thoraco lumbar spine injury
TRANSCRIPT

THORACOLUMBAR SPINE INJURY
Dr. Kevin J. Ambadan

ANATOMY OF THE CORD AND CAUDA
• Spinal cord from foramen magnum to L1
• Conus at L1 for bowel and bladder (nervi eriganties S1-S5)
• Peripheral nerves for lower extremities start from T9-T12
• L1 roots start innervation of lower extremities
• Thoracic blood supply to the cord tenuous at T10-T12 (artery of Adamkowitz)
• Lumbar blood supply abundant

PHYSIOLOGICAL ANATOMY OF THE THORACIC SPINE
• Facets lie in the frontal plane- allowing rotation
• Ribs resist rotation and add 3x the normal stiffness in lateral rotation
• Kyphosis of the T spine loads the anterior column
• Lower 2 vertebra have floating ribs and no costotransverse articulations
• Canal size in thoracic spine relatively small

PHYSIOLOGICAL ANATOMY OF THE LUMBAR SPINE
• Large discs allow more ROM
• Facets prevent rotation
• Spinal canal wider
• Lordosis is natural alignment
• Lordosis loads the facets

THORACOLUMBAR JUNCTION
• Thoracic spine stiffer in flexion (ribs) than lumbar spine (stress riser)
• Lowest 2 thoracic vertebra have less extrinsic stability secondary to changes in facet orientation and floating ribs (T11-12 have frontal facets but no conjoined ribs to stabilize, therefore less rotational resistance)
• In pure axial loading, thoracic spine deforms into kyphosis and lumbar spine into lordosis leaving the transition vertebra exposed to pure compression
• Force distributed over 10 thoracic and 4 lumbar vertebra is withstood only by 2 vertebra at the thoracolumbar junction

MECHANISMS OF INJURY
• Low-Energy Insufficiency Fractures arising from comparatively mild compressive stress in osteoporotic bone
• Minor Fractures of the Vertebral Processes due to compressive, tensile or tortionalstrains
• High-Energy Fractures or Fracture-Dislocations due to major injuries sustained in motor vehicle collisions, falls or diving from heights, sporting events, horse-riding and collapsed buildings.
• Neurological complications are mainly associated with the third group.

• Flexion Compression – failure of the anterior column and wedge-compression of the vertebral body. Usually stable, but greater than 50 per cent loss of anterior height suggests some disruption of the posterior ligamentous structures.
• Lateral compression – lateral wedging of the vertebral body resulting in a localized ‘scoliotic’ deformity.
• Axial compression – failure of anterior and middle columns causing a ‘burst’ fracture and the danger of retropulsion of a posterior fragment into the spinal canal. Often unstable.
• Flexion–rotation – failure of all three columns and a risk of displacement or dislocation. Usually unstable.
• Flexion–distraction – the so-called ‘jack-knife’ injury causing failure of the posterior and middle columns and sometimes also anterior compression.
• Extension – tensile failure of the anterior column and compression failure of the posterior column. Unstable.
MECHANISMS OF INJURY

IMAGING - XRAYS
AP View:
• May show loss of height or splaying of the vertebral body with a crush fracture.
• Widening of the distance between the pedicles at one level, or an increased distance between two adjacent spinous processes, is associated with posterior column damage.
Lateral View:
• Examined for alignment, bone outline, structural integrity, disc space defects and soft-tissue shadow abnormalities.
• Evidence of fragment retropulsion towards the spinal canal.

IMAGING – CT & MRI
• Rapid screening CT scans are now routine in many accident units.
• More reliable than x-rays in showing bone injuries throughout the spine, and indispensable if axial views are necessary,
• Eliminate the multiple attempts that may be required to ‘get the right views’ with plain x-rays.
• MRI also may be needed to evaluate neurological or other soft-tissue injuries.

COBB’S ANGLE
• Used to classify sagittal plane deformity, especially in the setting of traumatic thoracolumbar spine fractures.
• Cobb angle is defined as the angle formed between a line drawn parallel to the superior endplate of one vertebra above the fracture and a line drawn parallel to the inferior endplate of the vertebra one level below the fracture.
• The Cobb angle is the preferred method of measuring post-traumatic kyphosis in a recent meta-analysis of traumatic spine fracture classifications
• Scoliosis is defined as a lateral spinal curvature with a Cobb angle of 10° or more


