the treatment of addiciton in older adults · cognitive behavioral therapy, and medications...
TRANSCRIPT
The Treatment of Addiciton in
Older Adults
Byron Bair,M.D.
Professor Geriatric Internal Medicine & Geriatric Psychiatry
University of Utah School of Medicine
Basic Demographics
• Aging population
– age 65 or older: 130%+ per year
• Life expectancy
– birth: 75 - 79 years
– at age 85: 6 - 8 more years
• Unique features of aging
– physiology changes
– disease presentation
Unique Features of Aging
• Pharmacodynamic changes of age
– increased receptor sensitivity
• opioids, benzodiazapines
– decreased receptor sensitivity
• beta blockers, beta agonists
• Pharmacokenetic changes of age
– absorption: little clinical effect
– distribution: lipid vs water soluble
– metabolism: phase I vs phase II
– excretion: Kidneys, bowels, tears, saliva, sweat
Diagnosis in DSM-5 — Substance use disorder, replaced substance abuse / dependence:
A problematic pattern of substance use leading to clinically significant impairment or distress, as manifested by at least two of the following
occurring within a 12-month period:
●The substance is often taken in larger amounts or over a longer period than was intended.
●There is a persistent desire or unsuccessful efforts to cut down or control use of the substance.
●A great deal of time is spent in activities necessary to obtain the substance, use the substance, or recover from its effects.
●Craving, or a strong desire or urge to use the substance.
●Recurrent use resulting in a failure to fulfill major role obligations at work, school, or home.
●Continued use despite having persistent or recurrent social or interpersonal problems caused by or exacerbated by its effects.
●Important social, occupational, or recreational activities are given up or reduced because of use.
●Recurrent use in situations in which it is physically hazardous.
●Continued use despite persistent or recurrent physical or psychological problems caused or exacerbated by the substance.
