the view from the faculty of clinical oncology: a new … · management of late effects and better...
TRANSCRIPT
The View from the Faculty of
Clinical Oncology: a new era for
management of late effects and
better multidisciplinary working?
Dr Diana Tait
Registrar, Faculty of Clinical Oncology,
Royal College of Radiologists
Consultant Clinical Oncologist
The Royal Marsden NHS Foundation Trust.
RCR – FACULTY OF CLINICAL ONCOLOGY
HIGH QUALITY RADIOTHERAPY –
NATIONAL IMPLEMENTATION
MEASURING OUTCOMES
GUIDELINES ON MANAGEMENT
RCR-FACULTY OF CLINICAL ONCOLOGY
HIGH QUALITY RADIOTHERAPY
Escalate Dose to Target
Tumour Control
Minimise Normal Tissue Dose
Late effects
“Conformal radiotherapy, using multi-
leaf collimators which allow treatment
using an irregularly shaped beam, is the
optimum mode of delivery and all
centres should aim to provide this form
of treatment”
National Institute for Clinical Excellence
Guidance on Cancer Services
IMPROVING OUTCOMES IN UROLOGICAL CANCERS The Manual
September 2002

7
8
RCR-FACULTY OF CLINICAL ONCOLOGY
HIGH QUALITY RADIOTHERAPY
PELVIC RT
PROSTATE
BLADDER
GYNAE
RECTUM
ANNUS
THORACIC RT
OESOPHAGUS
OGJ
LUNG
RCR-FACULTY OF CLINICAL ONCOLOGY
HIGH QUALITY RADIOTHERAPY
CT
MRI
PET CT
TARGET
DEFINITION
IMRT
IGRT
SBRT
CyberKnife
Brackytherapy
HIGHLY
CONFORMAL
PORTAL
IMAGES
(MV, KV)
CONE BEAM
VERIFICATION

RCR-FACULTY OF CLINICAL ONCOLOGY
HIGH QUALITY RADIOTHERAPY
AVOID/ DOSE NORMAL TISSUES
PELVIC CONFORMAL TRIAL – 1st
