the role of rigid contact lenses in the management of keratoconus
TRANSCRIPT

Journal of the British Contact Lens Association, Vot. 14, No. 4, pp 211-217, 1991 ©1991 British Contact Lens Association Printed in Great Britain
THE ROLE OF RIGID CONTACT LENSES IN THE MANAGEMENT OF KERATOCONUS
E. Geoffrey Woodward*
KEY WORDS: Keratoconus, contact lenses, keratoplasty.
T HE first full and adequate description of the condition of keratoconus that differentiated it
from other abnormalities of the cornea was given by Nottingham I in 1854. In his monograph, he gives accurate and painstaking descriptions of patients, differentiating clearly between keratoconus and other ectatic conditions. The most significant disclosure is that Nottingham was the first ophthalmologist to appreciate that the ectasia was a consequence of corneal thinning. Jaeger 2 in 1833 had noted corneal thinning in one patient at post-mortem, but as the patient had died of tuberculosis he attributed the thinning to this.
Prior to the advent of contact lenses the methods of management were either optical or surgical. Not- tingham describes the use of high-power negative cylindrical lenses with vertical axes, pin holes, and stenopaic slits. The surgical approaches were all based on scarring the apex of the cornea in an attempt to strengthen it, cauterisation using silver nitrate and mercury is also described, as is the passing of a seton through the cornea without perforating it. However, Nottingham's conclusion was that the most simple and least dangerous procedure was a straightforward puncturing of the cornea. Surprisingly at that date, he gives a long discussion on keratoplasty and reports that Hiley 3 in 1840 had attempted keratoplasty unsuc- cessfully, using heterografts.
There is also a hint of early inter-professional rival- ries in the nineteenth century, when Nottingham writes on the prevalence of the condition (page 7):
Conical cornea is a malady which does not, in most cases, diminish the clearness or brightness of the eye. Hence those who suffer from it, not finding themselves troubled with any visible disease of the organ which they are able to appreciate will, doubtless, very often seek relief in the aid of spectacles, and hence apply to the optician instead of the surgeon; and if so, the number of cases of conical cornea really existing in any community may not be adequately known by consulting surgical reports; to which we may add that the fame of individual opticians may tend to lessen considerably the opportunities which neighbouring surgeons may have of observing or study- ing this interesting affection of the organ of vision.. .
* PhD, FBCO, DCLP
It is in Nottingham that we find the first reference to the role of rigid contact lenses in the management of keratoconus, when on page 19 he reports:
Lenses of transparent animal jelly, contained in capsules of glass, to be placed in front of the eye and kept there as long as the patient will bear.
It is not stated what was the wearing time of these devices.
Contemporary Use of Rigid Lenses During the most recent decade, there have been five major studies published relating to the management of keratoconus (Table 1). Although the presentation of information varies between articles, it is possible in most cases to establish the role of rigid contact lenses (Tables 2-5).
Table 1. Published studies 1981-1990.
Number Year Authors Country o f Eyes Follow-up
1984 Cox 4 UK 176 5 years 1986 Ihalainen 5 Finland 424 4 years 1986 Kennedy et al. 6 USA 122 20 years 1988 Smiddy et al. 7 USA 230 5 years 1990 Lass et al.8 USA 746 4 years
Ihalainen 5 herself describes the percentage of patients grafted as atypical, giving the reason that many patients were specifically referred to her hospi- tal for transplantation. Methods of management are not specified by Kennedy et al., 6 but at the end of the study period 12 eyes had been grafted. Again, Smiddy et al. 7 report that many patients had been referred to the centre (Wilmer Eye Institute) specifi- cally for keratoplasty. Of the transplanted patients, 60% wore rigid corneal lenses after surgery. In Lass et al. s a new treatment modality is identified, epiker- atoplasty. Of the patients undergoing penetrating keratoplasty, 56% wore rigid corneal lenses after surgery. Of the epikeratoplasty group, 53% wore rigid corneal lenses after surgery.
