the unmet need in copd management: right treatment for the ... · the unmet need in copd...
TRANSCRIPT
The Unmet Need in COPD management: Right treatment for
the Right PatientOng Thun How
Senior Consultant, Department RCCM SGHAdj Assistant Professor YLL and Duke-NUS
Medical School
Please log onto pollev.com/thunong474

• 71 years old• Smoked since 15 years old• Increasing SOB on exertion• “normal cough”
• Thin, BMI 19• L Air Entry poor. No
rhonchi heard • Taking blue inhaler
for some time already
The best initial management of Mr. Lim should beA. Add ipratropium ( atrovent)B. Add theophyllineC. Add long-acting bronchodilatorD. Add combination ICS/LABAE. Do more investigations first
DIAGNOSIS OF COPD GOLD GUIDELINES 2011
Chronic Obstructive Pulmonary Disease (CODP), a common preventable and treatable disease, is characterized by
persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory
response in the airways and the lung to noxious particles or gases. Exacerbations and comorbidities contribute to
the overall severity in individual patients.

Diagnosis of COPD
• Clinical history:– Chronic cough– Chronic Decreased effort tolerance– Wheeze– SMOKER
• Unlike in asthma, Spirometry and CXR are mandatory for diagnosis and long-term management
Symptoms of COPD• Dyspnea:
– Progressive– Usually worse with exercise– Persistent– Many patients ( especially locally!) don’t complain
– they tailor activities to effort tolerance– Age per se does not cause dyspnea!
Symptoms of dyspnea
• Chronic cough– “smoker’s cough”– May be intermittent and may be unproductive
• Chronic sputum production– Any pattern of chronic sputum production may
indicate COPD
• History of exposure to risk factors– Smoking– Occupational dusts/chemicals– Smoke from home cooking and heating fuels
Causes of wheezing: top ten list• Bronchitis• Asthma• COPD• CCF• Vocal cord dysfunction• Foreign body• Recurrent aspiration• Bronchiectasis• Pulmonary embolism• Tumor• Broncholith/ airway stricture
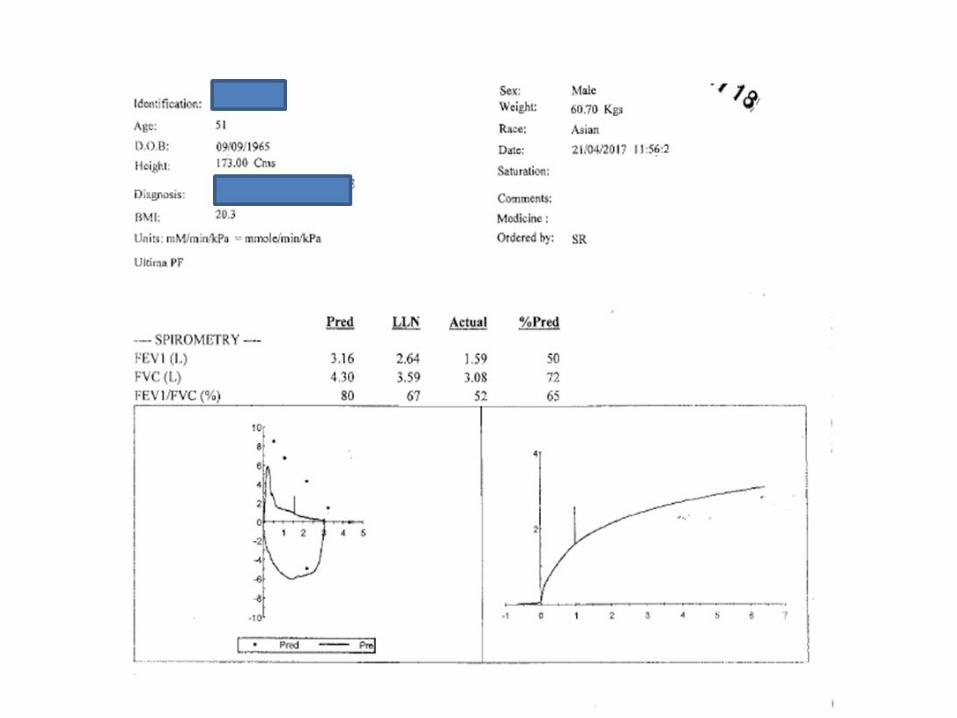

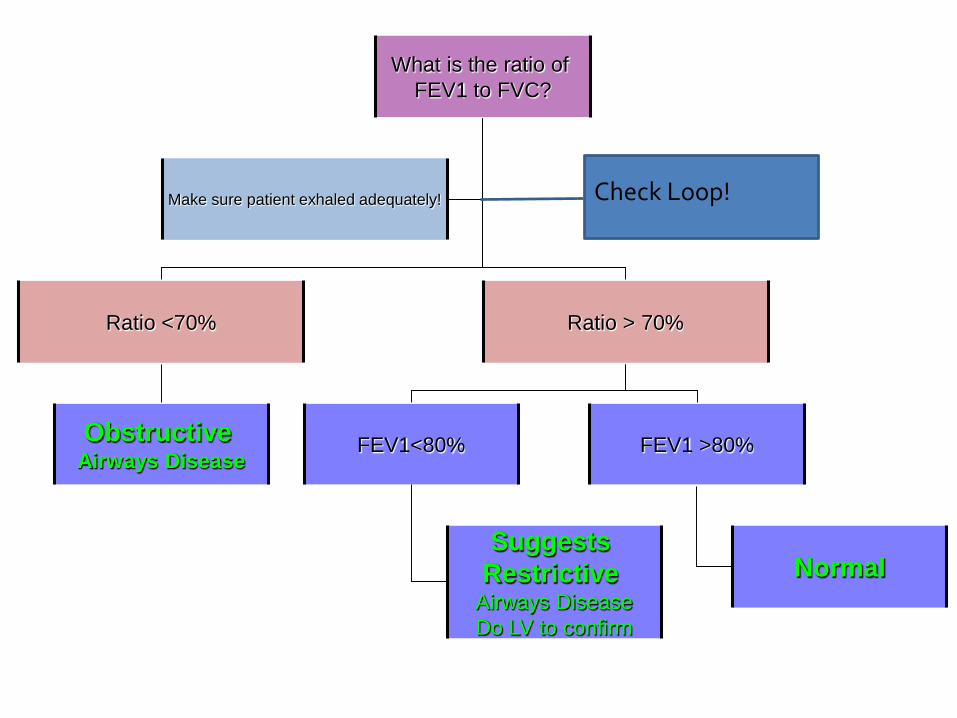
What is the ratio of FEV1 to FVC?
Ratio <70% Ratio > 70%
Obstructive Airways Disease
FEV1<80% FEV1 >80%
Suggests Restrictive
Airways DiseaseDo LV to confirm
Normal
Make sure patient exhaled adequately! Check Loop!