RANDOMISED TRIAL
• LESS ACUTE TOXICITY
• LESS LATE EFFECTS
• IMPROVED QOL
• 1993 ACUTE EFFECTS
• 1997
• 1999 LATE EFFECTS
RCR-FACULTY OF CLINICAL ONCOLOGY
HIGH QUALITY RADIOTHERAPY
ANAL CANCER
ACT II CR Rate 94%
Grade 3-4 Acute Toxicity 61%
RTOG 98-11 - Similar results
RCR-FACULTY OF CLINICAL ONCOLOGY
HIGH QUALITY RADIOTHERAPY
ANAL CANCER - IMRT
RTOG 98 – 11 RTOG 0529
CLINICAL RESPONSES EQUIVALENT
REDUCED Grade 2-3 ACUTE TOXICITY
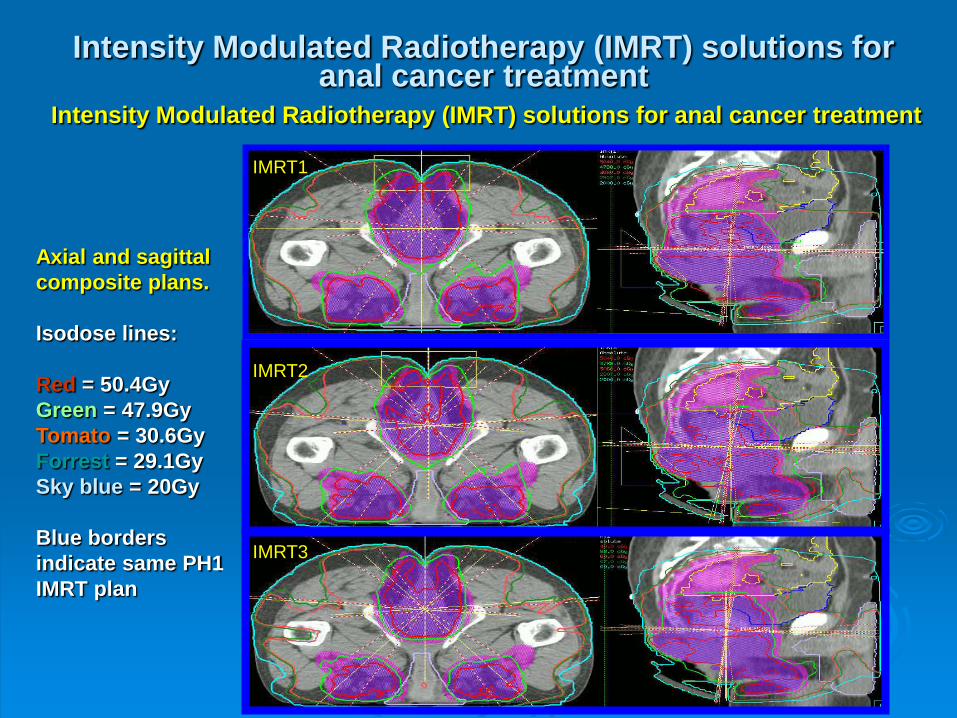
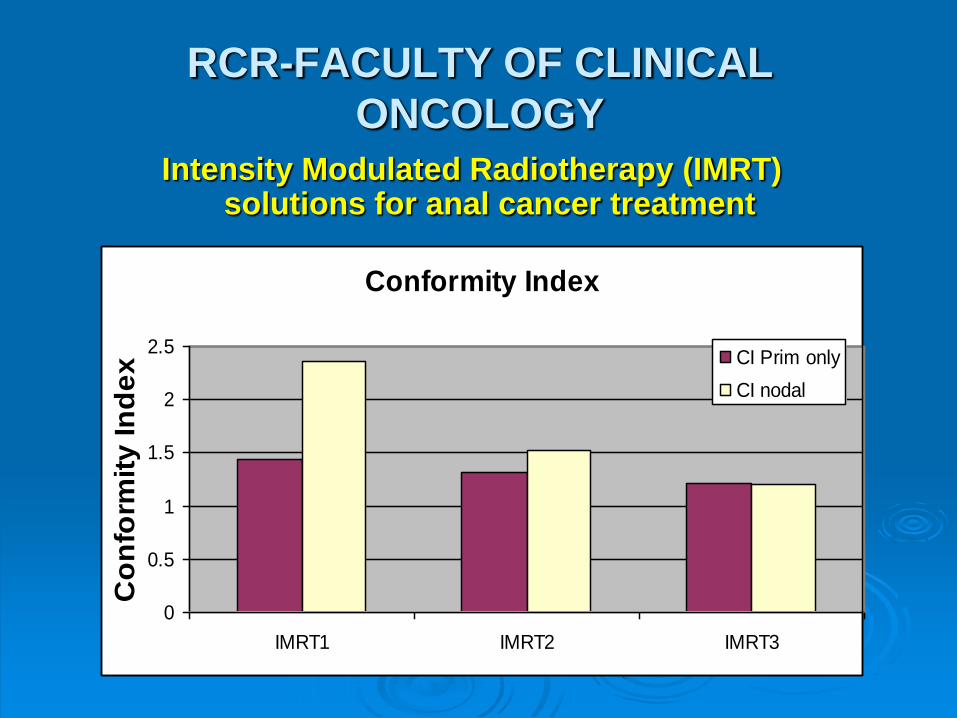
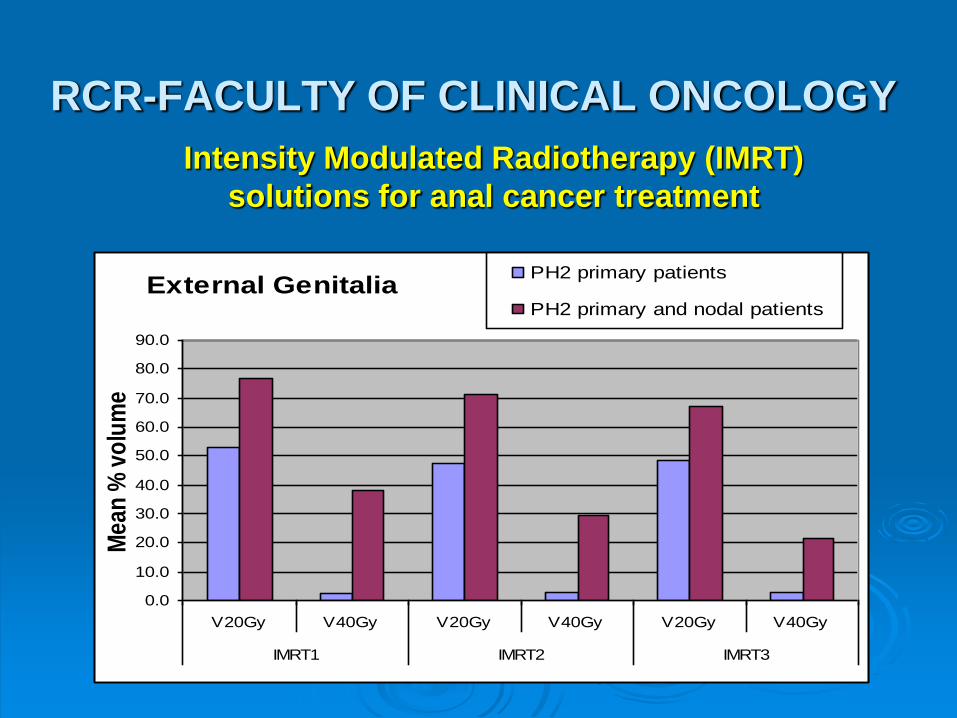
Intensity Modulated Radiotherapy (IMRT) solutions for anal cancer treatment
Intensity Modulated Radiotherapy (IMRT) solutions for anal cancer treatment
Axial and sagittal
