the medicine and human rights special study module: a physicians for human rights (uk) initiative
TRANSCRIPT

The Medicine and Human Rights special studymodule: a Physicians for Human Rights (UK) initiative
R.S. MAXWELL & D.J. POUNDERDepartment of Forensic Medicine, University of Dundee, Scotland, UK
SUMM AR Y Human rights have been much neglected in medical
education. An attempt to ® ll this gap was made by introducing a
`Medicine and Human Rights’ special study module into the
undergraduate programme at Dundee. It covers issues such as
physician participation in torture and the death penalty, rape in
war, and the physical and psychological results of torture. Var ious
teaching methods were used, with an emphasis on self-directed
learning. Assessment was by students’ par ticipation in the
programme, including a formal presentation to the class. An
evaluation of the programme showed it to be appreciated by
tutors and students. As a subject, human rights is worthy of
in-depth study by medical students; its study also helps them
acquire a variety of important generic competences. Some aspects
of human rights may merit inclusion in the core programme,
`Man in Society’ .
Introduction
The General Medical Council (1993) published a key docu-
ment: Tomorrow’s Doctors: Recommendations on Undergraduate
Medical Education. This lays out a series of recommended
changes in basic medical education. The recommendations
were designed to solve two problems: they would reduce
curriculum overload and allow courses to adapt to recent
changesÐ social, cultural and technological. A key feature
of the GMC document is the creation of a core curriculum
de® ning the ª requirements that must be satis® ed before a
newly quali® ed doctor can assume the responsibilities of a
pre-registration house officerº . It was recognized that the
diversity among medical schools might be lost with the
introduction of a more stringent core course. To maintain
that diversity, the core curriculum was reduced by 33%.
That time was given over to special study modules (SSMs)
which allow students ª to study in depth in areas of particular
interest to themº .
The GMC recommendations have prompted medical
schools throughout the UK to create SSMs and introduce
them into the MB ChB curriculum. The University of
Dundee introduced a new curriculum in the academic year
1995± 96; since then, SSMs have been playing an important
part in the course (Harden et al., 1997).
In Phase 2 of Dundee’s new curriculum (academicYears
2 and 3), SSMs account for 23% of teaching time. The
relationship between core and options is sequential (Harden
& Davis, 1995). Students proceed to the modules only after
mastering the core. This arrangement caters for differences
in learning speeds. Modules last 2 weeks or 4 weeks.
This paper describes the introduction of an SSM on a
previously neglected subject: the interactions between
medicine and human rights.
Why a special study module on medicine and human
rights?
Respect for human rights is generally agreed to be desir-
able. It is also a vital aspect of international social and
economic development. Medicine has a multifaceted
interface with human rights.Their special skills, their role in
society and their ethical standards make doctors particularly
well placed to promote respect for human rights. Through
lack of a clear awareness of the issues, doctors are also at
risk of being drawn into human rights abuses. Violations
can and do occur in western societies. We are just as guilty
as some countries in the Middle East or the Third World.
Prior to the new Dundee medical curriculum, the subject
had not been studied. However, it had become increasingly
apparent that human rights was an important topic and
merited study. Students could now do so by choosing this
SSM, to enhance their awareness and appreciation of human
rights in medicine.
In keeping with the GMC recommendations, the module
was designed to help students acquire various generic compe-
tences. In particular, the GMC stated that, on completion
of their degrees, medical students should possess a know-
ledge of and understanding of ª ethical and legal issues
relevant to the practice of medicineº ; an ª awareness of the
moral and ethical responsibilities involved in individual
patient careº and should develop an attitude which
recognizes patients’ rights in all respects (GMC, 1993).