CXR

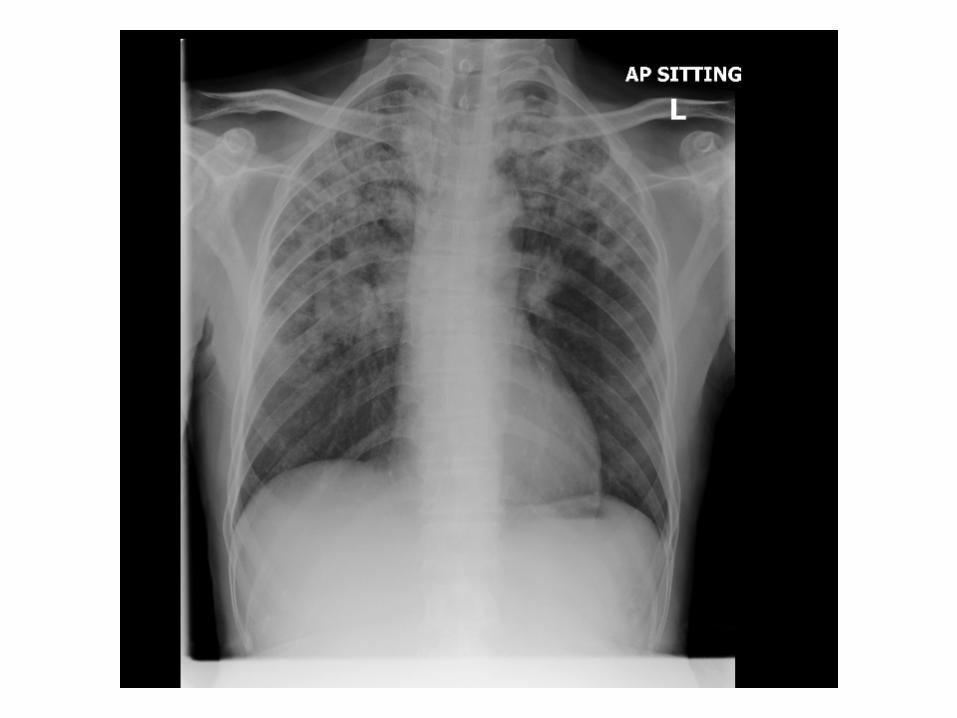

ONEGet the diagnosis right – COPD has
many mimics!
ONETWOTHREEFOUR FIVESIX
• Confirmed diagnosis of COPD from • History, • CXR to exclude other pathology, • Spirometry with obstructive ratio FEV1/FVC. FEV1 56%
predicted.
• He has been to see you in clinic three times over the last year –requiring antibiotics and prednisolone each time and needed a neb in your clinic once.
• He’s complaining that he’s breathless walking up to his 4th floor office
How bad is his COPD ( and why do you care anyway?)
A. .B. .C. .D. .
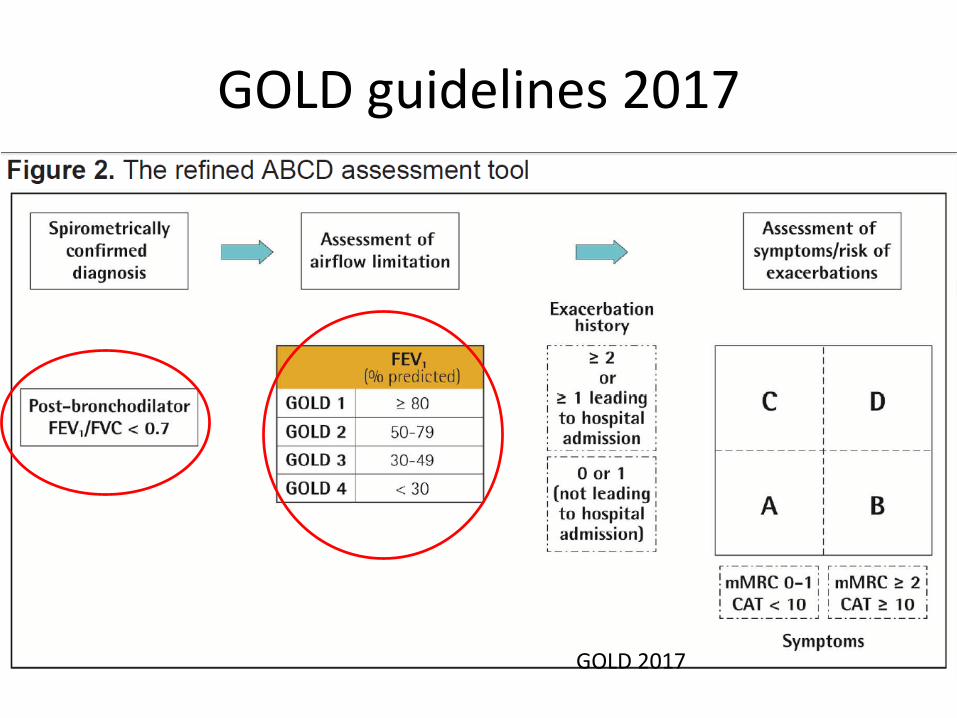
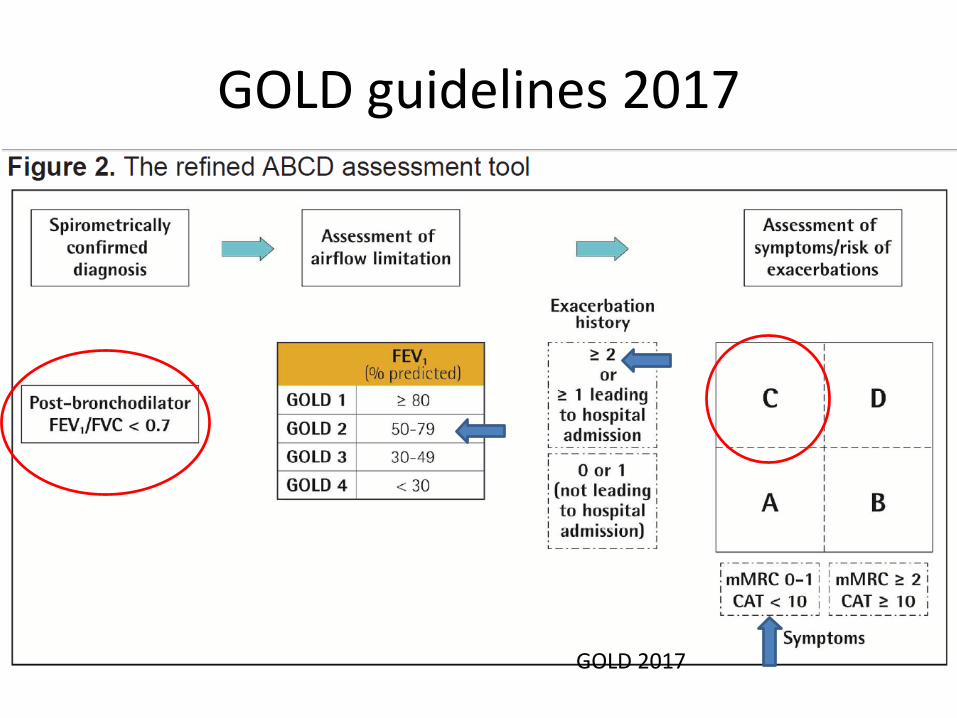
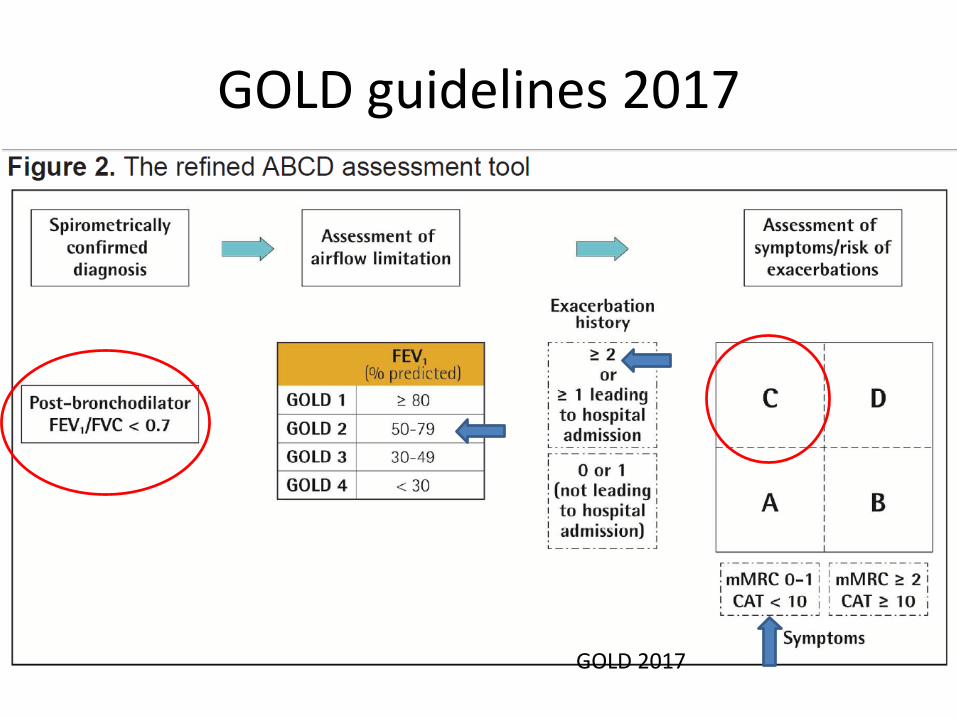