composite plans.
Isodose lines:
Red = 50.4Gy
Green = 47.9Gy
Tomato = 30.6Gy
Forrest = 29.1Gy
Sky blue = 20Gy
Blue borders
indicate same PH1
IMRT plan
IMRT2
IMRT1
IMRT3
RCR-FACULTY OF CLINICAL
ONCOLOGY
Intensity Modulated Radiotherapy (IMRT) solutions for anal cancer treatment
Conformity Index
0
0.5
1
1.5
2
2.5
IMRT1 IMRT2 IMRT3
Co
nfo
rmit
y In
de
x CI Prim only
CI nodal
RCR-FACULTY OF CLINICAL ONCOLOGY
External Genitalia
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
V20Gy V40Gy V20Gy V40Gy V20Gy V40Gy
IMRT1 IMRT2 IMRT3
Me
an
% v
olu
me
PH2 primary patients
PH2 primary and nodal patients
Intensity Modulated Radiotherapy (IMRT)
solutions for anal cancer treatment
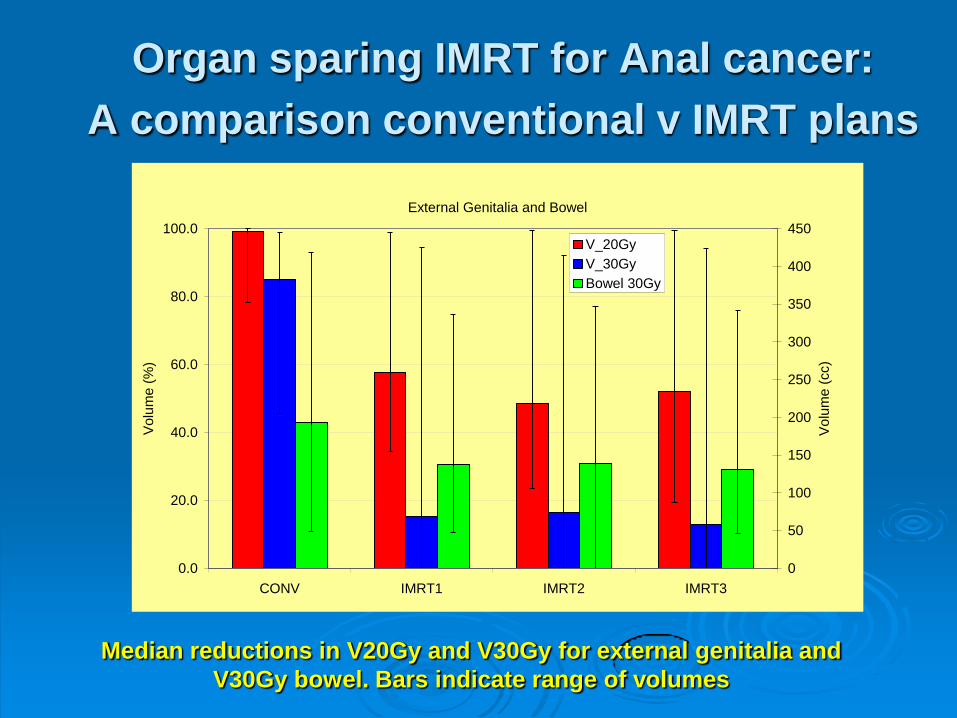
