the persistence of pain behaviors in patients with chronic back pain is independent of pain and...
TRANSCRIPT

w w w . e l s e v i e r . c o m / l o c a t e / p a i n
PAIN�
151 (2010) 330–336
The persistence of pain behaviors in patients with chronic back painis independent of pain and psychological factors
M.O. Martel, P. Thibault, M.J.L. Sullivan ⇑Department of Psychology, McGill University, Canada H3A 1B1
a r t i c l e i n f o a b s t r a c t
Article history:Received 13 September 2009Received in revised form 5 June 2010Accepted 6 July 2010
Keywords:Pain behaviorChronic painCatastrophizingFear of movementDisability
0304-3959/$36.00 � 2010 International Associationdoi:10.1016/j.pain.2010.07.004
⇑ Corresponding author. Address: Department of P1205 Docteur Penfield, Montréal, Québec, Canada H3
E-mail address: [email protected] (M.J.L.
The primary purpose of the present study was to examine the temporal stability of communicative andprotective pain behaviors in patients with chronic back pain. The study also examined whether the sta-bility of pain behaviors could be accounted for by patients’ levels of pain severity, catastrophizing, or fearof movement. Patients (n = 70) were filmed on two separate occasions (i.e., baseline, follow-up) whileperforming a standardized lifting task designed to elicit pain behaviors. Consistent with previous studies,the results provided evidence for the stability of pain behaviors in patients with chronic pain. The anal-yses indicated that communicative and protective pain behavior scores did not change significantly frombaseline to follow-up. In addition, significant test–retest correlations were found between baseline andfollow-up pain behavior scores. The results of hierarchical multiple regression analyses further showedthat pain behaviors remained stable over time even when accounting for patients’ levels of pain severity.Regression analyses also showed that pain behaviors remained stable when accounting for patients’ lev-els of catastrophizing and fear of movement. Discussion addresses the potential contribution of centralneural mechanisms and social environmental reinforcement contingencies to the stability of pain behav-iors. The discussion also addresses how treatment interventions specifically aimed at targeting painbehaviors might help to augment the overall impact of pain and disability management programs.
� 2010 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
1. Introduction with clinical pain conditions. Pain behaviors have been shown to
Pain behavior refers to the various actions or postural displaysthat are enacted during the experience of pain. Several authorshave supported a distinction between pain behaviors designed tocommunicate pain to others (e.g., grimaces and vocalizations)and pain behaviors designed to protect the body from symptomexacerbation or further injury (e.g., guarding and rubbing)[10,37,38,49].
A number of studies have shown an association between painbehaviors and negative health outcomes. For example, cross-sec-tional studies have shown that higher levels of pain behaviorsare associated with higher levels of functional disability[20,31,37] and lower tolerance for physical activity [16,41]. Pro-spective studies have shown that high levels of pain behaviorsshortly following work injury are predictive of longer duration ofoccupational disability [22,29,33].
The prospective predictive value of pain behaviors for poorhealth and occupational outcomes implies that pain behaviorsare stable over time. At present, there is a paucity of researchaddressing the stability of pain behaviors in individuals presenting
for the Study of Pain. Published by
sychology, McGill University,A 1B1.Sullivan).
be reproducible in patients with chronic back pain [27] and rheu-matoid arthritis [1], but only within relatively short periods oftime. Importantly, the mechanisms responsible for the stabilityof pain behaviors have never been systematically investigated.
One possibility is that pain behaviors are stable over time as afunction of their association with pain experience. Given the robustassociation between self-reports of pain intensity and pain behav-iors (for a review, see [18]), the persistence of pain might contrib-ute to the persistence of pain behaviors. A second possibility is thatpain behavior stability arises from the relation between painbehaviors and stable pain-related psychological variables such ascatastrophizing and pain-related fears. Previous research hasshown that catastrophizing and pain-related fears account for sig-nificant variance in measures of pain behaviors [14,19,41]. A thirdpossibility is that pain behavior stability exists independent of painintensity and pain-related psychological variables. Pain behaviors,like any expressive behaviors, might persist over time as a functionof environmental reinforcement contingencies [8,12,13,44].
Advancing knowledge on the determinants of the stability ofpain behaviors has both theoretical and clinical implications. Froma theoretical perspective, research aimed at elucidating the deter-minants of pain behavior stability might bring greater specificity toconceptual models addressing the relation between pain experi-ence and pain expression [38,48]. From a clinical perspective,
Elsevier B.V. All rights reserved.

M.O. Martel et al. / PAIN�
151 (2010) 330–336 331
interventions specifically targeting the determinants of the stabil-ity of pain behaviors and their associated negative consequencesmight help to augment the overall impact of pain and disabilitymanagement programs.
In the present study, patients with back pain were filmed ontwo separate occasions (i.e., baseline and follow-up) while per-forming a standardized lifting task designed to elicit pain behav-iors. The primary purpose of the study was to examine thedegree to which communicative and protective pain behaviorswere stable across time. Analyses also examined whether the sta-bility of pain behaviors could be accounted for by patients’ levels ofpain severity, catastrophizing, or fear of movement.
2. Methods
2.1. Participants
The sample consisted of 70 participants (37 men and 33 wo-men) with chronic back pain. At the time of initial assessment,the mean age of the sample was 38.6 years with a range of 20–55 years. The mean duration of pain was 111.4 months with arange of 24–432 months. Participants were recruited through localpain treatment centres and newspaper advertisements in Mon-treal. Participants were considered for participation if they hadbeen experiencing symptoms of back pain for more than 6 months.All participants underwent a medical evaluation in order to ensurethat there were no medical contraindications to performing thephysical manoeuvres involved in the lifting task.
2.2. Measures
2.2.1. Pain severityThe McGill Pain Questionnaire [21] was used as a measure of
pain severity associated with participants’ musculoskeletal condi-tion. Participants were asked to endorse adjectives that best de-scribed their back pain. For each participant, the Pain RatingIndex (MPQ-PRI) was computed as the weighted sum of all adjec-tives. The MPQ-PRI has been shown to be a reliable and valid mea-sure of chronic pain experience [43].