●Tolerance.
●Withdrawal.
Current severity can be specified in the diagnosis based on the number of symptoms present:
●Mild: Two to three symptoms
●Moderate: Four to five symptoms
●Severe: Six or more symptoms
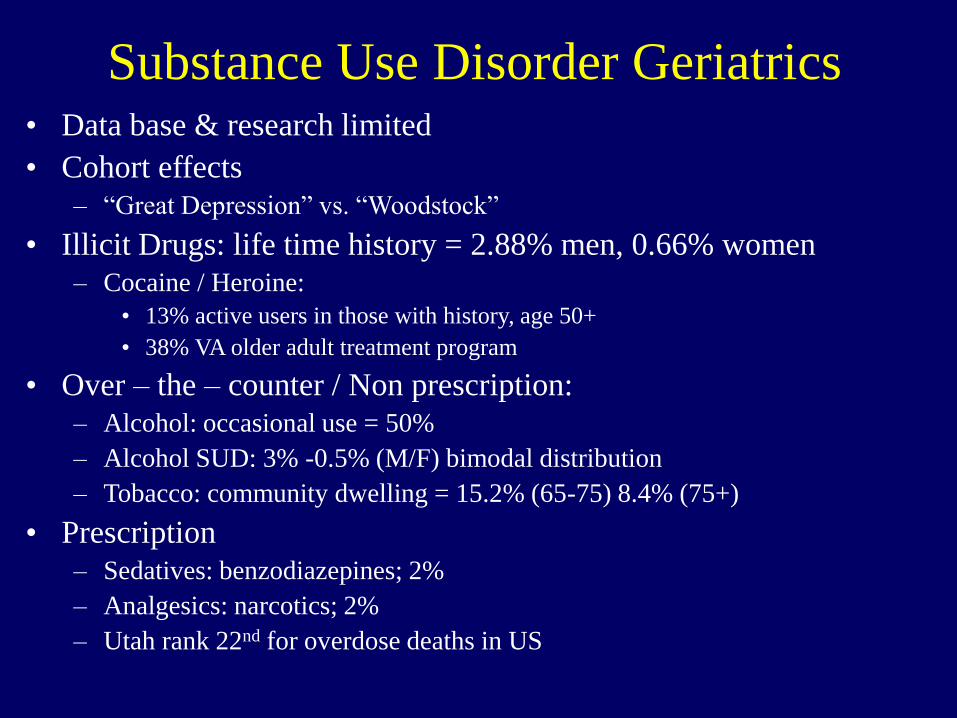
Substance Use Disorder Geriatrics• Data base & research limited
• Cohort effects
– “Great Depression” vs. “Woodstock”
• Illicit Drugs: life time history = 2.88% men, 0.66% women
– Cocaine / Heroine:
• 13% active users in those with history, age 50+
• 38% VA older adult treatment program
• Over – the – counter / Non prescription:
– Alcohol: occasional use = 50%
– Alcohol SUD: 3% -0.5% (M/F) bimodal distribution
– Tobacco: community dwelling = 15.2% (65-75) 8.4% (75+)
• Prescription
– Sedatives: benzodiazepines; 2%
– Analgesics: narcotics; 2%
– Utah rank 22nd for overdose deaths in US
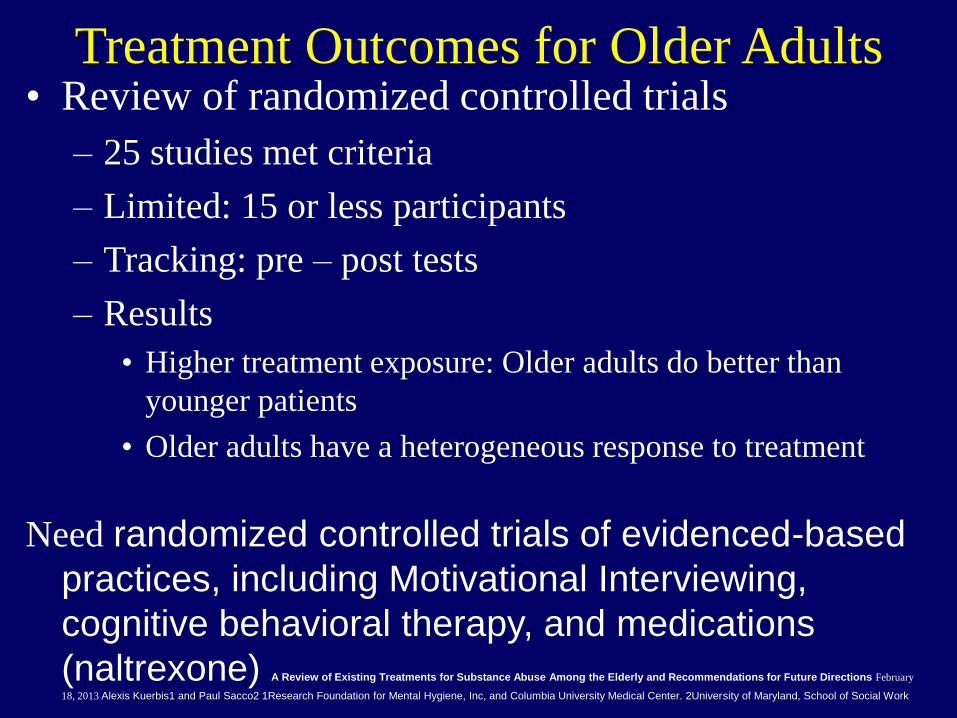
Treatment Outcomes for Older Adults• Review of randomized controlled trials
– 25 studies met criteria
– Limited: 15 or less participants
– Tracking: pre – post tests
– Results
• Higher treatment exposure: Older adults do better than
younger patients
• Older adults have a heterogeneous response to treatment
Need randomized controlled trials of evidenced-based
practices, including Motivational Interviewing,
cognitive behavioral therapy, and medications
(naltrexone) A Review of Existing Treatments for Substance Abuse Among the Elderly and Recommendations for Future Directions February
18, 2013 Alexis Kuerbis1 and Paul Sacco2 1Research Foundation for Mental Hygiene, Inc, and Columbia University Medical Center. 2University of Maryland, School of Social Work
Older Adults 5 Years after treatment
Compared to young and middle age adults
Older adults are:
• Less likely to be drug dependent at baseline
• Longer retention in treatment
• Less likely to be encouraged to take drugs / ETOH
• 12% higher abstinence last 30 days (52%)
– Older women had highest rates of abstinence
