threatened miscarriage
TRANSCRIPT
ABOUBAKR ELNASHAR
ABOUBAKR ELNASHAR
Vaginal bleeding < 20 ges ws is the commonest
complication in pregnancy, occurring in 1/5 of cases.
17% of cases are expected to present complications
later in pregnancy (Johns et al, 2003).
Management is mostly empirical.
Bed rest is routinely recommended.
ABOUBAKR ELNASHAR
There was a significant association between TM
and:
(Elnashar et al, 1998)
1. Abruptio placentae (bleeding in 2nd trimester)
2. PTL
3. SFGA
4. Increased CS rate (bleeding in 2nd trimester)
ABOUBAKR ELNASHAR
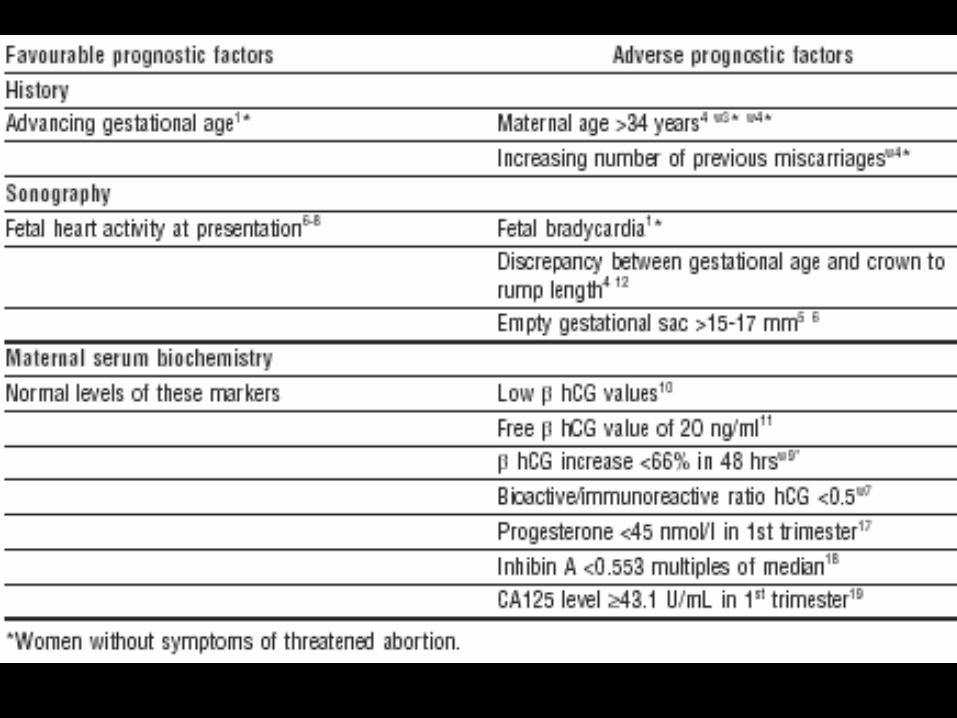
•One in five pregnancies is complicated by TM
•Adverse prognostic factors:
1.
advanced maternal age,
history of RPL,
2.
large empty gest sac,
discrepancy bet gest age &CRL,
fetal bradycardia or absence of FH,
3.
progesterone < 45 nmol/l or
low hCG or inhibin A
ABOUBAKR ELNASHAR
•Favorable prognosis
FH activity and
lack of adverse prognostic factors
•Although bed rest and progesterone supplements
are often advised, little evidence supports their
effectiveness
•Give anti-Rh D Ig to non-sensitized women with
symptoms near, at, or after 12 gest weeks
ABOUBAKR ELNASHAR
ABOUBAKR ELNASHAR
1. Older women (>34 ys)
are at increased risk of miscarriage.
2. Previous miscarriages is associated with
increased risk in future pregnancies, especially in
older women (Falco et al, 1996)
ABOUBAKR ELNASHAR
To dd between genital and extragenital causes.
uterus,
cervix,
vagina, or
extragenital.
ABOUBAKR ELNASHAR
1.DD between intrauterine pregnancy
(viable or non-viable), molar pregnancy,
inevitable abortion.