2.2.2. Pain catastrophizingThe Pain Catastrophizing Scale (PCS; [34]) was used as a measure
of catastrophic thinking about pain. The PCS contains 13 itemsdescribing different thoughts and feelings that individuals mayexperience when they are in pain. Participants were asked to reflecton past painful experiences and to indicate the degree to which theyexperienced each of 13 thoughts or feelings when experiencing pain,on a 5-point scale from (0) not at all to (4) all the time. Several studieshave supported the reliability and the validity of the PCS as a mea-sure of pain-related catastrophic thinking [34,35,45].
2.2.3. Fear of movement/(re)injuryThe Tampa Scale for Kinesophobia (TSK; [17]) was used to as-
sess fear of movement and re-injury associated with pain. Partici-pants were asked to indicate their level of agreement with each ofthe 17 statements reflecting worries or concerns about the conse-quences of participating in physical activity. The TSK has beenshown to be internally reliable and correlates with measures ofdisability [46].
2.3. Procedure and apparatus
The protocol of this study received ethical approval from theInstitutional Review Board of the Centre de recherche interdiscipli-naire en réadaptation du Montréal métropolitain (CRIR). At the time
of initial assessment (i.e., baseline), participants were informedthat the study was aimed at developing a new assessment proce-dure for chronic pain. They were made aware that the lifting taskmight lead to temporary increases in discomfort and that theywere free to discontinue at any point. Participants were invitedto sign a consent form and to complete the MPQ [21], the PCS[34] and the TSK [17] prior to performing the lifting task. At fol-low-up, participants completed the same questionnaires (MPQ,PCS, and TSK) and performed the same lifting task that was per-formed at baseline. The mean test–retest time interval was22.9 days (SD = 6.9) ranging from 11 to 43 days. Baseline and fol-low-up assessment sessions were carried out by the same researchassistant.
The lifting task was the same as that described in Sullivan et al.[37]. Participants stood in front of a table (surface: 80 � 120 cm)adjusted to waist height and were asked to lift 18 canisters thatwere partially filled with sand. The canisters weighed 2.9, 3.4 or3.9 kg and were arranged in three rows of six canisters. All canis-ters were identical so that the participants were not able to visu-ally discern the variations in weight. The canisters werepositioned such that each weight was represented twice in eachlocation of a double latin square. The canister locations corre-sponded to three functional anthropometric postural positions:normal, maximum and extreme reaches. In the normal reach posi-tion, the participant stood erect with his or her elbow bent at 90�(position 1); in the maximum reach position, the participant stooderect with his or her arm fully extended (position 2); in the extremereach condition, the participant was forwardly flexed with his orher arm fully extended (position 3) [3]. The task was designed suchthat the forward flexion and arm extension required to lift canis-ters positioned further away from the body would increase theloading on the lumbar portion of the spine, momentarily increasingdiscomfort [42].
At both baseline and follow-up, participants performed the lift-ing task twice. In one trial, participants were asked to lift each ofthe 18 canisters and to provide a pain rating after each lift. In aseparate trial, participants were asked to lift each of the 18 canis-ters and to estimate the weights of the canisters. The order of thepain rating and weight estimation trials was counterbalancedacross participants. The participants were asked to lift the canisterswith their dominant arm in a pre-determined sequence. For all theparticipants, the experimenter modeled the lift of the first threecanisters in order to minimize inter-individual variations in theapproach to the lifting task.
Participants were videotaped throughout the lifting task. Acamera, behind an opaque dome, was positioned at a 45�angle tothe table. The camera afforded a frontal view of the face, trunkand upper extremities. Participants were aware that they werebeing videotaped but they could not see the video camera. Theresearch assistant sat approximately 2 m in front of the table andrecorded participants’ pain ratings and weight estimates.
2.4. Assessment of pain behaviors
Two trained coders, blind to experimental hypotheses, indepen-dently coded each video record for instances of pain behavior. Theprocedure used for assessing pain behaviors was modeled after thecoding system developed by Keefe and Block [11]. Coders weretrained to competency using a pain behavior coding manual devel-oped in our laboratory and adapted to the lifting task.
Each video record was divided into 18 different cycles corre-sponding to the lift of each different canister. A cycle was definedas the period starting with the participant touching the handle ofone canister and ending with the moment the participant touchedthe handle of the next canister. Consistent with previousresearch in our laboratory, pain behaviors were classified as either

Table 1Means and standard deviations for measures of pain severity and psychologicalfactors.
Time 1 Time 2 p
M SD M SD
MPQ-PRI 29.0 13.7 31.9 15.2 <.05PCS 27.1 11.8 24.7 13.3 nsTSK 44.8 7.4 44.3 8.1 ns
Note: M, mean; SD, standard deviation. MPQ-PRI, McGill Pain Questionnaire PainRating Index; PCS, Pain Catastrophizing Scale; TSK, Tampa Scale for Kinesophobia.
332 M.O. Martel et al. / PAIN�
151 (2010) 330–336
communicative or protective [37,41]. Communicative pain behav-iors included (1) facial expressions such as grimacing or wincing,and (2) verbal or paraverbal pain expressions such as pain words,grunts, sighs, and moans. Protective pain behaviors included move-ments such as guarding, holding, touching, or rubbing. For each cy-cle, judges recorded the duration (in seconds) of communicativeand protective pain behaviors. For facial expressions, judges addi-tionally provided intensity ratings on a three-point scale with thefollowing anchors: (1) mild, (2) moderate and (3) intense. Indicesof facial expressions were computed by multiplying the durationof pain behavior by its intensity [28,37].
Mean percentage agreement for the duration of each category ofpain behavior was 97% and 90% for communicative and protectivepain behaviors, respectively. Percentage agreement for the ratingsof pain behavior intensity was 96%. Separate indices of communi-cative and protective pain behaviors were computed by summingpain behavior scores across all 18 cycles of the lifting task. Forthe purposes of the present study, indices of communicative andprotective pain behaviors were collapsed (i.e., summed) acrossthe pain rating and weight estimation trials.
2.5. Data analytic approach
2.5.1. Temporal stability of communicative and protective painbehaviors
The temporal stability of communicative and protective painbehaviors was addressed using two different data analytical ap-proaches. First, separate repeated measures analyses of variance(ANOVAs) were conducted to examine the overall changes in com-municative and protective pain behavior scores from baseline tofollow-up (i.e., absolute stability). The data were initially analyzedusing four-way (time X canister position X canister weight X sex)mixed ANOVAs, separately for communicative and protective painbehaviors. Given that initial analyses revealed no significant mainor interaction effects involving sex, this factor was omitted fromthe presentation of ANOVA results.