– ETOH only = no differences in age groups
Medical Conditions: Older Adults• Sensory Deficits
– Check or refer for evaluation of:• Vision
• hearing
• Malnutrition– Follow weights: un-intended weight loss > 5lb within 1 month
or 10 lb. in 3 months = high risk morbidity / mortality
• Cognition & Behavior
• Polypharmacy
• Depression
• Functional impairment
• Environmental status
• Prognosis & Life Expectancy
• Patient Goals
• Frailty
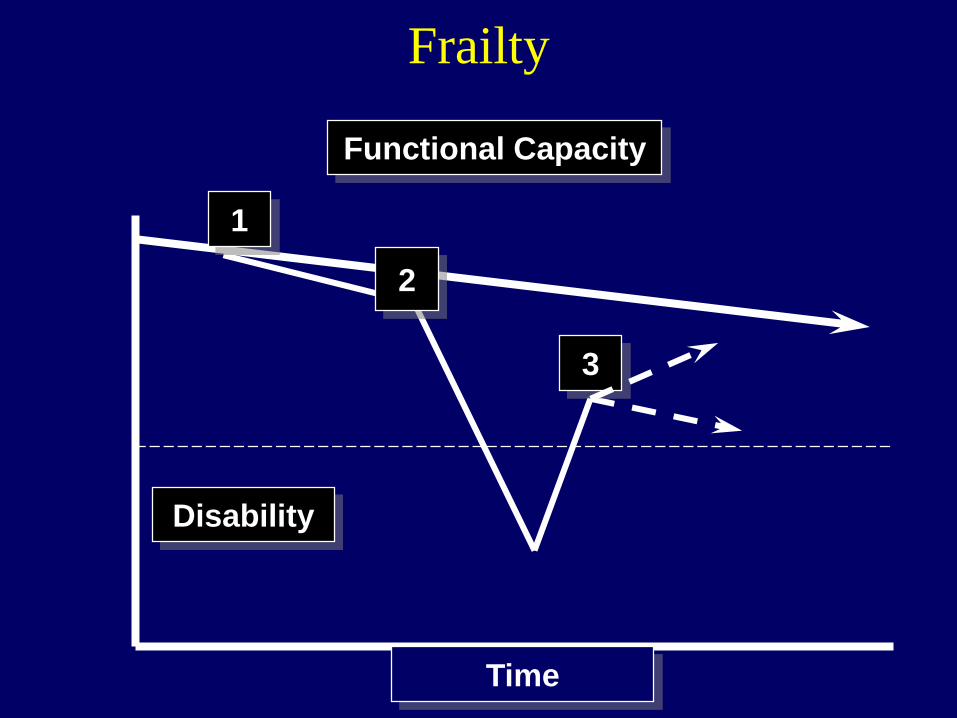
Frailty
1
2
3
Functional Capacity
Disability
Time
Treatment Models
• chronic/relapsing substance use disorders (SUD)
in the United States
– episodic treatment vs. continuing care
– Conceptualize as a chronic disease
– Serial patient assessments & monitoring
– modification of patients’ level of care over time based
on:
• phase of illness
• clinical status
• co-occurring conditions
• treatment needs/preferences
Substance Use Disorders Treatment
• provided via a continuum of care
• multiple tiers of clinical services that vary by:
– Setting
– types of treatment
– intensity of services
• Standard levels of care include:
– Inpatient
– Residential
– partial hospital
– intensive outpatient
– outpatient care
Treatment Considerations
The patient’s clinical status and risk of relapse are
monitored systematically and longitudinally
As the patient’s addiction waxes and wanes over
time (ie, experiences periods of abstinence, relapse,
or fluctuations in risk of relapse), the intensiveness
and types of treatment are adjusted along with the
level of care at which treatment is delivered
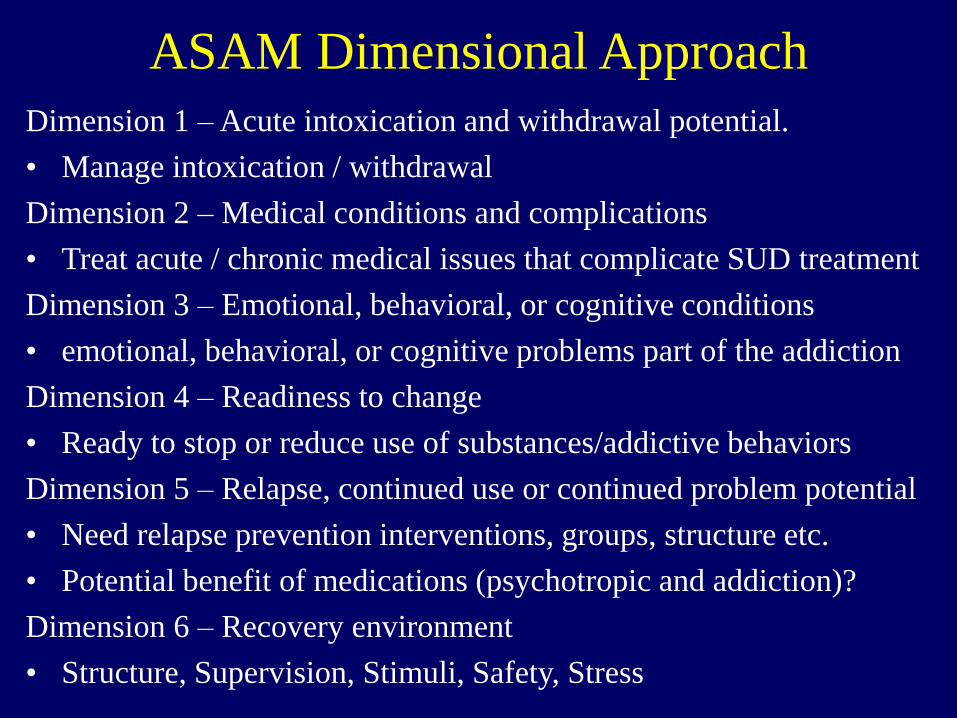
ASAM Dimensional Approach
Dimension 1 – Acute intoxication and withdrawal potential.
• Manage intoxication / withdrawal
Dimension 2 – Medical conditions and complications
• Treat acute / chronic medical issues that complicate SUD treatment
Dimension 3 – Emotional, behavioral, or cognitive conditions
• emotional, behavioral, or cognitive problems part of the addiction
