the problem of non-compliance in long-term antihypertensive therapy
TRANSCRIPT
Symposium on hypertension 86
Dr K.P. O'Brien (Auckland): As I understand it, there is no doubt that there is this overshoot phenomenon from c1onidine. We have also been talking about 'overshoot' from P-blockers this afternoon and I wonder if that is a misnomer. There is evidence to suggest that angina and arrhythmias and myocardial infarction occur more fre-quently after the sudden withdrawal of p-blockers, but is there evidence to show that the blood pressure goes up above the usual levels?
this can be controlled with phentolamine so that the probability is that it is an overshoot due to release of catecholarnines. As far as /3-blockers are concerned, there have been a number of reports which have indicated that a few patients get rises of blood pressure when /3-blockers are given. I personally don't know of any convincing reports of thiS occurring on their withdrawal.
Now, I think it is all very well for Prof. Simpson to say that he doesn't think we should stop drugs suddenly but one of the important points is that patients do default or stop taking drugs. This gives us a lead in now to the next paper by Dr Abernethy, Director of the National Blood Pressure Study in Canberra, who is going to deal with the problem of defaulters.
Prof. Doyle: Perhaps I might just clarify the situation. As far as I know there is no reasonable doubt that in a few patients who have been taking clonidine, when the drug is stopped or withdrawn even temporarily, the blood pressure may rise to a very high level. As Dr Stokes said,
Summmy
Drugs 11 (Suppl. 11: 86-90 (1976) © ADIS Press 1976
The Problem of Non-Compliance in Long-Term Antihypertensive Therapy
J.D. Abernethy
Australian National Blood Pressure Study, National Heart Foundation, Canberra
Of 1,593 subjects admitted to the Australian National Blood Pressure Study 1 to 2 years ago, a substantial number (391 or 24.5%) ceased attending, in 85% of cases voluntarily.
Withdrawal rates were very high in the first 4 months, settling to 5% per annum by the second year. Extrapolation to clinical practice is hazardous but contributory factors elicited by questionnaire suggest certain 11IIlnagement strategies: maximisation of efforts to enlist subject co-operation at the onset of treatment; 11IIlnagement of treatment by family doctor or health centre with appointments flexible in time and infrequent in number; minimisation of doctors' ambivalence about treatment effectiveness and the withholding of infor11llltion from the subject.
It is inevitable that a proportion of subjects will reject long-term drug treatment. This adds further weight to the need for research on alternatives such as low salt diets.
Non-compliance and antihypertensive therapy
1. Introduction
Defaulters from long-term treatment have a profoundly negative effect on the conduct of clinical trials (Clark, 1975), and in cost-benefit analyses of community-wide antihypertensive programmes (Sackett, 1974). My purpose is to report on experience in the Australian National Blood Pressure Study (NBPS), and attempt some resolution of the problem in ordinary clinical practice.
In brief, the NBPS is a Single-blind controlled trial designed to test the hypothesis that treatment is of benefit in mild hypertension (Abernethy, 1974). The active treatment group receive a diu-retic (chlorothiazide) in the first instance, with the addition of a J3-blocker and/or methyldopa if necessary, while the control group receive matching placebos. Steps are taken to ensure that both groups attend follow-up clinics with approxi-mately equal frequencies.
By the end of 1975, up to 104,000 subjects will have been screened and up to 4,000 subjects randomised into a clinical trial destined to last for. at least 5 years. At first sight then the NBPS ought to be a useful experiment for observing the problem. However, it should be stressed that ethical and statistical design factors built into this clinical trial preclude any rigorous extrapolation to clinical practice for a number of reasons.
Firstly, the population sample is not a random one, having been selected from particular suburban locations for the presence of untreated, uncompli-cated mild hypertension in a specific age range (30 to 69), and including whatever factors are associ-ated with self-selection.
Secondly, prior to accepting treatment, subjects are advised that treatment is offered with three pre-conditions: that no undertaking can be given that lowering of blood pressure in mild hyper-tension reduces the risk of complications; that in any case tablets received mayor may not be active in lowering blood pressure; that specific inform-ation on the blood pressure response to treatment
87
will not be divulged to the subject. These represent quite an unusual departure from accepted clinical practice and as such may aggravate the tendency to withdraw.