Pearson correlations were computed to examine the stability ofindividual differences in communicative and protective painbehaviors (i.e., relative stability). Test–retest correlations werecomputed between baseline and follow-up pain behavior scores,separately for communicative and protective pain behaviors.Test–retest stability coefficients were computed separately formen, women and the overall sample (i.e., collapsed across sexes).A Fisher’s Z-test was performed to examine whether stability coef-ficients for communicative and protective pain behaviors differedsignificantly between sexes.
2.5.2. Accounting for the relative stability of communicative andprotective pain behaviors
Pearson correlations were first used to examine the concurrentand prospective relations between pain severity (e.g., MPQ-PRI),psychological factors (PCS, TSK) and pain behavior scores. Hierar-chical multiple regression analyses were then used to examinewhether the relative stability of communicative and protectivepain behaviors could be accounted for by individual differencesin pain severity or in psychological factors. Overall, four regressionmodels were built according to a procedure described by Santoret al. [32]. Regression models were built separately for communi-cative and protective pain behaviors.
The first set of two regression analyses was performed usingfollow-up communicative pain behavior scores as the dependentvariable. In the first regression, pain severity scores, assessed atboth baseline (MPQ-T1) and follow-up (MPQ-T2), were enteredin the first step of the analysis. Baseline communicative painbehavior scores were entered in the final step of the analysis.In the second regression, catastrophizing and fear of movement,
assessed at both baseline (PCS-T1, TSK-T1) and follow-up (PCS-T2,TSK-T2), were entered in the first step of the analysis. Baselinecommunicative pain behavior scores were entered in the final stepof the analysis. The second set of two regression analyses wasperformed identical to that described above, but using protectivepain behavior scores as the dependent variable.
The regression models follow the assumption that the relativestability of pain behaviors may be attributable to individual differ-ences in pain severity and/or psychological factors at eitherbaseline or follow-up, or both [32]. Therefore, any variance infollow-up pain behavior scores that could be attributed to painseverity or psychological factors is removed in the first step of eachregression analysis. Based on the procedure described by Santoret al [32], showing that variance in follow-up pain behavior scorescan be predicted from baseline pain behavior scores over andabove the effects of MPQ, PCS and TSK would demonstrate thatthe relative stability of pain behaviors cannot be entirely attributedto patients’ pain severity or psychological factors.
3. Results
3.1. Sample characteristics
Mean scores on measures of pain severity (MPQ), catastrophiz-ing (PCS) and fear of movement (TSK) are presented in Table 1, sep-arately for baseline and follow-up assessment sessions. One-wayrepeated measures analyses of variance (ANOVAs) revealed no sig-nificant difference from time 1 (i.e., baseline) to time 2 (i.e., follow-up) on the PCS, F(1, 69) = 3.06, ns, or the TSK, F(1, 69) = 0.47, ns. Asignificant difference was found on the MPQ-PRI, F(1, 69) = 4.40,p < 0.05, with patients reporting more severe pain at follow-upthan at baseline. Scores on these measures are comparable to thosethat have been reported in previous research on patients withchronic back pain [5,39,41].
3.2. Absolute stability of communicative pain behaviors
A three-way (time X canister weight X canister position) re-peated measures analysis of variance (ANOVA) was performed oncommunicative pain behavior scores. Means and standard devia-tions are presented in Table 2. The analysis revealed significantmain effects for canister weight, F(2, 68) = 41.57, p < 0.001, andcanister position, F(2, 68) = 50.63, p < 0.001. Examination of mar-ginal means indicated that patients expressed more communica-tive pain behaviors when lifting heavier canisters, and whenlifting canisters positioned further away from the body. No mainor interaction effects were found for time.
3.3. Absolute stability of protective pain behaviors
A three-way (time X canister weight X canister position) re-peated measures analysis of variance (ANOVA) was performed onprotective pain behavior scores (see Table 2). The analysis revealed
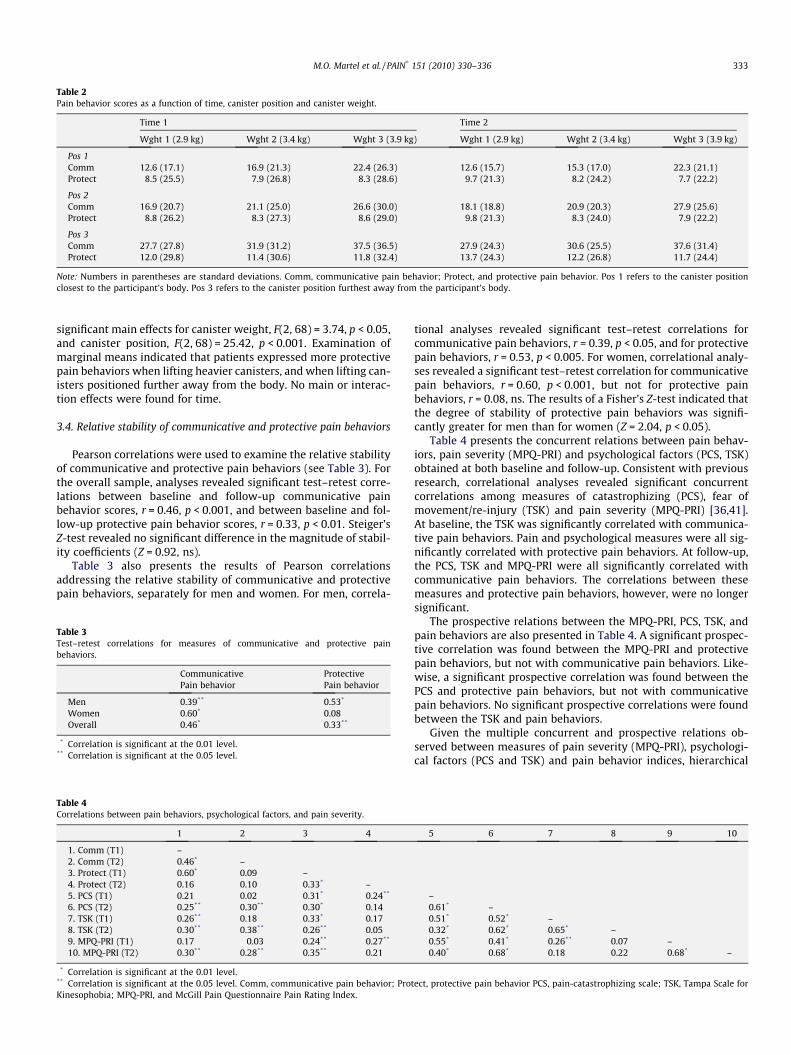
Table 2Pain behavior scores as a function of time, canister position and canister weight.