Pressure for teaching on human rights to be included in
the medical curriculum has existed throughout the world
for many years. In the UK, a non-governmental organiza-
tion, PHR (UK), lists among its objectives a desire to educate
health professionals about human rights. Until recently, this
had been impossible owing to competition for curriculum
space. However, a statement in Tomorrow’s Doctors provided
the long-awaited opportunity: the extent and range of
modules offered should closely re¯ ect and depend upon the
ª interests, resources and individual enthusiasms of medical
school staff and . . . the wider range of opportunities within
their universitiesº .The implementation of the new Dundee
curriculum built on pre-existing links between PHR (UK)
and the Department of Forensic Medicine, where PHR
(UK) is based. Dundee medical students can now enhance
their knowledge of human rights and widen their perspec-
tive.
Correspondence: Professor D.J. Pounder, Department of Forensic Medicine,
University of Dundee, Dundee DD1 4HN, Scotland, UK.Tel: 44 1382 348020.
Fax: 44 1382 348021. Email: [email protected]
Medical Teacher, Vol. 21, No. 3, 1999
0142-159X/99/030294-05 ½ 1999 Taylor & Francis Ltd294
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.
Module organization
External funding from PHR (UK) allowed the authors to
develop a medicine and human rights module. Develop-
ment took 8 months. At the end of academic year 1995± 96
the SSM was ® rst taught to 27 Phase 1 students.
Initially, we concentrated on aspects of human rights
with which PHR (UK) were already involved. However, as
the course was developed, this extended. Contact was made
with over 100 national and international organizations. Over
700 resources were collected: medical journals, legal texts,
textbooks, news reports and publications and videos from
non-governmental organizations. Only some were actively
employed on the course.
Aims and objectives
The Medicine and Human Rights SSM had six aims:
· to provide students with a knowledge of human rights
standards as expressed in internationally agreed texts; the
supervisory mechanisms which encourage compliance;
and the ways in which practical respect for human rights
is ensured;
· to encourage in students an appreciation of the ways in
which medical personnel can be drawn unwittingly into
human rights abuses;
· to help students develop a knowledge of how medical
personnel and their professional organizations can protect
and respect human rights;
· to assist students to develop the capability of working
efficiently and effectively in groups.
· to assist students to develop the capability of communi-
cating through seminar presentations and discussions;
· to assist students to develop an attitude which views respect
for human rights as an integral part of medical practice.
These aims are in the course guide given to students on
starting the module.
Structure and content
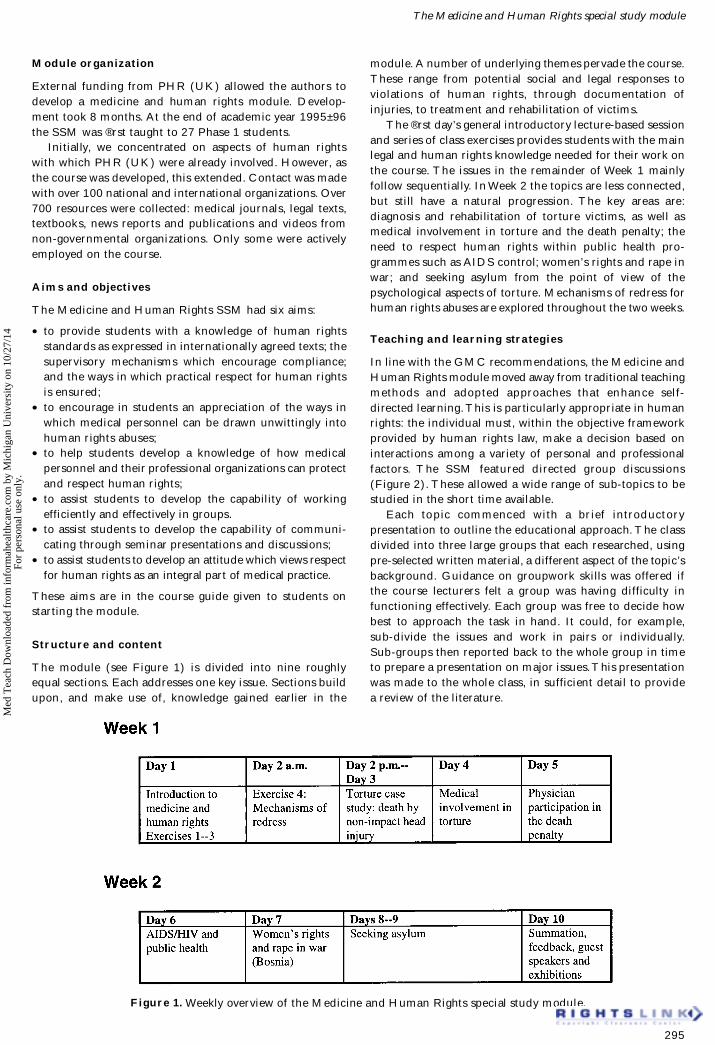
The module (see Figure 1) is divided into nine roughly
equal sections. Each addresses one key issue. Sections build
upon, and make use of, knowledge gained earlier in the
module. A number of underlying themes pervade the course.
