margin andthus avoids unnecessary current drain. Thisfeature allows construction of pacemakers incor-porating smaller batteries without reduced long-evity. For example, the Microny pulse generatorwith a battery capacity of only 0.35 Ah and avolume of only 5.9 cm3 has a predicted longevityof 7.1 years (100% pacing at 60 bpm; 500 Ohmimpedance; 1.5 V pulse amplitude; rate responseactive).
The longevity of pulse generators may bederived by the formula [23];
Longevity �years� �C�Useful Battery Capacity in Ah�
I �Continuous drain in mA� � 24 � 365
Lithium iodine batteries used in commercialpulse generators usually have a capacity in therange of 0.8±3.0 Ah. For example, for a batterycapacity of 0.85 Ah and battery drain of 5 mA, thecalculated battery longevity from the formula is19.4 y. Of the 5 mA battery drain, 2.8 mA is used forthe circuit operation and approximately 2.2 mA isleft for stimulation and miscellaneous additionaldrain. While the Autocapture pacing system doesrequire a small amount of additional energy tooperate (0.2 mA), this is offset by the ef®ciencygained in the signi®cantly reduced chronic pulseamplitude.
The pacemaker output energy is proportionalto the square of a given voltage. The energyconsumption is overall low with modern leadsand the main bene®t of Autocapture in thisgroup is patient safety considering the few occa-sions with an unpredictable late thresholdincrease above the twofold voltage safetymargin. However, this group can have furtherenergy saving using the Autocapture feature.More substantial energy savings by Autocapturecan be obtained at elevated chronic thresholds,otherwise requiring much higher voltage outputs[27].
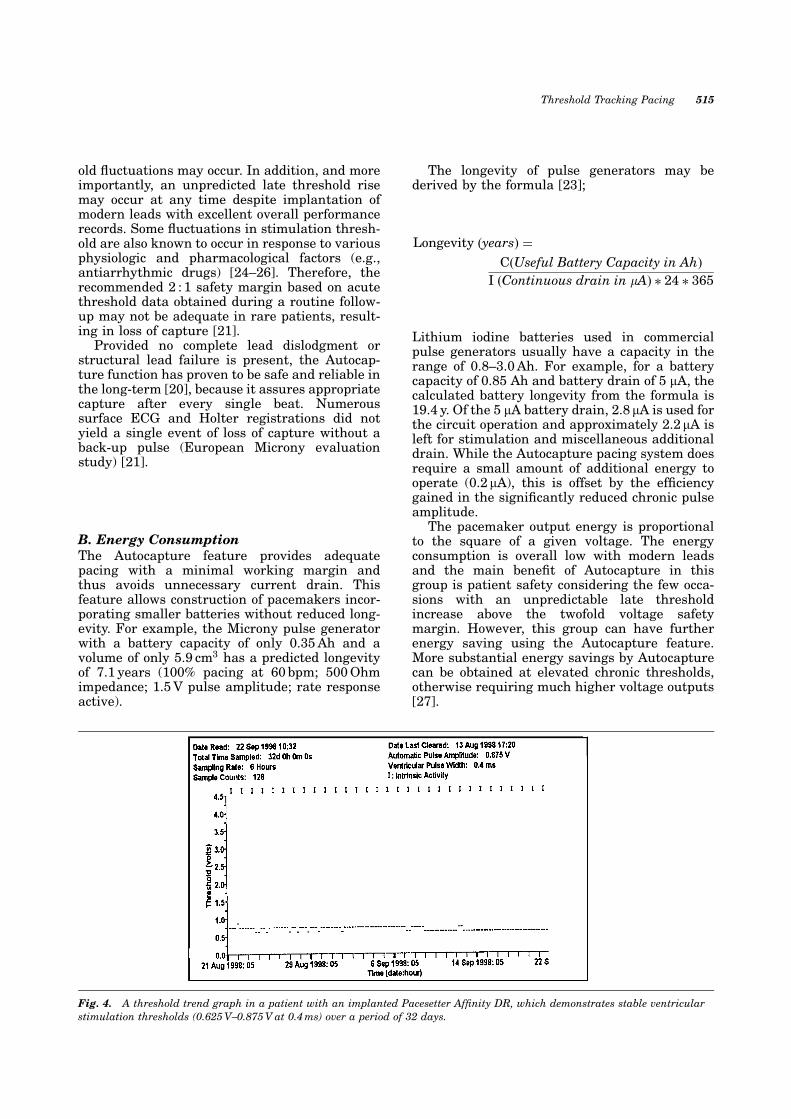
Fig. 4. A threshold trend graph in a patient with an implanted Pacesetter Af®nity DR, which demonstrates stable ventricularstimulation thresholds (0.625 V±0.875 V at 0.4 ms) over a period of 32 days.