Time 1 Time 2
Wght 1 (2.9 kg) Wght 2 (3.4 kg) Wght 3 (3.9 kg) Wght 1 (2.9 kg) Wght 2 (3.4 kg) Wght 3 (3.9 kg)
Pos 1Comm 12.6 (17.1) 16.9 (21.3) 22.4 (26.3) 12.6 (15.7) 15.3 (17.0) 22.3 (21.1)Protect 8.5 (25.5) 7.9 (26.8) 8.3 (28.6) 9.7 (21.3) 8.2 (24.2) 7.7 (22.2)
Pos 2Comm 16.9 (20.7) 21.1 (25.0) 26.6 (30.0) 18.1 (18.8) 20.9 (20.3) 27.9 (25.6)Protect 8.8 (26.2) 8.3 (27.3) 8.6 (29.0) 9.8 (21.3) 8.3 (24.0) 7.9 (22.2)
Pos 3Comm 27.7 (27.8) 31.9 (31.2) 37.5 (36.5) 27.9 (24.3) 30.6 (25.5) 37.6 (31.4)Protect 12.0 (29.8) 11.4 (30.6) 11.8 (32.4) 13.7 (24.3) 12.2 (26.8) 11.7 (24.4)
Note: Numbers in parentheses are standard deviations. Comm, communicative pain behavior; Protect, and protective pain behavior. Pos 1 refers to the canister positionclosest to the participant’s body. Pos 3 refers to the canister position furthest away from the participant’s body.
M.O. Martel et al. / PAIN�
151 (2010) 330–336 333
significant main effects for canister weight, F(2, 68) = 3.74, p < 0.05,and canister position, F(2, 68) = 25.42, p < 0.001. Examination ofmarginal means indicated that patients expressed more protectivepain behaviors when lifting heavier canisters, and when lifting can-isters positioned further away from the body. No main or interac-tion effects were found for time.
3.4. Relative stability of communicative and protective pain behaviors
Pearson correlations were used to examine the relative stabilityof communicative and protective pain behaviors (see Table 3). Forthe overall sample, analyses revealed significant test–retest corre-lations between baseline and follow-up communicative painbehavior scores, r = 0.46, p < 0.001, and between baseline and fol-low-up protective pain behavior scores, r = 0.33, p < 0.01. Steiger’sZ-test revealed no significant difference in the magnitude of stabil-ity coefficients (Z = 0.92, ns).
Table 3 also presents the results of Pearson correlationsaddressing the relative stability of communicative and protectivepain behaviors, separately for men and women. For men, correla-
Table 3Test–retest correlations for measures of communicative and protective painbehaviors.
Communicative ProtectivePain behavior Pain behavior
Men 0.39** 0.53*
Women 0.60* 0.08Overall 0.46* 0.33**
* Correlation is significant at the 0.01 level.** Correlation is significant at the 0.05 level.
Table 4Correlations between pain behaviors, psychological factors, and pain severity.
1 2 3 4
1. Comm (T1) –2. Comm (T2) 0.46* –3. Protect (T1) 0.60* 0.09 –4. Protect (T2) 0.16 0.10 0.33* –5. PCS (T1) 0.21 0.02 0.31* 0.24**
6. PCS (T2) 0.25** 0.30** 0.30* 0.147. TSK (T1) 0.26** 0.18 0.33* 0.178. TSK (T2) 0.30** 0.38** 0.26** 0.059. MPQ-PRI (T1) 0.17 �0.03 0.24** 0.27**
10. MPQ-PRI (T2) 0.30** 0.28** 0.35** 0.21
* Correlation is significant at the 0.01 level.** Correlation is significant at the 0.05 level. Comm, communicative pain behavior; ProtKinesophobia; MPQ-PRI, and McGill Pain Questionnaire Pain Rating Index.
tional analyses revealed significant test–retest correlations forcommunicative pain behaviors, r = 0.39, p < 0.05, and for protectivepain behaviors, r = 0.53, p < 0.005. For women, correlational analy-ses revealed a significant test–retest correlation for communicativepain behaviors, r = 0.60, p < 0.001, but not for protective painbehaviors, r = 0.08, ns. The results of a Fisher’s Z-test indicated thatthe degree of stability of protective pain behaviors was signifi-cantly greater for men than for women (Z = 2.04, p < 0.05).
Table 4 presents the concurrent relations between pain behav-iors, pain severity (MPQ-PRI) and psychological factors (PCS, TSK)obtained at both baseline and follow-up. Consistent with previousresearch, correlational analyses revealed significant concurrentcorrelations among measures of catastrophizing (PCS), fear ofmovement/re-injury (TSK) and pain severity (MPQ-PRI) [36,41].At baseline, the TSK was significantly correlated with communica-tive pain behaviors. Pain and psychological measures were all sig-nificantly correlated with protective pain behaviors. At follow-up,the PCS, TSK and MPQ-PRI were all significantly correlated withcommunicative pain behaviors. The correlations between thesemeasures and protective pain behaviors, however, were no longersignificant.
The prospective relations between the MPQ-PRI, PCS, TSK, andpain behaviors are also presented in Table 4. A significant prospec-tive correlation was found between the MPQ-PRI and protectivepain behaviors, but not with communicative pain behaviors. Like-wise, a significant prospective correlation was found between thePCS and protective pain behaviors, but not with communicativepain behaviors. No significant prospective correlations were foundbetween the TSK and pain behaviors.