ABOUBAKR ELNASHAR
U/S findings of TM:
1. Intact pregnancy (50 % )
2. Missed abortion (25 %)
3. Blighted ovum (20 %)
4. Incomplete abortion (3 %)
5. Ectopic pregnancy (2 %)
6. Hydatiform mole (< 1 %)
ABOUBAKR ELNASHAR

ABOUBAKR ELNASHAR
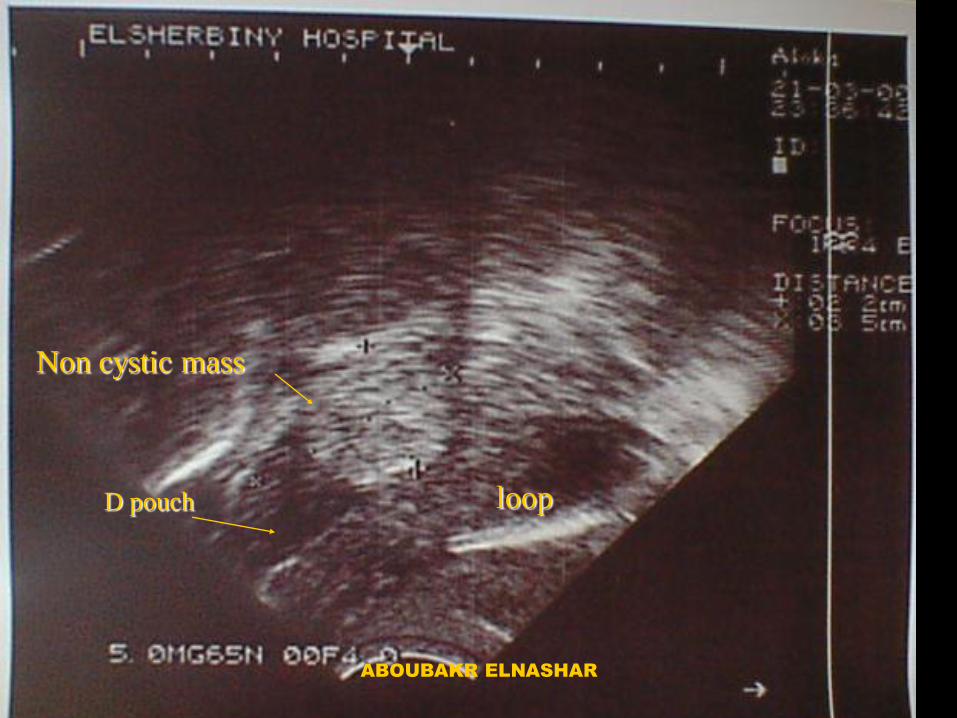
loop
Non cystic mass
D pouch
ABOUBAKR ELNASHAR
2. Prediction of outcome. a. An empty ges sac 15 mm at 7 w & 21 mm at 8 W has diagnostic accuracy of
90.8% (Falco et al, 2003).
b. A mean sac diameter 17 mm without an embryo or 13 mm without a yolk sac can predict non-
viable gestation with a specificity and a positive predictive value of 100%
(Tongsong et al, 1996).
