three-dimensional structure small intestinal mucosa health · gut, 1969, 10, 6-12 three-dimensional...
TRANSCRIPT

Gut, 1969, 10, 6-12
Three-dimensional structure of the human smallintestinal mucosa in health and disease
C. A. LOEHRY AND B. CREAMER
From the Gastrointestinal Laboratory, St Thomas' Hospital, London
Variations in the three-dimensional structure of thesmall intestinal mucosa have only been appreciatedsince the dissecting microscope was introduced as atool for examining mucosal specimens (Rubin,Brandborg, Phelps, and Taylor, 1960). Although it isnow widely accepted that the changes in mucosalstructure from finger villi to leaves, convolutions,and a flat mucosa are all gradations of a singleprocess, the reason for the mucosa adopting thesemorphological variations in disease states hasremained largely obscure. Different authors havequoted a variety of possible mechanisms. Townley,Cass, and Anderson (1964) suggested that theprimary mucosal defect was injury to the exposedupper parts of the villi causing denudation of theepithelium and basement membrane, and that thesebare tips of villi 'fused', forming leaves and convolu-tions by 'bridging', producing a flat mucosa as pro-gressively more of these villous clumps fused to-gether. Himes and Adlersberg (1958) also suggestedthat epithelial cell injury caused villous fusion andclumping. Shiner and Doniach (1960), on the otherhand, considered that the appearances could be theresult of simple villous atrophy due to the 'defectiveformation and viability of villous epithelial cells'.Swanson and Thomassen (1965) in a study of tropicalsprue also subscribed to the idea of villous fusion,but considered that this began at the base of the villirather than at the tips.
Previous studies of mucosal structure under thedissecting microscope have been limited in that onlythe upper part of the villi is directly visible, as thethick epithelial cell layer precludes any vision of thebase of villi, of crypts, and of the crypt/villus rela-tionship. In the present study the mucosa has beenexamined under the dissecting microscope afterautolysis of epithelial cells, and histologically byserial horizontal cross sections through conven-tionally fixed specimens.
METHODS
AUTOLYSIS TECHNIQUE After death epithelial cells under-go rapid autolytic changes and can be washed away. The
skeleton structure of the mucosa, however, remains,consisting of the basement membrane and connectivetissue framework. These structures provide a true repre-sentation of the mucosal patterns present in vivo, and inaddition allow direct vision of the crypt openings. Thedetails of this technique have been previously described(Loehry and Creamer, 1966) and Fig. 1 shows the normalhuman jejunal mucosa before and after autolysis. Thereis no loss of villi by this technique, though their size issomewhat reduced after removal of the epithelial celllayer.
HORIZONTAL SERIAL SECTIONS In order to confirm theresults obtained with the autolysed material and todemonstrate that the structures seen by this method didtruly represent the mucosa in vivo, serial horizontal crosssections were taken down through fresh specimens ofboth normal and abnormal mucosa, and fixed in 10%formalin. Serial sections were taken at 10 to 15 g thick-ness from the tips of the villi to the crypt zone, stainedwith haematoxylin and eosin, and photographed. Thismethod of examining the mucosa has also been employedby Cocco, Dohrmann, and Hendrix (1966), and byfollowing down progressive sections the three-dimen-sional structure of the mucosa can be reconstituted.
RESULTS
Studied in these ways it becomes clear that the three-dimensional structure of the small intestinal mucosais more complex than has been thought. Over 200specimens ofmucosa were examined by the autolysedtechnique from necropsies so that a whole spectrumof variations in mucosal architecture in a largepopulation was obtained. In these autolysed speci-mens structures became visible that had been pre-viously obscured, revealing a smooth progressionof changes in mucosal architecture from finger villito a completely flat mucosa. For convenience ofdescription the structural features of the mucosa aregraded into five groups: stage 1, normal appear-ances in jejunum and ileum; stage 2, normal appear-ances in duodenum; stage 3, mildly abnormal,characterized by broadened villi; stage 4, moderatelyabnormal, characterized by convolutions; and6
on 10 Novem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.6 on 1 January 1969. Dow
nloaded from

Three-dimensional structure of the human small intestinal mucosa in health and disease 7
FIG. 1.
FIG. 1. Human jejunal mucosa before andafter autolysis. Removal of epithelial cellsallows direct vision of the crypt openings. x 90.