Given the multiple concurrent and prospective relations ob-served between measures of pain severity (MPQ-PRI), psychologi-cal factors (PCS and TSK) and pain behavior indices, hierarchical
5 6 7 8 9 10
–0.61* –0.51* 0.52* –0.32* 0.62* 0.65* –0.55* 0.41* 0.26** 0.07 –0.40* 0.68* 0.18 0.22 0.68* –
ect, protective pain behavior PCS, pain-catastrophizing scale; TSK, Tampa Scale for
334 M.O. Martel et al. / PAIN�
151 (2010) 330–336
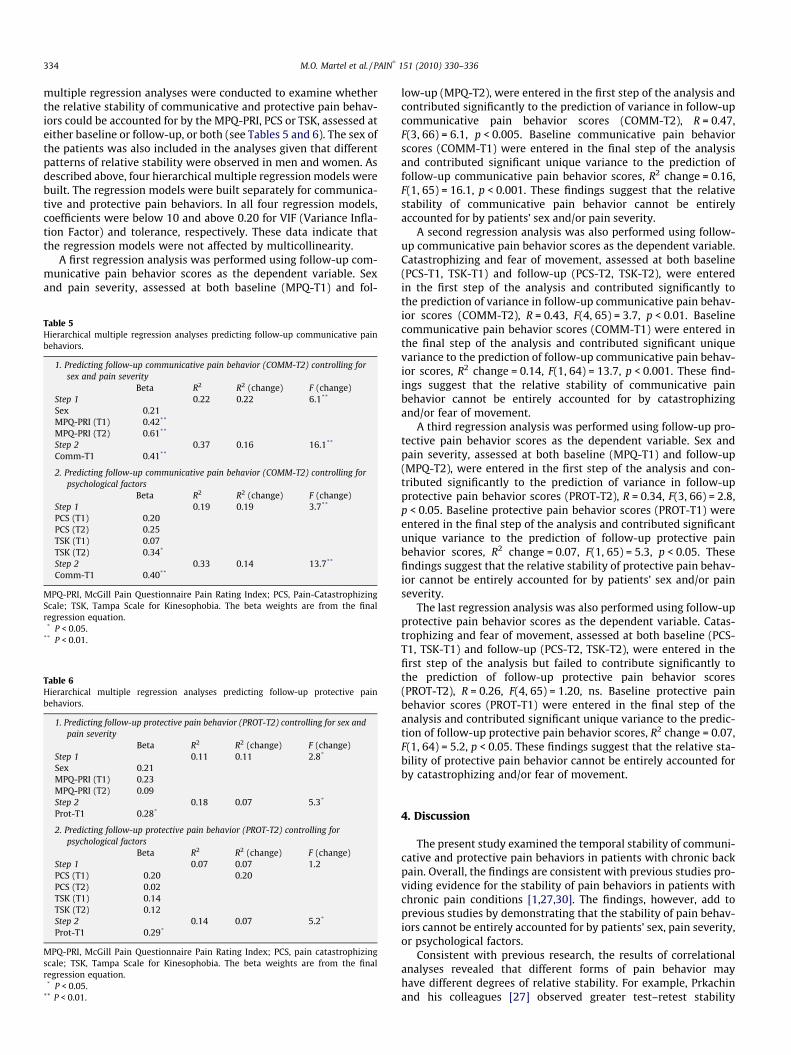
multiple regression analyses were conducted to examine whetherthe relative stability of communicative and protective pain behav-iors could be accounted for by the MPQ-PRI, PCS or TSK, assessed ateither baseline or follow-up, or both (see Tables 5 and 6). The sex ofthe patients was also included in the analyses given that differentpatterns of relative stability were observed in men and women. Asdescribed above, four hierarchical multiple regression models werebuilt. The regression models were built separately for communica-tive and protective pain behaviors. In all four regression models,coefficients were below 10 and above 0.20 for VIF (Variance Infla-tion Factor) and tolerance, respectively. These data indicate thatthe regression models were not affected by multicollinearity.
A first regression analysis was performed using follow-up com-municative pain behavior scores as the dependent variable. Sexand pain severity, assessed at both baseline (MPQ-T1) and fol-
Table 5Hierarchical multiple regression analyses predicting follow-up communicative painbehaviors.
1. Predicting follow-up communicative pain behavior (COMM-T2) controlling forsex and pain severity
Beta R2 R2 (change) F (change)Step 1 0.22 0.22 6.1**
Sex 0.21MPQ-PRI (T1) �0.42**
MPQ-PRI (T2) 0.61**
Step 2 0.37 0.16 16.1**
Comm-T1 0.41**
2. Predicting follow-up communicative pain behavior (COMM-T2) controlling forpsychological factors
Beta R2 R2 (change) F (change)Step 1 0.19 0.19 3.7**
PCS (T1) �0.20PCS (T2) 0.25TSK (T1) �0.07TSK (T2) 0.34*
Step 2 0.33 0.14 13.7**
Comm-T1 0.40**
MPQ-PRI, McGill Pain Questionnaire Pain Rating Index; PCS, Pain-CatastrophizingScale; TSK, Tampa Scale for Kinesophobia. The beta weights are from the finalregression equation.
* P < 0.05.** P < 0.01.
Table 6Hierarchical multiple regression analyses predicting follow-up protective painbehaviors.
1. Predicting follow-up protective pain behavior (PROT-T2) controlling for sex andpain severity
Beta R2 R2 (change) F (change)Step 1 0.11 0.11 2.8*
Sex 0.21MPQ-PRI (T1) 0.23MPQ-PRI (T2) 0.09Step 2 0.18 0.07 5.3*
Prot-T1 0.28*
2. Predicting follow-up protective pain behavior (PROT-T2) controlling forpsychological factors
Beta R2 R2 (change) F (change)Step 1 0.07 0.07 1.2PCS (T1) 0.20 0.20PCS (T2) 0.02TSK (T1) 0.14TSK (T2) �0.12Step 2 0.14 0.07 5.2*
Prot-T1 0.29*
MPQ-PRI, McGill Pain Questionnaire Pain Rating Index; PCS, pain catastrophizingscale; TSK, Tampa Scale for Kinesophobia. The beta weights are from the finalregression equation.
* P < 0.05.** P < 0.01.
low-up (MPQ-T2), were entered in the first step of the analysis andcontributed significantly to the prediction of variance in follow-upcommunicative pain behavior scores (COMM-T2), R = 0.47,F(3, 66) = 6.1, p < 0.005. Baseline communicative pain behaviorscores (COMM-T1) were entered in the final step of the analysisand contributed significant unique variance to the prediction offollow-up communicative pain behavior scores, R2 change = 0.16,F(1, 65) = 16.1, p < 0.001. These findings suggest that the relativestability of communicative pain behavior cannot be entirelyaccounted for by patients’ sex and/or pain severity.
