the mechanisms and comorbidities of hypertensive disease files/syllabus files... · session 3:...
TRANSCRIPT
the mechanisms and comorbidities
of hypertensive diseasean action plan for the primary care practitioner

Session 3: Mechanisms and Comorbidities of Hypertensive Disease: An Action Plan for the Primary Care Practitioner Learning Objectives
• Outline strategies for cardiometabolic risk reduction in patients with hypertension. • Discuss options for minimizing end-organ damage in patients with hypertension and diabetes.
Faculty
Biff Franklin Palmer, MD Professor of Internal Medicine Nephrology Fellowship Director University of Texas Southwestern Medical School Dallas, Texas Dr Biff Franklin Palmer is professor of internal medicine at University of Texas (UT) Southwestern Medical Center in Dallas, where he is also Nephrology Fellowship Program Director. He is board-certified in internal medicine and nephrology.
Dr Palmer received his medical degree from UT Southwestern and underwent residency training in internal medicine at Walter Reed Army Medical Center in Washington, DC. He then went on to complete a research fellowship in the Department of Nephrology at the Walter Reed Army Institute of Research and a clinical fellowship in the Division of Nephrology at UT Southwestern Medical Center–Parkland Memorial Hospital. Dr Palmer has authored more than 100 articles and chapters, including works published in the New England Journal of Medicine, Transplantation, the American Journal of Medicine, the American Journal of Medical Science, and Advances in Internal Medicine. He has contributed chapters to more than 50 books, including the Atlas of Diseases of the Kidney, Textbook of Nephrology, and Diseases of the Kidney. In addition to his work as an author, Dr Palmer serves as co-editor of the Southwestern Internal Medicine Conference and the American Journal of Medical Sciences. He also serves on the editorial boards of the Clinical Journal of the American Society of Nephrology and the Nephrology Self-Assessment Program (NephSap).
Henry A. Punzi, MD, FCP
Session 3
Medical Director, Clinical Trials Trinity Hypertension Research Institute Trinity Medical Center Carrollton, Texas Clinical Professor Allied Health Institute, Texas Women’s University
Dallas Texas Dr Henry A. Punzi is in private practice and conducts clinical research at the Trinity Hypertension Research Institute in Carrollton, Texas. He is also a clinical professor at Texas Women’s University in Dallas and is an attending physician of internal medicine at Trinity Medical Center in Carrollton. Dr Punzi received his medical degree and postgraduate training from the University of Buenos Aires in Argentina. He completed fellowships in clinical and research hypertension at UT Southwestern Medical School–Parkland Memorial Hospital and St Paul Hospital, all in Dallas. A fellow of the American College of Clinical Pharmacology, Dr Punzi is a member of the Council for High Blood Pressure Research of the American Heart Association, the American Society of Hypertension, and the American Society for Clinical Pharmacology and Therapeutics. He also serves as a reviewer for the Journal of Human Hypertension, the Journal of Clinical Research and Pharmacoepidemiology, the Journal of Geriatric Cardiovascular Medicine, Drugs & Aging, and the American Journal of Hypertension. Dr Punzi chairs the editorial committee of the Dallas Medical Journal. He has published numerous articles in medical journals and written 4 book chapters.
Session 3
Faculty Financial Disclosure Statements The presenting faculty report the following: Dr Palmer is a speaker for Novartis Pharmaceuticals Corporation. Dr Punzi has nothing to disclose. Education Partner Financial Disclosure Statement The content collaborators at SciMed have nothing to disclose. Drug List Generic Trade acarbose Precose amlodipine Norvasc aliskiren Tekturna atenolol Tenormin atorvastatin Lipitor benazepril Lotensin benazepril + Lotensin HCT hydrochlorothiazide hydrochlorothiazide Esidrix, HydroDIURIL, Oretic