Threshold Tracking Pacing 515

C. Threshold DocumentationA valuable feature of pacemakers with the Auto-capture function is the storage and retrieval ofinformation about the variations in the stimula-tion threshold over time. A unique thresholdtrend graph with programmable sampling rates(two seconds to 24 hours) assists in evaluatingthe pacing system and clinical status of thepatient (Fig. 4). The Autocapture feature mayalso assist in the diagnosis of minor electrodedisplacements, which are not evident radiogra-phically [28,29]. Inadequate lead position andlead tip microinstability may be suspected inthe presence of excessive stimulation thresholdvariations and can be con®rmed by repetitiveVario tests (Fig. 5).
D. Research ToolThe retrieved threshold data over time provides avaluable research tool for the study of pacingphysiology. In a study performed at our institu-tion, we were able to evaluate the in¯uence ofacute exposure to high altitudes with accomp-anying hypoxemia (established in a hypobaricchamber) on chronic ventricular stimulationthresholds by using the Autocapture feature [30].
Potential Problems and Limitations
Despite many clinical bene®ts, threshold-track-ing pacing enabled by the Autocapture feature isalso associated with potential problems andlimitations:
A. Lead SelectionBecause of the complexity of the lead-myocar-dium interface, the choice of lead type and con®g-uration allowed for ER detection has beenrestricted. The use of a bipolar lead with lowpolarization properties is mandatory in order toobtain a substantial difference in signal ampli-tude between the ER signal and polarizationsignals. Many old leads and some newer models,as well as unipolar leads are not compatible withthe present algorithm. Sensing is programmedbipolar in order to avoid interference from muscleactivity, whereas pacing has to be unipolar toincrease the signal-to-noise ratio. Because of therequirement for unipolar pacing, the Autocapturepacing system is not compatible with implantablecardioverter-de®brillators. In addition, pocketstimulation may occur during high output back-up pulses.
B. Sensing ProblemsCorrect sensing of an appropriate ER signal afteran effective pacemaker stimulus or the immedi-ate delivery of a back-up pulse in case of ineffec-tive stimulation are key elements of normalAutocapture function [31]. ER sensing disordersmay occur similar to that seen with R wavesensing. In the presence of high polarizationamplitudes, as experienced in connection withunsuitable leads, and during subthreshold stimu-lation Polarization oversensing may be observed(Fig. 6). In this case, no back-up pulse will bedelivered subsequently and thus the algorithmfails to compensate for ineffective stimulation.
Fig. 5. High initial stimulation threshold (1.5 V at 0.4 ms) in a patient post-implantation who has a relatively unstable trend andfurther increases in threshold after 2±3 weeks. This might have been caused by inadequate postion of the lead initially or delayed®xation of the lead tip due to temporary microinstability.
516 Duru et al.
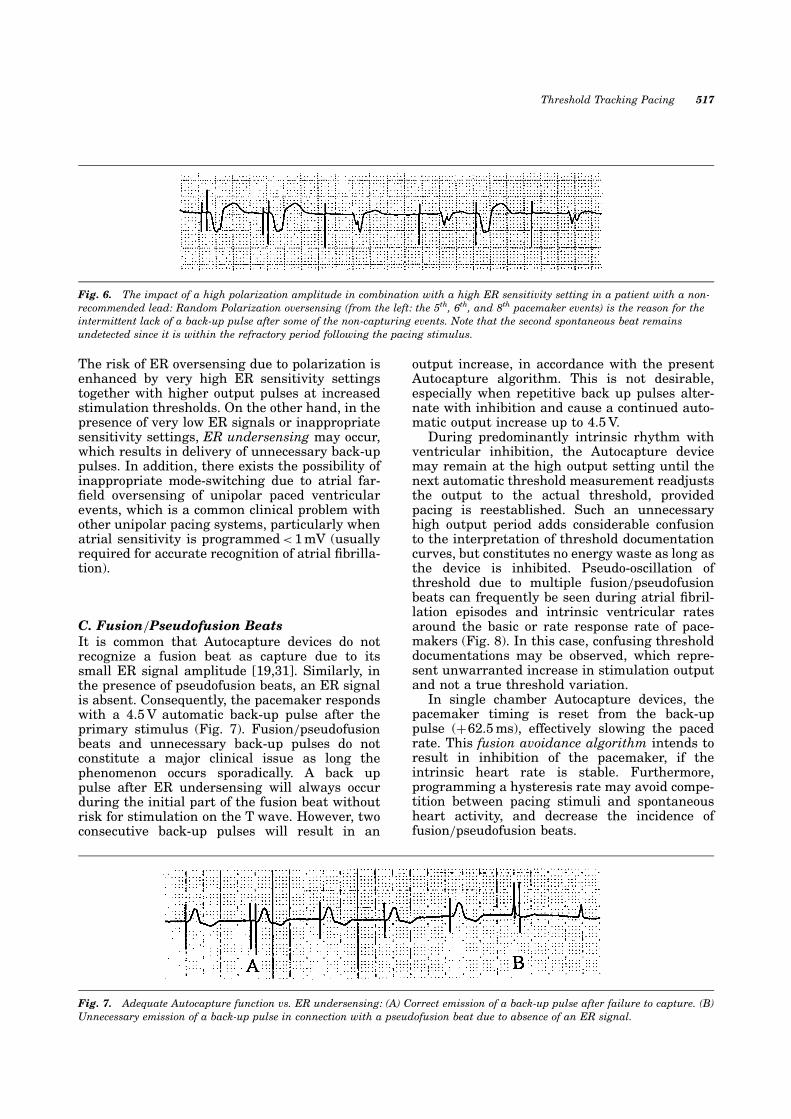
The risk of ER oversensing due to polarization isenhanced by very high ER sensitivity settingstogether with higher output pulses at increasedstimulation thresholds. On the other hand, in thepresence of very low ER signals or inappropriatesensitivity settings, ER undersensing may occur,which results in delivery of unnecessary back-uppulses. In addition, there exists the possibility ofinappropriate mode-switching due to atrial far-®eld oversensing of unipolar paced ventricularevents, which is a common clinical problem withother unipolar pacing systems, particularly whenatrial sensitivity is programmed< 1 mV (usuallyrequired for accurate recognition of atrial ®brilla-tion).