211
E. GEOFFREY WOODWARD
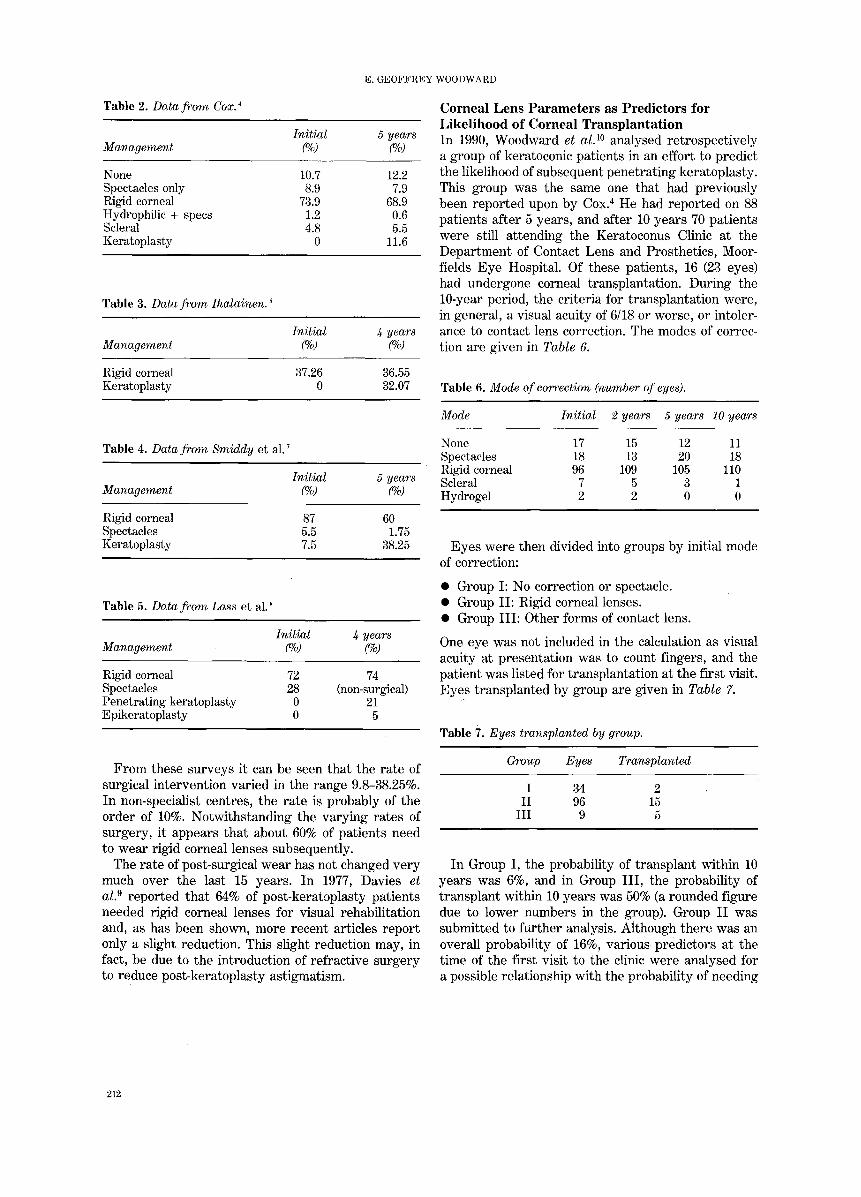
Table 2. Data from Cox. 4
Initial 5 years Management (%) (%)
None 10.7 12.2 Spectacles only 8.9 7.9 Rigid corneal 73.9 68.9 Hydrophilic + specs 1.2 0.6 Scleral 4.8 5.5 Keratoplasty 0 11.6
Table 3. Data from Ihalainen. 5
Initial 4 years Management (%) (%)
Rigid corneal 37.26 36.55 Keratoplasty 0 32.07
Cornea l L e n s P a r a m e t e r s as P r e d i c t o r s for L i k e l i h o o d o f Cornea l T r a n s p l a n t a t i o n In 1990, Woodward et al. 1° analysed retrospectively a group of keratoconic patients in an effort to predict the likelihood of subsequent penetrating keratoplasty. This group was the same one that had previously been reported upon by Cox. 4 He had reported on 88 patients after 5 years, and after 10 years 70 patients were still attending the Keratoconus Clinic at the Department of Contact Lens and Prosthetics, Moor- fields Eye Hospital. Of these patients, 16 (23 eyes) had undergone corneal transplantation. During the 10-year period, the criteria for transplantation were, in general, a visual acuity of 6/18 or worse, or intoler- ance to contact lens correction. The modes of correc- tion are given in Table 6.