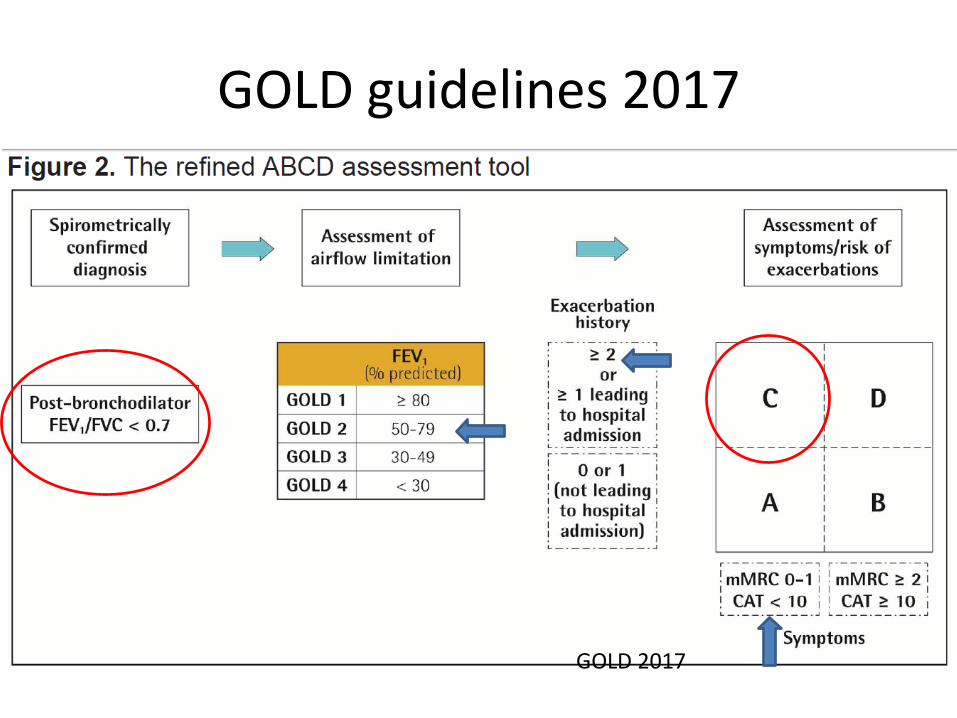
GOLD guidelines 2017
GOLD 2017
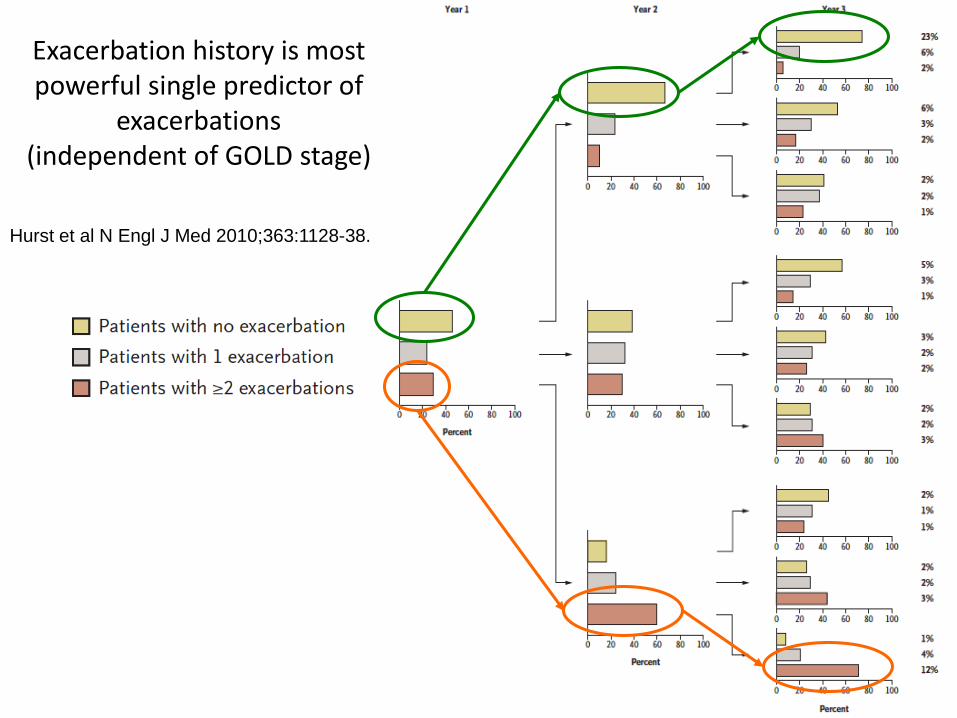
Hurst et al N Engl J Med 2010;363:1128-38.Exacerbations in following year
Exacerbation history is most powerful single predictor of
exacerbations (independent of GOLD stage)
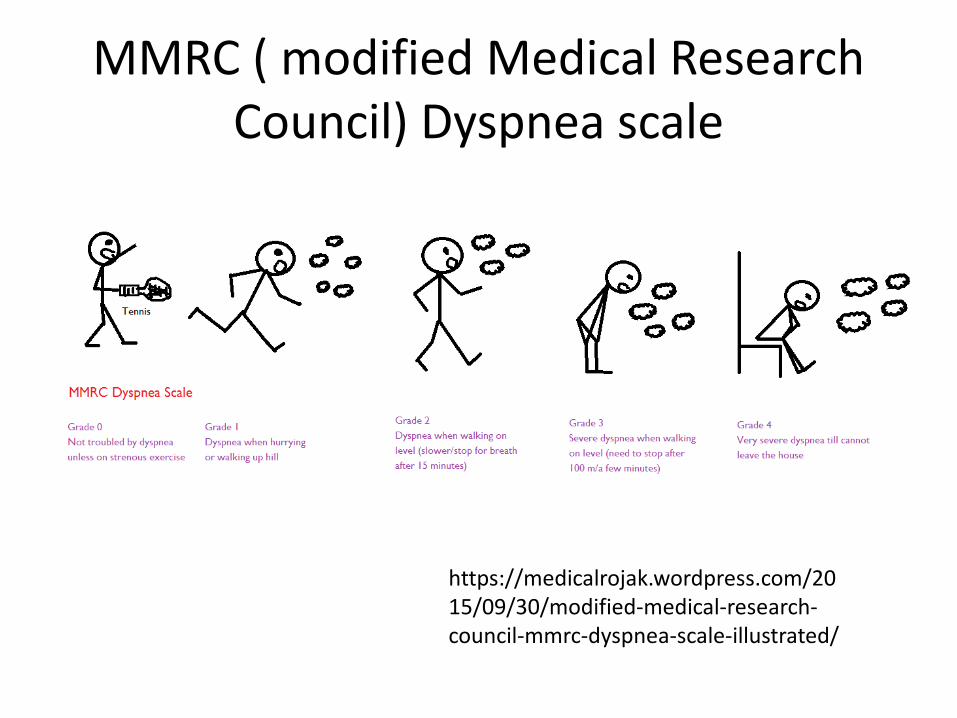
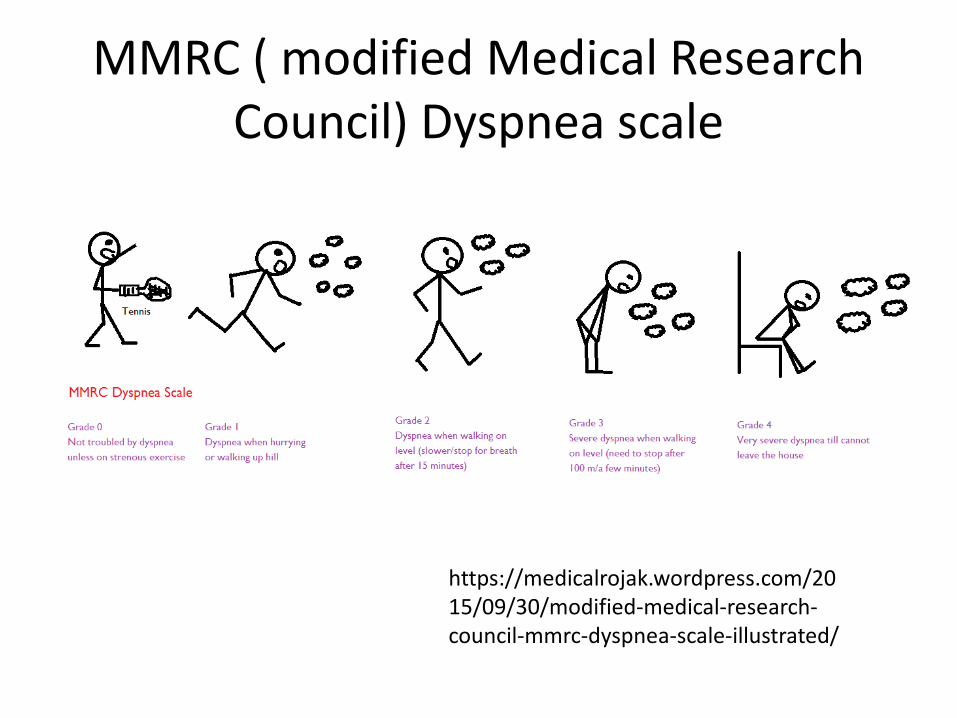
MMRC ( modified Medical Research Council) Dyspnea scale
https://medicalrojak.wordpress.com/2015/09/30/modified-medical-research-council-mmrc-dyspnea-scale-illustrated/
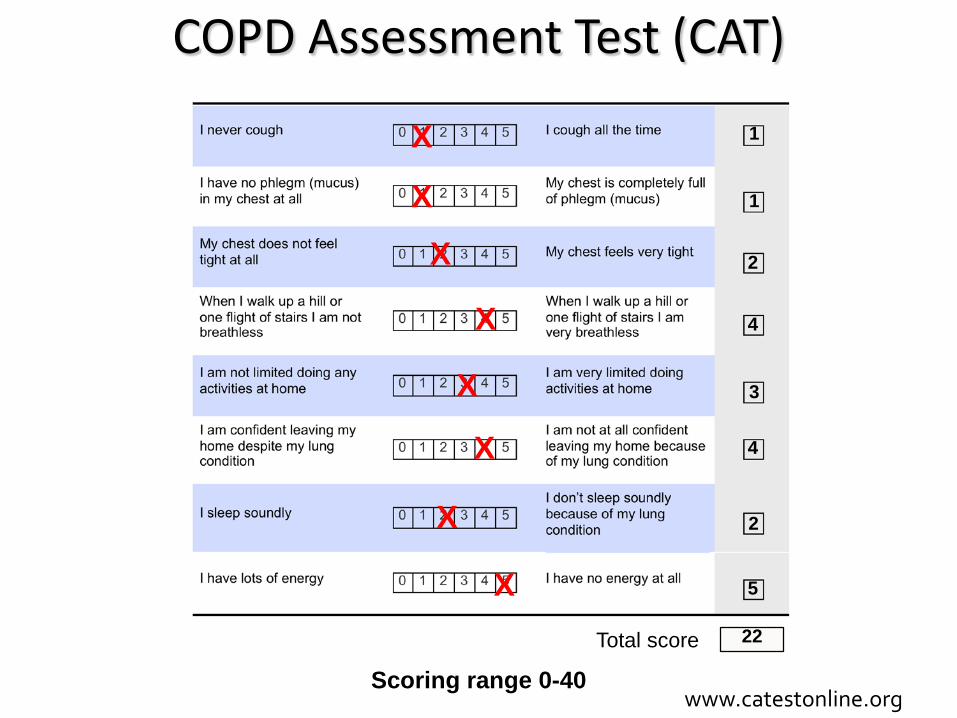
Scoring range 0-40
COPD Assessment Test (CAT)
Total score
1
1
2
4
3
4
2
5
22
X
X
X
X
X
X
X
X
www.catestonline.org