C. Fusion=Pseudofusion BeatsIt is common that Autocapture devices do notrecognize a fusion beat as capture due to itssmall ER signal amplitude [19,31]. Similarly, inthe presence of pseudofusion beats, an ER signalis absent. Consequently, the pacemaker respondswith a 4.5 V automatic back-up pulse after theprimary stimulus (Fig. 7). Fusion=pseudofusionbeats and unnecessary back-up pulses do notconstitute a major clinical issue as long thephenomenon occurs sporadically. A back uppulse after ER undersensing will always occurduring the initial part of the fusion beat withoutrisk for stimulation on the T wave. However, twoconsecutive back-up pulses will result in an
output increase, in accordance with the presentAutocapture algorithm. This is not desirable,especially when repetitive back up pulses alter-nate with inhibition and cause a continued auto-matic output increase up to 4.5 V.
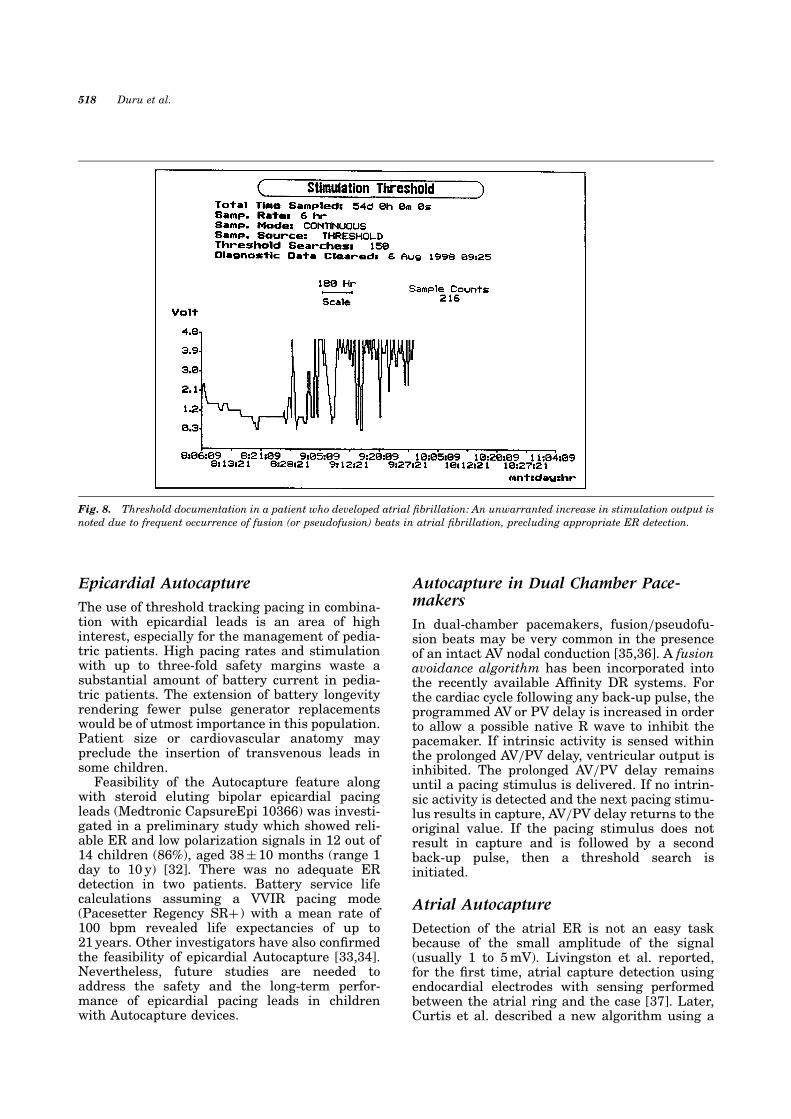
During predominantly intrinsic rhythm withventricular inhibition, the Autocapture devicemay remain at the high output setting until thenext automatic threshold measurement readjuststhe output to the actual threshold, providedpacing is reestablished. Such an unnecessaryhigh output period adds considerable confusionto the interpretation of threshold documentationcurves, but constitutes no energy waste as long asthe device is inhibited. Pseudo-oscillation ofthreshold due to multiple fusion=pseudofusionbeats can frequently be seen during atrial ®bril-lation episodes and intrinsic ventricular ratesaround the basic or rate response rate of pace-makers (Fig. 8). In this case, confusing thresholddocumentations may be observed, which repre-sent unwarranted increase in stimulation outputand not a true threshold variation.