Table 6. Mode of correction (number of eyes).
Mode Initial 2 years 5 years 10 years
Table 4. Data from Smiddy et al. 7
Initial 5 years Management (%) (%)
Rigid corneal 87 60 Spectacles 5.5 1.75 Keratoplasty 7.5 38.25
Table 5. Data from Lass et al. 8
Initial 4 years Management (%) (%)
Rigid corneal 72 74 Spectacles 28 (non-surgical) Penetrating keratoplasty 0 21 Epikeratoplasty 0 5
None 17 15 12 11 Spectacles 18 13 20 18 Rigid corneal 96 109 105 110 Scleral 7 5 3 1 Hydrogel 2 2 0 0
Eyes were then divided into groups by initial mode of correction:
• Group I: No correction or spectacle. • Group II: Rigid corneal lenses. • Group III: Other forms of contact lens.
One eye was not included in the calculation as visual acuity at presentation was to count fingers, and the patient was listed for transplantation at the first visit. Eyes transplanted by group are given in Table 7.
Table 7. Eyes transplanted by group.
Group Eyes Transplanted
I 34 2 II 96 15
III 9 5
From these surveys it can be seen that the rate of surgical intervention varied in the range 9.8-38.25%. In non-specialist centres, the rate is probably of the order of 10%. Notwithstanding the varying rates of surgery, it appears that about 60% of patients need to wear rigid corneal lenses subsequently.
The rate of post-surgical wear has not changed very much over the last 15 years. In 1977, Davies et al2 reported that 64% of post-keratoplasty patients needed rigid corneal lenses for visual rehabilitation and, as has been shown, more recent articles report only a slight reduction. This slight reduction may, in fact, be due to the introduction of refractive surgery to reduce post-keratoplasty astigmatism.
In Group I, the probability of transplant within 10 years was 6%, and in Group III, the probability of transplant within 10 years was 50% (a rounded figure due to lower numbers in the group). Group II was submitted to further analysis. Although there was an overall probability of 16%, various predictors at the time of the first visit to the clinic were analysed for a possible relationship with the probability of needing
212

THE ROLE OF RIGID CONTACT LENSES IN THE MANAGEMENT OF KERATOCONUS
a transplant within 10 years. The factors analysed were:
• Age at initial visit. • Initial visual acuity. • Sex. • Back optic radius, initial lens.
Using the standard computer package GLIM, the data were analysed using the method of logistic re- gression. The only significant predictor found was the back optic radius of the initially fitted lens. A keratoconic eye with a corneal radius within normal limits, at first visit, has the same risk of having a transplant as those in Group I, i.e., 6%. Whereas, if the initial back optic radius is 6mm or less, the risk is comparable to an eye in Group III, i.e., 50%. These findings are illustrated graphically in Figure 1, which shows the estimated probability of corneal transplant plotted against back optic radius at initial visit.
The back optic radius of the lens fitted was found to be a better indicator of the progression of the condition than keratometry. Keratometry becomes increasingly inaccurate as keratoconus progresses. The optical theory is based on catoptric images
,.Q ~3
• . Q
~!~ ~ 6:2 ~ 71~
BCOR
Figure 1. Estimated probability of transplant for given BCORs.
reflected from an axially symmetrical system, a situ- ation that does not pertain, even in moderate kerato- conus. The fitting philosophy used in the clinic was agreed by all the clinic staff, so it was considered that changes in back optic radius did represent pro- portionate changes in corneal contour. Furthermore, patients attended the clinic wearing their contact lenses, so this would also render unrepresentative keratometric values obtained immediately after lens removal.
Patients often have the impression, or may even have been told, that they wilt inevitably need surgery for this condition. Although this will vary with the treatment protocol of an individual unit, the results of this study give probabilities that are statistically significant when related to measurements taken at
the first visit. In terms of patient management, this enables the clinician to inform the patient of the likelihood of a corneal transplant being required within 10 years of diagnosis. It has been shown that many keratoconus patients are young and economi- cally active, and so this information should be of help to them in planning their life and career for the next 10 years.