Dimension 4 – Readiness to change
• Ready to stop or reduce use of substances/addictive behaviors
Dimension 5 – Relapse, continued use or continued problem potential
• Need relapse prevention interventions, groups, structure etc.
• Potential benefit of medications (psychotropic and addiction)?
Dimension 6 – Recovery environment
• Structure, Supervision, Stimuli, Safety, Stress
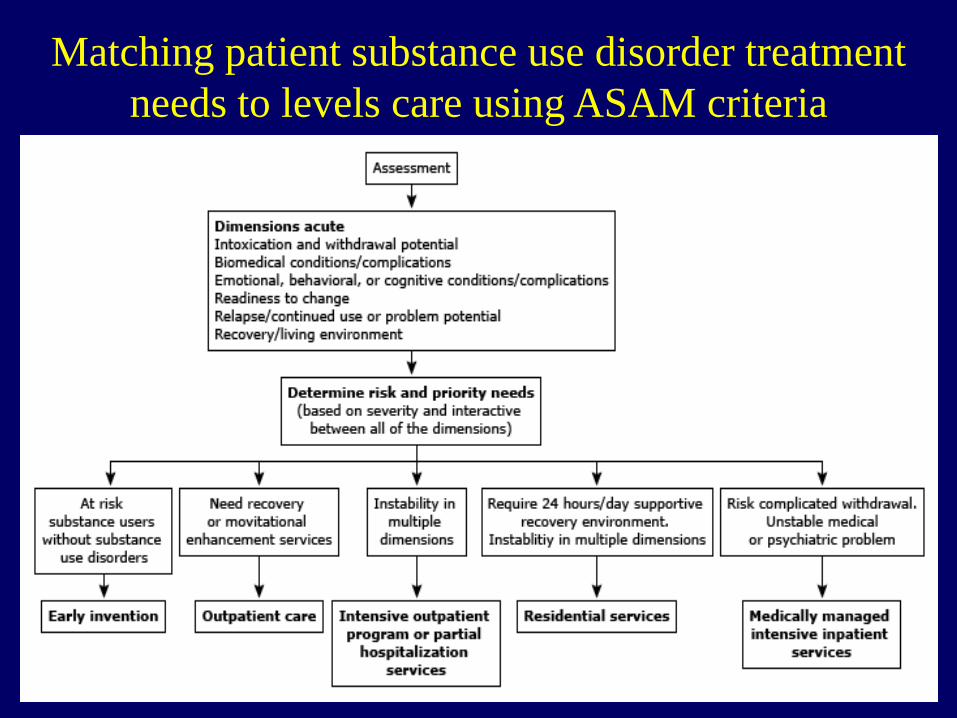
Matching patient substance use disorder treatment
needs to levels care using ASAM criteria
Evaluation
• Purpose:
– detect factors contributing to the current problem
– improve: function, comfort, dignity, quality of life
• It is common for multiple processes to be
occurring simultaneously in older adults
• Recognize role of Geriatric “frailty”
– aging = reduced reserve capacity
– increased propensity for “small” insults to result in
disability
Evaluation
• History: changes; acute vs chronic
– IADL’s: independent, assist, dependent
• use telephone, shopping, food preparation, housekeeping,
laundry, transportation, finances, medication
– ADL’s: independent, assist, dependent
• bathing, dressing toileting, transfers, continence, feeding
– Detect: common changes from baseline
• new or exacerbation of illness: self /spouse
• death in family
• psycho-social, environmental, economic
• vision, hearing, constipation, fluid intake
Evaluation• Physical Exam
– vital signs:
• weight, height, orthostatic BP, HR, RR, Temp.
– geriatric functional exam:
• get-up-and-go, ROM
– sensory:
• hearing, sight
– neurological
• gait, reflexes
– screening exams:
• PHQ9, GAD7, MOCA, PTSD etc.
Evaluation
• Laboratory
– Blood work:
• lytes, BUN/creatinine, Ca++, Mg++, albumen, (pre-
albumen), LFT’s, CBC & diff., TSH, B12, folate,
FTA, HIV
– Pulse oximetry
– EKG
– Imaging: Chest x-ray, CT without contrast?
– PVR
– Other:
• Other neuropsych. testing
Cognitive Function
Cognition comprises all mental
functions used to deal with the
internal & external world