In single chamber Autocapture devices, thepacemaker timing is reset from the back-uppulse (�62.5 ms), effectively slowing the pacedrate. This fusion avoidance algorithm intends toresult in inhibition of the pacemaker, if theintrinsic heart rate is stable. Furthermore,programming a hysteresis rate may avoid compe-tition between pacing stimuli and spontaneousheart activity, and decrease the incidence offusion=pseudofusion beats.
Fig. 7. Adequate Autocapture function vs. ER undersensing: (A) Correct emission of a back-up pulse after failure to capture. (B)Unnecessary emission of a back-up pulse in connection with a pseudofusion beat due to absence of an ER signal.
Fig. 6. The impact of a high polarization amplitude in combination with a high ER sensitivity setting in a patient with a non-recommended lead: Random Polarization oversensing (from the left: the 5th, 6th, and 8th pacemaker events) is the reason for theintermittent lack of a back-up pulse after some of the non-capturing events. Note that the second spontaneous beat remainsundetected since it is within the refractory period following the pacing stimulus.
Threshold Tracking Pacing 517
Epicardial Autocapture
The use of threshold tracking pacing in combina-tion with epicardial leads is an area of highinterest, especially for the management of pedia-tric patients. High pacing rates and stimulationwith up to three-fold safety margins waste asubstantial amount of battery current in pedia-tric patients. The extension of battery longevityrendering fewer pulse generator replacementswould be of utmost importance in this population.Patient size or cardiovascular anatomy maypreclude the insertion of transvenous leads insome children.
Feasibility of the Autocapture feature alongwith steroid eluting bipolar epicardial pacingleads (Medtronic CapsureEpi 10366) was investi-gated in a preliminary study which showed reli-able ER and low polarization signals in 12 out of14 children (86%), aged 38� 10 months (range 1day to 10 y) [32]. There was no adequate ERdetection in two patients. Battery service lifecalculations assuming a VVIR pacing mode(Pacesetter Regency SR� ) with a mean rate of100 bpm revealed life expectancies of up to21 years. Other investigators have also con®rmedthe feasibility of epicardial Autocapture [33,34].Nevertheless, future studies are needed toaddress the safety and the long-term perfor-mance of epicardial pacing leads in childrenwith Autocapture devices.
Autocapture in Dual Chamber Pace-makers
In dual-chamber pacemakers, fusion=pseudofu-sion beats may be very common in the presenceof an intact AV nodal conduction [35,36]. A fusionavoidance algorithm has been incorporated intothe recently available Af®nity DR systems. Forthe cardiac cycle following any back-up pulse, theprogrammed AV or PV delay is increased in orderto allow a possible native R wave to inhibit thepacemaker. If intrinsic activity is sensed withinthe prolonged AV=PV delay, ventricular output isinhibited. The prolonged AV=PV delay remainsuntil a pacing stimulus is delivered. If no intrin-sic activity is detected and the next pacing stimu-lus results in capture, AV=PV delay returns to theoriginal value. If the pacing stimulus does notresult in capture and is followed by a secondback-up pulse, then a threshold search isinitiated.
Atrial Autocapture
Detection of the atrial ER is not an easy taskbecause of the small amplitude of the signal(usually 1 to 5 mV). Livingston et al. reported,for the ®rst time, atrial capture detection usingendocardial electrodes with sensing performedbetween the atrial ring and the case [37]. Later,Curtis et al. described a new algorithm using a
Fig. 8. Threshold documentation in a patient who developed atrial ®brillation: An unwarranted increase in stimulation output isnoted due to frequent occurrence of fusion (or pseudofusion) beats in atrial ®brillation, precluding appropriate ER detection.
518 Duru et al.
special triphasic pacing pulse in order to mini-mize polarization signals and allow detection ofthe atrial ER [38]. Atrial ER detection in conjunc-tion with low polarization titanium-nitride coatedelectrodes are currently under investigation toenable construction of truly threshold trackingdual chamber pacemaker systems. An algorithmhas been developed recently that automaticallydetermines the atrial capture thresholds on achronic basis using the atrial ER, which matchthe manually determined thresholds within� 0.25 V for 95% of the recorded searches [39].
Considerations for Future Devices
The inability of the single chamber Autocapturedevices to recognize capture during fusion=pseu-dofusion beats is likely to remain in the nearfuture. However, the automatic output increasethat occurs after two consecutive back-up pulsesmay be avoided by a change in the algorithm (i.e.programmable number of beats for outputincrease). In our experience with single chamberunits in the presence of atrial ®brillation, thelikelihood of three or more consecutive fusion=pseudofusion beats to occur subsequently israther low. In contrast, fusion=pseudofusioncomplexes may be very common in dual chamberunits depending on the programmed AV interval.