Progession of Keratoconus in Rigid Lens Wearers For many years it was suggested that scleral lens wear had a direct therapeutic effect on the kerato- conic eye 11,12, in that progressive deterioration may be halted. But Ruben and Trodd 18 showed no recession in the rate of progression between lens wearing and non:lens wearing groups. Kemmetmuller 14 had no doubt that large corneal lenses had a direct thera- peutic effect on keratoconus, but Woodward 15 showed no difference in the rate of progression between lens wearing and non-lens wearing groups.
The claims for retardation, remission, or reversal being produced by contact lens wear have all been based upon keratometry. This is inevitably misleading because contact lens wear can produce a temporary flattening of the cornea. As keratoconus is essentially a disease of corneal thinning, it can only properly be monitored by serial topographical pachometry. When this is done, contact lenses are found to have no effect on the progression of the condition. In some cases, the disease progresses very little, but in most cases it tends to stabilise at a corneal thickness 60% of n o r m a l . 16
Some patients arrive for contact lens fitting with the impression that it will control the disease and that this is an indication for fitting as early as possible. It should be explained to them that the only purpose of fitting is visual rehabilitation. In patients where the condition in one eye has not progressed sufficiently to affect vision, the success rate for contact lens tolerance is low. There is little point in fitting these patients until or unless vision is reduced in the second eye. It is not particularly easy to tolerate a lens in one eye only, unless there is high motivation, such as cases where binocular vision is required for a particular occupation.
Most keratoconic patients fitted with contact lenses are of above average intelligence 5,17, and demand a clear explanation of the rationale of their treatment.
Rigid Corneal Lens Wear as a Risk Factor for Kerotoconus Over the years it has been suggested that contact lens wear may precipitate keratoconus. Gasset et al.lS compared the number of patients in their clinics who developed keratoconus after having worn hard and soft contact lenses, and went on to claim an associ- ation between hard contact lens wear and the risk of
213

E. G E O F F R E Y WOODWARD
keratoconus. However, the soft lens Wearers were analysed prospectively, while they were compared with a group of patients who had already worn rigid corneal lenses for some time. Although the refractive errors of the two groups were said to be similar in terms of spherical equivalents, it seems unlikely that the proportion of cases with irregular or high astigma- tism were equal, since these conditions would suggest the use of rigid lenses. In the early stages of kerato- conus, before diagnosis, many cases will show high regular astigmatism. A population of hard lens wear- ers is thus much more likely to contain undiagnosed keratoconic patients than a population of soft lens wearers.
Discussion of the possibility of rigid lens wear preci- pitating keratoconus has recently been reopened in an article by Macsai et al . 19 This was again a retro- spective study, in which 53 of a total of 199 patients had previously worn contact lenses when they developed keratoconus. The authors state:
The absence of keratoconus at the time of contact lens fitting was confirmed by slit lamp examination, kerato- metry readings, and manifest refraction.
However, corneal thickness had not been measured prior to fitting, so the possibility of undiagnosed keratoconus still exists, as thinning of the cornea precedes ectasia, refractive changes, or clinical signs. 15 Nevertheless, the authors consider that in some cases long-term rigid lens wear is a risk factor for keratoconus.
This possibility cannot be ruled out of hand. It has been shown that contact lens wear over a period of years does produce slight stromal thinning. It has also been shown that atopic patients with normal vision have an abnormal distribution of corneal thick- ness skewed to the thinner end of the range. 2°
In view of these two findings it is perhaps possible that prolonged contact lens wear in atopic patients could precipitate latent keratoconus.