2. Results
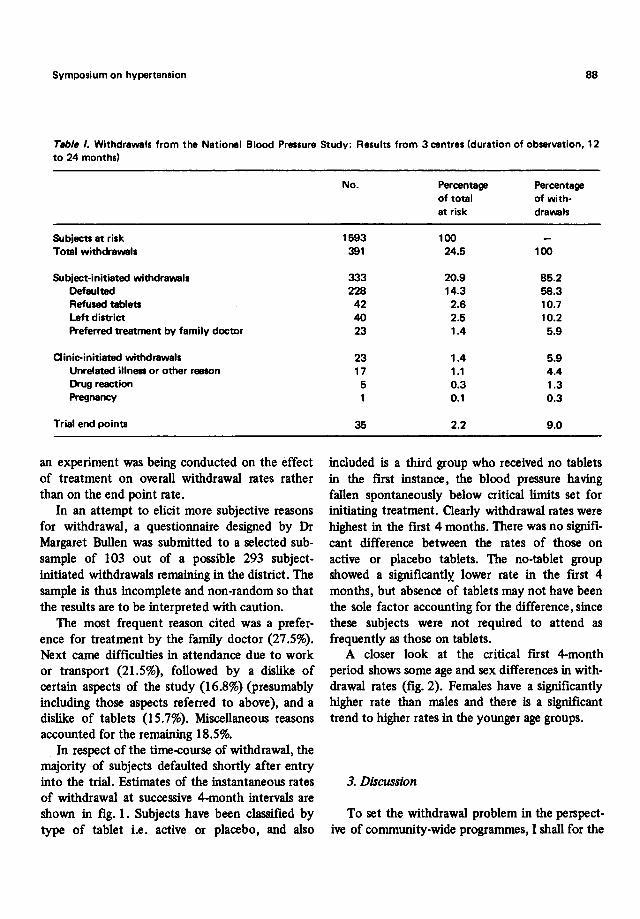
The above caveats accepted, a breakdown of 391 withdrawals in 1,593 subjects is presented in table I. Withdrawals have been broadly classified into subject-initiated withdrawals, clinic-initiated withdrawals and trial end points (stroke, hyper-tensive heart and renal disease, ischaemic heart disease, death). Subject-initiated withdrawals account for 85% out-numbering trial end points by about 10 to 1. If end points are regarded as 'signals' and other withdrawals as 'noise' then the signal-to-noise ratio is very low. In fact a man from Mars observing all this activity might conclude that
~ • active
10 • placebo
~ • no tablets
0 ... 0 ~ 0 ... • ""0 • ~ • • -·i • •
0
time Vrs
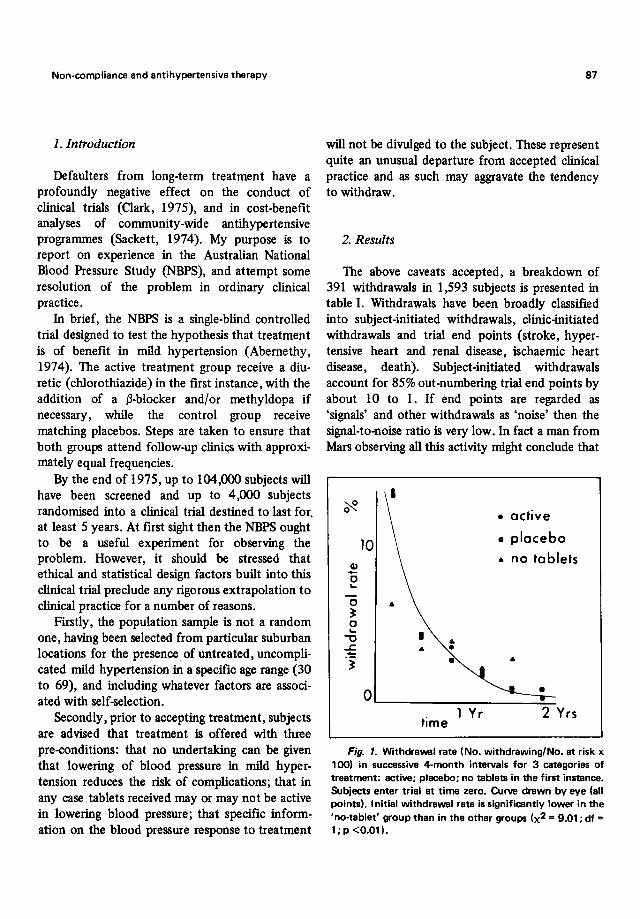
Fig. 1. Withdrawal rate (No. withdrawing/No. at risk x 100) in successive 4-month intervals for 3 categories of treatment: active; placebo; no tablets in the first instance. Subjects enter trial at time zero. Curve drawn by eye (all points). Initial withdrawal rate is significantly lower in the 'no-tablet' group than in the other groups (x2 = 9.01; df = 1; p <0.01).
Symposium on hypertension 88
Table I. Withdrewals from the Netionel Blood Pressure Study: Results from 3 centres (duration of observation, 12 to 24 months)
Subjects at risk Total withdrawals
Subject-initiated withdrawals Defaulted Refused tablets Left district Preferred treatment by family doctor
Clinic-initiated withdrawals Unrelated illness or other reason Drug reaction Pregnancy
Trial end points
an experiment was being conducted on the effect of treatment on overall withdrawal rates rather than on the end point rate.