Correlation between CAT and SGRQ (US, n=227)
0
5
10
15
20
25
30
35
40
0 10 20 30 40 50 60 70 80 90 100
CATscore
SGRQ score
r = 0.80
Jones et al. Eur Respir J 2009; 34: 648–654
China
Europe
GOLD guidelines 2017
GOLD 2017
TWOObjective assessment of breathlessness and
exacerbation history needed forABCDs of COPD
• He has been to see you in clinic three times over the last year –requiring antibiotics and prednisolone each time and needed a neb in your clinic once.
• He’s complaining that he’s breathless walking up to his 4th floor office
Does ABCD matter?

http://hardluckasthma.blogspot.sg/2012/01/history-of-back-door-bronchodilators.html
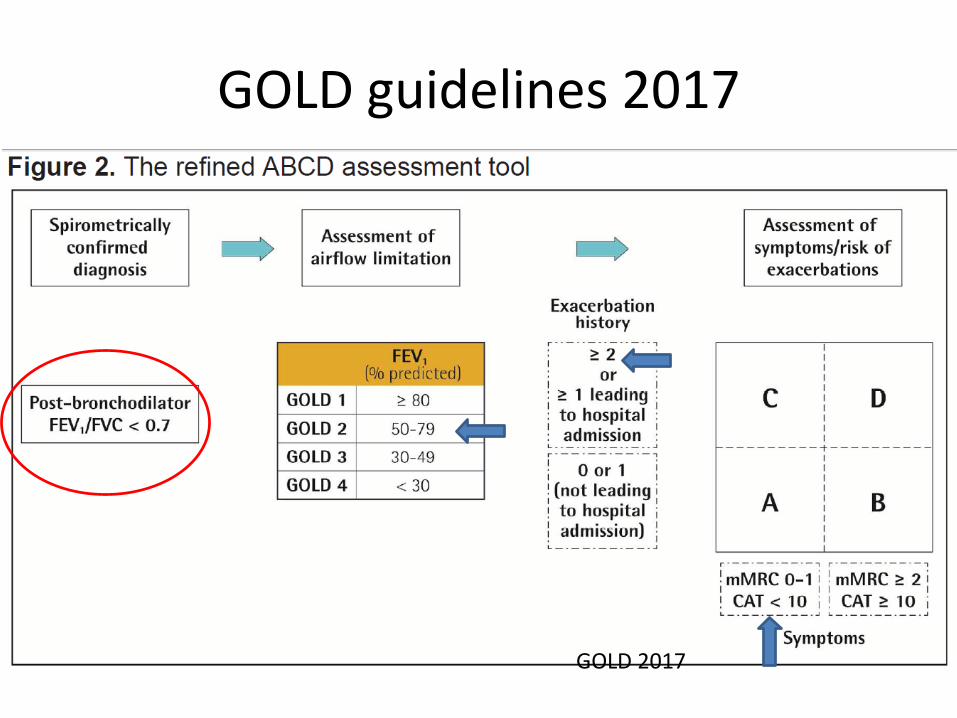
GOLD guidelines 2017
GOLD 2017

Short-Acting Bronchodilators
MMRC ( modified Medical Research Council) Dyspnea scale
https://medicalrojak.wordpress.com/2015/09/30/modified-medical-research-council-mmrc-dyspnea-scale-illustrated/
GOLD guidelines 2017
GOLD 2017
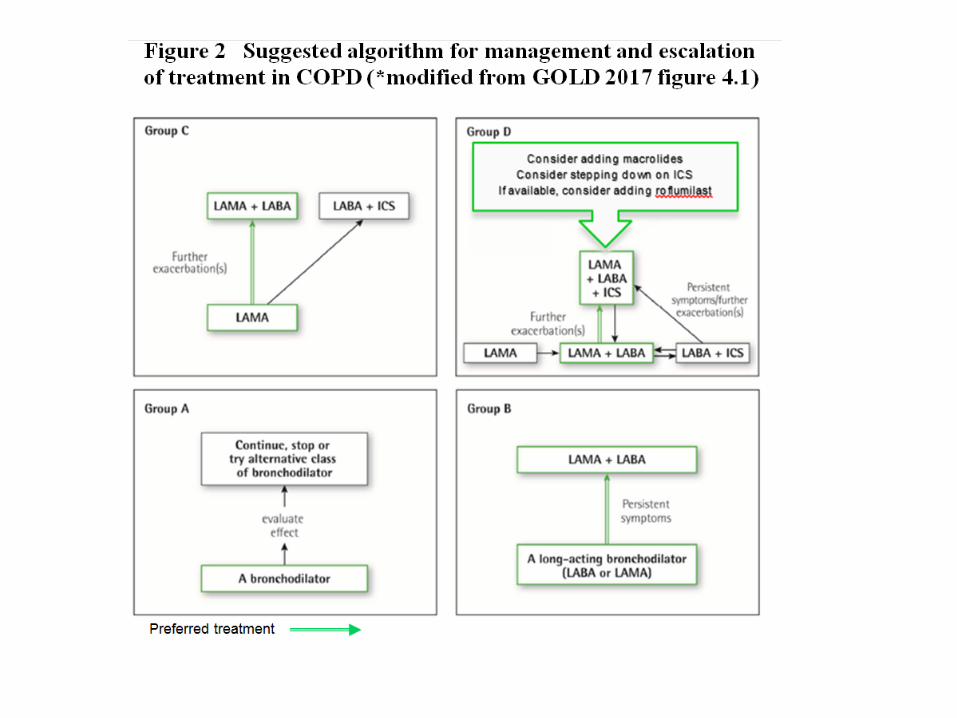
THREETreatment of acute COPD
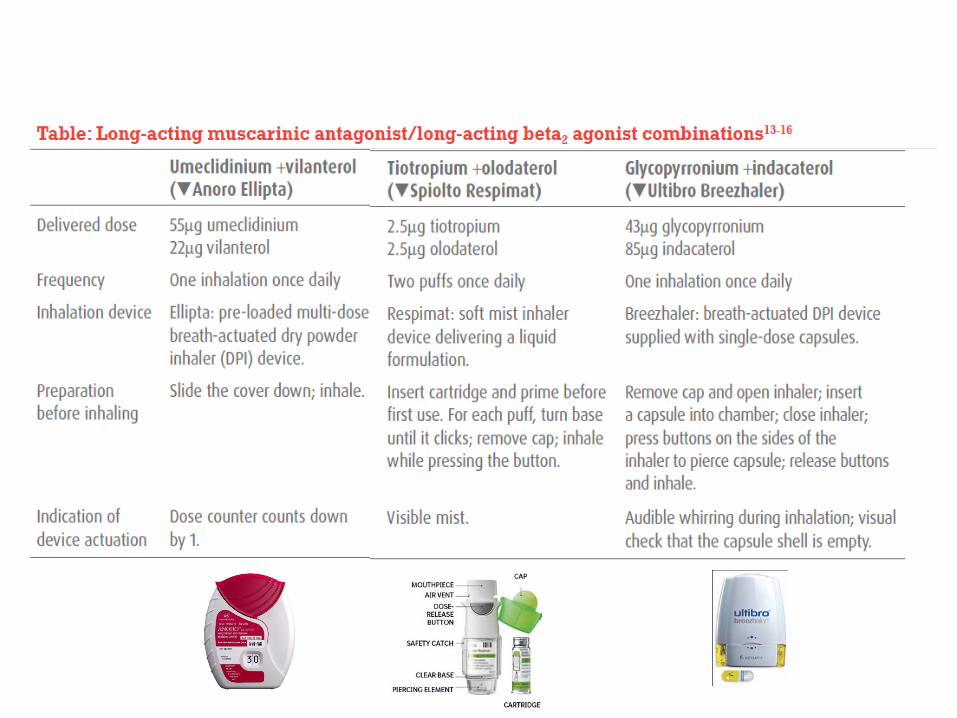
Long-acting Bronchodilators
LAMAs LABAs 喇叭