Generic Trade irbesartan Avapro losartan Cozaar metformin Glucophage pioglitazone Actos ramipril Altace sitagliptin Januvia telmisartan Micardis trandolapril Mavix valsartan Diovan
®
TM
Notes ___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
1
The Mechanisms and Comorbidities
of Hypertensive Disease
An Action Plan for the
Primary Care Practitioner
Optimizing Blood Pressure Control: An Integral Component
of Cardiometabolic Risk ManagementHenry A. Punzi, MD, FCP
Medical Director, Clinical TrialsTrinity Hypertension Research Institute,
Trinity Medical CenterCarrollton, Texas
Clinical Professor, Allied Health InstituteTexas Women’s University
Dallas, Texas
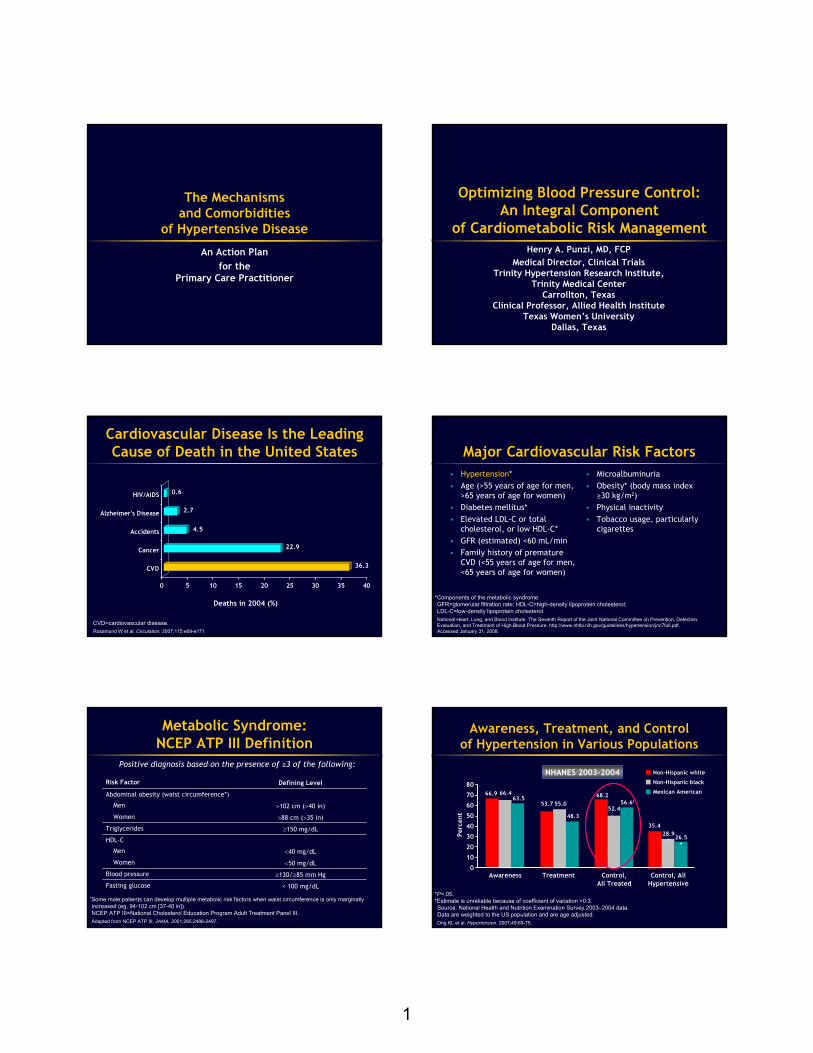
Cardiovascular Disease Is the Leading Cause of Death in the United States
0 5 10 15 20 25 30 35 40
CVD
Cancer
Accidents
Alzheimer's Disease
HIV/AIDS
36.3
4.5
2.7
0.6
22.9
Deaths in 2004 (%)
CVD=cardiovascular disease.Rosamond W et al. Circulation. 2007;115:e69-e171.
Major Cardiovascular Risk Factors• Hypertension*• Age (>55 years of age for men,
>65 years of age for women)• Diabetes mellitus*• Elevated LDL-C or total
cholesterol, or low HDL-C*• GFR (estimated) <60 mL/min• Family history of premature
CVD (<55 years of age for men, <65 years of age for women)
• Microalbuminuria• Obesity* (body mass index
≥30 kg/m2)• Physical inactivity• Tobacco usage, particularly
cigarettes
*Components of the metabolic syndrome. GFR=glomerular filtration rate; HDL-C=high-density lipoprotein cholesterol; LDL-C=low-density lipoprotein cholesterol.National Heart, Lung, and Blood Institute. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. http://www.nhlbi.nih.gov/guidelines/hypertension/jnc7full.pdf. Accessed January 31, 2008.
*Some male patients can develop multiple metabolic risk factors when waist circumference is only marginally increased (eg, 94-102 cm [37-40 in]).NCEP ATP III=National Cholesterol Education Program Adult Treatment Panel III.Adapted from NCEP ATP III. JAMA. 2001;285:2486-2497.
Positive diagnosis based on the presence of ≥3 of the following:
Metabolic Syndrome: NCEP ATP III Definition
Risk Factor Defining Level
Abdominal obesity (waist circumference*)
Men >102 cm (>40 in)
Women >88 cm (>35 in)
Triglycerides ≥150 mg/dL
HDL-C
Men <40 mg/dL
Women <50 mg/dL
Blood pressure ≥130/≥85 mm Hg
Fasting glucose < 100 mg/dL
Awareness, Treatment, and Control of Hypertension in Various Populations
80
70
60
50
40
30
20
10
0
Perc
ent
Awareness Treatment Control,All Treated
Control, AllHypertensive
66.9 66.463.5
53.7 55.0
48.3
68.2
52.456.6†
35.428.9
* 26.5*
Non-Hispanic white
Non-Hispanic black
Mexican American
*P<.05. †Estimate is unreliable because of coefficient of variation >0.3.Source: National Health and Nutrition Examination Survey 2003–2004 data. Data are weighted to the US population and are age adjusted. Ong KL et al. Hypertension. 2007;49:69-75.
NHANES 2003-2004

2
Consequences of Hypertension: Organ Damage
Hypertension
Retinopathy
Peripheral arterialdisease Chronic kidney disease
LVH, CHD, CHFTransient ischemic attack, stroke
CHD=coronary heart disease; CHF=congestive heart failure; LVH=left ventricular hypertrophy.Chobanian AV et al. JAMA. 2003;289:2560-2572.
↓ NO Synthesis
VasoconstrictionThrombosisSuperoxide
↑ COX Activity
Thromboxane A2
Prostaglandin H2
Prostacyclin
Inflammation
Leukocyte adhesion
Endothelialpermeability
Foam cellformation
T-cell activation
↑ Endothelin
VasoconstrictionCalcium
mobilization
Endothelial Dysfunction
DiabetesDyslipidemiaHypertension
Integrated Cellular Mechanisms of Cardiovascular Disease
COX=cyclooxygenase.Ross R. N Engl J Med. 1999;340:115-126.