FIG. 2. Autolysed jejunal mucosa. Stage 1:the crypts outnumber villi in a ratio of approxi-mately 3 to 1. x 90.
on 10 Novem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.6 on 1 January 1969. Dow
nloaded from
C. A. Loehry and B. CreamerU _ ~~~~~~~~..J -.WI F .v
i~~~~~~~~LL.I_
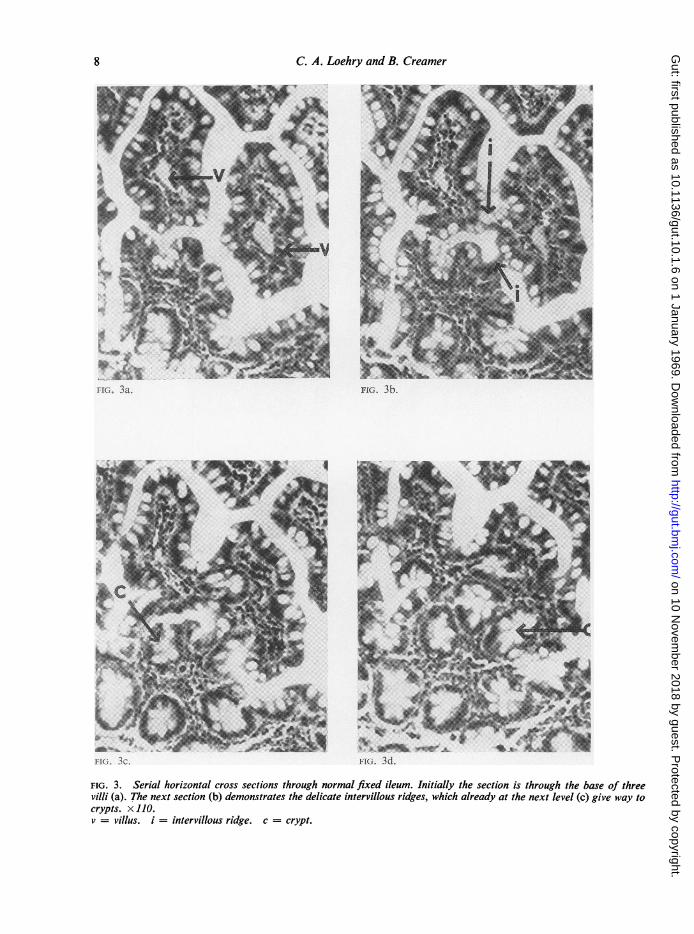
FIG. 3. Serial horizontal cross sections through normal fixed ileum. Initially the section is through the base of threevilli (a). The next section (b) demonstrates the delicate intervillous ridges, which already at the next level (c) give way tocrypts. x 110.v = villus. i = intervillous ridge. c = crypt.
8
on 10 Novem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.6 on 1 January 1969. Dow
nloaded from

Three-dimensional structure of the hunman small intestinal mucosa in health and disease
stage 5, severely abnormal, characterized by a flatmucosa.
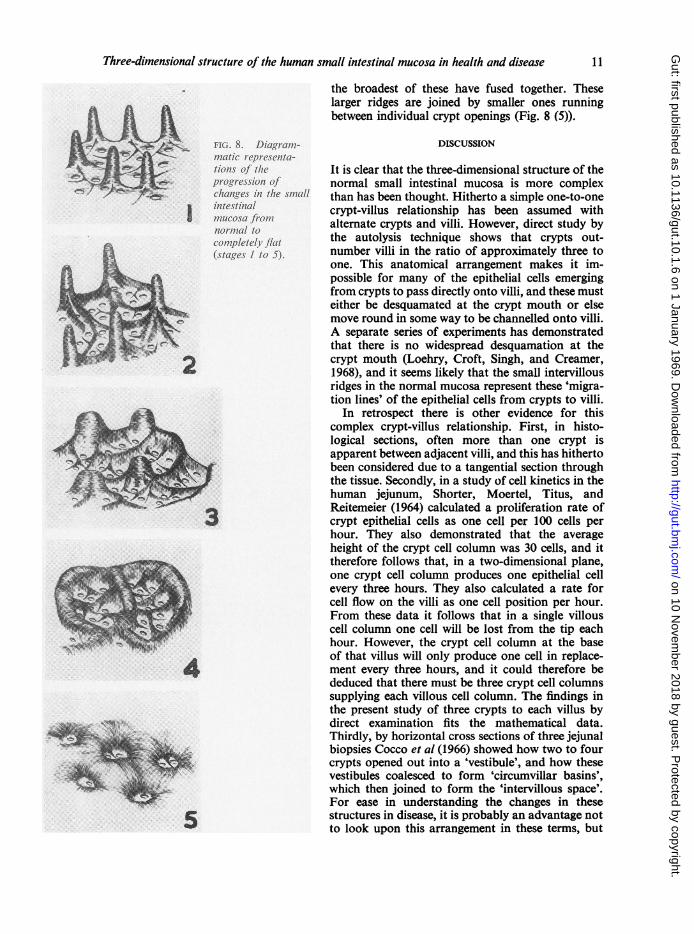
STAGE 1 (FIG. 2) In the autolysed mucosa cryptsare easily visible and outnumber villi in the ratio ofapproximately three to one. In many cases there aretwo crypts between villi and the greater part of eachcrypt mouth is adjacent not to villi, but to othercrypts. Clearly, therefore, the migration of epithelialcells from crypts to villi cannot be a simple directprogression. Running in between adjacent cryptsand joining up onto villi are many small delicatestructures that we have termed 