A second regression analysis was also performed using follow-up communicative pain behavior scores as the dependent variable.Catastrophizing and fear of movement, assessed at both baseline(PCS-T1, TSK-T1) and follow-up (PCS-T2, TSK-T2), were enteredin the first step of the analysis and contributed significantly tothe prediction of variance in follow-up communicative pain behav-ior scores (COMM-T2), R = 0.43, F(4, 65) = 3.7, p < 0.01. Baselinecommunicative pain behavior scores (COMM-T1) were entered inthe final step of the analysis and contributed significant uniquevariance to the prediction of follow-up communicative pain behav-ior scores, R2 change = 0.14, F(1, 64) = 13.7, p < 0.001. These find-ings suggest that the relative stability of communicative painbehavior cannot be entirely accounted for by catastrophizingand/or fear of movement.
A third regression analysis was performed using follow-up pro-tective pain behavior scores as the dependent variable. Sex andpain severity, assessed at both baseline (MPQ-T1) and follow-up(MPQ-T2), were entered in the first step of the analysis and con-tributed significantly to the prediction of variance in follow-upprotective pain behavior scores (PROT-T2), R = 0.34, F(3, 66) = 2.8,p < 0.05. Baseline protective pain behavior scores (PROT-T1) wereentered in the final step of the analysis and contributed significantunique variance to the prediction of follow-up protective painbehavior scores, R2 change = 0.07, F(1, 65) = 5.3, p < 0.05. Thesefindings suggest that the relative stability of protective pain behav-ior cannot be entirely accounted for by patients’ sex and/or painseverity.
The last regression analysis was also performed using follow-upprotective pain behavior scores as the dependent variable. Catas-trophizing and fear of movement, assessed at both baseline (PCS-T1, TSK-T1) and follow-up (PCS-T2, TSK-T2), were entered in thefirst step of the analysis but failed to contribute significantly tothe prediction of follow-up protective pain behavior scores(PROT-T2), R = 0.26, F(4, 65) = 1.20, ns. Baseline protective painbehavior scores (PROT-T1) were entered in the final step of theanalysis and contributed significant unique variance to the predic-tion of follow-up protective pain behavior scores, R2 change = 0.07,F(1, 64) = 5.2, p < 0.05. These findings suggest that the relative sta-bility of protective pain behavior cannot be entirely accounted forby catastrophizing and/or fear of movement.
4. Discussion
The present study examined the temporal stability of communi-cative and protective pain behaviors in patients with chronic backpain. Overall, the findings are consistent with previous studies pro-viding evidence for the stability of pain behaviors in patients withchronic pain conditions [1,27,30]. The findings, however, add toprevious studies by demonstrating that the stability of pain behav-iors cannot be entirely accounted for by patients’ sex, pain severity,or psychological factors.
Consistent with previous research, the results of correlationalanalyses revealed that different forms of pain behavior mayhave different degrees of relative stability. For example, Prkachinand his colleagues [27] observed greater test–retest stability

M.O. Martel et al. / PAIN�
151 (2010) 330–336 335
coefficients for measures of facial and paraverbal pain expressions(i.e., communicative pain behaviors) than for measures of guardingand rubbing (i.e., protective pain behaviors). In the present study,the test–retest stability coefficient was also greater for communi-cative pain behavior (r = 0.46) than for protective pain behavior(r = 0.33), however, the difference in the magnitude of stabilitycoefficients was not statistically significant. The difference in thedegree of stability of communicative and protective pain behaviorsis consistent with conceptual models of pain expression suggestingthat there are at least two distinct subsystems of behavior associ-ated with pain [25,38,41,48].
The results of the present study are also consistent with previ-ous research showing sex differences in the stability of pain behav-iors [27]. While stability coefficients for communicative painbehavior were similar in men and women, analyses indicated thatthe stability coefficient for protective pain behavior was signifi-cantly greater for men (r = 0.53) than for women (r = 0.08, ns).The low degree of stability observed for protective pain behaviorsin women raises questions concerning the impact of sex on factorsresponsible for the elicitation and persistence of protective painbehaviors over time. For example, it is possible that women’s pro-tective pain behaviors result from more varied or more contextu-ally determined factors than men’s protective pain behaviors.Although the testing protocol was identical at both test points,contextual features such as novelty, expectancies and interper-sonal familiarity would have still varied across testing sessions.
Like previous research, positive relations were found betweenpain severity and the expression of pain behaviors (for a review,see [18]). Overall, higher levels of pain severity (MPQ-PRI) wereassociated with higher levels of communicative and protectivepain behaviors. Interestingly, however, the results of regressionanalyses indicated that individual differences in pain behaviors re-mained stable from baseline to follow-up even when accountingfor pain severity. These findings are consistent with conceptualmodels that suggest that as pain conditions become chronic, therelation between pain severity and pain behavior becomes weaker[8,18].
Significant positive relations were also found between patients’levels of catastrophizing (PCS), fear of movement (TSK) and theexpression of pain behaviors. The contribution of psychologicalfactors to the variability observed in communicative and protectivepain behaviors was modest, but significant [14,41]. Individual dif-ferences in pain behaviors remained stable over time even whenaccounting for the joint contribution of catastrophizing and fearof movement. The present findings suggest that pain behaviorsare likely to persist at least partially independent of patients’ cata-strophic and fearful thoughts about pain.
A number of explanations might account for the stability ofindividual differences in the expression of pain behaviors. Forexample, a number of investigators have discussed the operationof ‘central motor programs’ responsible for the organization of var-ious forms of behavior in response to pain [10,26,47]. Motor pro-grams operate via neural mechanisms, at both the spinal andsupraspinal levels of the central nervous system (CNS). The neuralarchitecture of motor programs associated with pain is assumed tobe genetically determined, but multiple inputs, including psycho-logical variables, may modulate the activity of these programs[10,26]. In the present study, it is possible that stable individualdifferences in patients’ pain behaviors reflect, to some extent, var-iability in the activity of motor programs responsible for theexpression of pain. Research in neuroscience has shown thatchronic pain states can lead to long-term neuroplastic changes indifferent regions of the CNS, including regions subserving the mo-tor programs involved in the expression of pain [2,23]. As a resultof chronic pain, patients may thus develop motor programs thatlead to automated and stereotyped patterns of pain behaviors dur-
ing pain-eliciting situations. While the degree to which motorprograms can be overridden by contextual or environmental influ-ences remains to be determined, inter-individual variability in theactivity of central motor programs is an explanation that deservesconsideration in trying to account for the stability of patients’ painbehaviors.