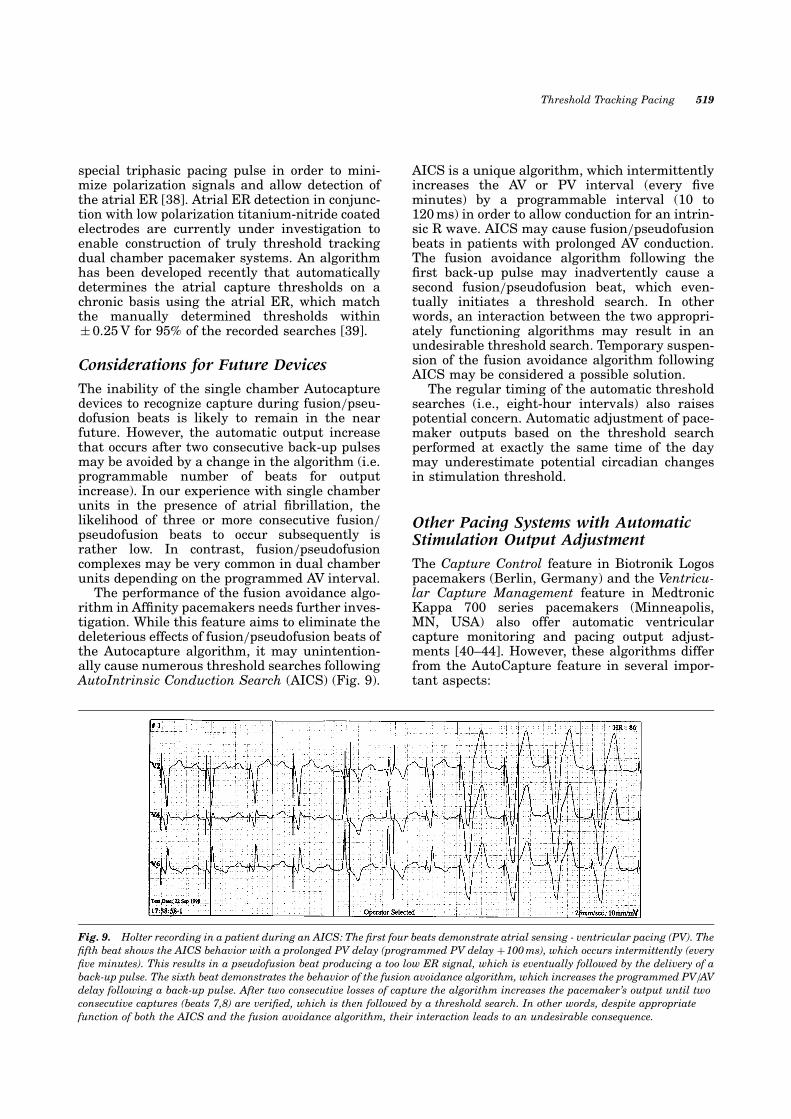
The performance of the fusion avoidance algo-rithm in Af®nity pacemakers needs further inves-tigation. While this feature aims to eliminate thedeleterious effects of fusion=pseudofusion beats ofthe Autocapture algorithm, it may unintention-ally cause numerous threshold searches followingAutoIntrinsic Conduction Search (AICS) (Fig. 9).
AICS is a unique algorithm, which intermittentlyincreases the AV or PV interval (every ®veminutes) by a programmable interval (10 to120 ms) in order to allow conduction for an intrin-sic R wave. AICS may cause fusion=pseudofusionbeats in patients with prolonged AV conduction.The fusion avoidance algorithm following the®rst back-up pulse may inadvertently cause asecond fusion=pseudofusion beat, which even-tually initiates a threshold search. In otherwords, an interaction between the two appropri-ately functioning algorithms may result in anundesirable threshold search. Temporary suspen-sion of the fusion avoidance algorithm followingAICS may be considered a possible solution.
The regular timing of the automatic thresholdsearches (i.e., eight-hour intervals) also raisespotential concern. Automatic adjustment of pace-maker outputs based on the threshold searchperformed at exactly the same time of the daymay underestimate potential circadian changesin stimulation threshold.
Other Pacing Systems with AutomaticStimulation Output Adjustment
The Capture Control feature in Biotronik Logospacemakers (Berlin, Germany) and the Ventricu-lar Capture Management feature in MedtronicKappa 700 series pacemakers (Minneapolis,MN, USA) also offer automatic ventricularcapture monitoring and pacing output adjust-ments [40±44]. However, these algorithms differfrom the AutoCapture feature in several impor-tant aspects:
Fig. 9. Holter recording in a patient during an AICS: The ®rst four beats demonstrate atrial sensing - ventricular pacing (PV). The®fth beat shows the AICS behavior with a prolonged PV delay (programmed PV delay �100 ms), which occurs intermittently (every®ve minutes). This results in a pseudofusion beat producing a too low ER signal, which is eventually followed by the delivery of aback-up pulse. The sixth beat demonstrates the behavior of the fusion avoidance algorithm, which increases the programmed PV=AVdelay following a back-up pulse. After two consecutive losses of capture the algorithm increases the pacemaker's output until twoconsecutive captures (beats 7,8) are veri®ed, which is then followed by a threshold search. In other words, despite appropriatefunction of both the AICS and the fusion avoidance algorithm, their interaction leads to an undesirable consequence.