Organ sparing IMRT for Anal cancer:
A comparison conventional v IMRT plans
External Genitalia and Bowel
0.0
20.0
40.0
60.0
80.0
100.0
CONV IMRT1 IMRT2 IMRT3
Vo
lum
e (
%)
0
50
100
150
200
250
300
350
400
450
Vo
lum
e (
cc)
V_20Gy
V_30Gy
Bowel 30Gy
Median reductions in V20Gy and V30Gy for external genitalia and
V30Gy bowel. Bars indicate range of volumes
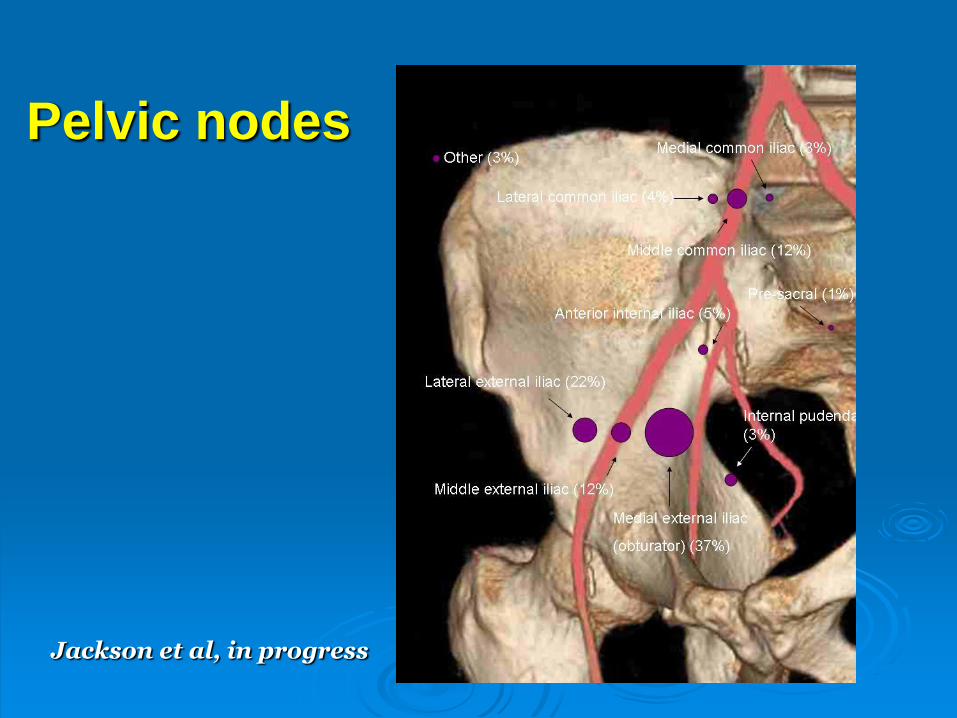
Pelvic nodes
Jackson et al, in progress
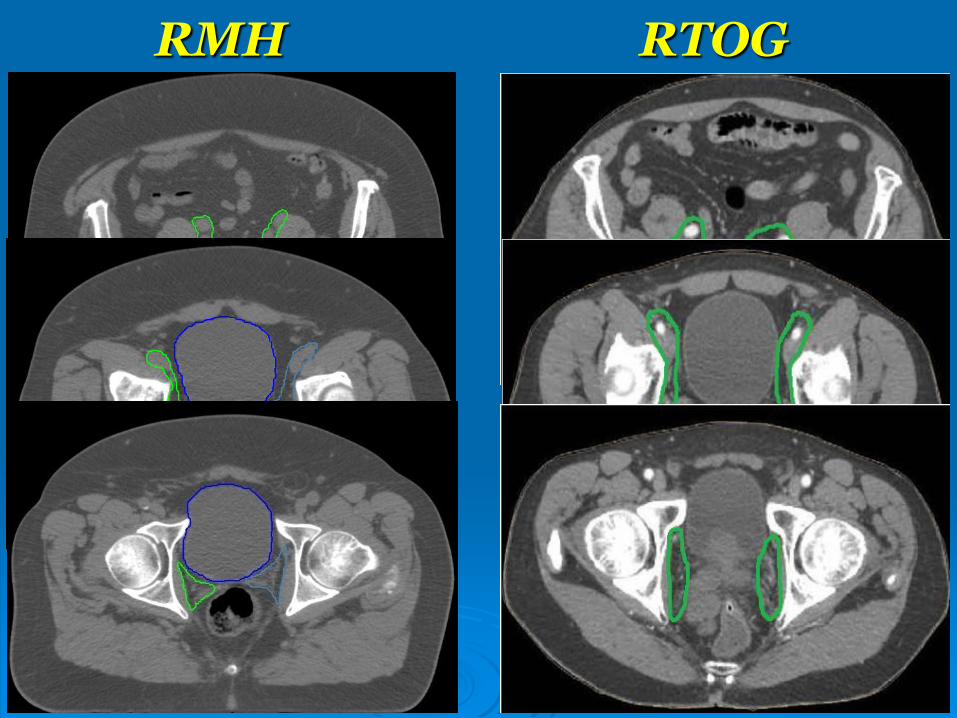
RMH RTOG
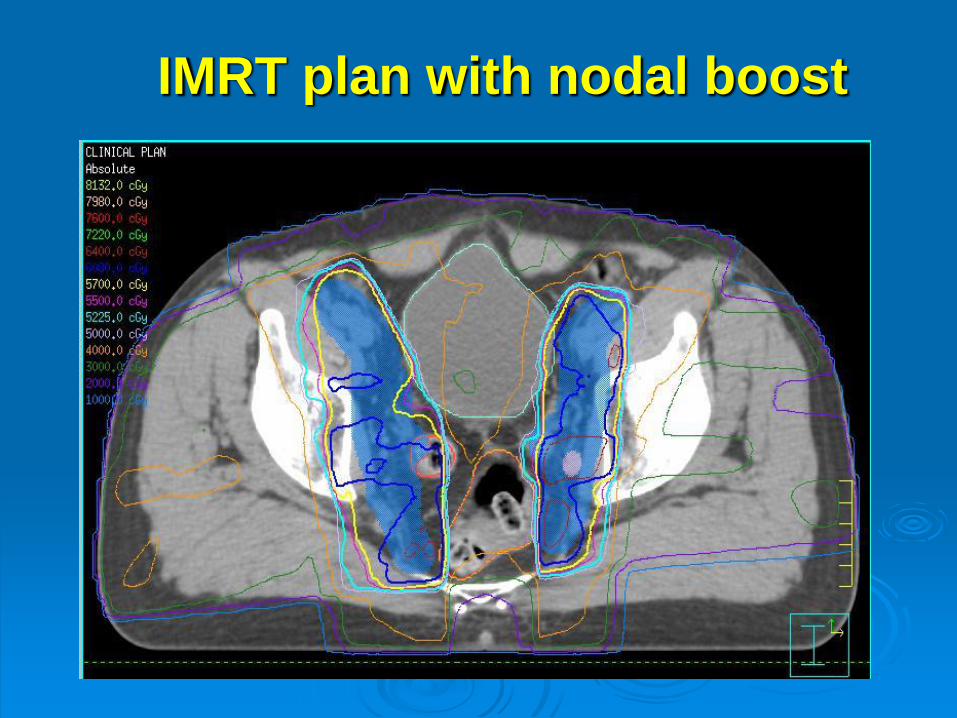
IMRT plan with nodal boost
IMRT can safely deliver 60Gy
to the pelvic lymph node regions
in patients with prostate cancer:
Report of a Phase I/II dose
escalation study
McVey G, Van As N, Thomas K, Bidmead M, South C,