Long-acting Bronchodilators
LAMAs• Tiotropium• Glycopyrronium• Umeclidinium• Aclidinium
LABAs• Salmeterol• Fomoterol• Indacaterol• Vilanterol• Olodaterol
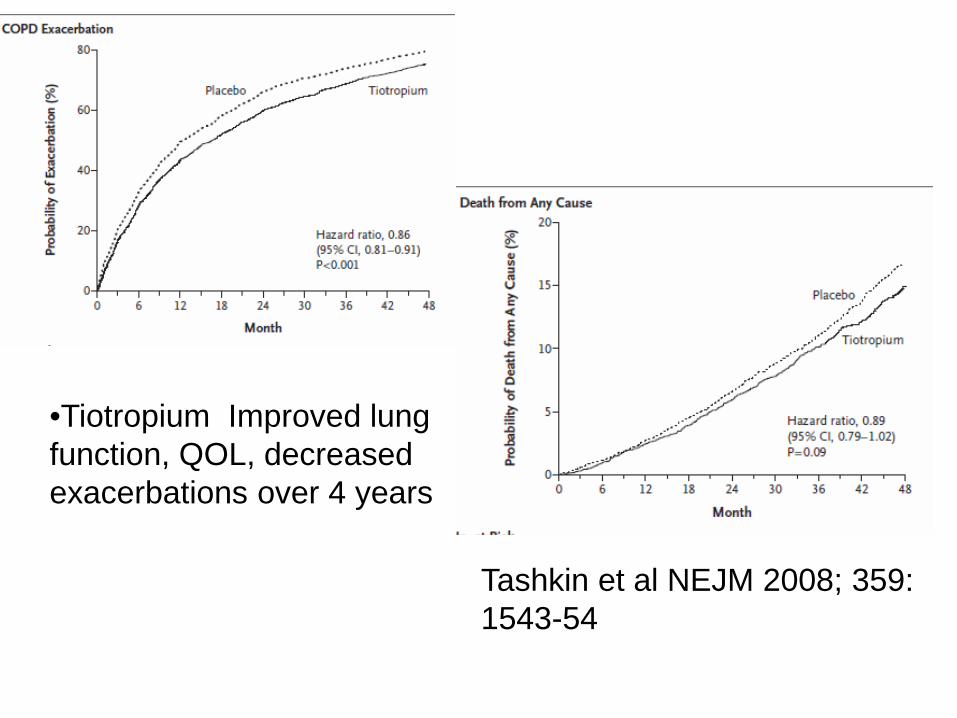
Tashkin et al NEJM 2008; 359: 1543-54
•Tiotropium Improved lung function, QOL, decreased exacerbations over 4 years
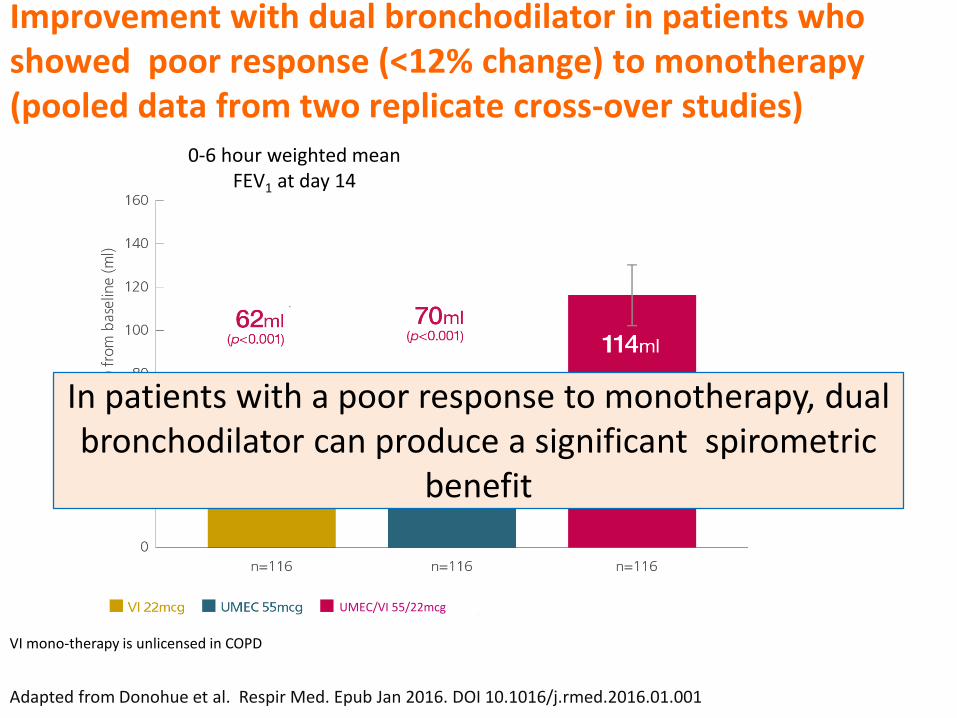
0-6 hour weighted mean FEV1 at day 14
Improvement with dual bronchodilator in patients who showed poor response (<12% change) to monotherapy (pooled data from two replicate cross-over studies)
Adapted from Donohue et al. Respir Med. Epub Jan 2016. DOI 10.1016/j.rmed.2016.01.001
VI mono-therapy is unlicensed in COPD
UMEC/VI 55/22mcg
In patients with a poor response to monotherapy, dual bronchodilator can produce a significant spirometric
benefit
VI 22mcg is an unlicensed investigational medicinal product* A Responder was defined as a patient with an increase in 0-6h WM FEV1 of ≥12% and ≥200ml on Day 1.Two replicate responder studies were performed as double-blind, three-way 14-day, cross-over trials (DB2116132 n=207; DB2116133 n=182;
clinicaltrials.gov numbers: NCT02014480; NCT01716520). WM=weighted mean
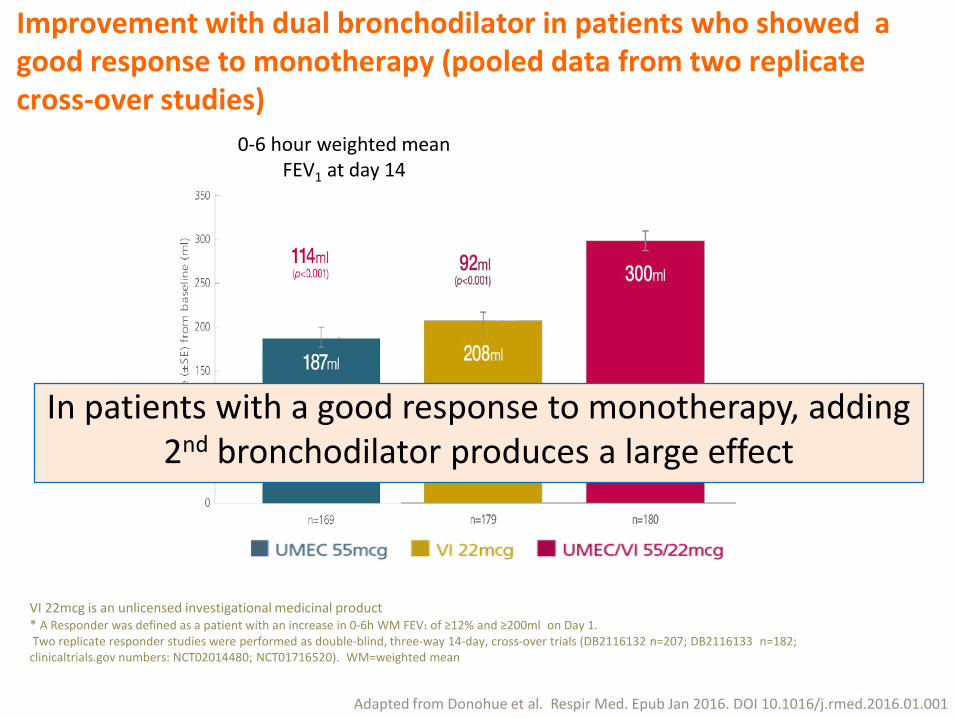
Improvement with dual bronchodilator in patients who showed a good response to monotherapy (pooled data from two replicate cross-over studies)
In patients with a good response to monotherapy, adding 2nd bronchodilator produces a large effect
Adapted from Donohue et al. Respir Med. Epub Jan 2016. DOI 10.1016/j.rmed.2016.01.001
0-6 hour weighted mean FEV1 at day 14
In other words….
• 2 bronchodilators better than 1:• Bronchodilation, symptoms, QOL
WHAT ABOUT ICS?
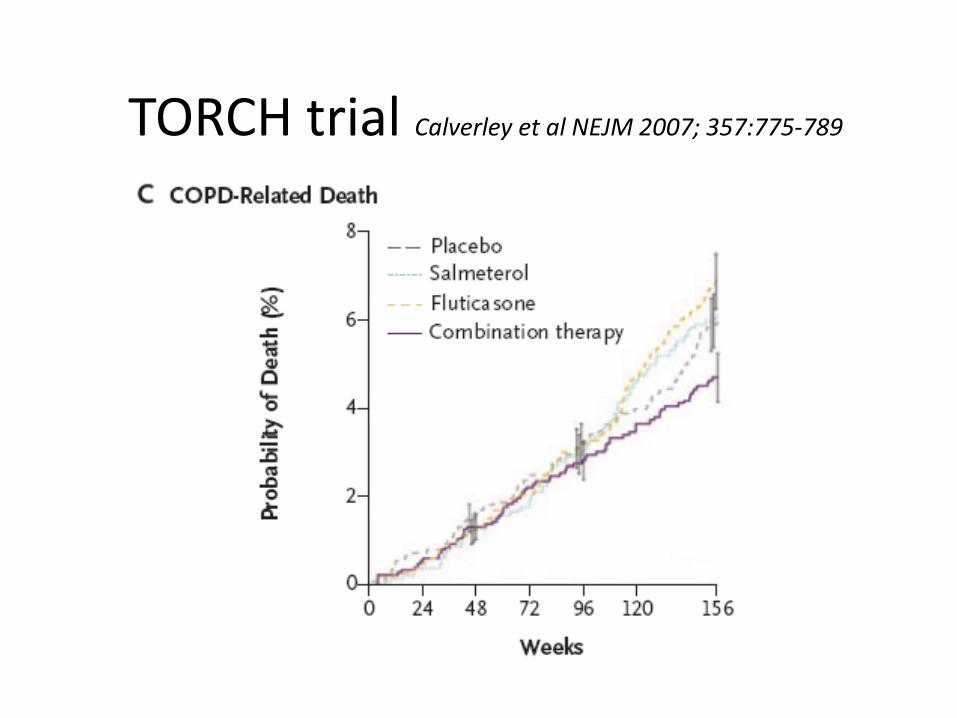
TORCH trial Calverley et al NEJM 2007; 357:775-789
ICS/LABA Combination inhalers
• Proven:– Maintain QOL– Decreased FEV1decline– Improve mortality
• HOWEVER:– increased pneumonia in some studies and in
meta-analysis– Later studies show alternatives….