These range from potential social and legal responses to
violations of human rights, through documentation of
injuries, to treatment and rehabilitation of victims.
The ® rst day’s general introductory lecture-based session
and series of class exercises provides students with the main
legal and human rights knowledge needed for their work on
the course. The issues in the remainder of Week 1 mainly
follow sequentially. In Week 2 the topics are less connected,
but still have a natural progression. The key areas are:
diagnosis and rehabilitation of torture victims, as well as
medical involvement in torture and the death penalty; the
need to respect human rights within public health pro-
grammes such as AIDS control; women’s rights and rape in
war; and seeking asylum from the point of view of the
psychological aspects of torture. Mechanisms of redress for
human rights abuses are explored throughout the two weeks.
Teaching and learning strategies
In line with the GMC recommendations, the Medicine and
Human Rights module moved away from traditional teaching
methods and adopted approaches that enhance self-
directed learning.This is particularly appropriate in human
rights: the individual must, within the objective framework
provided by human rights law, make a decision based on
interactions among a variety of personal and professional
factors. The SSM featured directed group discussions
(Figure 2). These allowed a wide range of sub-topics to be
studied in the short time available.
Each topic commenced with a br ief introductory
presentation to outline the educational approach. The class
divided into three large groups that each researched, using
pre-selected written material, a different aspect of the topic’s
background. Guidance on groupwork skills was offered if
the course lecturers felt a group was having difficulty in
functioning effectively. Each group was free to decide how
best to approach the task in hand. It could, for example,
sub-divide the issues and work in pairs or individually.
Sub-groups then reported back to the whole group in time
to prepare a presentation on major issues.This presentation
was made to the whole class, in sufficient detail to provide
a review of the literature.
Figure 1. Weekly overview of the Medicine and Human Rights special study module.
The Medicine and Human Rights special study module
295
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

This newly acquired knowledge was then applied to
human rights issues. New groups were formed of approxi-
mately six students to introduce students to the idea of
teamwork and changing team composition. Groups received
a series of ® ctionalized case studies or a number of relevant
questions. Unlike the parallel research session, these smaller
groups all worked on the same tasks. They tried to agree
about the issues raised before a whole-class discussion.
Student assessment
At the start, students were told what assessment procedures
would be employed by tutors. This information was also
printed in the course guide. Because the module is highly
participatory, every student who attended and actively
contributed was likely to pass. However, to gain more than a
mere pass students had to contribute signi® cantly in the group
exercises and presentations. Groups were monitored for how
well they worked together and for whether they achieved their
tasks efficiently and effectively. This was possible, despite the
constant ¯ ux in group composition, simply by observing the
strategies adopted by the group and how well the group
responded to available guidance. Being vocal was not the only
pro® ciency in groupworking; involving all group members
and listening actively were of equal importance.
Knowing that assessment depended so heavily on
presentations made to the class, some of the more confident
members spoke at the ® rst opportunity.Towards the end of
the module, those who had not yet presented began to push
themselves more. As they gained con® dence, they sought to
improve their grading. Guidance in presentation skills was
offered to all students.