ABOUBAKR ELNASHAR
c. Fetal heart activity should be visible with
TVS once the fetal pole is 5 mm long (Falco et al, 2003). a loss rate of 5% if bleeding occurs after FH starts (Tanninrandorn et al, 2003)
Identification of FH carries a 97% likelihood for the pregnancy continuing beyond 20 ws (Everett et al,1996)
This favorable effect has not been universally repeated, as miscarriage rates of 20-30% have been reported (La Marca et al, 1998)
ABOUBAKR ELNASHAR
d. Fetal bradycardia Discrepancy bet ges sac & CRL Discrepancy bet ges & US age>1w
(Makridimas et al, 2003) increases the rate of abortion from 6% when none are present to 84% when all 3 are present (Falco et al, 1996)
ABOUBAKR ELNASHAR
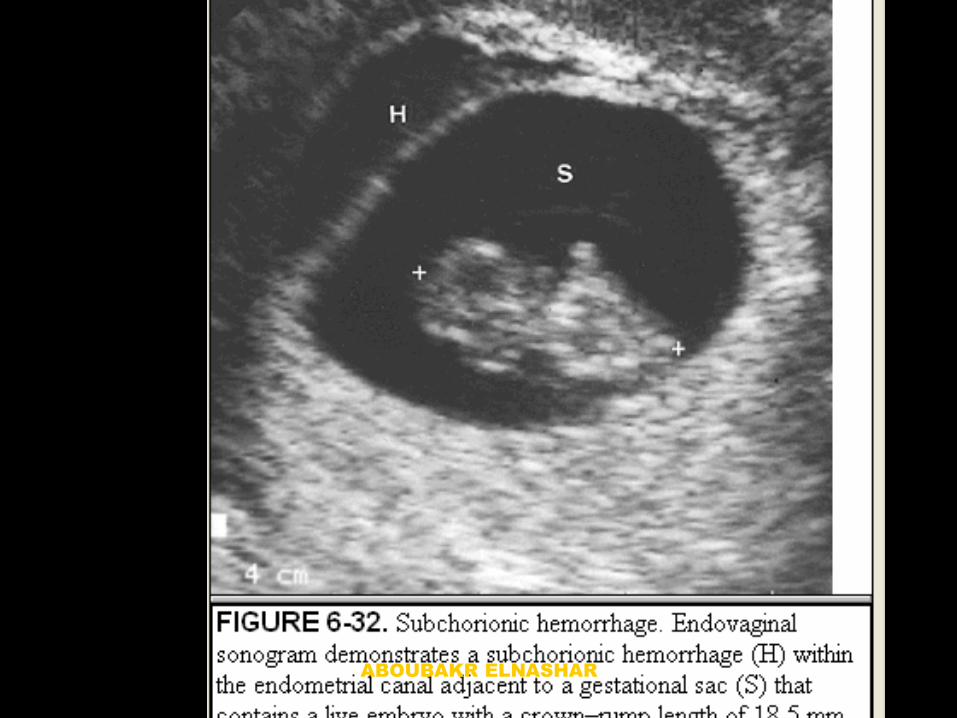
e. Subchorionic haematoma.
•large haematoma:
3fold increase of risk of miscarriage (19% v 71%) (Bennet et al, 1996)
•The presence or the vol of haematoma:
did not affect miscarriage rate (10% v 11%) (Falco et al, 2003)
•Relative vol (vol of haematoma/vol of ges sac)
>40%:
increase risk of miscarriage (Elnashar, 1999)
ABOUBAKR ELNASHAR
ABOUBAKR ELNASHAR
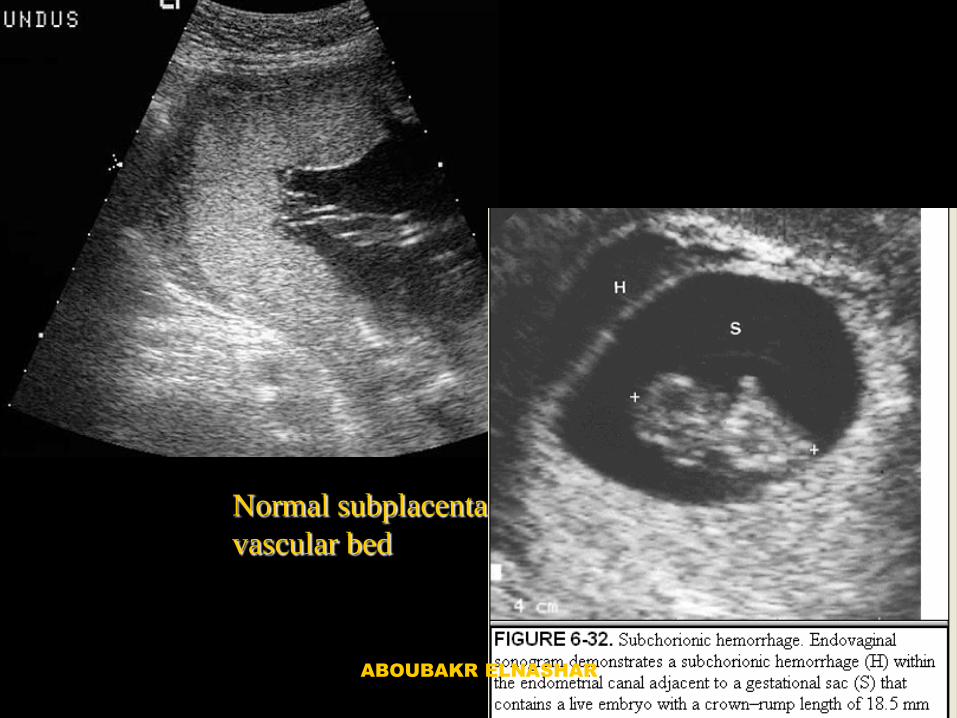
Normal subplacental
vascular bed
ABOUBAKR ELNASHAR
•The presence of haematoma in the first trimester:
increases the risk of severe obstetric complications,
irrespective of the presence of symptoms of TM (Nagy et al, 2003)
•However, the presence of a haematoma did not
influence the risk for subsequent complications in a
smaller study of symptomatic women (Johns et al, 2003)
ABOUBAKR ELNASHAR
1.HCG:
a. In first trimester a free hCG cut-off value of 20
ng/ml could dd bet normal (control and
threatened continuing)& abnormal (non-
continuing TM and tubal) pregnancies, with
88.3% sensitivity and
82.6% positive predictive value (Alsebaie et al, 1996)
ABOUBAKR ELNASHAR
b. The bioactive to immunoreactive ratio of serum
hCG was higher in symptomatic women who