CLASSIFICATION SYSTEM
• Holdsworth 2 column theory
• Denis 3 column theory

3 COLUMN THEORY - DENIS 83
• Based on radiographic review of 412 cases
• 5 types, 20 subtypes• Anterior- ALL , anterior 2/3 body• Middle - post 1/3 body, PLL• Posterior- all structures posterior to PLL
• Same as Holdsworth• Posterior injury-not sufficient to cause instability
Spinal injury and Three column concept:
• One column injury is stable
• Two column injury is unstable
• Three column injury is invariably unstable


CLASSIFICATION OF INJURIES
• Simple Compression (1-2 column injury)
• Stable burst (2-3 column injury)
• Unstable burst (3 column injury)
• Flexion distraction (2 nonconjoined columns)
• Chance (3 column failure all in tension)
• Fracture dislocation (3 column injury)
• Pure Dislocation (rare) (3 column injury)
• Pathological (any and all)
• Insufficiency (any and all)
• Multiple contiguous fractures (nly 1-2 columns)

COMPRESSION FRACTURES
• Only anterior column injury
• Middle and post. OK
• Ant. column less than 30%
• No more than 10 degrees kyphosis
• No neuro injury

FLEXION DISTRACTION
• Easy to miss - may look benign
• Anterior column > 50% crushed
• Middle column mainly intact
• Significant spinous process widening
• Unstable

STABLE BURST
• Both ant and middle column involvement
• Minimal kyphosis
• No neuro involvement
• No laminar fracture
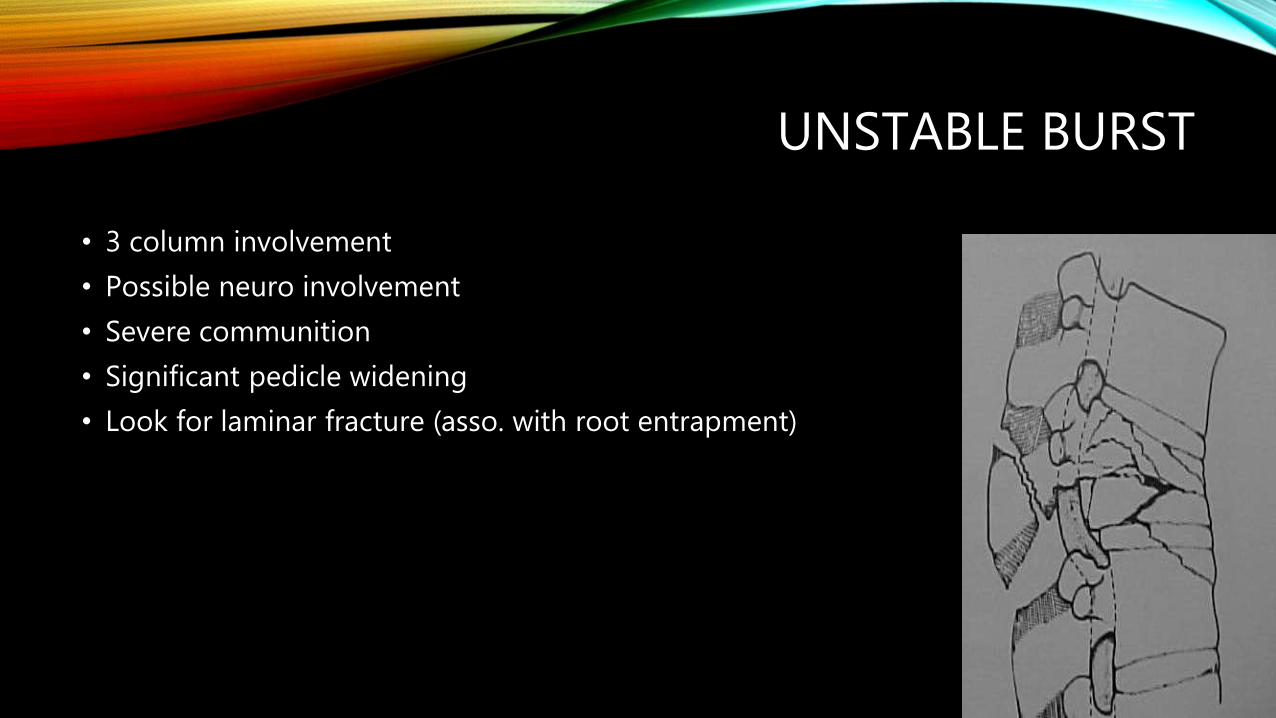
UNSTABLE BURST
• 3 column involvement
• Possible neuro involvement
• Severe communition
• Significant pedicle widening
• Look for laminar fracture (asso. with root entrapment)