Classification of Blood Pressure for Adults
Blood Pressure Classification
SBP(mm Hg)
DBP(mm Hg)
Normal <120 and <80
Prehypertension 120-139 or 80-89
Stage 1 hypertension 140-159 or 90-99
Stage 2 hypertension ≥160 or ≥100
DBP=diastolic blood pressure; SBP=systolic blood pressure.National Heart, Lung, and Blood Institute. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. http://www.nhlbi.nih.gov/guidelines/hypertension/jnc7full.pdf. Accessed January 31, 2008.
Cardiovascular Disease Risk Doubles With Each 20/10 mm Hg BP Increment*
Card
iova
scul
ar
dise
ase
risk
SBP/DBP (mm Hg)
0
1
2
3
4
5
6
7
8
115/75 135/85 155/95 175/105
*Individuals aged 40 to 70 years, over the BP range 115/75 to 185/115 mm Hg. Chobanian AV et al. JAMA. 2003;289:2560-2572.
High Normal BP Increases the Risk of Cardiovascular Disease
National Heart, Lung, and Blood Institute. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. http://www.nhlbi.nih.gov/guidelines/hypertension/jnc7full.pdf. Accessed January 31, 2008; Vasan RS et el. N Engl J Med. 2001;345:1291-1297.
Number at risk
Optimal 1875 1867 1851 1839 1821 1734 887
Normal 1126 1115 1097 1084 1061 974 649
High normal 891 874 859 840 812 722 520
Years
Cum
ulat
ive
inci
denc
e (%
) Women
High normalNormalOptimal
0 2 4 6 8 10 12 1402
6
8
10
4
12
14
High Normal BP Increases the Risk of Cardiovascular Disease (cont’d)
0 2 4 6 8 10 12 14
Men
National Heart, Lung, and Blood Institute. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. http://www.nhlbi.nih.gov/guidelines/hypertension/jnc7full.pdf. Accessed January 31, 2008; Vasan RS et el. N Engl J Med. 2001;345:1291-1297.
Cum
ulat
ive
inci
denc
e (%
)
High normalNormalOptimal
Number at risk
Optimal 1005 995 973 962 934 892 454
Normal 1059 1039 1012 982 952 892 520
High normal 903 879 857 819 795 726 441
02
6
8
10
4
12
14
Years
3
Even Small Decreases in BP Produce Benefits
• 2-mm Hg decrease in SBP – 10% reduction in stroke mortality– 7% reduction in IHD mortality
• 10-mm Hg decrease in SBP/5-mm Hg decrease in DBP – 40% reduction in stroke mortality– 30% reduction in IHD mortality
IHD=ischemic heart disease.Lewington S et al. Lancet. 2002;360:1903-1913.
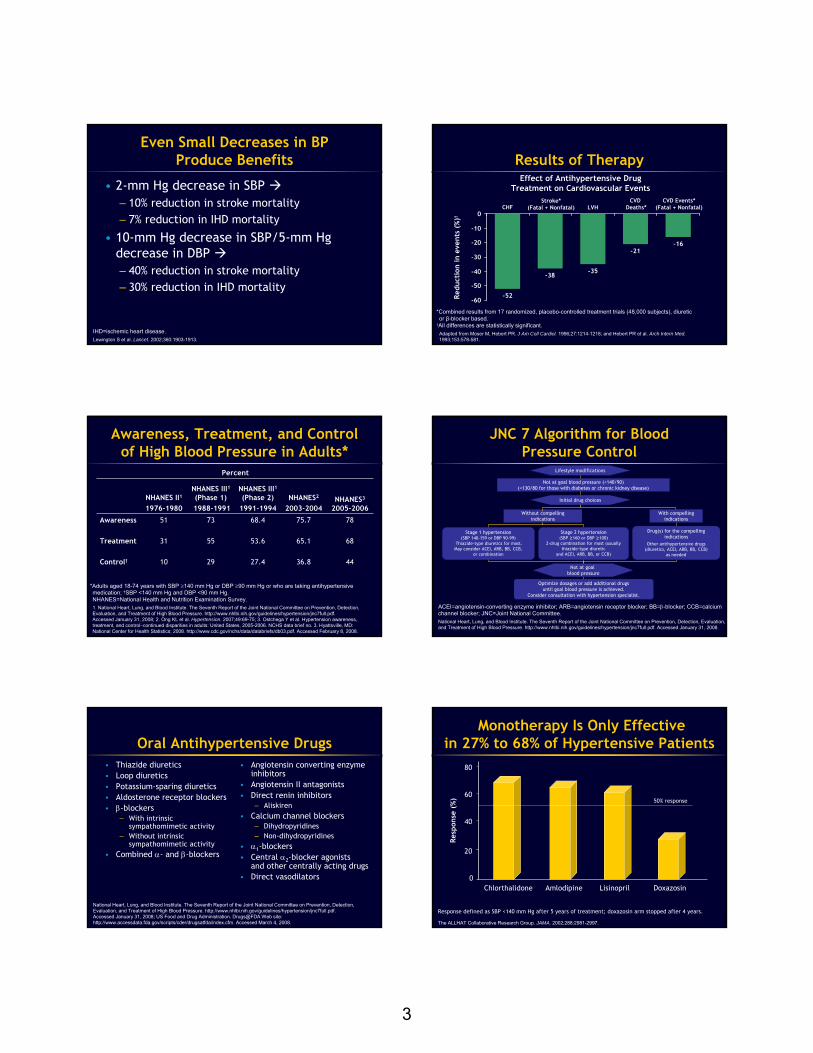
Results of Therapy
-52
-38-35
-21-16
-60
-50
-40
-30
-20
-10
0
CVD Events*(Fatal + Nonfatal)
CVD Deaths*LVH
Stroke*(Fatal + Nonfatal)CHF
Effect of Antihypertensive DrugTreatment on Cardiovascular Events
Redu
ctio
n in
eve
nts
(%)†
*Combined results from 17 randomized, placebo-controlled treatment trials (48,000 subjects), diuretic or β-blocker based.