Khoo V, Parker C, Huddart R, Horwich A, Dearnaley D
Royal Marsden Hospital
Pelvic IMRT Trial
60Gy/35# cohort (nodal regions)
135 pts
Nov. 2003 – Dec 2007
Median follow-up 2.9 years (1.9 – 5.8)
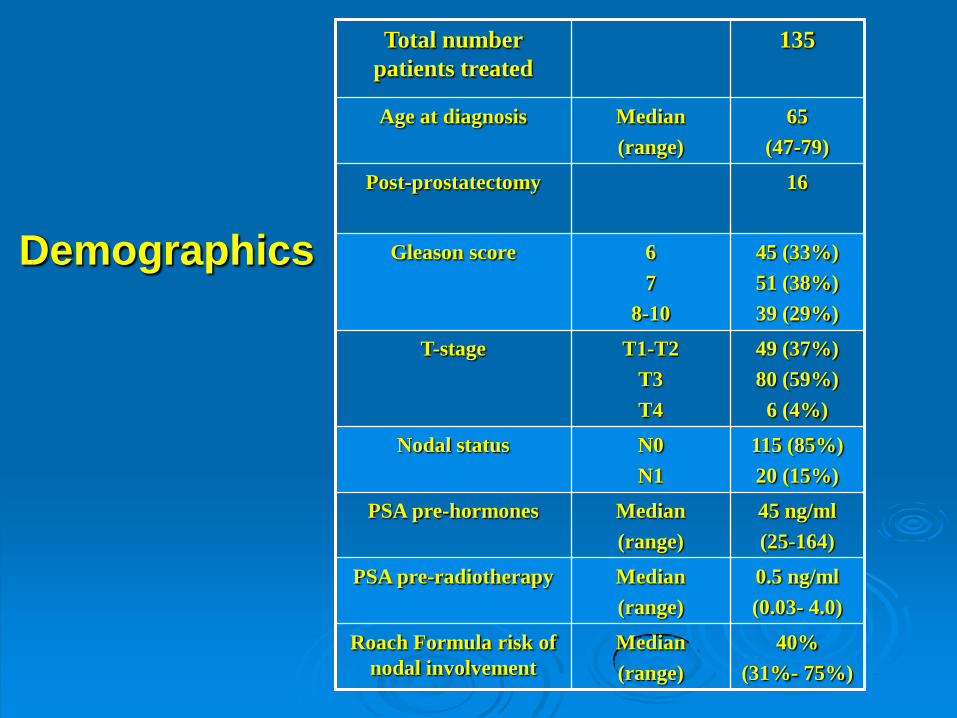
Demographics
Total number
patients treated
135
Age at diagnosis Median
(range)
65
(47-79)
Post-prostatectomy 16
Gleason score 6
7
8-10
45 (33%)
51 (38%)
39 (29%)
T-stage T1-T2
T3
T4
49 (37%)
80 (59%)
6 (4%)
Nodal status N0
N1
115 (85%)
20 (15%)
PSA pre-hormones Median
(range)
45 ng/ml
(25-164)
PSA pre-radiotherapy
Median
(range)
0.5 ng/ml
(0.03- 4.0)
Roach Formula risk of
nodal involvement
Median
(range)
40%
(31%- 75%)
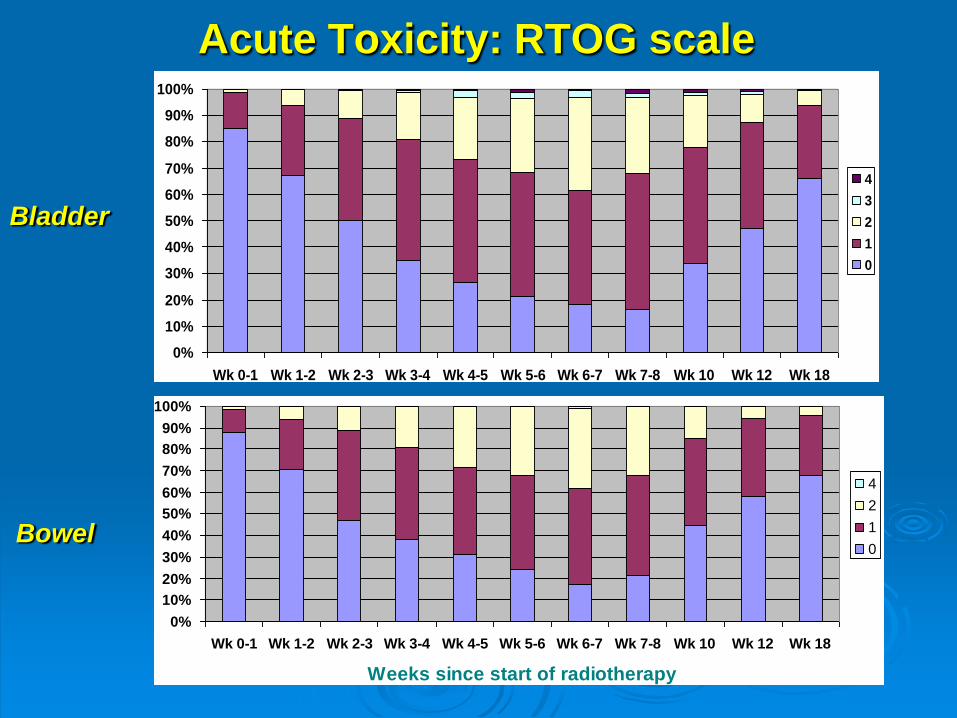