Fitting Philosophies for Keratoconus The question of the most appropriate fitting philoso- phy for this condition has been debated for many years. In the early days of contact lenses, large relatively flat-fitting lenses were advocated and this approach, in a modified form, still has it proponents in Scandinavia and the German-speaking countries. As originally described, there was a specific intention to reshape the cornea using a large fiat lens, the curvature of which bore no relationship to the cornea contour, depending entirely on the plasticity of the cornea. 12 The lenses had total diameters between 9.50-11.50mm and had a single back curve, apart from a well-blended edge bevel 0.50-1.00mm wide. Initially, these lenses rode high with the lower edge often standing away from the cornea. The weight of
the lens then tended to push back the cone and 'sphericise' the cornea; after this, the next lens to try would be even flatter. The fit was also evaluated by repeated refraction, the flattening of the cone reducing both its refractive power and the axial length of the eye. The definitive lens was the one that required the least minus power.
Although not taken to these extremes, fiat-fitting lenses are still fitted currently, often being preferred by patients and offering some other advantages. An example of this approach is the Persecon E kerato- conus lens. 21 The advantages of this type of fitting are mainly optical, flatter fitting lenses giving significant visual improvement. In addition, the patient's vision may be enhanced for some time after the removal of the lens due to the cornea remaining relatively flattened. Reservations concerning the use of this approach relate to its possible effect on the natural history of the disease. The majority of patients with keratoconus exhibit corneal scarring, whether or not they wore contact lenses 2e but several writers have suggested that the wearing of a fiat-fitting corneal lens hastens the rate of scarring in sub-Bowman's stroma.23,e4
The design of a controlled clinical trial to test the hypothesis that flat-fitting rigid corneal lenses exacerbate corneal scarring in keratoconus would be logistically difficult and ethically dubious. The pro- gression of the condition is so unpredictable and the location of scarring so random that large groups of patients would be needed. Nevertheless, many practitioners who work in the field have the clinical impression that a causal relationship does exist.
Currently, the most widely accepted rigid corneal lens fitting philosophy is one in which the intention is to distribute the weight of the lens between the cone and the more normal peripheral cornea. The peripheral cornea does thin in keratoconus, but at only half the rate of the centre. 15 In cases where the cone is well established, this results in a lens showing an apical contact area of 2-3mm, an intermediate clearance zone, and a mid-peripheral contact annulus with conventional edge clearance at the periphery. In the earlier stages of the condition, owing to the vertical asymmetry of the ectasia, the intermediate zone forms a crescent rather than an annulus. With the exception of very early cases, it is necessary to use specifically designed lenses to achieve this type of fit. If conventionally designed lenses are used, the lens with the desired central fit usually has insuf- ficient edge clearance.
Full toroidal back surface corneal lenses are rarely used in fitting keratoconus. Although the cornea is highly astigmatic, the irregularity of the astigmatism is such that it has asymmetry in any one meridian, and centrally a toroidal back surface fits no better than a spherical one. However, toroidal back periph-
214

THE ROLE OF RIGID CONTACT L E N S E S IN THE MANAGEMENT OF K E R A T O C O N U S
eral surfaces can often be used to enhance lens centration.
A survey of keratoconic lens designs and fitting procedures is not within the scope of this article, but both are well described in the literature. With the advent of highly sophisticated techniques for analys- ing corneal topography, we are seeing an increasing number of software packages to 'design' lenses for keratoconus. The limitation of these designs is that they are still based on a mathematical model which is symmetric along one axis. The keratoconic cornea is not of this form and, even if a lens could be designed to follow corneal contours, it would be extremely difficult to manufacture, except by a moulding technique. Furthermore, if the lens were to closely match the shape of the cornea, its optical performance would be markedly inferior to that of current lens designs.
It would thus appear that there is not a great deal of scope in improving the design of rigid corneal lenses for keratoconus. This is not the case for materials used to manufacture such lenses. For a group of patients who will probably be wearing lenses for most of their lives, it is obviously desirable to use the most gas permeable materials available. However, with keratoconus there is usually an extremely effec- tive tear pump, so such qualities as a low wetting angle and dimensional stability become equally important. The steep, high minus lens usually necess- ary in keratoconus is very prone to distortion if manufactured from materials with a high percentage of siloxane. In advanced keratoconus, powers of gre- ater than 20D are often required, and a high refrac- tive index material would be most advantageous.