†All differences are statistically significant.Adapted from Moser M, Hebert PR. J Am Coll Cardiol. 1996;27:1214-1218; and Hebert PR et al. Arch Intern Med.1993;153:578-581.
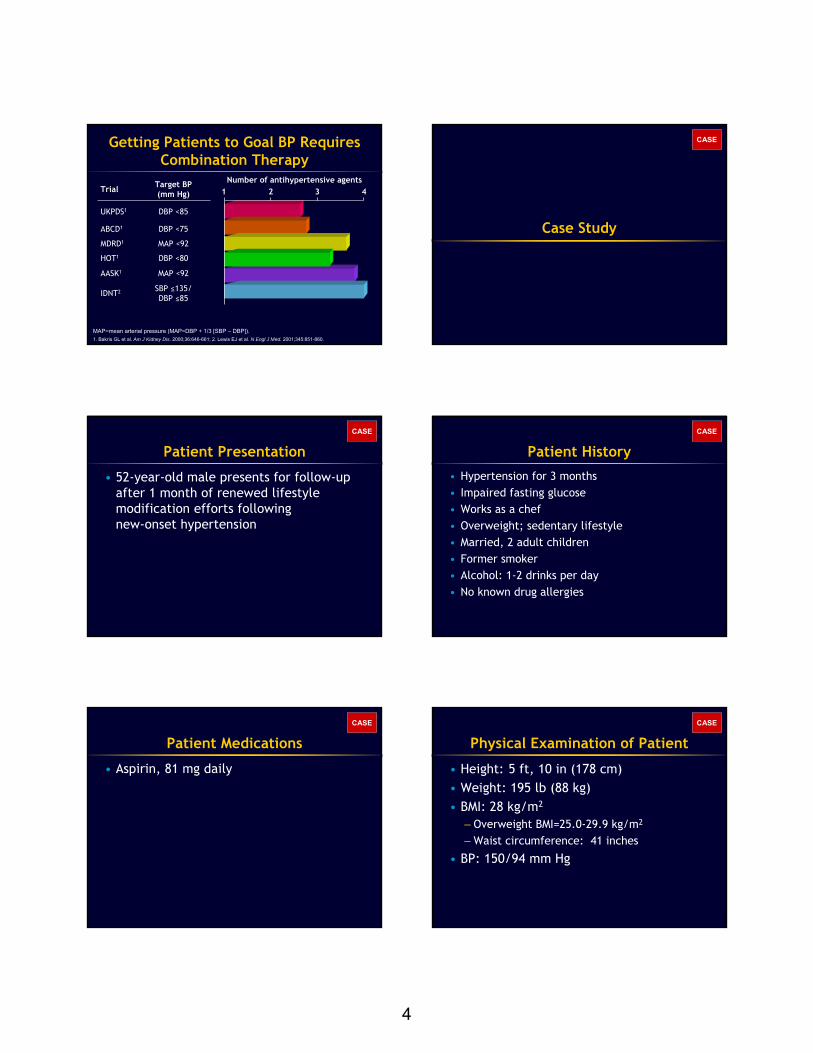
Awareness, Treatment, and Control of High Blood Pressure in Adults*
Percent
NHANES II1
1976-1980
NHANES III1(Phase 1)1988-1991
NHANES III1(Phase 2)
1991-1994NHANES2
2003-2004NHANES3
2005-2006
Awareness 51 73 68.4 75.7 78
Treatment 31 55 53.6 65.1 68
Control† 10 29 27.4 36.8 44
*Adults aged 18-74 years with SBP ≥140 mm Hg or DBP ≥90 mm Hg or who are taking antihypertensive medication; †SBP <140 mm Hg and DBP <90 mm Hg.NHANES=National Health and Nutrition Examination Survey.1. National Heart, Lung, and Blood Institute. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. http://www.nhlbi.nih.gov/guidelines/hypertension/jnc7full.pdf. Accessed January 31, 2008; 2. Ong KL et al. Hypertension. 2007;49:69-75; 3. Ostchega Y et al. Hypertension awareness, treatment, and control–continued disparities in adults: United States, 2005-2006. NCHS data brief no. 3. Hyattsville, MD: National Center for Health Statistics; 2008. http://www.cdc.gov/nchs/data/databriefs/db03.pdf. Accessed February 8, 2008.