In an attempt to elicit more subjective reasons for withdrawal, a questionnaire designed by Dr Margaret Bullen was submitted to a selected sub-sample of 103 out of a possible 293 subject-initiated withdrawals remaining in the district. The sample is thus incomplete and non-random so that the results are to be interpreted with caution.
The most frequent reason cited was a prefer-ence for treatment by the family doctor (27.5%). Next came difficulties in attendance due to work or transport (21.5%), followed by a dislike of certain aspects of the study (16.8%) (presumably including those aspects referred to above), and a dislike of tablets (15.7%). Miscellaneous reasons accounted for the remaining 18.5%.
In respect of the time-course of withdrawal, the majority of subjects defaulted shortly after entry into the trial. Estimates of the instantaneous rates of withdrawal at successive 4-month intervals are shown in fig. 1. Subjects have been classified by type of tablet i.e. active or placebo, and also
No.
1593 391
333 228
42 40 23
23 17
5 1
35
Percentage of total at risk
100 24.5
20.9 14.3
2.6 2.5 1.4
1.4 1.1 0.3 0.1
2.2
Percentage of with-drawals
100
85.2 58.3 10.7 10.2
5.9
5.9 4.4 1.3 0.3
9.0
included is a third group who received no tablets in the first instance, the blood pressure having fallen spontaneously below critical limits set for initiating treatment. Qearly withdrawal rates were highest in the first 4 months. There was no signifi-cant difference between the rates of those on active or placebo tablets. The no-tablet group showed a significantly. lower rate in the first 4 months, but absence of tablets may not have been the sole factor accounting for the difference, since these subjects were not required to attend as frequently as those on tablets.
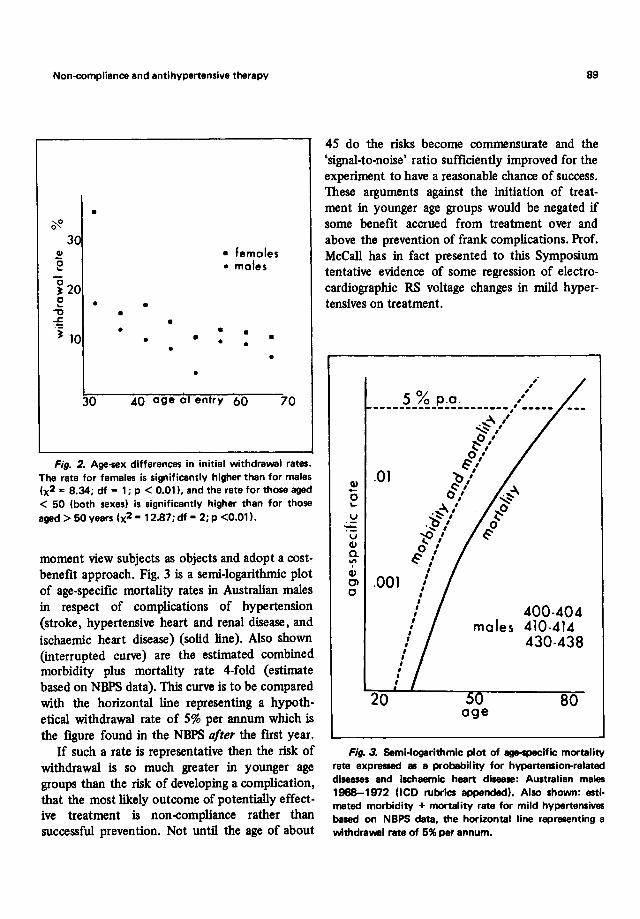
A closer look at the critical first 4-month period shows some age and sex differences in with-drawal rates (fig. 2). Females have a significantly higher rate than males and there is a Significant trend to higher rates in the younger age groups.
3. Discussion
To set the withdrawal problem in the perspect-ive of community-wide programmes, I shall for the
Non-compliance and antihypertensive therapy
• ~
30 41 "0 ~
~ 20 0 • ~
" • -= 'j 10 •
30
• • • • • • •
•
• femoles • moles
• • •
•
40 age ot entry 60 70
Fig. 2. Age-wx differences in initial withdrawal rates. The rate for females is significently higher than for males (x2 = 8.34; df = 1; p < 0.011. and the rate for those aged < 50 (both sexes) is significantly higher than for those aged> 50 years (x2 = 12.87; df = 2; p <0.011.
moment view subjects as objects and adopt a cost-benefit approach. Fig. 3 is a semi-logarithmic plot of age-specific mortality rates in Australian males in respect of complications of hypertension (stroke, hypertensive heart and renal disease, and ischaemic heart disease) (solid line). Also shown (interrupted curve) are the estimated combined morbidity plus mortality rate 4-fold (estimate based on NBPS data). This curve is to be compared with the horizontal line representing a hypoth-etical withdrawal rate of 5% per annum which is the figure found in the NBPS after the first year.