Threshold Tracking Pacing 519

Capture ControlThis feature introduced by Biotronik averagesthe ER signals of several effective pacingimpulses, and by using this reference curve, itmonitors the effectiveness of every ventricularimpulse [40±43]. Similar to the Autocapturefeature, Capture Control requires the use of alead with low polarization properties. The ERsignal is evaluated in a time frame in the rangefrom 70 to 100 ms following a ventricular pulse. Ifno response is detected, the AV interval isreduced to 50 ms in the DDD mode or thepacing cycle duration is extended by 100 ms inthe VVI mode to exclude the possibility of falseinterpretation caused by a fusion=pseudofusionbeat. There is no back-up safety pulse, but ifthere is persistent loss of capture, theprogrammed output is increased by 2 V steps(i.e.,�2 V,�4 V). After a programmable timeinterval has elapsed, the amplitude is reducedto the programmed value to determine whether asmaller amplitude will suf®ce.
The Capture Control feature intends to act as asafety against unforeseen or transient elevatedventricular pacing thresholds. The algorithm isnot intended to accurately evaluate the pacingthreshold since it only decreases the amplitude toa predetermined value to con®rm ventricularcapture. The absence of a back-up pulse maytheoretically lead to patient discomfort.
Ventricular Capture ManagementThe Ventricular Capture Management feature inMedtronic Kappa 700 pacemakers allows aventricular pacing threshold search at a prede-termined interval, ranging from once every 15minutes to 42 days [44]. The pacemaker deter-mines two threshold points (to approximate therheobase and chronaxie), from which a strength±duration curve is constructed. For rheobase test,amplitude is reduced (at a constant 1.0 ms) andfor chronaxie, pulse duration is reduced (at twotimes rheobase amplitude) to produce loss ofcapture. After loss of capture, the amplitude orpulse width is increased to regain capture,thereby establishing rheobase or chronaxie. Ifcapture is lost during a test sequence, there is aback-up pulse within 110 ms to ensure capture forevery paced beat. The maximum output withautomatic capture during threshold search is5.0 V at 1.0 ms pulse duration.
Ventricular Capture Management can beprogrammed to adaptive, monitor only, or off. Ifprogrammed to the adaptive mode, the algorithmautomatically adjusts pacing parameters withina clinician-de®ned capture safety margin. Someof the parameters (amplitude and pulse durationsafety margins, and minimum adapted amplitude
and pulse duration) have to be preprogrammed.The pacing output is adjusted to prede®nedtarget margins or programmed minimumoutput, whichever is greater. However, for aprogrammable period following implantation,de®ned as the Acute Phase (i.e., during leadmaturation), the pacing output settings do notdecrease.
There is no requirement for specially designedlead types and pacing=sensing con®guration forthe function of this Medtronic feature. This ismade possible by modi®cations to the standardsense ampli®er circuitry, which allow for discri-mination of the ER signal from the lead polariza-tion, based on the polarization slope observed viathe electrogram. Therefore, the clinician mayimplant any type of endocardial lead. However,the feature has also some limitations. The pace-maker output remains constant until the nextthreshold search and there is no back-up pacingin case of loss of capture during this period. Sincethere is no beat-by-beat monitoring of ventricularcapture, this feature cannot be truly considered athreshold-tracking feature. In addition, since thealgorithm functions with a relatively broad work-ing margin, its impact on energy consumptionmay be limited.
Conclusion
Automatic output regulation, which has been along-standing goal of the pacing community, hasbeen reached with the introduction of the Auto-capture feature. Pacing with adequate stimula-tion safety (back-up pulses) but minimal workingmargin avoids unnecessary current drain andeliminates the dangers of unpredictable stimula-tion threshold oscillations, furthermore allowingsmaller pacemakers with greater longevity.Retrieval of stimulation trend graphs is veryhelpful in evaluating the integrity of the pacingsystem and clinical status of the patient. Itprovides an excellent tool for research in evaluat-ing the dynamic physiology of pacing. However,the Autocapture feature is also associated withpotential problems. Fusion=pseudofusion beats,with resultant insuf®cient or absent ER signalamplitudes, cause unnecessary delivery of back-up pulses and a possible unwarranted increase inpacemaker output. Epicardial pacing with Auto-capture and dual-chamber pacing with ventricu-lar Autocapture are already in clinical use andare the subject of ongoing studies. The CaptureControl and the Ventricular Capture Manage-ment features offer alternative approaches forthreshold monitoring and pacing output adjust-ments, and have their own bene®ts and limita-tions. Automatic adjustment of atrial pacingthreshold is among the new frontiers of the
520 Duru et al.
pacing community to enable construction of dualchamber threshold tracking pacemakers.