Selected Cognitive Functions
• Memory
• Attention
• Orientation
• Language
• Writing
• Calculation
• Praxis
• Initiation
• Abstraction
• Planning
• Visuospatial
• Sequencing
• Personality
• Judgement
• Insight
• Behavior
7 D’s of Cognitive Dysfunction• Dementia
– Alzheimer's, Vascular, Mixed, Lewy Body, Frontotemporal
• Delirium
– Drugs +/- infections; acute vs subacute / chronic
• Damaged Brain
– Chemical (ETOH), traumatic, surgical
• Depression:
– Psychiatric disorders, mania, psychosis, PTSD, bereavement
• Developmental Delay
• Deficient Education
• Decision Making Capacity
Delirium: DSM V Criteria
• Disturbance of Consciousness
• Change in Cognition
• Acute Onset (hours - days)
• Result of General Medical Condition
Delirium: Etiology
Common Endpoint for Many Illnesses:
• Infections: UTI, pneumonia
• MI
• Pain
• Dehydration
• Medications / drugs
– intoxicated or withdrawal
Delirium: Significance
• 50-80% of Hospitalized Elderly
• Listed as Discharge Diagnosis: 5 -23%
• M.D. Recognition during course: < 1%
• Length of Stay: 2 x > controls
• Nursing Home D/C: 5 x > controls
• Inpatient Mortality: 8 x > controls
Evaluation: Delirium
• ANY acute change in mental status or behavior
may signal a delirium
• Delirium requires prompt medical evaluation
• differing evaluations is suspicious for delirium
• TREAT UNDERLYING MEDICAL ILLNESS
– haloperidol & lorazepam may help tranquilize to
allow evaluation and intervention but are not “tx”
Unrecognized Medical Issues
• 80% have at least 1 chronic medical condition
• An average of 8 different prescriptions, OTC, herbals
• New “behavioral” symptoms may reflect underlying comorbid disorders or new disorders layered on previous conditions
• 1 set of symptoms may reflect multiple interacting etiologies
Unrecognized Medical Issues
• Sleep disorders
– medications: diuretics, benzodiazepines, caffeine
– symptom of other illness: depression
– sleep apnea: 30 - 70%
• Pain, nutrition, hydration, HTN, CAD, Lipids, etc.