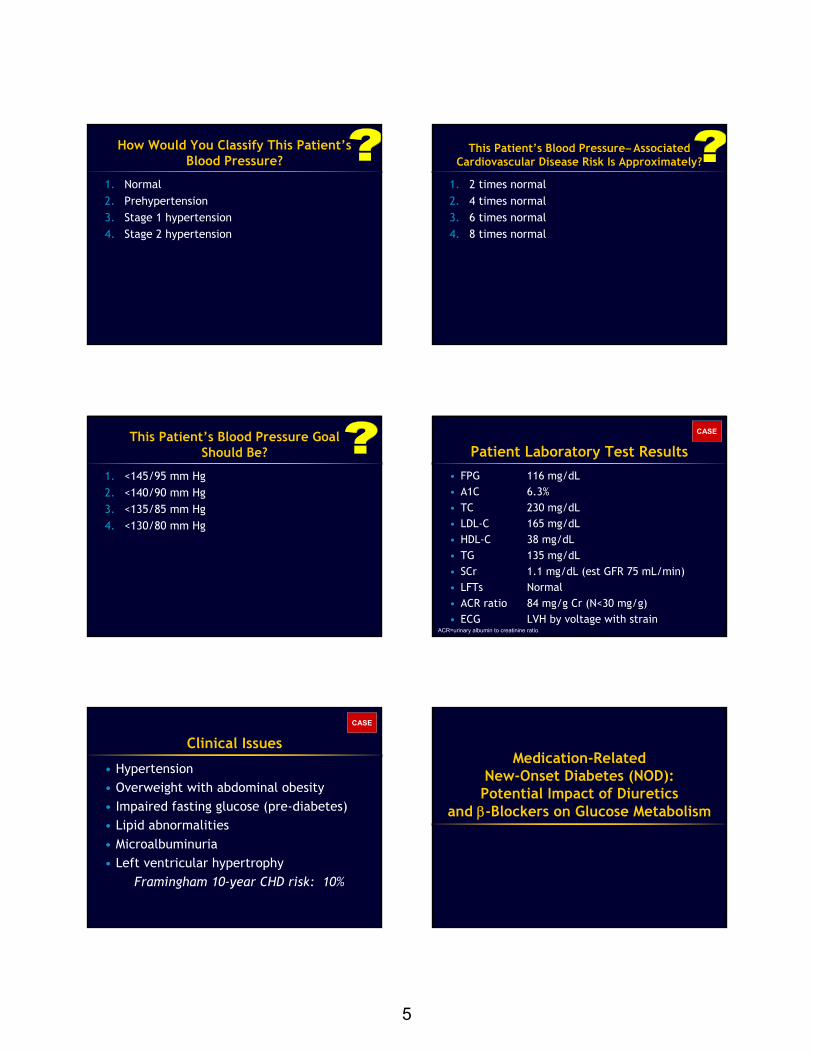
JNC 7 Algorithm for BloodPressure Control
Not at goal blood pressure (<140/90) (<130/80 for those with diabetes or chronic kidney disease)
Lifestyle modifications
Optimize dosages or add additional drugs until goal blood pressure is achieved.
Consider consultation with hypertension specialist.
Stage 2 hypertension (SBP ≥160 or DBP ≥100)
2-drug combination for most (usually thiazide-type diuretic
and ACEI, ARB, BB, or CCB)
Stage 1 hypertension(SBP 140-159 or DBP 90-99)
Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB,
or combination
Without compelling indications
Not at goal blood pressure
With compelling indications
Drug(s) for the compelling indications
Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB)
as needed
ACEI=angiotensin-converting enzyme inhibitor; ARB=angiotensin receptor blocker; BB=β-blocker; CCB=calcium channel blocker; JNC=Joint National Committee.National Heart, Lung, and Blood Institute. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. http://www.nhlbi.nih.gov/guidelines/hypertension/jnc7full.pdf. Accessed January 31, 2008.
Initial drug choices
Oral Antihypertensive Drugs• Thiazide diuretics• Loop diuretics• Potassium-sparing diuretics• Aldosterone receptor blockers• β-blockers
– With intrinsic sympathomimetic activity
– Without intrinsic sympathomimetic activity
• Combined α- and β-blockers
• Angiotensin converting enzyme inhibitors
• Angiotensin II antagonists• Direct renin inhibitors
– Aliskiren• Calcium channel blockers
– Dihydropyridines– Non-dihydropyridines
• α1-blockers• Central α2-blocker agonists
and other centrally acting drugs• Direct vasodilators
National Heart, Lung, and Blood Institute. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. http://www.nhlbi.nih.gov/guidelines/hypertension/jnc7full.pdf. Accessed January 31, 2008; US Food and Drug Administration. Drugs@FDA Web site: http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm. Accessed March 4, 2008.