Fordyce [8] argued that environmental influences such as rein-forcement contingencies could be sufficient to explain the persis-tence of pain behaviors in patients with pain. According toFordyce [8,9], pain behaviors that are positively reinforced (e.g.,by empathic attention) are likely to be repeated under similar con-ditions in the future, regardless of the level of pain. In contrast,pain behaviors that are punished or ignored are less likely to be re-peated in the future [8,13]. In our study, it is possible that individ-ual differences in pain behaviors reflected patients’ histories ofenvironmental reinforcement contingencies. Perhaps the featuresand physical demands associated with the lifting task resembledpast situations in which patients’ expressive pain behaviors wereeither reinforced or punished [37], leading to stable individual dif-ferences in the expression of pain behaviors. Future studies shouldsystematically manipulate the presence of significant others (e.g.,spouse) and other contextual features of the test sessions in orderto specifically examine the influence of reinforcement contingen-cies on the stability of patients’ pain behaviors.
Finally, it is possible that psychological factors operating out-side of conscious awareness account, at least in part, for the stabil-ity of expressive pain behaviors in patients with pain. Traditionalpsychodynamic models of persistent pain conditions proposed thatunconscious psychological conflicts may, in some cases, take theform of physical symptoms and expressive behaviors [7,24,40].Although psychodynamic models offer a tentative explanation forthe stability of pain behaviors in patients with pain, there are nomethods currently available to reliably assess psychological vari-ables operating outside of conscious awareness that may contrib-ute to the persistence of pain behaviors.
The findings of the present study have implications for thetreatment of patients presenting with clinical pain conditions. Asnoted earlier, there is evidence to indicate that pain behaviors havedeleterious effects on health and occupational outcomes[22,29,33]. The use of treatment interventions specifically aimedat targeting pain behaviors might complement other techniquesused in pain management programs. The findings here suggest thatpain behaviors are likely to persist if treatment efforts are exclu-sively devoted towards the reduction of patients’ pain intensity,catastrophic thinking or fear of movement. In order to successfullyeliminate patients’ pain behaviors, it might become necessary toaddress the social environmental reinforcement contingencies thatcontribute to the persistence of pain behaviors. Recently, there hasbeen an increased specification of the social factors contributing topain behaviors in patients with chronic pain [4]. One of the chal-lenges in the treatment of patients with pain, however, is that pa-tients may not be aware of their own patterns of pain behaviors orthe cognitive or emotional determinants of their pain behavior [6].The use of innovative tools such as video feedback interventionsmay help increase patients’ awareness of maladaptive forms ofpain behavior [15,38]. It may also set the stage for subsequent tar-geted interventions aimed at minimizing pain behaviors and theirassociated negative outcomes.
There are limitations to the current study that must be consid-ered in the interpretation of the findings. Although the patterns ofresults are generally consistent with previous research, the magni-tude of test-retest correlations obtained for measures of painbehaviors is nevertheless lower than that previously reportedamong patients with chronic pain conditions [1,27,30]. In addition,the laboratory setting may not have been fully representative ofthe environmental context in which pain is typically experienced

336 M.O. Martel et al. / PAIN�
151 (2010) 330–336
and expressed, raising questions about the ecological validity ofthe findings. Finally, the stability of patients’ pain behaviors wasexamined while controlling only for a limited number of psycho-logical variables. Other psychological variables such as depression,self-efficacy, extraversion or self-monitoring should be consideredin future research.
In spite of these limitations, the present study is the first todemonstrate that the stability of pain behaviors in patients withchronic pain cannot be entirely accounted for by the persistenceof pain symptoms. The study also demonstrates that the stabilityof pain behaviors cannot be entirely accounted for by psychologicalfactors such as catastrophic thinking and fear of movement. Theactivity of central motor programs is one factor that needs to beconsidered in future research examining the stability of painbehaviors. Research examining the neuroanatomical correlates ofpain behavior might shed light on the mechanisms contributingto the stability of pain behaviors. More research is also needed toelucidate the psychological and social environmental factors thatmight underlie the stability of pain behaviors. Examining the ef-fects of therapeutic interventions on pain behaviors might providean avenue for clarifying the nature of psychological variables thatcontribute to the stability of pain behaviors.
Acknowledgements
The authors thank Ms. Nicole Davidson, Ms. Beatrice Garfinkiel,Nirel Witz and Rebecca Guttman who assisted with recruitment,testing and coding of pain behaviors. This research was supportedby Grants from the Canadian Institutes of Health Research and theSocial Sciences and Humanities Research Council of Canada. Theauthors have no financial interest in the research findings reportedin this paper.
References
[1] Anderson KO, Bradley LA, McDaniel LK, Young LD, Turner RA, Agudelo CA, GabyNS, Keefe FJ, Pisko EJ, Snyder RM, Semble EL. The assessment of pain inrheumatoid arthritis: disease differentiation and temporal stability of abehavioral observation method. J Rheumatol 1987;14:700–4.
[2] Apkarian AV, Bushnell MC, Treede RD. Human brain mechanisms of painperception and regulation in health and disease. Eur J Pain 2005;9:463–84.
[3] Butler H, Kozey J. The effect of load and posture on the relative and absoluteload estimates during simulated manual material handling tasks in femalecheckout operators. Int J Ind Ergonom 2003;31:331–41.
[4] Cano A. Introduction to the special issue on pain in couples. Clin J Pain2008;24:651–3.
[5] Ciechanowski P, Sullivan M, Jensen M, Romano J, Summers H. The relationshipof attachment style to depression, catastrophizing and health care utilizationin patients with chronic pain. Pain 2003;104:627–37.
[6] Craig KD. The social communication model of pain. Can Psychol 2009;50:22–3.[7] Engel G. Psychogenic pain and the pain prone patient. Am J Med
1959;26:899–918.[8] Fordyce WE. Behavioral methods in chronic pain and illness. St. Louis: CV
Mosby; 1976.[9] Fordyce WE. Behavioral science and chronic pain. Postgrad Med J
1984;60:865–8.[10] Hadjistavropoulos T, Craig KD. A theoretical framework for understanding self-
report and observational measures of pain: a communications model. BehavRes Ther 2002;40:551–70.
[11] Keefe FJ, Block AR. Development of an observational method for assessing painbehavior in chronic low back pain patients. Behav Ther 1982;13:363–75.
[12] Keefe FJ, Dunsmore J. Pain behavior: concepts and controversies. Am Pain Soc J1992;1:92–100.