During the active phase of the condition, where re-fitting as frequently as every 3 months may be necessary, the patient usually complains of an unstable lens which easily falls out of the eye; fluo- rescein usually demonstrates heavy pressure on the cone with no peripheral support. If corneal hydrops occurs, corneal lens wear has to be discontinued until all stromal oedema has resolved. Re-fitting is not always necessary following an episode of hydrops, but where it is a flatter fit is often required, thus supporting Nottingham's ideas in 1854 of managing the condition by controlled corneal scarring.
Rigid Corneal Lens Fitting following Keratoplasty In the western world, keratoconus is the most com- mon indication for keratoplasty and it also has the best prognosis. 25 Even so, as described earlier in this article, around 60% of patients still require rigid contact lenses for optimum visual correction. Thus, despite the current availability of surgical techniques, such as wedge resections and relaxing incisions, these patients have unacceptable visual distortion that is
produced by significant degrees of corneal astigma- tism. In 1977, Davies et al2, reporting on 100 grafts for keratoconus, found a mean corneal astigmatism of 4.1D, with a range of 0-12D. Despite improvements in suturing techniques, Smiddy et al. 7, reporting in 1988 on 88 grafts for keratoconus, found a mean corneal astigmatism of 4.5D, with again a range of 0-12D. It would thus appear that there will be a role for rigid corneal post-keratoplasty for fitting some years to come.
Such fitting is not to be undertaken lightly. Basic measurements demonstrate that both its physiology and topography are abnormal and that a grafted eye lacks many of the~ in-built safety margins of the normal eye and must be regarded with particular caution. 26 Its intrinsic vulnerability, due to reduced corneal sensation and low endothelial cell density, must never be forgotten. It is, of course, essential that the lenses are manufactured from the most oxygen permeable material available that is compatible with dimensional stability.
On grafts of long standing, where corneal topo- graphy has begun to approximate to normal, it may be possible to fit lenses of conventional design. But on more recently grafted eyes, the aggregation of the various donor-host irregularities often produces a surface on which conventional-design lenses will not centre on or near the visual axis. In order to obtain centration, it is usually necessary to fit a larger lens.
These larger lenses vary between 10.0-12.0mm in diameter and are of a simple bi-curve or tri-curve construction. As the intention is to span both the graft and the irregular host-donor junction, it is essential that the back optic zone diameter be larger than the diameter of the graft itself. Currently, the majority of grafts performed have diameters between 7.0-8.0mm. Hence the back optic zone diameters usu- ally prescribed vary between 8.0-10.0mm. It is almost impossible to design a dedicated fitting set for post- keratoplasty fitting. Most practitioners build one up from unsuccessful lenses.
Keratometry represents graft curvature measure- ments taken near the centre of the graft, so is not of great value in the fitting. For these relatively large lenses, however, the flatter keratometry reading can be considered as an indication of a possible back radius for a first lens. Fenestrations are often employed, usually two or three 0.30mm diameter holes 2mm from the lens edge. Their function is not so much to enhance tear ingress, but to avoid the trapping of static bubbles. These frequently occur where the graft is slightly raised from the host cor- nea, producing a gutter. Over a period of years the host-donor interface tends to become less irregular and it may then be possible to fit lenses of a more conventional design.
215

E. GEOFFREY WOODWARD
Post-Keratoplasty Dimensional Changes in Corneal Lens Wearers It has long been reported that astigmatism following corneal transplantation decreases with time. It has also been suggested that this reduction may be faster in patients who wear contact lenses than those whose vision is corrected with spectacles. In 1990, Wood- ward et a l Y analysed retrospectively two groups of patients who had corneal transplantation for kerato- conus. One group (C) had been visually corrected with rigid corneal lenses and the other group (S) had worn spectacles or used no optical correction.
The method of regression in groups was used to analyse the meridional differences in corneal curva- ture with time for the two groups of patients. It was expected that patients with greater degrees of corneal astigmatism were more likely to have contact lens correction. However, the reverse was found (Table 8). All the measurements were taken after the removal of graft sutures. Sutures were removed between 3-30 months following transplantation (Group S, mean 15.59_+6.60, range 3-30; Group C, mean 12.38_+4.37, range 6-20).
Table 8. Characteristics of Groups S and C.