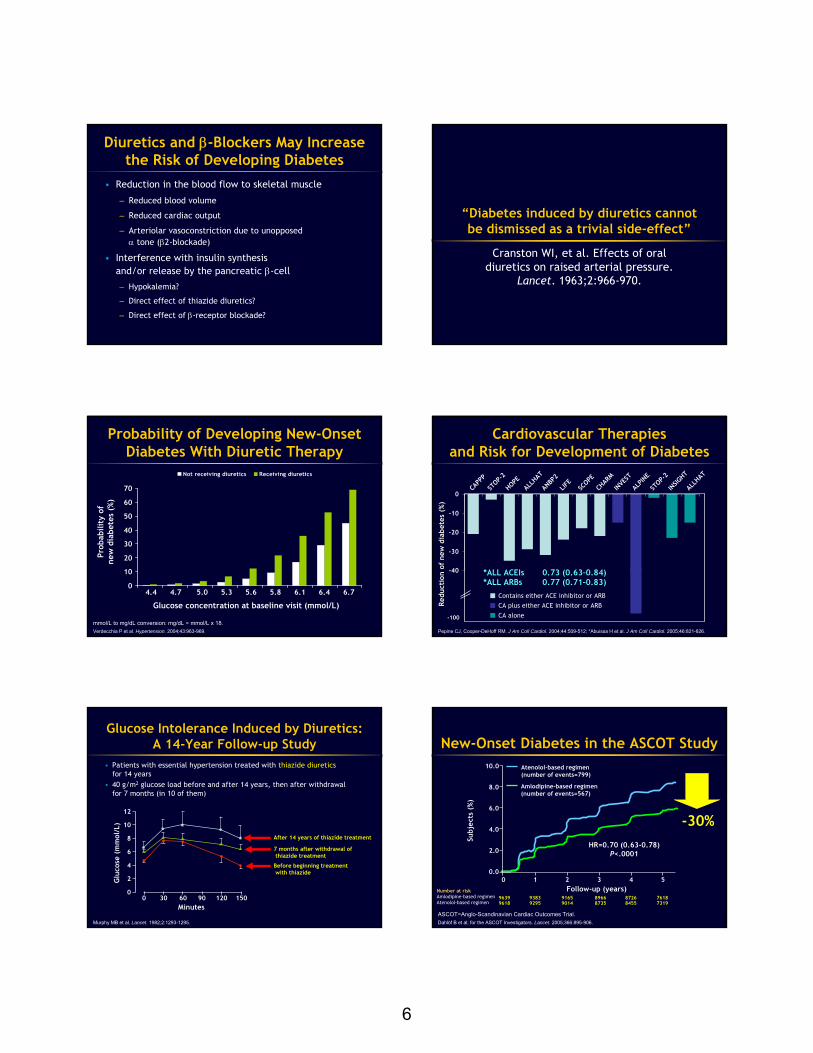
0
20
40
60
80
50% response
Chlorthalidone Amlodipine Lisinopril Doxazosin
Response defined as SBP <140 mm Hg after 5 years of treatment; doxazosin arm stopped after 4 years.
The ALLHAT Collaborative Research Group. JAMA. 2002;288:2981-2997.
Resp
onse
(%
)
Monotherapy Is Only Effective in 27% to 68% of Hypertensive Patients
4
Getting Patients to Goal BP Requires Combination Therapy
Number of antihypertensive agents1 2 3 4Trial Target BP
(mm Hg)
UKPDS1 DBP <85
ABCD1 DBP <75
MDRD1 MAP <92
HOT1 DBP <80
AASK1 MAP <92
IDNT2 SBP ≤135/DBP ≤85
MAP=mean arterial pressure (MAP=DBP + 1/3 [SBP – DBP]).1. Bakris GL et al. Am J Kidney Dis. 2000;36:646-661; 2. Lewis EJ et al. N Engl J Med. 2001;345:851-860.
Case Study
CASE
Patient Presentation
• 52-year-old male presents for follow-up after 1 month of renewed lifestyle modification efforts following new-onset hypertension
CASE
Patient History
• Hypertension for 3 months• Impaired fasting glucose• Works as a chef• Overweight; sedentary lifestyle• Married, 2 adult children• Former smoker• Alcohol: 1-2 drinks per day• No known drug allergies
CASE
Patient Medications
• Aspirin, 81 mg daily
CASE
Physical Examination of Patient
• Height: 5 ft, 10 in (178 cm)• Weight: 195 lb (88 kg)• BMI: 28 kg/m2
– Overweight BMI=25.0-29.9 kg/m2
– Waist circumference: 41 inches
• BP: 150/94 mm Hg
CASE
5
How Would You Classify This Patient’s Blood Pressure?
1. Normal2. Prehypertension3. Stage 1 hypertension4. Stage 2 hypertension
This Patient’s Blood Pressure–Associated Cardiovascular Disease Risk Is Approximately?
1. 2 times normal2. 4 times normal3. 6 times normal4. 8 times normal
This Patient’s Blood Pressure Goal Should Be?
1. <145/95 mm Hg2. <140/90 mm Hg3. <135/85 mm Hg4. <130/80 mm Hg
Patient Laboratory Test Results• FPG 116 mg/dL• A1C 6.3%• TC 230 mg/dL• LDL-C 165 mg/dL• HDL-C 38 mg/dL• TG 135 mg/dL• SCr 1.1 mg/dL (est GFR 75 mL/min)• LFTs Normal• ACR ratio 84 mg/g Cr (N<30 mg/g)• ECG LVH by voltage with strain
ACR=urinary albumin to creatinine ratio.
CASE
Clinical Issues
• Hypertension• Overweight with abdominal obesity• Impaired fasting glucose (pre-diabetes)• Lipid abnormalities• Microalbuminuria• Left ventricular hypertrophy
Framingham 10-year CHD risk: 10%
CASE
Medication-Related New-Onset Diabetes (NOD): Potential Impact of Diuretics
and β-Blockers on Glucose Metabolism
6
Diuretics and β-Blockers May Increase the Risk of Developing Diabetes
• Reduction in the blood flow to skeletal muscle
– Reduced blood volume
– Reduced cardiac output
– Arteriolar vasoconstriction due to unopposed α tone (β2-blockade)
• Interference with insulin synthesis and/or release by the pancreatic β-cell
– Hypokalemia?