Acute Toxicity: RTOG scale
Acute Bowel RTOG grade
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Wk 0-1 Wk 1-2 Wk 2-3 Wk 3-4 Wk 4-5 Wk 5-6 Wk 6-7 Wk 7-8 Wk 10 Wk 12 Wk 18
Weeks since start of radiotherapy
4
2
1
0Bowel
Acute RTOG Bladder Toxicity
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Wk 0-1 Wk 1-2 Wk 2-3 Wk 3-4 Wk 4-5 Wk 5-6 Wk 6-7 Wk 7-8 Wk 10 Wk 12 Wk 18
4
3
2
1
0
Bladder
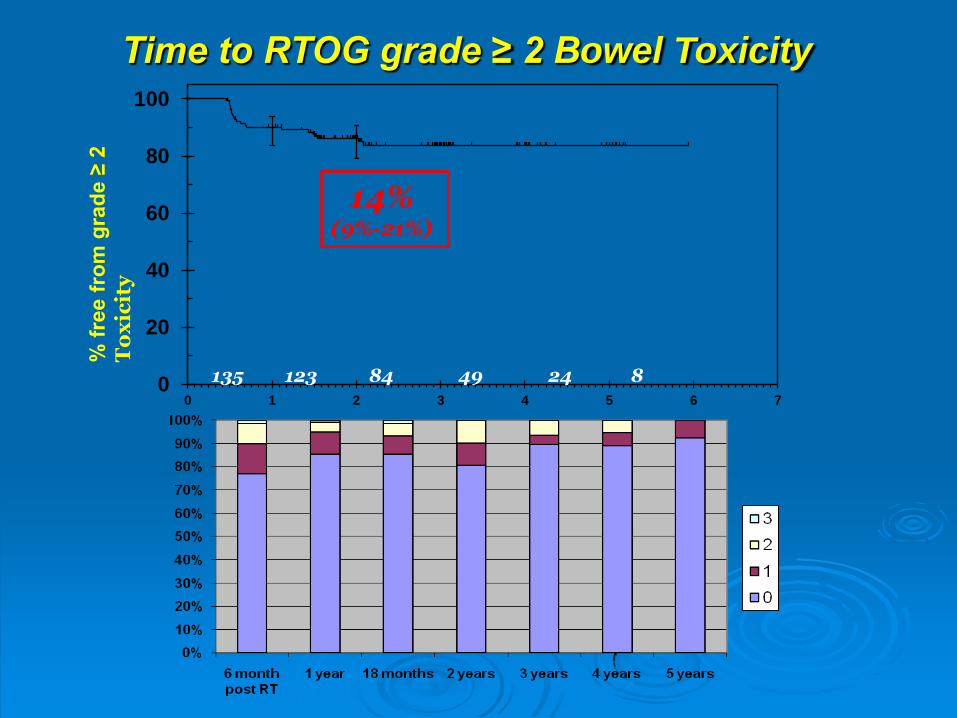
0
20
40
60
80
100
0 1 2 3 4 5 6 7
Time to RTOG grade ≥ 2 Bowel Toxicity %
fre
e f
rom
gra
de ≥
2
To
xic
ity
Years since start of radiotherapy
135 123 84 49 24 8
14% (9%-21%)
RCR-FACULTY OF CLINICAL ONCOLOGY
HIGH QUALITY RADIOTHERAPY –
NATIONAL IMPLEMENTATION
NRAG
NRIG
PEER REVIEW
RCR-FACULTY OF CLINICAL ONCOLOGY