'intervillous ridges'.These are extremely small and delicate in the normaljejunum and are best seen in the serial horizontalsections (Fig. 3). By this technique the delicateintervillous ridges present at this stage are seenjoining the base of villi. This appearance of thenormal jejunum and ileum, with crypts outnumber-ing villi, and small delicate intervillous ridges isshown as a diagram in Figure 8 (1).
STAGE 2 (FIG. 4) This stage represents the typicalappearance seen in the normal duodenum. Many ofthe crypts appear to be lying in groups of two tofour in 'pits' beneath the surface. Seen directly underthe dissecting microscope it is clear that this appear-ance is due to hypertrophy of many of the delicate
intervillous ridges, which here have become fullerand broader, giving, in the stained specimens, theappearance seen in Figure 4. The structures presentat this stage are shown in a diagram in Figure 8 (2).
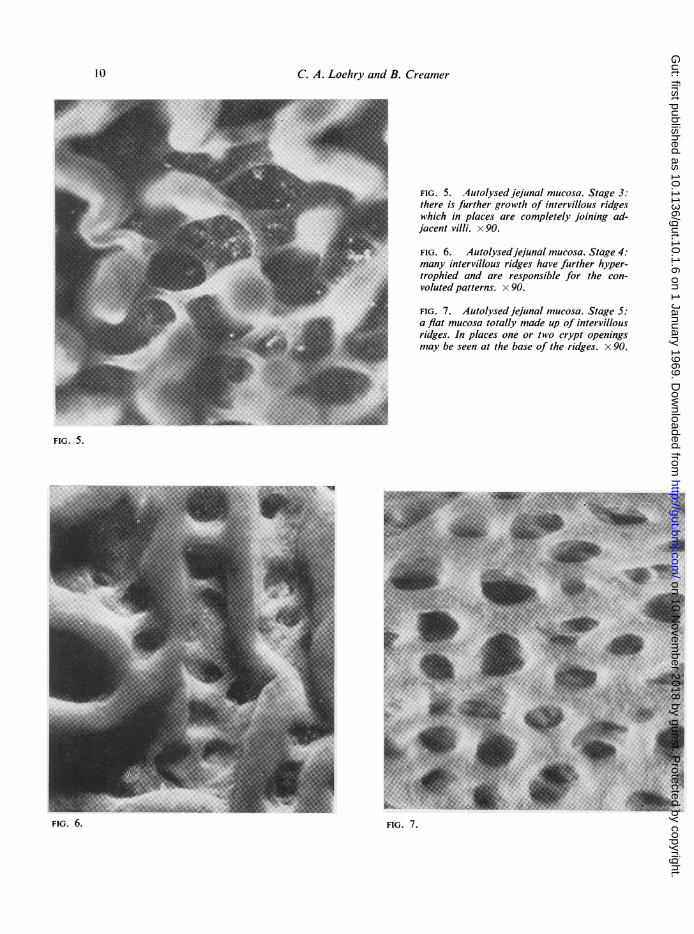
STAGE 3 (FIG. 5) The appearances at this stage wereseen in several of the specimens examined. Heremore intervillous ridges have hypertrophied, andvilli have become correspondingly shorter and wider.In unautolysed material only the tops of the broad-ened villi and the occasional intervillous ridge wouldbe visible at the surface to give the mucosa thetypical appearance of leaves with occasional ridges.The progression to this stage is shown in Figure 8 (3).