– Direct effect of thiazide diuretics?
– Direct effect of β-receptor blockade?
“Diabetes induced by diuretics cannot be dismissed as a trivial side-effect”
Cranston WI, et al. Effects of oral diuretics on raised arterial pressure.
Lancet. 1963;2:966-970.
mmol/L to mg/dL conversion: mg/dL = mmol/L x 18.Verdecchia P et al. Hypertension. 2004;43:963-969.
0
10
20
30
40
50
60
70
Not receiving diuretics Receiving diuretics
Prob
abili
ty o
fne
w d
iabe
tes
(%)
Glucose concentration at baseline visit (mmol/L)
4.4 4.7 5.0 5.3 5.6 5.8 6.1 6.4 6.7
Probability of Developing New-Onset Diabetes With Diuretic Therapy
-40
-30
-20
-10
0CA
PPP
STOP-
2
HOPEALL
HAT
ANBP2
LIFE
SCOPE
CHAR
M
INVES
T
ALPIN
E
STOP-
2
INSIG
HT
ALLHAT
Cardiovascular Therapies and Risk for Development of Diabetes
Redu
ctio
n of
new
dia
bete
s (%
)Re
duct
ion
of n
ew d
iabe
tes
(%)
--100100
Contains either ACE inhibitor or ARBCA plus either ACE inhibitor or ARB
CA alone
Pepine CJ, Cooper-DeHoff RM. J Am Coll Cardiol. 2004;44:509-512; *Abuissa H et al. J Am Coll Cardiol. 2005;46:821-826.
*ALL ACEIs 0.73 (0.63–0.84)*ALL ARBs 0.77 (0.71–0.83)
CAPP
P
STOP-
2
HOPEAL
LHAT
ANBP
2
LIFE
SCOPE
CHAR
M
INVE
ST
ALPIN
E
STOP-
2
INSIG
HT
ALLH
AT
Murphy MB et al. Lancet. 1982;2:1293-1295.
Before beginning treatmentwith thiazide
After 14 years of thiazide treatment
7 months after withdrawal ofthiazide treatment
Glucose Intolerance Induced by Diuretics: A 14-Year Follow-up Study
• Patients with essential hypertension treated with thiazide diureticsfor 14 years
• 40 g/m2 glucose load before and after 14 years, then after withdrawal for 7 months (in 10 of them)
12
10
8
6
4
2
00 30 60 90 120 150
Minutes
Glu
cose
(m
mol
/L)
New-Onset Diabetes in the ASCOT Study
Amlodipine-based regimen(number of events=567)
Atenolol-based regimen(number of events=799)
0 1 2 3 4 5
HR=0.70 (0.630.78)P<.0001
9639 9383 9165 8966 8726 76189618 9295 9014 8735 8455 7319
0.0
10.0
6.0
4.0
8.0
2.0
-30%
Number at riskAmlodipine-based regimenAtenolol-based regimen
Follow-up (years)
Subj
ects
(%
)
ASCOT=Anglo-Scandinavian Cardiac Outcomes Trial.Dahlöf B et al; for the ASCOT Investigators. Lancet. 2005;366:895-906.

7
Incidence of New-Onset Diabetes Among 12,550 Adults: The ARIC Study
Antihypertensive MedicationHazard Ratio*
(95% CI)None 1.0
ACEIs 0.98 (0.72-1.34)
β-Blockers 1.28 (1.04-1.57)†
CCBs 1.17 (0.83-1.66)
Thiazide diuretics 0.91 (0.73-1.13)
*After adjustment for age, sex, race, use of other drugs, BMI, waist-to-hip ratio, level of education, smoking, alcohol use, level of physical activity, SBP, DBP, fasting insulin, hypercholesterolemia, previous CVD disease, previous pulmonary disease, renal insufficiency, family history of diabetes; †P<.05 for comparison with subjects taking no antihypertensive medications.ARIC=Atherosclerosis Risk in Communities.Gress TW et al. N Engl J Med. 2000;342:905-912.
-25%
HR 0.75 (95% CI: 0.63-0.88)
• The risk of new-onset diabetes was 25% lower with losartan than it was with atenolol
• When the population was stratified into 4 groups, based on the likelihood of new-onset diabetes (logistic regression analysis),the protective effectof losartan on incidence of new-onset diabetes emerged in each group
New-Onset Diabetes in the LIFE Study
P<.001
Atenolol + HCTZLosartan + HCTZ
0 6 12 18 24 30 36 42 48 54 60 66Study month
Prop
orti
on o
f pa
tien
ts (
%)
Prop
orti
on o
f pa
tien
ts (
%)
0 6 12 18 24 30 36 42 48 54 60 66Study month26
242220181614121086420
0
2
4
6
8
10
Atenolol + HCTZLosartan + HCTZ
Quartile 4P=.03
Quartile 4
Quartile 3P=.15Quartile 2P=.02Quartile 1P=.04
HCTZ=hydrochlorothiazide (12.5 mg); LIFE= Losartan Intervention For Endpoint reduction in hypertension study. Lindholm LH et al. J Hypertens. 2002;20:1879-1886; Dahlöf B et al. Lancet. 2002;359:995-1003.