Overall 11%decrease
in exacerbations
and longer time to first
exacerbation
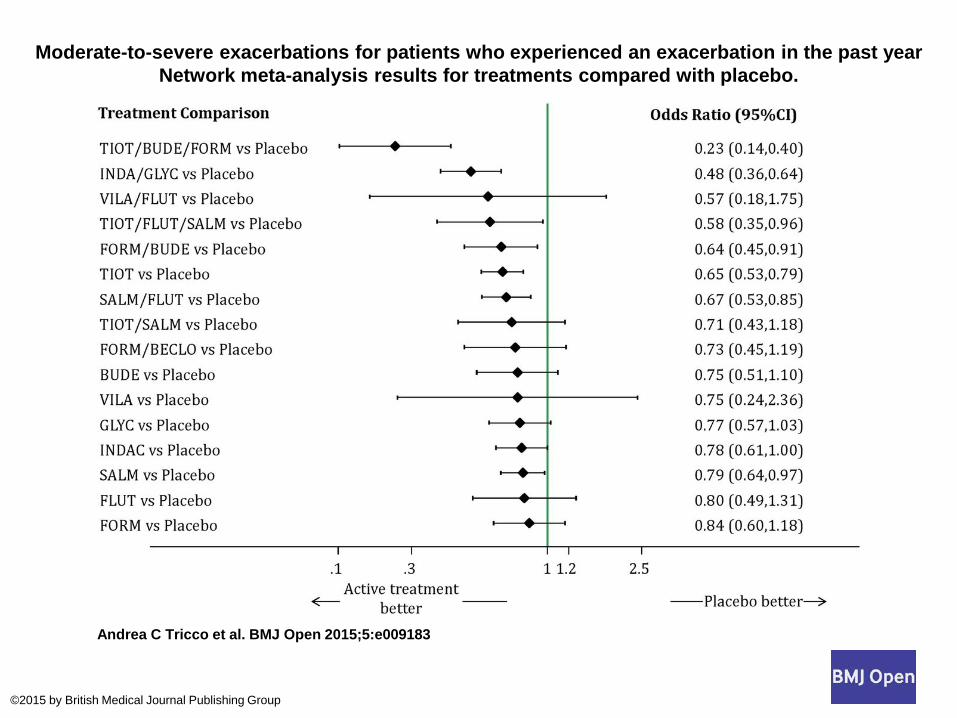
Moderate-to-severe exacerbations for patients who experienced an exacerbation in the past year Network meta-analysis results for treatments compared with placebo.
Andrea C Tricco et al. BMJ Open 2015;5:e009183
©2015 by British Medical Journal Publishing Group
STANDALONE ICS NOT RECOMMENDED FOR COPD

Oral Prednisolone?
• Short bursts of oral prednisolone are effective in treating acute exacerbations
• Long-term oral steroids are NOT reccommended:– Long-term treatment leads to steroid myopathy,
which contributes to muscle weakness, decreased functionality and repiratory failure in severe COPD(level A evidence, GOLD guidelines)
Theophylline in COPD
• Well-established place in COPD treatment– Improves inspiratory mucle function– Decreases exacerbations– Evidence that it helps to reverse steroid resistance
in COPD– No effect on mortality or FEV1– Low therapeutic index
ThreeEffective treatment is available for
treatment of stable COPD

MDIs: How often do patients use the inhalers right?
A. All the time, if properly taught
B. 75%C. 50%D. 25%E. <10%
• % patients with correct technique:– MDI 23-43%– DPI 53-59%– MDI with spacer 55-57%
• after teaching:– MDI 63%– DPI 65%– breath actuated MDI 75%
Broklebank, Ram, Wright et al Health Technol Assess 2001;5: 1-149
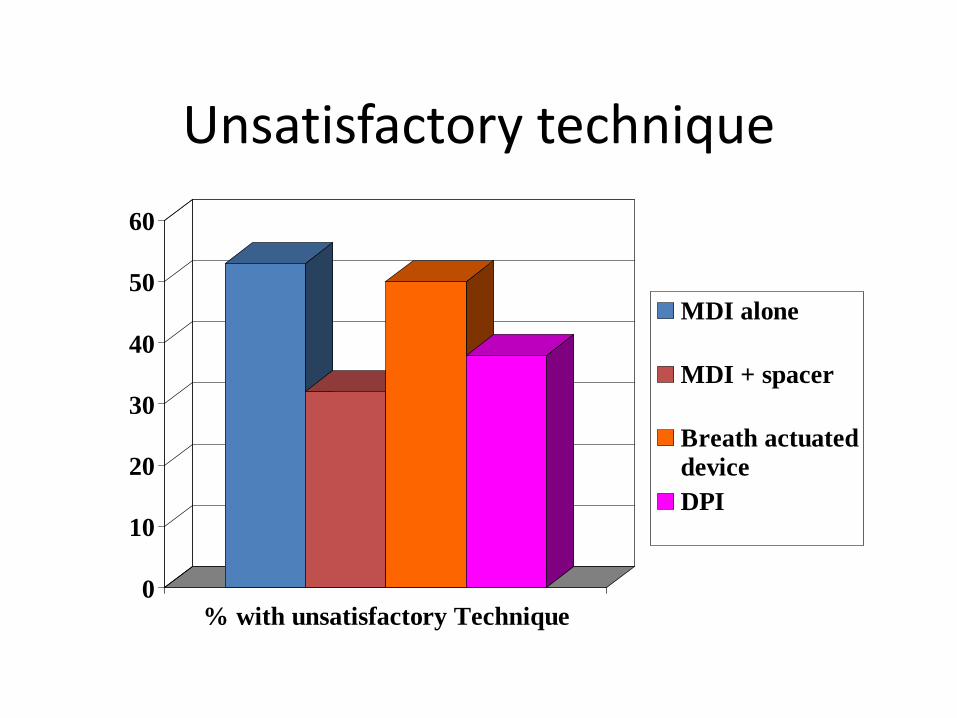
Unsatisfactory technique
0
10
20
30
40
50
60
% with unsatisfactory Technique
MDI alone
MDI + spacer
Breath actuateddeviceDPI
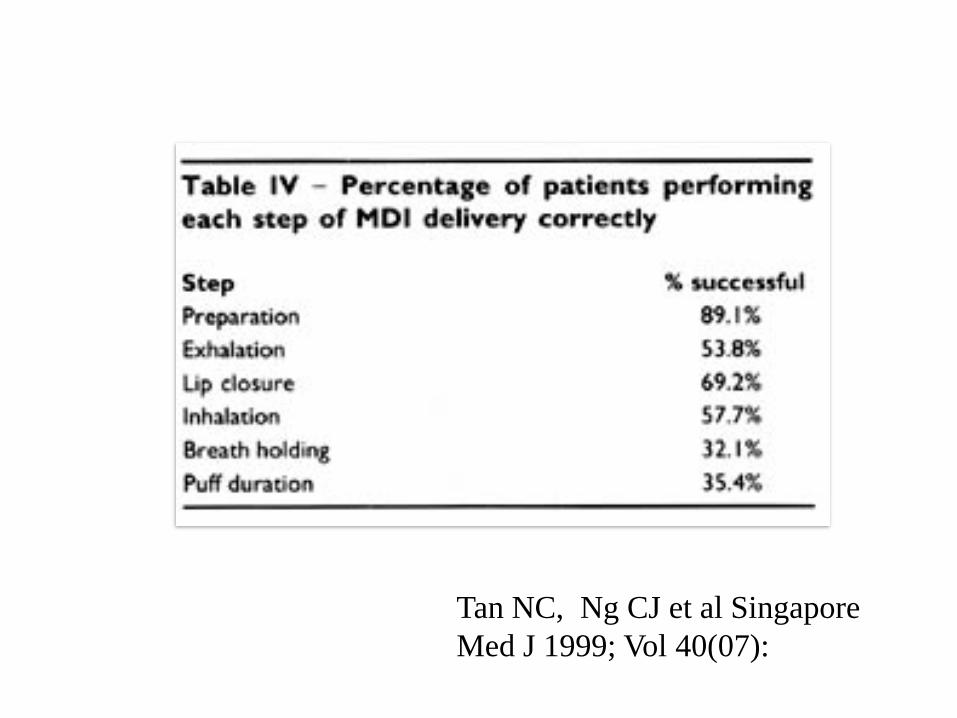
Tan NC, Ng CJ et al Singapore Med J 1999; Vol 40(07):
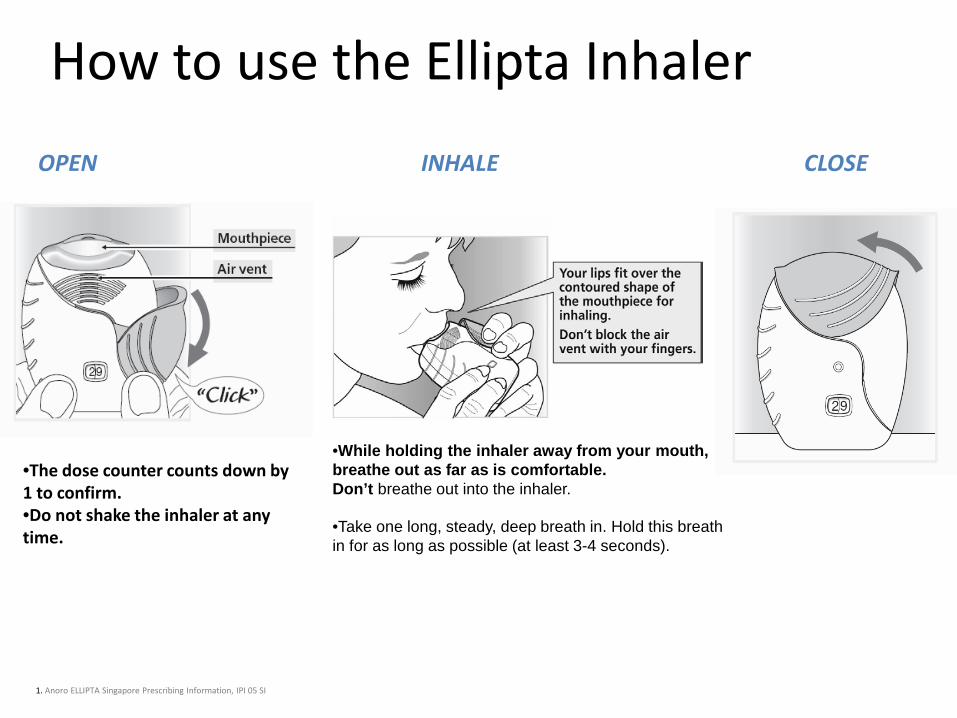
How to use the Ellipta InhalerOPEN INHALE CLOSE
•Take one long, steady, deep breath in. Hold this breath in for as long as possible (at least 3-4 seconds).
•While holding the inhaler away from your mouth, breathe out as far as is comfortable. Don’t breathe out into the inhaler.
1. Anoro ELLIPTA Singapore Prescribing Information, IPI 05 SI
•The dose counter counts down by 1 to confirm.•Do not shake the inhaler at any time.