Group S a,b Group C a
Mean length of follow-up (months)
Mean number of follow-up visits
Mean corneal astigmatism b, first visit
Mean corneal astigmatism b, last visit
Reduction in corneal astigmatism b (%)
20+_12.19 24+_18.18 (5-41) (5-120)
3.74_+0.84 3.70_+0.17 (3-6) (3-5)
0.95+-0.60 0.91+_0.45 (0.10-2.30) (0.29-1.62)
0.78+_0.66 0.68+_0.32 (0.05-2.90) (0.20-1.43)
17.65 25.46
a The range is given in brackets. b Astigmatism is expressed as the meridional corneal difference
(ram).
As can be seen from Table 8, both groups demon- strated a reduction in corneal astigmatism over the period analysed and the percentage reduction was greater in the contact lens wearing group. Regression in groups was used to verify this finding. The method used yielded a measure of variance associated with the best gradient for each group and thus provided a means of testing the significance of the difference between the two gradients that describe the change in corneal astigmatism with time for each group. The difference in gradients was found to be significant at the 6% level.
As described earlier, the choice of contact lens correction did not appear to be based upon the amount of corneal astigmatism. Factors that influ-
enced the choice were mode of correction of the contralateral eye, a history of successful contact lens wear, the degree of anisometropia, and the quality of visual acuity obtainable. The demonstrated changes in corneal shape confirm the clinical finding that post-keratoplasty patients frequently need refitting following the removal of graft sutures.
It must also be noted that the measurements were usually taken immediately following contact lens removal, and there may have been a transient mould- ing effect. Were it possible to repeat the measure- ments some days after contact lens wear, different results may have been obtained. Unfortunately, it is very difficult to persuade patients with good contact lens acui ty to cease lens wear to obtain these measurements.
Post-Keratoconic Epikeratoplasty Use of Rigid Lenses As reported above, epikeratoplasty is now being increasingly used in the management of keratoconus. It is mainly used where contact lens tolerance is poor or the cornea is too steep for ft t ing. It is, of course, only suitable where there is minimal corneal scarring, otherwise penetrating keratoplasty is required to restore vision.
Lass et alY reported in 1990 that, after undergoing this treatment, 53% of patients wore rigid corneal lenses. Lembach et al. 2s reported in 1989 that 37.5% wore rigid lenses following epikeratoplasty. The reasons why patients who previously had not toler- ated contact lenses did so subsequently are not abso- lutely clear. Of course, in the majority of cases a less steep and less highly minus powered contact lens is required. But in addition to the more suitable corneal topography, Koenig et al. 29 have demonstrated alt- ered corneal sensation post-operatively in a patient who had undergone epikeratoplasty. Corneal hypo- esthesia may thus provide some improvement in con- tact lens tolerance.
It is likely that more will emerge in the next few years on this topic and also on the optical effects at the host-explant interface.
Address for Correspondence Professor E. Geoffrey Woodward, Department of Optometry and Visual Science, City University, Nor- thampton Square, London ECIV 0HB, United Kingdom.
R E F E R E N C E S
1 Nottingham, J. Practical Observations on the Conical Cornea, Churchill, London (1854).
2 Jaeger (1833), cited by Nottingham. 1 3 Hiley (1840), cited by Nottingham.' 4 Cox, S.N. Management of keratoconus. J. Br. Contact Lens
Assoc., 7(2), 86-92 (1984). 5 Ihalainen, A. Clinical and epidemiological features of kerato-
conus. Acta Ophthal., 64(Suppl. 178), 1-64 (1986).
216

THE ROLE OF RIGID CONTACT LENSES IN THE MANAGEMENT OF KERATOCONUS
6 Kennedy, R.H., Bourne, W.M., and Dyer, J.A. A 48 year clinical and epidemiological study of keratoconus. Am. J. Ophth., 101(3), 267-273 (1986).
7 Smiddy, W.E., Hamburg, T.R., Kracher, G.P., and Stark, W.J. Keratoconus: contact lens or keratoplasty. Ophthalmology, 95(4) 487-492 (1988).
s Lass, J.H., Lembach, R.G., Park, S.B., Horn, D.L., Fritz, M.E., Svilar, G.M., Nuamah, I.F., Reinhart, W.J., Stocker, E.G., Keates, R.H., Moran, C.T., Cobo, L.M., and Foulks, G.N. Clini- cal management of keratoconus. Ophthalmology, 97(4), 443-445 (1990).