STAGE 4 (FIG. 6) Here the intervillous ridges areeven broader and more prominent, and have in-corporated all villous projections. Even in un-autolysed material many of the larger ridges wouldbe visible and give rise to a convoluted pattern.Figure 8 (4) is a diagram of the mucosa at this stage.
STAGE 5 (FIG. 7) This is a flat mucosa. Here moreintervillous ridges have come up, broadened andflattened, and the surface of the mucosa is nowtotally made up of these hypertrophied structures.Obviously some of the intervillous ridges haveenlarged more than others, and, in the flat mucosa,
FIG. 4. Autolysed dhodenal mucosa. Stage2: here the intervillous ridges have begun tohypertrophy and the crypts are seen at theirbase. x 90.
9
on 10 Novem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.6 on 1 January 1969. Dow
nloaded from
C. A. Loehry and B. Creamer
FIG. 5. Autolysedjejunal mucosa. Stage 3:there is further growth of intervillous ridgeswhich in places are completely joining ad-jacent villi. x 90.
FIG. 6. Autolysedjejunal mucosa. Stage 4:many intervillous ridges have further hyper-trophied and are responsible for the con-voluted patterns. x 90.
FIG. 7. Autolysedjejunal mucosa. Stage 5:a flat mucosa totally made up of intervillousridges. In places one or two crypt openingsmay be seen at the base of the ridges. x 90.
FIG. 5.
FIG. 6.
10
FIG. 7.
on 10 Novem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.6 on 1 January 1969. Dow
nloaded from
Three-dimensional structure of the human small intestinal mucosa in health and disease
the broadest of these have fused together. Theselarger ridges are joined by smaller ones runningbetween individual crypt openings (Fig. 8 (5)).
FIG. 8. Diagram-matic representa-tions of theprogression ofchanges in the smallintestinalmucosa fromnormal tocompletely flat(stages 1 to 5).
DISCUSSION
It is clear that the three-dimensional structure of thenormal small intestinal mucosa is more complexthan has been thought. Hitherto a simple one-to-onecrypt-villus relationship has been assumed withalternate crypts and villi. However, direct study bythe autolysis technique shows that crypts out-number villi in the ratio of approximately three toone. This anatomical arrangement makes it im-possible for many of the epithelial cells emergingfrom crypts to pass directly onto villi, and these musteither be desquamated at the crypt mouth or elsemove round in some way to be channelled onto villi.A separate series of experiments has demonstratedthat there is no widespread desquamation at thecrypt mouth (Loehry, Croft, Singh, and Creamer,1968), and it seems likely that the small intervillousridges in the normal mucosa represent these 'migra-tion lines' of the epithelial cells from crypts to villi.
In retrospect there is other evidence for thiscomplex crypt-villus relationship. First, in histo-logical sections, often more than one crypt isapparent between adjacent villi, and this has hithertobeen considered due to a tangential section throughthe tissue. Secondly, in a study of cell kinetics in thehuman jejunum, Shorter, Moertel, Titus, andReitemeier (1964) calculated a proliferation rate ofcrypt epithelial cells as one cell per 100 cells perhour. They also demonstrated that the averageheight of the crypt cell column was 30 cells, and ittherefore follows that, in a two-dimensional plane,one crypt cell column produces one epithelial cellevery three hours. They also calculated a rate forcell flow on the villi as one cell position per hour.From these data it follows that in a single villouscell column one cell will be lost from the tip eachhour. However, the crypt cell column at the baseof that villus will only produce one cell in replace-ment every three hours, and it could therefore bededuced that there must be three crypt cell columnssupplying each villous cell column. The findings inthe present study of three crypts to each villus bydirect examination fits the mathematical data.Thirdly, by horizontal cross sections of three jejunalbiopsies Cocco et al (1966) showed how two to fourcrypts opened out into a 'vestibule', and how thesevestibules coalesced to form 'circumvillar basins',which then joined to form the 'intervillous space'.For ease in understanding the changes in thesestructures in disease, it is probably an advantage notto look upon this arrangement in these terms, but
11
on 10 Novem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.6 on 1 January 1969. Dow
nloaded from

12 C. A. Loehry and B. Creamer
as a series of intervillous ridges of varying height,which in fact represent the walls of the vestibulesand basins that Cocco et al describe. In the presentstudy it is shown how the hypertrophy of theseintervillous ridges provides the structural basis forthe changes in mucosal pattern in disease. In the'normal' duodenum the beginnings of this hyper-trophy are already present, and it has been recog-nized for some time that minor variations in villousarchitecture are common in biopsies from this site.It is only, however, after autolysis that it can be seenhow widespread are these minor changes in thisarea. As the mucosa becomes more abnormal moreof the intervillous ridges hypertrophy even furtheras the villi shorten forming leaves, convolutions, andfinally a flat mucosa where the whole mucosalstructure is made up solely of hypertrophied andbroadened intervillous ridges.