References
1. Funke HD, Der Schwellenwertschrittmacher. Einneuartiges Prinzip der elektrischen Myokard-Stimu-lation. Inaugural-Dissertation, University of Bonn,Germany, 1972.
2. Preston TA, Bowers DL. Report of a continuousthreshold tracking system. In J Hilbert, Th Thalen(eds.): Cardiac Pacing. Assen, Van Gorcum, 1973, pp295±299.
3. Mugica J, Lazarus B, Buffet J. Pacemaker with auto-matic adaptation to the pacing threshold. In: JHilbert, Th Thalen (eds.): Cardiac Pacing. Assen,Van Gorcum, 1973, pp 150±155.
4. Preston TA, Bowers DL. The automatic thresholdtracking pacemaker. Med Instrument 1974;8:322±325.
5. Preston TA, Bowers DL. Clinical applications of thethreshold tracking pacemaker. Am J Cardiol 1975;36:322±326.
6. Thalen H, Rickards A, Wittkampf F, et al. Evokedresponse sensing as automatic control of pacemakeroutput. Cardiac Pacing, Piccin Medical Books, Padova,Italy, 1982, pp 1229±1234.
7. Brouwer J, Nagelkerke D, De Jongste MJ, Boute W,Den Heijer P, Lie KI. Analysis of the morphology of theunipolar endocardial paced evoked response. PacingClin Electrophysiol 1990;13:302±313.
8. Curtis AB, Vance F, Miller K. Automatic reduction ofstimulus polarization artifact for accurate evaluationof ventricular evoked responses. Pacing Clin Electro-physiol 1991;14:529±537.
9. Bolz A, Hubmann M, Hardt R, Riedmuller J, Schal-dach M. Low polarization pacing lead for detecting theventricular-evoked response. Med Prog Technol 1993;19:129±137.
10. Danilovic D, Ohm OJ, Stroebel J, Breivik K, Hoff PI,Markowitz T. An algorithm for automatic measure-ment of stimulation thresholds: clinical performanceand preliminary results. Pacing Clin Electrophysiol1998;21:1058±1068.
11. Vonk BF, Van Oort G. New method of atrial andventricular capture detection. Pacing Clin Electrophy-siol 1998;21:217±222.
12. Kadhiresan VA, Olive A, Gornick C, Spinelli J, VillaltaD. Automatic capture veri®cation by charge-neutralsensing. Pacing Clin Electrophysiol 1999;22:73±78.
13. SchuÈ ller H, Fahraeus T, Thuesen L, Kruse I, Skog G.First experience with an automatic output adaptationpacemaker based on evoked response. (abstract)Pacing Clin Electrophysiol 1995;18:824.
14. Kennergren C, Cappuci M, Walfridsson H. Clinicalexperience with autocapture. (abstract) Eur JCPE1996;6:161.
15. Ebner E, HuÈmmer A. Autocapture-ein neuer Algor-ithmus zur kontinuierlichen Anpassung der Stimula-tions-amplitude an die Reizschwelle. Herzshritt-macher 1996;16:115±120.
16. Sermasi S, Marconi M, Libero L, Moracchini PV,Rusconi L, Mininno A, Sigliano R Italian experiencewith AutoCapture in conjunction with a membrane
lead. Pacesetter Automatic Control of Energy andMembrane Automatic Threshold Evaluation (Pace-mate) Study Group. Pacing Clin Electrophysiol 1996;19:1799±1804.
17. Candinas R, Radicke D, SchoÈnbeck M, Brockes M,Duru F. First experience with a dual-chamber pace-maker with automatic adjustment of the stimulationoutput based on beat-by-beat ventricular capturecon®rmation. (abstract) Pacing Clin Electrophysiol1999;22:59.
18. SchuÈ ller H, Lindgren A. Principles and utility ofautocapture. In KK Sethi (ed.): VI Asian-Paci®csymposium on cardiac pacing and electrophysiology.Bologna, Monduzzi Editore, 1997;pp 187±192.
19. Levine PA, Barold SS. Pacemaker automaticity:Enabled by a multiplicity of new algorithms. In:Singer I, Barold SS, Camm AJ (eds). Nonpharmacolo-gical therapy of arrhythmias for the 21st century.Futura, Armonk, NY, 1999, pp. 845±880.
20. SchuÈ ller H, FaÈhraeus T, Kruse I, Svensson O,Mortensen P. Long-term follow-up of Autocapture(� 5 y). (abstract) Pacing Clin Electrophysiol 1999;22:4.
21. Clarke M, Liu B, SchuÈ ller H, Binner L, Kennergren C,Guerola M, Weinmann P, Ohm OJ. Automatic adjust-ment of pacemaker stimulation output correlated withcontinuously monitored capture thresholds: A multi-center study. Pacing Clin Electrophysiol 1998;21:1567±1575.
22. Candinas R, Duru F, Bauersfeld U, SchoÈnbeck M,SchuÈ ller H. Principles and bene®ts of Autocapture.In: Santini M., Progress in Clinical Pacing 1998, pp.333±338.