Assessment of student presentations was based on a form
obtained from Richard Ellis, an Edinburgh-based trainer
and consultant in communication. The form assessed
presentations under ® ve headings:
· verbal skills, e.g. audibility, clarity and pronunciation;
· non-verbal skills such as eye contact and use of gestures;
· content and structure of the presentation;
· strengths (according to the examiner);
· areas requiring attention.
Under each heading, the examiner put the presentation into
one of three categories. For example, under audibilityÐ the
® rst verbal skill to be assessedÐ the choices were:
· volume well suited to room;
· reasonable, occasional difficulty in hearing;
· poor, difficult to hear, under-projected.
Every student was given a copy of the assessment form in
advance so that they all knew the criteria. They were told
that con® dential feedback on their presentation would be
available, if requested. Every aspect of a presentation was
transferred directly to a numerical scale. These numbers
were totalled, then combined with the tutors’ assessment of
that individual’s contribution to group exercises and to class
discussions. When overall student gradings for the module
were being decided, the forms gave some objective guidance
in classifying students against each other.
Evaluation
The Medicine and Human Rights module was assessed
with a standard feedback questionnaire from the Curriculum
Development Section of Dundee’s Medical Faculty. Students
also completed a questionnaire from the Department of
Forensic Medicine that examined the SSM as a complete
unit and assessed different aspects of individual topics.The
departmental questionnaire gave students space to make
free-text responses: these were later combined with vocal
comments made during the two weeks. Finally, the tutors
themselves assessed the course.
Tables 1 and 2 contain quantitative data from the 26
completed Curriculum Development feedback forms. That
form listed a number of statements concerning module
organization (Statements 1.1 ± 1.5), and delivery (State-
ments 2.1± 2.18). Each was evaluated on a ® ve-point scale,
ranging from 1 (strongly disagree) to 5 (strongly agree).
Figure 2. Typical educational strategy employed in the Medicine and Human Rights SSM.
Table 1. Student opinions of the Medicine and Human Rights SSM organization.
Statement Responsea
Blank
/invalid
1 2 3 4 5 Mean
valueb
1.1 The course was well organized 0 0 0 0 3 23 4.9
1.2 The study/course guide was useful 1 0 0 1 10 14 4.5
1.3 I always knew where I should be 1 0 0 0 7 18 4.7
1.4 I chose this module 1 0 0 0 5 20 4.8
1.5 The process for allocating modules was
appropriate
0 0 1 5 11 9 4.1
a 1 = strongly disagree; 2 = disagree; 3 = uncertain; 4 = agree; 5 = strongly agreeb
Excludes blank/invalid entries
R.S. Maxwell & D.J. Pounder
296
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

The success of the course is obvious from the responses
to all but two of the statements. Question 2.14 asked students
whether they had been able to decide the area of study.
Their responses had a mean of 3.6, signi® cantly lower than
that for most other questions. However, this merely re¯ ects
the highly de® ned module structure, in terms of areas of
study and time per subject. The subjects for group discus-
sion were largely determined by what material was avail-
able.To aid digestion of a large volume of material, guidance
was given on which documents would be of most use.
The lowest mean value (2.5) came in response to ques-
tion 2.16, which asked whether students would have liked
more time to study. In contrast with all other questions, this
low value is actually positive. It states that students were
satis® ed with the time allocated to speci® c tasks, within the
topic and to the whole topic.
Of the 21 participants who completed the Department
of Forensic Medicine questionnaire, 15 rated the course
`excellent’ and the remaining six `very good’ . Many students
stated how enlightening they had found their studies; they
wished to continue learning about the issues they had
touched upon. It was evident that most enjoyed having had
the chance to look at these important issues.
The course provided ample opportunity for individuals
to assess and to question their own attitudes and perspec-
tive towards many issues. Contentious topics, such as the
death penalty and physician participation in torture,
provoked many lively discussions, especially with participants
whose life experiences differed from those of most students.
Class members found themselves continuing to discuss
issues during lunchtimes and at the end of the day with
peers who had selected different modules. The grasping of
essential legal knowledge proved an exciting challenge to
many, widening their perspective and intellectual abilities
through comprehension of a different academic discipline
and teaching style.