AUDIT
National Audit COAC
National Data Sets
MEASURING OUTCOMES
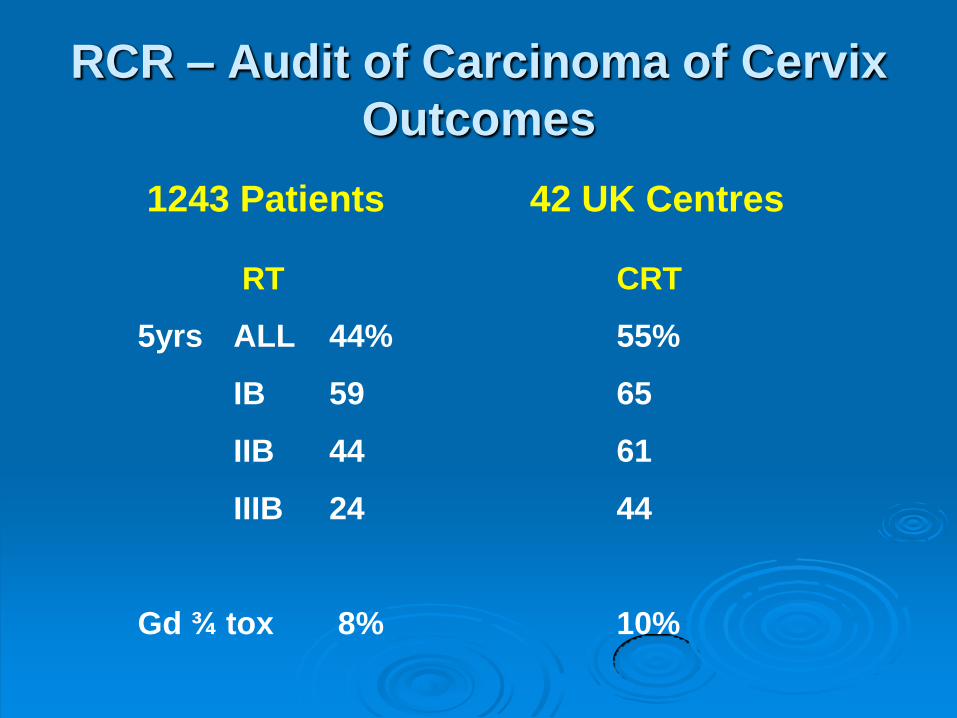
RCR – Audit of Carcinoma of Cervix
Outcomes
1243 Patients 42 UK Centres
RT CRT
5yrs ALL 44% 55%
IB 59 65
IIB 44 61
IIIB 24 44
Gd ¾ tox 8% 10%
RCR-FACULTY OF CLINICAL ONCOLOGY
Practice Guidance on the Management of
Acute and Chronic Gastrointestinal problems
arising as a result of treatment for cancer
Guidelines on Management
The View from the Faculty of Clinical
Oncology: a new era for management
of late effects and better
multidisciplinary working?
Dr Diana Tait
Registrar, Faculty of Clinical Oncology,
Royal College of Radiologists
Consultant Clinical Oncologist
The Royal Marsden NHS Foundation Trust.