If such a rate is representative then the risk of withdrawal is so much greater in younger age groups than the risk of developing a complication, that the most likely outcome of potentially effect-ive treatment is non-compliance rather than successful prevention. Not until the age of about
89
45 do the risks become commensurate and the 'signal-to-noise' ratio sufficiently improved for the experiment to have a reasonable chance of success. These arguments against the initiation of treat-ment in younger age groups would be negated if some benefit accrued from treatment over and above the prevention of frank complications. Prof. McCall has in fact presented to this Symposium tentative evidence of some regression of electro-cardiographic RS voltage changes in mild hyper-tensives on treatment .
~ o ... u
u Q) a. '" Q) 01 o
,. , % ' 5 0 p.o. " ---------------------,'-----
.01
~ " ~/ '1'0.0 ,' , , o 1 Sl
b/ ~/
0 1 1
.~/ ~/ .~,
~,' o '
S " , , .001
, , ,
20
, , , , , , , , , , , , , , ,
400-404 males 410-414
430-438
80 age
Fig. 3. Semi-logarithmic plot of age~ific mortality rate expressed 85 a probability for hypertension-related diseases and ischaemic heart disease: Australian males 1968-1972 (leo rubrics appended). Also shown: esti-mated morbidity + mortality rate for mild hypertensives based on NBPS data. the horizontal line representing a withdrawal rate of 5% per annum.
Symposium on hypertension
4. Conclusions
In respect of the long-term management of anti-hypertensive treatment some strategies can be defmed:
1) The majority of withdrawals are preventable in principle, insofar as it is possible to alter human behaviour by encouraging subjects to continue (such techniques have been instituted in the NBPS but it is still too soon to assess their impact).
2) Such efforts directed at improving com-pliance would need to be maximally applied during the initial stages of treatment.
3) Management of therapy would best be placed at the grass-roots level of family doctor and/or health centre.
4) Frequency of appointments should be minimised and appointments tailored to suit indi-vidual subjects.
5) Ambivalefice on the doctor's part about treatment effectiveness and lack of free flow of information between doctor and subject are likely to be negative factors. (Insofar as mild hyper-tension is concerned there is a 'Catch-22'. Ambi-valence evidently causes subjects to discontinue, which impedes the completion of trials and yet trials such as the NBPS are necessary to resolve the ambivalence ).
Would the man from Mars or even from the highlands of New Guinea reach a different con-clusion? We have an ethnocentric view of hyper-tension and of its management by Western-tech-nological means. The highland New Guinean is not faced with the problem of hypertension due pre-sumably to environmental factors such as low-sodium/high-potassium intake. There are other powerful epidemiological and physiological reasons for launching clinical trials of low~odium/ high-potassium diets (Langford and Watson, 1975; Tobian, 1975). Attempting to fmd answers to the problem about the effectiveness of long-term drug
90
treatment are laudable objectives but the question is couched in terms of traditional medicine. Could it be that the high dropout rates encountered are a rejection of the context of the question, i.e. are a substantial proportion of people looking for alternative means of blood pressure control by diet or even by changes of attitude induced by medi-tation or bio-feedback? Such motivation, if it exists, would indeed be useful in long overdue research on dietary methods.
Acknowledgements
I thank my friends and colleagues, Drs Jennifer Baker, Margaret Bullen, Margaret Lamb and Mary Stewart (Study Centre Directors) for their help as well as members of the NBPS Management Com-mittee and the National Heart Foundation of Australia.
References
Abernethy, J.D.: The Australian National Blood Pressure Study. Medical Journal of Australia 1: 821-824 (1974).
Qark, V.A.: Survival distribution. Annual Review of Biophysics and Bioengineering 4: 431-448 (1975).
Langford, H.G. and Watson, R.L.: Electrolytes and hyper-tension; in Paul (Ed.) Epidemiology and Control of Hypertension, p.119-130 (Stratton Intercontinental Medical Book Corporation, New York 1975).
Sackett, D.L: Cardiovascular diseases. Lancet 2: 1189-1191 (1974).
Tobian, L: Current status of salt in hypertension; in Paul (Ed.) Epidemiology and control of Hypertension, p.131-146 (Stratton Intercontinental Medical Book Corporation, New York 1975).
Author's address: Dr J.D. Abernethy, Study Director, National Blood Pressure Study, P.O. Box 691, Canberra City, ACT 2601 (Australia).