Comments and observations from staff and students led
to slight modi® cations of the course material. Primarily
these adjusted the time allocated to certain subjects and,
during the initial sessions, offered guidance on groupwork
skills and presentation skills.
From a teaching perspective, the course was highly
successful, drawing a great deal of active participation from
class members.The inherently ¯ exible nature of the module
allowed progress to be matched to class needs. Sub-issues
were included or omitted as time permitted. Groupworking
and the reconstitution of groups permitted dissemination of
a large quantity of material and the discussion of a wide
range of issues.
The free-text responses were encouraging. Additional
Table 2. Student opinions of the Medicine and Human Rights SSM.
Statement Responsea
Blank
/invalid
1 2 3 4 5 Mean
valueb
2.1 I understood the objectives of the module 0 0 0 0 8 18 4.7
2.2 The structured events of the module were
well delivered
0 0 0 0 7 19 4.7
2.3 There was adequate time available for
private study
1 0 0 3 6 16 4.5
2.4 There was adequate time to re¯ ect on what
I learnt
0 0 0 3 8 15 4.5
2.5 I explored in depth the subject material 0 0 0 5 7 14 4.4
2.6 The course was exciting 1 0 0 0 8 17 4.7
2.7 I felt I had responsibility for my learning 0 0 0 1 11 14 4.5
2.8 I felt able to in¯ uence the running of the
module
0 0 1 4 10 11 4.2
2.9 The module gave me new insight into
medicine
0 0 0 0 6 20 4.8
2.10 I was able to explore the material at my
own pace
0 0 1 5 11 9 4.1
2.11 There was appropriate guidance and
direction
0 0 0 0 9 17 4.7
2.12 The module helped me consider my future
career development
1 0 0 2 9 14 4.5
2.13 The assessment allowed me to express the
work I had done
0 0 1 2 11 12 4.3
2.14 I was able to decide the speci® c area of
study
0 1 1 11 8 5 3.6
2.15 A range of learning materials were used 0 0 0 1 8 17 4.6
2.16 I would have liked more time to study 3 6 6 6 4 1 2.5
2.17 I found this module challenging 0 0 0 0 8 18 4.7
2.18 I enjoyed the module 0 0 0 0 2 24 5.0
a1 = strongly disagree; 2 = disagree; 3 = uncertain; 4 = agree; 5 = strongly agree
bExcludes blank / invalid entries
The Medicine and Human Rights special study module
297
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

module strengths outlined by students included: organiza-
tion and structure, range of content, provision of all relevant
material, logical nature, success of self-directed learning
mechanisms, learning how to review literature, immediate
application of acquired knowledge.
In contrast, concerns about information overload led to
a few calls for issues to be summarized rather than asking
students to extract the important aspects themselves. In
response, it was explained that one purpose of the course
was for students to learn the skill of selective information
retrieval for themselves. Indeed, certain students considered
information availability to be one of the module’s strengths.
There were also calls for additional time to be spent on the
issues, perhaps by making the SSM a three-week or four-
week module, thereby enabling a more complete picture to
be gained.
Discussion and conclusion
Lessons to be learnt from this module are signi® cant to
those who implement change in medical education as well
as those interested in human rights. A signi® cant majority of
students felt human rights was both important and useful: it
deserved a place in the medical curriculum. Inclusion of the
topic as a special study module allowed human rights to
enter the medical curriculum.
The SSM educated students on how to avoid becoming
ensnared in situations where violations are allowed to occur. It
provided them with information about how to respond,
individually or collectively, should abuses be brought to their
attention. Evaluation revealed secondary bene® ts in develop-
ment of generic competences and skills, all of which are
essential to the wider practice of medicine. Approaches that
gave students more responsibility for their own learning were
successful. Directed small-group teaching and self-learning,
while requiring more active participation from students,
facilitated understanding and appreciation. Students were
eager to become more personally involved in the issues they
were studying.The Medicine and Human Rights SSM success-
fully encouraged an alternative approach to learning, where
personal transferable skills are developed and actively applied.