• Substance use disorders
– ETOH, benzodiazepines, opioids, other
• Polypharmacy: Prescription abuse?
– ADE’s: 40-50% vs 2-10% in younger populations
– pharmacodynamic, pharmacokenitic changes of age

Polypharmacy: Unintentional
Prescription Abuse?
• Average person over the age of 65
– 80% have 2 or more chronic medical conditions
– 4.5 prescriptions
– 3.5 over the counter (OTC) medications
– ? Herbals
– 12-17 new prescriptions per year
Polypharmacy: Unintentional Prescription
abuse In Older Adults?
• 596 “unique” admissions
– 15% readmission rate
– range of 2-6 admissions
• Reasons for readmission
– “new” clinical problem
– “clinical failure”
– “other” (scheduled test)
• Discharge medications: 12.8
• 72 hour follow-up discrepancies: 20.2
Polypharmacy and ADE’s
• 75% office visits include prescription
• 15% hospital admissions from ADE
• 50% of hospital stays are complicated by
ADE
• Longer hospitalization = more medications
Treatment Tools
• Trust + Verify
• Random blood / urine tests
• Continuity of care & monitoring
• Substance Abuse Database
Pharmacological Interventions
Restricted Prescription Drugs
• Utah Controlled Substance Database
– Access to providers + designee, pharmacy staff
• Exemptions:
– Prescriptions filled at federal facilities (military or
VA);
– Prescriptions filled at pharmacies licensed by other
states; or
– Controlled substances administered in an in-patient
setting.
Environmental Interventions• Finances and resources
• Assess individual needs before suggesting living
environment
– Supervision
• Independent vs dependent
– Structure
• Self vs external
– Stimuli
• Conducive vs chaotic
– Stress
• Self + others
– Safety
• Home, weapons, medications, driving
Pharmacological Interventions
ETOH Older Adults
• Few trials in older adults
• Inpatient supervised withdrawal
• Outpatient care
– 70% relapse after psychosocial treatments alone
– Psychosocial + Medication: older adults?
– Medications modulate effects of ETOH
• Naltrexone (ReVia, Depade); liver toxicity / opioids;
available as depot
• Acamprosate (Campral): liver safe; opioids
• Disulfiram (Antabuse): highly motivated and compliant
Pharmacological Interventions
Opioids Older Adults
• Structured & Experienced environment
• Agents: Geriatric studies limited
– Buprenorphine – naloxone combo
– Methadone: overdose & cardiac toxicity
– Clonidine: symptomatic relief
Pharmacological Interventions
Benzodiazepines Older Adults
• Structured environment
• Outpatient
– Gradual tapper under supervision
• Inpatient
– Unknown dose or unsafe environment
Utah Centers that Advertise Older
Adult Treatment
• 16 Centers
– https://www.psychologytoday.com/us/treatment
-rehab/elderly-persons-disorders/utah
• 70 Centers
– https://www.drug-rehab-
headquarters.com/utah/category/older-adult-
and-senior-drug-rehab/
• Advertisements vs. Reality
Additional Addition Information
• https://americanaddictioncenters.org/rehab-
guide/elderly/
• https://www.recovery.org/topics/elderly/