continued with pregnancy than in women who
eventually miscarried (Tongsong et al, 1995)
ABOUBAKR ELNASHAR
2. Progesterone concentrations
•5.1 ng/ml: The lowest concentration associated with
a viable first trimester pregnancy (Tannirandorn et al, 2003)
•25 ng/ml: 97% likelihood for viable IU pregnancy
more sensitive than two serial hCG measurements (Everett et al, 1996)
•<14 ng/ml (45 nmol/l ) dd bet abnormal and normal
(ongoing) pregnancies, with a sensitivity of 87.6% &
specificity of 87.5% (Alsebaei et al, 1995)
3. CA125:
•Constant or increasing over 5-7 days: Miscarriage
•Constantly low or steeply declining: Pregnancy
continuation (Schmidt et al, 2001)
•>43.1 IU/ml: greater risk of miscarriage (Fiegler et al, 2003)
ABOUBAKR ELNASHAR
4. Pregnancy associated placental protein A
(PAPP-A) is lower in symptomatic women with FH
than in normal controls,
its predictive value for miscarriage was only 18.7% (Ruge et al, 1990)
ABOUBAKR ELNASHAR

ABOUBAKR ELNASHAR
•Doctors:
96% prescribe bed rest
1/8: it is mandatory
1/3: it affects outcome (Everett et al,1987)
• One small RCT
one observational study
one retrospective study, yielding conflicting results.
•An observational cohort study:
Bed rest: Miscarriage rate of 9.9%
No bed rest: Miscarriage rate 23.3% (P = 0.03) (Ben-Haroush et al, 2003).
ABOUBAKR ELNASHAR
Cochrane library (2005):
•There is insufficient evidence of high quality that
supports bed rest in order to prevent miscarriage in
women with confirmed fetal viability and vaginal
bleeding in first half of pregnancy
•There was no statistically significant difference in
the risk of miscarriage in the bed rest group Vs the
no bed rest group
•Neither bed rest in hospital nor bed rest at home
showed a significant difference in the prevention of
miscarriage.
ABOUBAKR ELNASHAR
for a couple of days may help women feel safer (La Marca et al, 1998)
thus providing emotional relief.