Issues debated in the module can be applied to most
core courses. The course fostered an attitude that viewed
respect for human rights as an integral part of medical
practice. This attitude should remain with students forever.
Although originally designed to run for 2 weeks, the SSM’s
modular structure allows topics to be selected at will then
studied to the required or desired depth. If run in full, there is
material for a full 3 weeks. Careful use of groups made it
possible, within the 2 weeks, for a sufficiently comprehensive
understanding of the background information to be obtained
prior to application of the principles. The modular structure,
chosen deliberately, also allows the material to be used in a
variety of medical settings, in various cultures and within
differing traditions. Timetabling can be adjusted to ® t the
considered priorities of any given teaching environment.
How best, then, can the success of an individual module
spread beyond its creating institution? Not every medical
school in the UK has an organization like PHR (UK) within
its walls. Can special study material be exchanged or shared?
The GMC (1993) recognized the additional workload
created by introducing an optional element into the
curriculum; it encouraged medical schools not only to share
their ideas on development of special studies, but also to
make the necessary teaching and learning materials avail-
able to one another. PHR (UK) and the Department of
Forensic Medicine have done this. They both intend to
continue helping medical undergraduates develop an attitude
of respect for human rights protection. The Medicine and
Human Rights SSM is now freely available on the World
Wide Web for any interested parties to download and use as
required. The address is: http://www.dundee.ac.uk/
med&humanrights/SSM/welcome.html
In considering the practical details of the shift to the new
curriculum, the GMC (1993) was concerned that material
removed from the core should not resurface disguised as an
SSM , thereby perpetuating information overload and
preventing re® nement of core teaching. A unique initiative
such as this module makes consideration of the classi® ca-
tion of `core’ a pertinent debate. Traditionally, the content
of elective periods has been dictated by material already
included in core studies. However, our students have said
that all medical undergraduates should receive education
on human rights issues. Some Medicine and Human Rights
material would enhance core teaching on ethics. It may thus
open avenues revising what is classi® ed as `core.’
Acknowledgement
We gratefully acknowledge external funding from Physi-
cians for Human Rights (UK). That ® nancial help enabled
the creation of the Medicine and Human Rights special
study module.
Notes on contributors
MR S RACH EL MAXWELL obtained her LL.B law degree from the
University of Warwick in 1995. Since moving to Dundee and creating
this education module, she is presently writing her doctoral thesis
evaluating whether human rights law and medical ethics provide
sufficient regulation for the medical profession with respect to torture.
PROFESSOR DERR ICK J POUNDER has been head of the Department of
Forensic Medicine at the University of Dundee, Scotland since 1987 .
As founder member and past chairman of Physicians for Human
Rights (UK), he acts as consultant for a range of human rights agen-
cies internationally.
References
GENERAL M EDICAL COUNCIL (1993) Tomorrow’s Doctors: Recommenda-
tion on Underg raduate Medical Education (London, GMC).
HARDEN , R.M. & DAVIS, M.H. (1995) AMEE Medical Education
Guide No. 5. The core curriculum with options or special study
modules, Medica l Teacher, 17(2), pp. 125 ± 148. [Also available as a
booklet from: Association for Medical Education in Europe,
University of Dundee, Tay Park House, 484 Perth Road, Dundee,
DD2 1LR, Scotland, UK.]
HARDEN , R.M ., DAVIS, M.H. & CROSBY, J.R. (1997) The New Dundee
Medical Curriculum: AWhole that is Greater than the Sum of the Parts
Medical Education, 31, pp. 264 ± 271.
Bibliography
DOWDING , T.J. (1993) The application of a spiral curriculum model to
technical training curricula, Educational Technology, July, pp. 18± 28.
HARDEN , R.M. (1986) Ten questions to ask when planning a course
or curriculum, Medica l Education, 20, pp. 356 ± 365.
R.S. Maxwell & D.J. Pounder
298
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.