9 Davies, P.D., Ruben, M., and Woodward, E.G. Keratoconus: an analysis of the factors which affect the optical results of keratoplasty. Trans. Enropean Contact Lens Soc. Ophthalmo- log., Ghent, 97-99 (1977).
lo Woodward, E.G., Moodaley, L.C., and O'Hagan, A. Predictors for likelihood of corneal transplantation in keratoconus. Eye, 4, 493-496 (1990).
11 Voss, E.H., and Liberatore, J.C. Fitting the apex of kerato- conus. Trans. Int. Soc. Contact Lens Specialists, 7th Congress, Philadelphia, Contacto, 6, 33-37 (1962).
12 Clifford-Hall, K.G. A comprehensive study of keratoconus. Br. J. Physiol. Optics, 20, 215-256 (1963).
13 Ruben, M. and Trodd, C. Scleral lenses in keratoconus. Contact Intraoc. Lens Med. J., 2(1), 18-20 (1976).
14 Kemmetmuller, H. Corneal lenses and keratoconus. Trans. Int. Soc. Contact Lens Specialists, 7th Congress, Philadelphia, Con- tacto, 6, 17-21 (1962).
15 Woodward, E.G. The cornea in health and disease: Progression of keratoconus in eyes fitted with contact lenses. In Trans- actions of the Sixteenth Congress of the European Society of Ophthalmologists, P. Trevor-Roper (Ed), BMJ Press, London, 40, 531-536 (1980).
16 Woodward, E.G. Keratoconus: The Disease and its Progression. Doctoral Thesis, The City University, London (1980).
17 Woodward, E.G. Keratoconus: maternal age and social class. Br. J. Ophthal., 65(2), 104-107 (1981).
is Gasset, A.R., Haude, W.L., and Garcia-Bengochia, M. Hard contact lens wear an environmental risk in keratoconus. Am. J. Ophthal., 85(3), 39-41 (1978).
19 Macsai, M.S., Varley, G.A., and Krachmer, J.H. Development of keratoconus after contact lens wear: patient characteristics. Arch. Ophthalmol.,18, 534-538 (1990).
20 Kerr-Muir, M., Woodward, E.G., and Leonard, T. Corneal thick- ness, astigmatism and atopy. Br. J. Ophthal., 71,207-211 (1987).
21 Achatz, M., Eschmann, R., Rockert, H., Wilkens, B., and Grant, R. Keratoconus: a new approach using bi-elliptical contact len- ses. Contactologia, 7, 17-21 (1985).
22 Bron, A.J., Tripathi, R.G., Harding, J.J., and Crabbe, M.J. Stromal loss in keratoconus. Trans. Ophthal. Soc. UK, 98, 393-396 (1978).
2~ Ruben, M. Contact Lens Practice, pp 171 and 283-284, Balliere- Tindall, London (1975).
24 Korb, D.R., Finnemore, D.M., and Herman, J.P. Apical changes and scarring in keratoconus, as related to contact lens fitting techniques. J. Am. Optom. Ass., 53, 199-205 (1982).
25 Polack, F.M. Corneal Transplantation, Grune & Strattin, New York (1977).
2G Woodward, E.G. Contact Lenses, 3rd edn, A. Phillips and J. Stone (Eds), pp 764-771, But te~or ths , London (1989).
27 Woodward, E.G., Moodaley, L.C.M., Lyons, C., Davison, C. Buckley, R.J., and Barbur, V.A. Post-keratoplasty dimensional and refractive change in contact lens and spectacle corrected cases. Eye, 4, 689-692 (1990).
2s Lembach, R.G., Lass, J.H., Stocker, E.G., and Keates, R.R. The use of contact lenses after keratoconic epikeratoplasty. Arch. Ophthalmol., 107, 364-368 (1989).
29 Koenig, B.S., Berkowitz, A.R., and Beuerman, W.R. Corneal sensitivity after epikeratophakia. Ophthalmology, 90, 1213-1218 (1983).
217