CHANCE FRACTURES
• Old “Seatbelt injuries”
• Center of rotation is anterior to ALL
• May be “bony” chance or purely ligamentous
• Normally neuro intact
• “Bony” stable, ligamentous unstable even though all are 3 column injuries

FRACTURE DISLOCATIONS
• Translation in lower lumbar spine may be developmental (nly L3-S1 spondylolysthesis)
• Always abnormal in thoracic spine (ribs)
• Unstable
• Normally- neuro deficit
• Can be hidden at mid thoracic spine
• 3 column injury

PATHOLOGICAL FRACTURES
• Normally in patient with history of CA
• May be hard to distinguish from insufficiency fracture
• May be multiple levels
• Fracture out of proportion to force of trauma
• Suspicion calls for MRI and ?Bx

INSUFFICIENCY FRACTURES
• Normally in elderly females
• Osteopenia/malacia
• Bones have “washed out” appearance
• Minimal force vectors
• Multiple levels (normally)
• Kyphosis greater than 70 degrees may need surgery
• ?Vertebroplasty

THORACOLUMBAR INJURY CLASSIFICATION AND SEVERITY SCORE
(TLICS)

TREATMENT
• Injuries with 3 points or less = Non Operative
• Injuries with 4 points = Non-Op vs Op
• Injuries with 5 points or more = Surgery

EXAMPLESFLEXION COMPRESSION #
•Flexion compression (morphology) - 1
•Intact (neurology) - 0
•PLC (ligament) no injury - 0
Total Points = 1 point.
Non-Operative

COMPRESSION BURST FRACTURE
•Flexion compression burst - 2
•Intact ( neurology) - 0
•PLC (ligament) no injury (0)
Total Points = 2 point.
Non-Operative

COMPRESSIONBURST # - COMPLETE NEURO INJURY
•Axial compression burst with distraction posterior ligamentous complex -4
•Complete (neurology) - 2
•PLC (ligament) injury – 3
Total Points = 9 point.
Surgery

NON-OPERATIVE TREATMENT OF THORACIC SPINE INJURIES
Brace or Cast Treatment• Compression Fractures
• Stable Burst Fractures
• Pure Bony Flexion-Distraction Injury

SURGICAL MANAGEMENT OF THORACOLUMBAR INJURIES
• Unstable burst fractures
• Purely ligamentous
• Facet dislocations
• Translational injuries
• Neurologic deficit

ANTERIOR COLUMN # TREATMENT
• Simple compressions can be placed in a Jewett or TLSO off the shelf brace and discharged from the ED or office as long as pain is controlled, fracture is stable with new standing x-rays in brace and they don’t have an ileus. Cannot treat fractures above T6 without cervical extension

TLSO

STABLE BURSTS AND LATERAL COMPRESSION #
• Pain management
• Brace management
• Off the shelf TLSO (ThoracoLumboSacral Orthosis) for simple compressions greater than 30% and lateral compressions
• CASH (Cruciform Anterior Spinal Hyperextension) brace for insufficiency #

CASH

COMPLICATIONS FROM FRACTURE
• Pneumothorax (thoracic Fxs with asso rib Fxs)/
• Ileus (30-60%)
• Splenic, liver and vessel injury (mechanism of injury)
• DVT/PE
• Decubitis
• UTI
• Pneumonia
• Renal failure (hydronephrosis from cauda equina involvement)

SURGICAL INDICATIONS
• Neurological Involvement
• Flexion distraction injury
• Greater than 50% canal compromise with >15 degrees kyphosis
• >25 degrees kyphosis
• Failure of stress testing (severe pain, angulation above 25 degrees, neurosymptoms)
• Fracture dislocations
• Soft tissue “chance” fractures

LAMINECTOMY• Indications:
• Comminuted posterior elements causing direct neural compression
• Epidural hematoma requiring evacuation
• Repair of dural tear associated with burst and laminar fractures during posterior instrumentation and fusion
Contraindications:
• Canal compromise >67%
• Delay in operative treatment for > 4 days
• Where pedicle screw insertion is not feasible (atypical morphology, small dimension or traumatic fracture)
Requires intact PLC

VERTEBROPLASTY AND KYPHOPLASTY
Indications:
• Osteoporotic VCF not responding to conservative management
• Spinal metastatic lesions & fractures
• Hemangiomas
Goal of vertebroplasty is to improve strength and stability
Goal of Kyphoplasty is to restore vertebral body height and stability. The use of balooncreates a void for cement placement under lower pressure and thus results in lower incidence of cement extravasation
Can be safely done in patients with refractory pain to conservative treatments.

THANK YOU