ABOUBAKR ELNASHAR
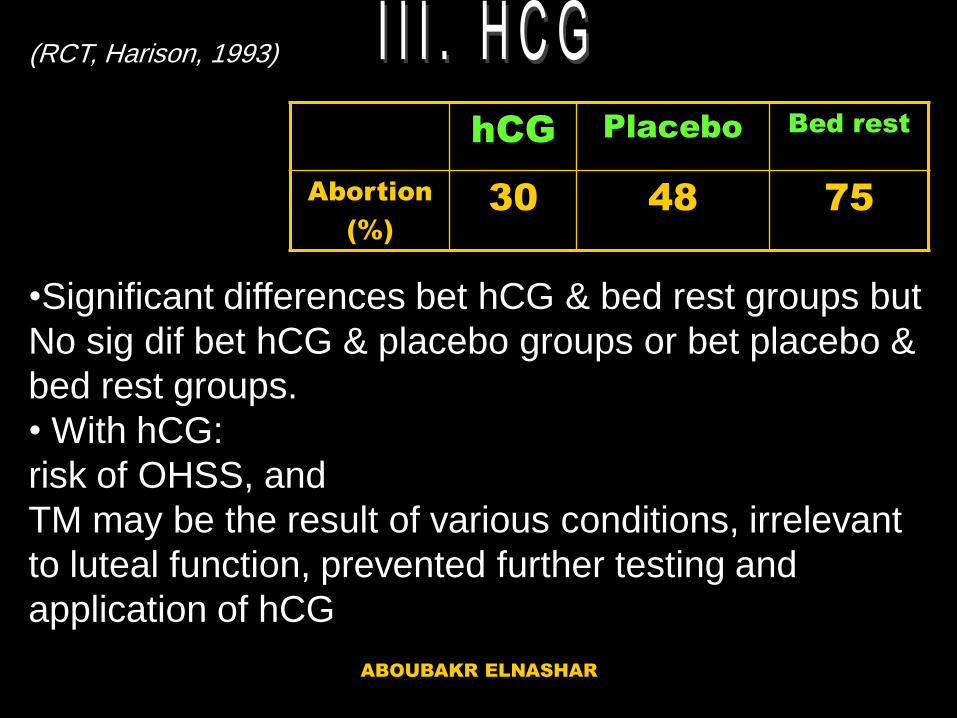
(RCT, Harison, 1993)
•Significant differences bet hCG & bed rest groups but
No sig dif bet hCG & placebo groups or bet placebo &
bed rest groups.
• With hCG:
risk of OHSS, and
TM may be the result of various conditions, irrelevant
to luteal function, prevented further testing and
application of hCG
hCG Placebo Bed rest
Abortion
(%)
30 48 75
ABOUBAKR ELNASHAR
•Prescribed in: 13-40% (Johns et al, 2003)
•Action: Support corpus luteum,
Relax the uterus
•RCT: Progestagen do not improve outcome (Pedersen & Mantoni, 1990; al-Sebaei et al, 1996).
•Local progestogen: decreases uterine
cramping more rapidly than bed rest (Dickey et al, 1992)
ABOUBAKR ELNASHAR
RCT:
Buphenine hydrochloride was better than placebo (Nagy et al, 2003) Cochrane library (2005):
There is insufficient evidence to support the use of
uterine muscle relaxant drugs for women with TM
ABOUBAKR ELNASHAR
RCOG & ACOG Guidelines:
•Rh D alloimmunisation attributable to first trimester
TM is rare
•Anti-D Img:
1. Non-sensitized Rh D negative with TM after 12 w
2. Heavy or repeated bleeding or
abdominal pain, particularly as gestation
approaches 12 w.
3. Not necessary in TM with a viable fetus &
cessation of bleeding <12 w
ABOUBAKR ELNASHAR
ABOUBAKR ELNASHAR
•TM occurs often and is a serious emotional
burden for women.
•Sonographic evaluation can dd between IU
and extrauterine pregnancy and offer some
prognostic clues.
•Demonstration of FH is associated with a
successful pregnancy rate of 85-97%,
•An empty large ges sac or a discrepancy bet
menstrual & sonographic age of >week
indicates a poor prognosis.
•Advanced maternal age and increasing
number of previous miscarriages deteriorates
prognosis.
ABOUBAKR ELNASHAR
•Serum hCG, progesterone, & CA125
concentrations may be helpful as
predictors; however, these tests may not
be useful in primary care settings.
•Although many women with TM are
given progestogens and are prescribed
bed rest, little evidence supports these
policies.
•Short term abstinence from usual
activity may be feasible for women to
relieve their stress.
•Rhesus sensitization is rare after first
trimester TM; however, anti-D Ig should
ABOUBAKR ELNASHAR

ABOUBAKR ELNASHAR