This hypertrophy, of course, does not occurequally at all sites at the same time, and explainswhy often a variety of villous shapes is evident in asingle biopsy specimen, though, if the specimen isexamined after autolysis, generalized intervillousridge hypertrophy will be evident in even the mostmildly abnormal mucosa. The crests of the mucosalfolds show more severe changes than the troughs(Creamer, 1964), and with its extremely rapid turn-over time the morphology of the mucosa must be ina state of continuous change, from one day to an-other and from one site to another, dependent uponmultiple factors affecting each particular area ofmucosa at any time. However, the characteristicchanges in mucosal architecture depend ultimatelyupon variations of normal structures, and the in-creased prominence of normal epithelial cell migra-tion lines is responsible for the changing patternsin disease states.
SUMMARY
The human small intestinal mucosa was examined
under the dissecting microscope after autolysis ofepithelial cells, and histologically by serial horizontalcross sections of conventionally fixed specimens.The normal three-dimensional mucosal structurewas shown to be complex, with a preponderance ofcrypts over villi, and small intervillous ridges run-ning between the crypts and joining up onto the baseof villi. As the mucosa becomes abnormal theseintervillous ridges hypertrophy to a varying degreeas the villi shorten, and are responsible for themucosal patterns that are seen in disease states.
We are indebted to Mr P. Leppard for technical assistanceand to the Endowment Fund of St Thomas' Hospital fora grant to one of us (C.L.) while undertaking this work.This work formed part of an M.D. thesis (C.L.) at theUniversity of Cambridge.
REFERENCES
Cocco, A. E., Dohrmann, M. J., and Hendrix, T. R. (1966). Recon-struction of normal jejunal biopsies: three-dimensionalhistology. Gastroenterology, 51, 24-31.
Creamer, B. (1964). Small-intestinal mucosal dynamics and theenvironment. Brit. med. J., 2, 1373-1375.
Himes, H. W., and Adlersberg, D. (1958). Pathologic changes in thesmall bowel in idiopathic sprue: biopsy and autopsy findings.Gastroenterology, 35, 142-154.
Loehry, C. A., and Creamer, B. (1966). Post-mortem study of small-intestinal mucosa. Brit. med. J., 1, 827-829.
, Croft, D. N., Singh, A. K., and Creamer, B. (1968). Cell turn-over in the rat small intestinal mucosa: an appraisal of cellloss. Gut, 10, 13-18.
Rubin, C. E., Brandborg, E. L., Phelps, P. C., and Taylor, H. C., Jr(1960). Studies of coeliac disease. I. The apparent identical andspecific nature of the duodenal and proximal jejunal lesion inceliac disease and idiopathic sprue. Gastroenterology, 38,28-49.
Shiner, M., and Doniach, I. (1960). Histopathologic studies insteatorrhoea. Gastroenterology, 38, 419-440.
Shorter, R. G., Moertel, C. G., Titus, J. L., and Reitemeier, R. J.(1964). Cell kinetics in the jejunum and rectum of man. Amer.J. dig. Dis., 9, 760-763.
Swanson, V. L., and Thomassen, R. W. (1965). Pathology of thejejunal mucosa in tropical sprue. Amer. J. Path., 46, 511-551.
Townley, R. R. W., Cass, M. H., and Anderson, C. M. (1964). Smallintestinal mucosal patterns of coeliac disease and idiopathicsteatorrhoea seen in other situations. Gut, 5, 51-55.
on 10 Novem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.6 on 1 January 1969. Dow
nloaded from