23. Furman S, Hayes DL, Holmes DR, eds. A practice ofcardiac pacing. Futura, Mount Kisco, New York, 1989.
24. Preston TA, Fletcher RD, Lucchesi BR, Judge RD.Changes in myocardial threshold. Physiologic andpharmacologic factors in patients with implantedpacemakers. Am Heart J 1967;74:235±242.
25. Preston TA, Judge RD. Alteration of pacemakerthreshold by drug and physiological factors. Ann N YAcad Sci 1969;167:686±692.
26. Dohrmann ML, Goldschlager NF. Myocardial stimula-tion threshold in patients with cardiac pacemakers:effect of physiologic variables, pharmacologicalagents, and lead electrodes. Cardiol Clin 1985;3:527±537.
27. Simeon L, Duru F, Radicke D, Fluri M, Jenzer HR,Candinas R. Increased pacemaker longevity inpatients with low and high chronic thresholds usingthe Autocapture feature. (abstract) KardiovaskulaÈreMedizin 1999;2:49.
28. Candinas R, HuÈmmer A, Varga L, SchoÈnbeck M.Diagnose und Verlaufskontrolle einer Mikrodisloka-tion bzw. MikroinstabilitaÈt mit Hilfe der FunktionAutocapture. Herzschrittmacher 1996;16:160±163.
29. Liebold A, Birnbaum DE. Diagnostische Nutzung vonAutocapture: Detektion einer Sondendislokation. ZKardiol 1997;86:521±523.
30. Weilenmann D, Duru F, SchoÈnbeck M, Schenk B,Zwicky P, Russi EW, Candinas R. In¯uence of acuteexposure to high altitude and hypoxemia on ventricu-lar stimulation thresholds in pacemaker patients.Pacing Clin Electrophysiol 2000;23:512±515.
Threshold Tracking Pacing 521

31. SchuÈ ller H, Duru F, Bauersfeld U, Candinas R. Auto-capture: Troubles and troubleshooting. In: Santini M.Progress in Clinical Pacing 1998, pp. 339±344.
32. Bauersfeld U, Nowak B, Molinari L, Malm T, Kamp-mann C, SchoÈnbeck MH, Schuller H. Low-energyepicardial pacing in children - The bene®t of autocap-ture. Ann Thorac Surg, 1999;68:1380±1383.
33. Adwani SS, Musumeci F, Stuart G. Epicardial pacingusing a pacemaker with Autocapture algorithm in aninfant. (letter) Int J Cardiol 1997;62:90±91.
34. Nowak B, Kampmann C, Schmid FX, Przibille O,Wippermann F, Himmrich E, Meyer J. Pacemakertherapy in premature children with high degreeAV block. Pacing Clin Electrophysiol 1998;21:2695±2698.
35. Sholder J, Bornzin GA, Florio J, Sloman L, Levine PA,Jalali L. Future directions with a threshold trackingpacer: the Autocapture pacing system (Pacesettertechnical notes).
36. Bornzin GA, Florio J, Sloman L, Levine PA, Sholder J,Jalali L. Dual-chamber Autocapture system algorithmthat saves pacing energy and avoids fusion in patientswith intact conduction. HeartWeb 1996;2:article no.96110024.
37. Livingston AR, Callaghan FJ, Byrd CL, Heemels JP,Hollander P, Van Mechelen R, Chappin JJ. Atrialcapture detection with endocardial electrodes.Pacing Clin Electrophysiol 1988;11:1770±1776.
38. Curtis AB, Vance F, Wuist SM, Domijan A, Keim SG,Duran A, Miller K. A new algorithm for minimizingpacemaker polarization artifact: universally applic-able in permanent pacing systems. Pacing Clin Elec-trophysiol 1991;14:1803±1808.
39. Bradley K, Sloman L, Bornzin GA, Florio J. An atrialautothreshold algorithm using the atrial evokedresponse. (abstract) Pacing Clin Electrophysiol 1999;Haase S, DoÈrffel EF, Stammwitz E. Clinical investiga-tion of an automatic capture control using the ventricu-lar evoked response. Prog in Biomed Res 1999;4:295±298.
40. Guilleman D, Bussillet H, Scanu P, Raguin D, Aisen-farb JC, Bienvenu P, Meunier JF, Canot N. Outputadjustment with the DDD pacemaker with automaticcapture-control algorithm. Prog in Biomed Res 1999;4:291±294.
41. Ramchurn HK, Berton F, Bouvy TH, Zakhia R. Relia-bility of determining ventricular pacing threshold by apurely automatic method using the ventricular evokedresponse signal. Prog in Biomed Res 1999; 4: 299±302.
42. Novak M, Kamaryt P, Haeuser T, Mach P. Simplifyingpacemaker follow-up using automatic threshold deter-mination in ventricle. Prog in Biomed Res 1999;4:287±290.
43. Current concepts in autocapture=Ventricular CaptureManagement operational details. Medtronic technicalconcept papers, July 1998.
522 Duru et al.