ARE YOU CONFUSED YET?
GOLD guidelines 2017
GOLD 2017

THREETreatment of acute COPD

• Choice depends on– Availability– Cost– Physician preference– Skills and ability of patient
Which is better?
FourInhaler technique and patient acceptability
are important for successful treatment of COPD
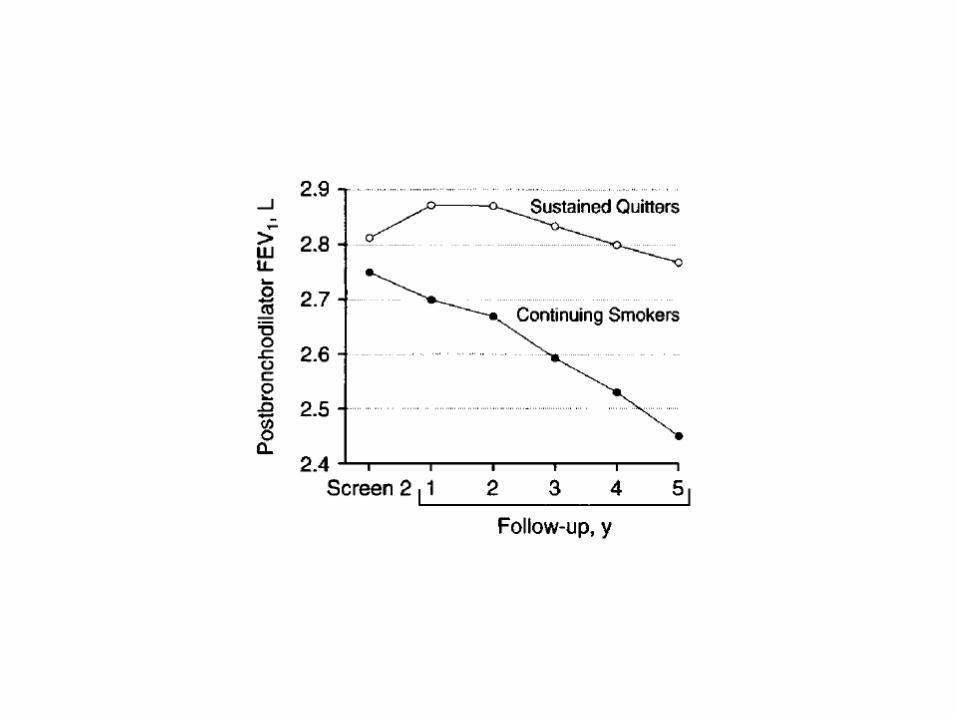
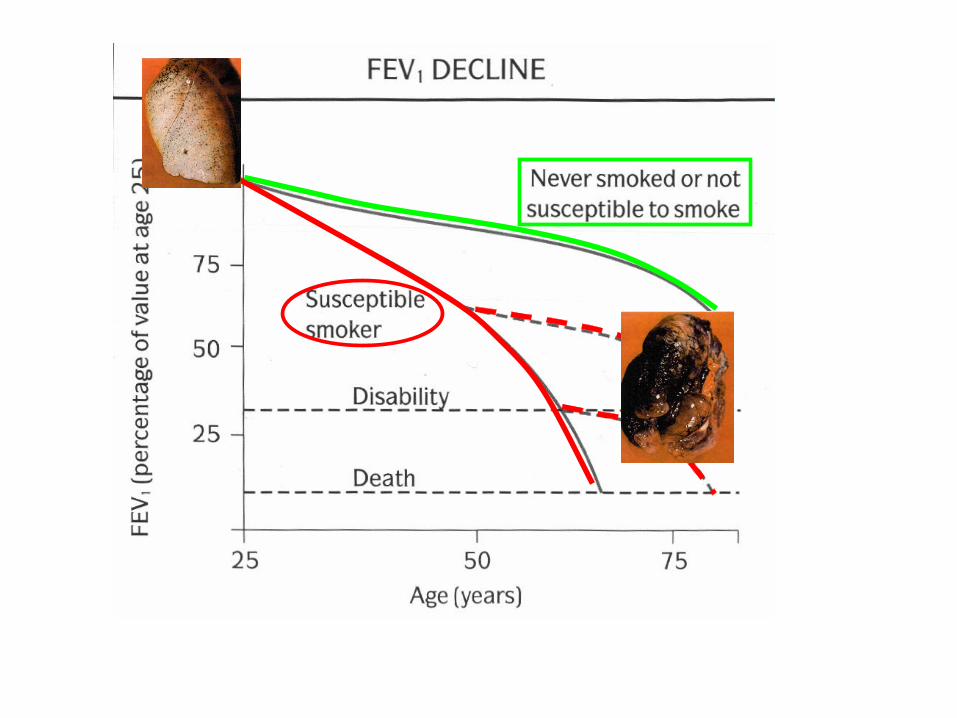
Anthonisen NR et al. The Lung Health Study. JAMA 1994;272(19):1497-505.
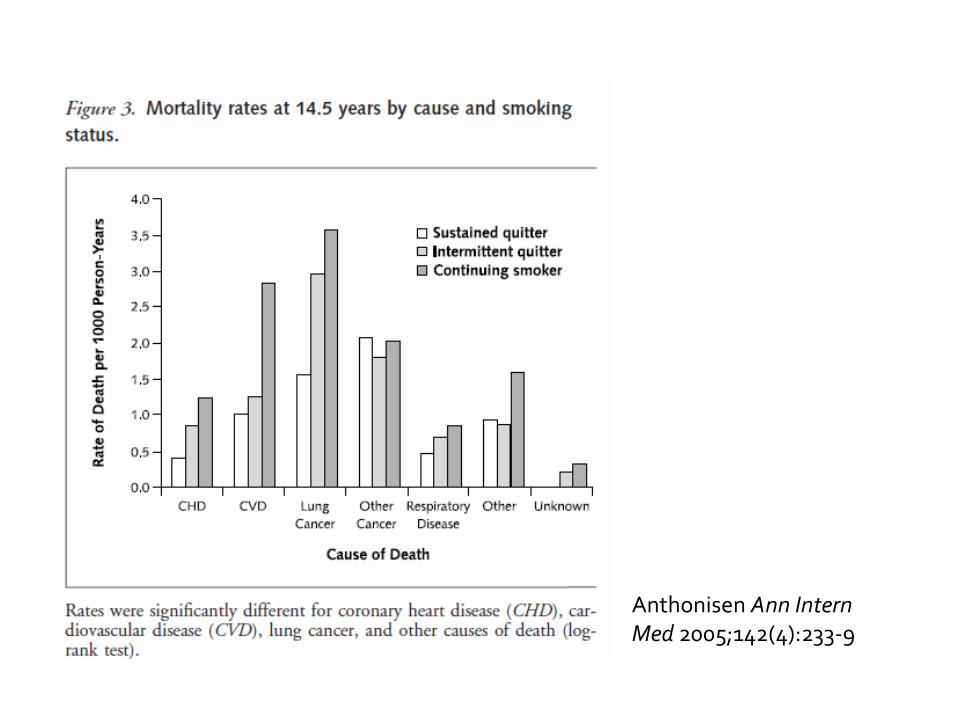
Anthonisen Ann InternMed 2005;142(4):233-9
"If you live each day as if it was your last, someday you'll most certainly be right."
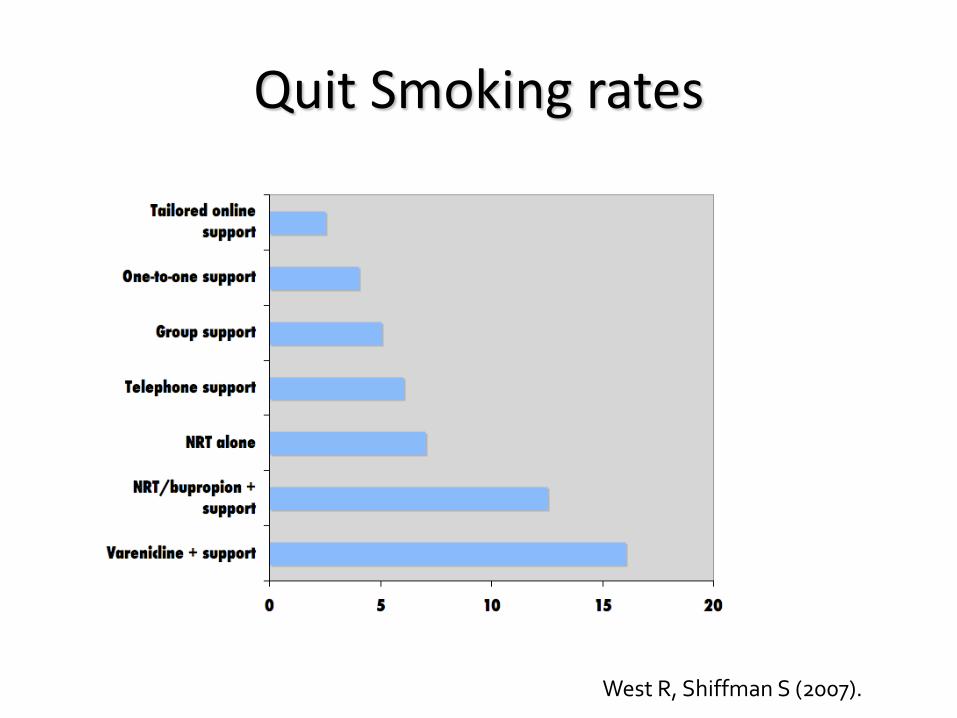
Quit Smoking rates
West R, Shiffman S (2007).