[13] Keefe FJ, Lefebvre JC. Behaviour therapy. In: Wall PD, Melzack R, editors.Textbook of pain. Edinburgh: Churchill Livingstone; 1994. p. 1367–80.
[14] Keefe FJ, Lefebvre JC, Egert JR, Affleck G, Sullivan MJ, Caldwell DS. Therelationship of gender to pain, pain behavior, and disability in osteoarthritispatients: the role of catastrophizing. Pain 2000;87:325–34.
[15] Keefe FJ, Williams DA, Smith S. Assessment of pain behaviors. In: Turk DC,Melzack R, editors. Handbook of pain assessment. New York: Guilford; 2001. p.170–87.
[16] Koho P, Aho S, Watson P, Hurri H. Assessment of chronic pain behaviour:reliability of the method and its relationship with perceived disability,physical impairment and function. J Rehabil Med 2001;33:128–32.
[17] Kori SH, Miller RP, Todd DD. Kinesophobia: a new view of chronic painbehavior. Pain Manag 1990;3:35–43.
[18] Labus JS, Keefe FJ, Jensen MP. Self-reports of pain intensity and directobservations of pain behavior: when are they correlated? Pain 2003;102:109–24.
[19] Main CJ, Watson PJ. Guarded movements: development of chronicity. JMusculoskel Pain 1996;4:163–70.
[20] McCahon S, Strong J, Sharry R, Cramond T. Self-report and pain behavioramong patients with chronic pain. Clin J Pain 2005;21:223–31.
[21] Melzack R. The McGill pain questionnaire: major properties and scoringmethods. Pain 1975;1:277–99.
[22] Ohlund C, Lindstrom I, Areskoug B, Eek C, Peterson LE, Nachemson A. Painbehavior in industrial subacute low back pain. Part I. Reliability: concurrentand predictive validity of pain behavior assessments. Pain 1994;58:201–9.
[23] Peyron R, Laurent B, Garcia-Larrea L. Functional imaging of brain responses topain. A review and meta-analysis. Neurophysiol Clin 2000;30:263–88.
[24] Pilowsky I, Spence ND. Pain, anger and illness behaviour. J Psychosom Res1976;20:411–6.
[25] Prkachin KM. Pain behavior is not unitary. Behav Brain Sci 1986;9:754–5.[26] Prkachin KM, Craig KD. Expressing pain: the communication and
interpretation of facial pain signals. J Nonverbal Behav 1995;19:191–205.[27] Prkachin KM, Hughes E, Schultz I, Joy P, Hunt D. Real-time assessment of pain
behavior during clinical assessment of low back pain patients. Pain2002;95:23–30.
[28] Prkachin KM, Mass H, Mercer SR. Effects of exposure on perception of painexpression. Pain 2004;111:8–12.
[29] Prkachin KM, Schultz IZ, Hughes E. Pain behavior and the development of pain-related disability: the importance of guarding. Clin J Pain 2007;23:270–7.
[30] Prkachin KM, Solomon PE. The structure, reliability and validity of painexpression: evidence from patients with shoulder pain. Pain 2009;139:267–74.
[31] Romano JM, Syrjala K, Levy R, Turner JA, Evans P, Keefe FJ. Overt painbehaviors: relationship to patient functioning and treatment outcome. BehavTher 1988;19:191–201.
[32] Santor DA, Bagby RM, Joffe RT. Evaluating stability and change in personalityand depression. J Pers Soc Psychol 1997;73:1354–62.
[33] Schultz IZ, Crook JM, Berkowitz J, Meloche GR, Milner R, Zuberbier OA,Meloche W. Biopsychosocial multivariate predictive model of occupationallow back disability. Spine 2002;27:2720–5.
[34] Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: developmentand validation. Psychol Assess 1995;7:524–32.
[35] Sullivan MJL, Tripp DA, Santor D. Gender differences in pain and pain behavior:the role of catastrophizing. Cogn Ther Res 2000;24:121–34.
[36] Sullivan MJL, Rodgers WM, Wilson PM, Bell GJ, Murray TC, Fraser SN. Anexperimental investigation of the relation between catastrophizing andactivity intolerance. Pain 2002;100:47–53.
[37] Sullivan MJL, Thibault P, Savard A, Catchlove R, Kozey J, Stanish WD. Theinfluence of communication goals and physical demands on differentdimensions of pain behavior. Pain 2006;125:270–7.
[38] Sullivan MJL. Toward a biopsychomotor conceptualization of pain:implications for research and intervention. Clin J Pain 2008;24:281–90.
[39] Sullivan MJL, Thibault P, Andrikonyte J, Butler H, Catchlove R, Larivière C.Psychological influences on repetition-induced summation of activity-relatedpain in patients with chronic low back pain. Pain 2009;141:70–8.
[40] Szasz TS. Pain and pleasure: a study of bodily feelings. London: Tavistock;1957.
[41] Thibault P, Loisel P, Durand MJ, Catchlove R, Sullivan MJL. Psychologicalpredictors of pain expression and activity intolerance in chronic pain patients.Pain 2008;139:47–54.
[42] Tsuang Y, Schipplein O, Trafimow J, Andersson G. Influence of body segmentdynamics on loads at the lumbar spine during lifting. Ergonomics 1992;35:437–44.
[43] Turk DC, Rudy T, Salovey P. The McGill pain questionnaire: confirming thefactor analysis and examining appropriate uses. Pain 1985;21:385–97.
[44] Turk DC, Flor H. Pain greater than pain behaviors: the utility and limitations ofthe pain behavior construct. Pain 1987;31:277–95.
[45] Van Damme S, Crombez G, Bijttebier P, Goubert L, Van Hoodenhove B. Aconfirmatory factor analysis of the pain catastrophizing scale: invariant factorsstructure across clinical and non-clinical populations. Pain 2002;96:319–24.
[46] Vlaeyen JW, Kole-Snijders AMJ, Boeren RBG, van Eek H. Fear of movement/(re)injury in chronic low back pain and its relation to behavioral performance.Pain 1995;62:363–72.
[47] Wall P. Pain: the science of suffering. London: Weidenfeld and Nicolson; 1999.[48] Williams A. Facial expressions of pain: an evolutionary account. Behav Brain
Sci 2002;25:439–55.[49] Williams A, Craig KD. A science of pain expression. Pain 2006;125:202–3.