Did you know……..
• 3 min targeted intervention consisting of GP advice + reading material
• Doubled quit smoking rates from 3% to 7.4% at one year
Wilson DH et al Med J Aust1990 May 21; 152 (10): 518-21
FIVESmoking cessation is VERY important –
don’t give up!
SIXIt’s important to teach patients how to
manage with a chronic disease like COPD


Disease Management of COPD
Smoking cessationVaccinations – influenza,
pneumoccocalinhaler technique compliance to medications staying physically active
Physical Activity for COPD patients• Stretching exercises – improve flexibility, good warm-
up• Aerobic exercises – walking/ cycling• Strengthening exercises
– Tightening muscles to the point of fatigue– Upper body strengthening can improve respiratory
muscles– Breathing exercises
• Frequently patients’ SOB leads to deconditioning – a vicious cycle.
• Ten minute’s exercise 3 times a day adds up to 30 min
Breathing Exercises for COPD patients
• Pursed lip breathing:1. Relax your neck and shoulder muscles.2. Breathe in for two seconds through your nose, keeping
your mouth closed.3. Breathe out for four seconds through pursed lips. If this
is too long for you, simply breathe out twice as long as you breathe in.
• Use pursed-lip breathing while exercising. If you experience shortness of breath, first try slowing your rate of breathing and focus on breathing out through pursed lips.
Breathing exercises for COPD patients
• Diaphragmatic breathing:1. Lie on your back with knees bent. You can put a
pillow under your knees for support.2. Place one hand on your belly below your rib cage.
Place the other hand on your chest.3. Inhale deeply through your nose for a count of 3.
(Your belly and lower ribs should rise, but your chest should remain still.)
4. Tighten your stomach muscles and exhale for a count of 6 through slightly puckered lips.

MMWR. 2000;49:5-6.
INACTIVATED INFLUENZA VIRUS VACCINE
Content Updated yearly to protect against anticipated strains,
consists of type A (2) and type B (1)
Grown in embryonated chicken eggs and formalin inactivated
• Decreased incidence of ARI in COPD patients from 28/100 patient-years to 6.8 per 100 patient years in COPD patients in Thailand Wongsurakiat Chest 2004
EFFICACY OF THE INFLUENZA VACCINE

EFFECTIVENESS OF INFLUENZA VACCINE IN THE COMMMUNITY-DWELLIN ELDERLY NICHOL ET AL NEJM 2007. 357:1373-1381
27% reduction in risk of hospitalization for pneumonia or influenza
48% reduction in risk of death
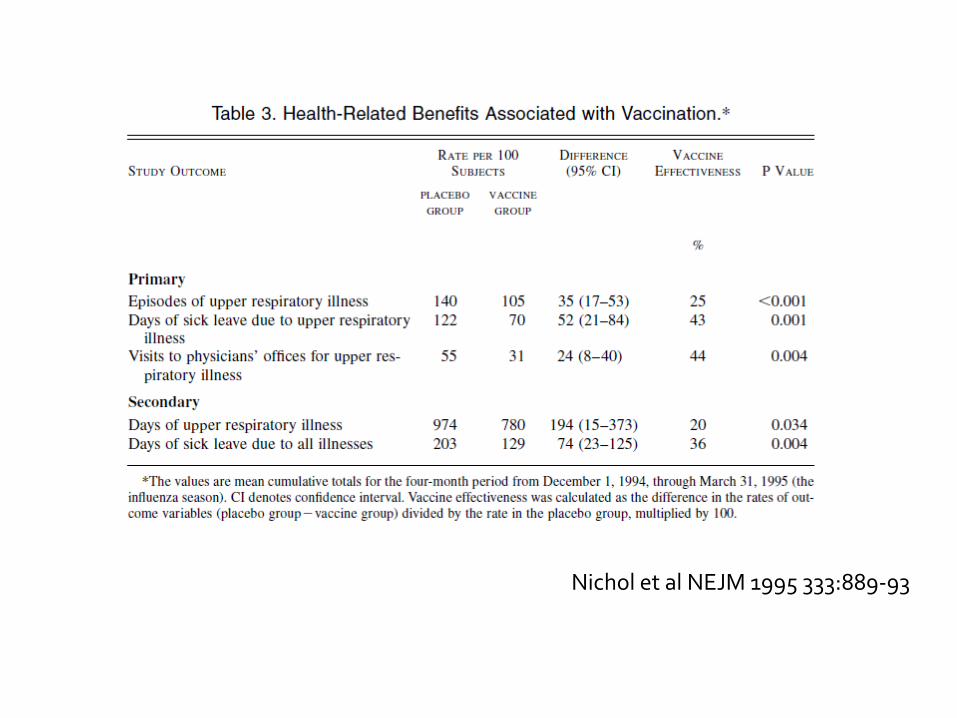
Nichol et al NEJM 1995 333:889-93
ONETWOTHREEFOUR FIVESIX
1. Correct diagnosis is critical to treatment of COPD – don’t miss cancer, TB etc.
2. Objective assessment and follow-up of COPD patients is necessary to guide treatment
3. Effective treatment is available for treatment of COPD
4. Treatment with inhalers will not be effective if pt doesn’t know how to use them!
5. Smoking cessation is VERY important – don’t give up!
6. It’s important to teach patients how to manage with a chronic disease like COPD