SBP 140–160 mm Hg SBP
>160 mm HG
NormoalbuminuriaSBP
<140 mm Hg
0
1
2
3
4
5
6
N=2085, 10-year follow-up.Borch-Johnsen K et al. Arterioscler Thromb Vasc Biol. 1999;19:1992-1997.
Microalbuminuria
Rela
tive
ris
k
IHD Risk Is Related to Microalbuminuria and BP
1.0 1.52.5
(0.9-2.7)(1.2-5.3)
2.2(1.3-3.7)
3.3(1.6-6.9)
5.3(2.2-3.0)
Summary• In hypertensive subjects without diabetes, 1.5-2.0 in every
100 patients per year develop NOD during treatment• NOD may confer a risk of major CV events similar to that of
previously known diabetes• Diuretics and β-blockers induce NOD more frequently than other
classes of drugs. However, independent of drugs, NOD is more common among predisposed subjects (those with obesity, low HDL, family history, etc)
• In subjects at high risk of NOD, in the absence of clear indications for diuretics or β-blockers, it may be reasonable to start treatment with ACEIs, CCBs, or ARBs
• However, because BP normalization is fundamental, diuretics may be considered in these patients, starting with a low dose and monitoring glucose carefully
Target-Organ Protection in Patients With Hypertension
and Diabetes: Critical Role of Combination Therapy
Biff Franklin Palmer, MDProfessor of Internal Medicine
and Nephrology Fellowship Program DirectorUT Southwestern Medical Center
Dallas, Texas
Diabetes and Stroke: Blood Pressure and Medication-Related Considerations

8
7%
18%18%18%
35%42%
0
25
50
75
100
0.0
0.5
1.0
1.5
2.0
2.5
Hazard ratios
1.6 1.6
1.9
1.51.4
1.3
Association Between Blood Pressure and Stroke in Metabolic Syndrome
NOMAS: Comparison of Vascular Risk Ratiosfor the Metabolic Syndrome and Each
of Its Components in Stroke
Att
ribu
tabl
e ri
sk (
%)
NOMAS=Northern Manhattan Study.Boden-Albala B et al. Stroke. 2008;39:30-35.
SBP ≥130 mm Hg,DBP ≥80 mm Hg, or Hx
≥110 mg/dL Women ≥35 inMen ≥40 in
Women ≤50 mg/dLMen ≤40 mg/dL
≥150 mg/dL
Metabolic syndrome
Fastingblood sugar
Blood pressure
Waistcircumference
HDL Triglycerides
According to the JNC VI classification, 60% of strokes occur among patients with high normal, normal, or mild hypertension. Risk begins at 115/75 mm Hg.
Percent of Stroke Induced by SBP in Subjects Aged 65–84 Years
Framingham Study
160–179 mm HgModerate HTN
140–159 mm HgMild HTN
≥180 mm HgSevere HTN
<130 mm HgNormal
130–139 mm HgHigh normal
HTN=hypertension.Joseph LN et al. Stroke. 1999;30:16-20.
21% 19%
12%
18%30%
Diabetes Mellitus and Cerebrovascular Disease
“Autopsy studies suggest that diabetic patients are susceptible to cerebral small-artery disease and lacunarinfarction and may be at risk for large-artery atherosclerotic occlusive disease. Epidemiological studies show that diabetes is a risk factor for ischemic stroke.”
“The pathogenesis of diabetes-associated stroke appears to be linked to excessive glycation and oxidation, endothelial dysfunction, increased platelet aggregation, impaired fibrinolysis and insulin resistance.”
Lukovits TG et al. Neuroepidemiology. 1999;18:1-14.
HOPE: Key Outcomes Ramipril vs Placebo
Outcome RRR (%) P value
Primary 22 <.001
CVD death 26 <.001
MI 20 <.001
Stroke 32 <.001
Incidence of DM 34 <.001
DM complications 16 <.03
Heart failure 23 <.001
Cardiac arrest 38 <.02Treatment: Ramipril vs matching placebo,
3/2 mm Hg blood pressure difference
DM=diabetes mellitus; HOPE=Heart Outcomes Prevention Evaluation study; MI=myocardial infarction; RRR=relative risk reduction.Yusuf S et al. N Engl J Med. 2000;342:145-153.
LIFE Study: Results
0
5
10
15
20
25
30
Primary end point: CV death, MI, and stroke
New-onset diabetes
Rate
per
100
0 pa
tien
t-ye
ars
Atenolol (n=4588)
Losartan (n=4605)
P<.001
23.8 25% reduction in RR
Dahlöf B et al. Lancet. 2002;359:995-1003.
P<.05
27.9
13.0
17.4
Intention-to-treat
LIFE: Fatal/Nonfatal Stroke
Losartan + HCTZ
Atenolol + HCTZ
Adjusted risk reduction 24.9%; P=.001Unadjusted risk reduction 25.8%; P=.0006
Prop
orti
on o
f pa
tien
ts
wit
h fi
rst
even
t (%
)
0
1
2
3
4
5
6
7
8
0 6 12 18 24 30 36 42 48 54 60 66Study time (months)
1.3/0.4 mm Hg bloodpressure differencebetween groups
HCTZ=hydrochlorothiazide.Dahlöf B et al. Lancet. 2002;359:995-1003.
9
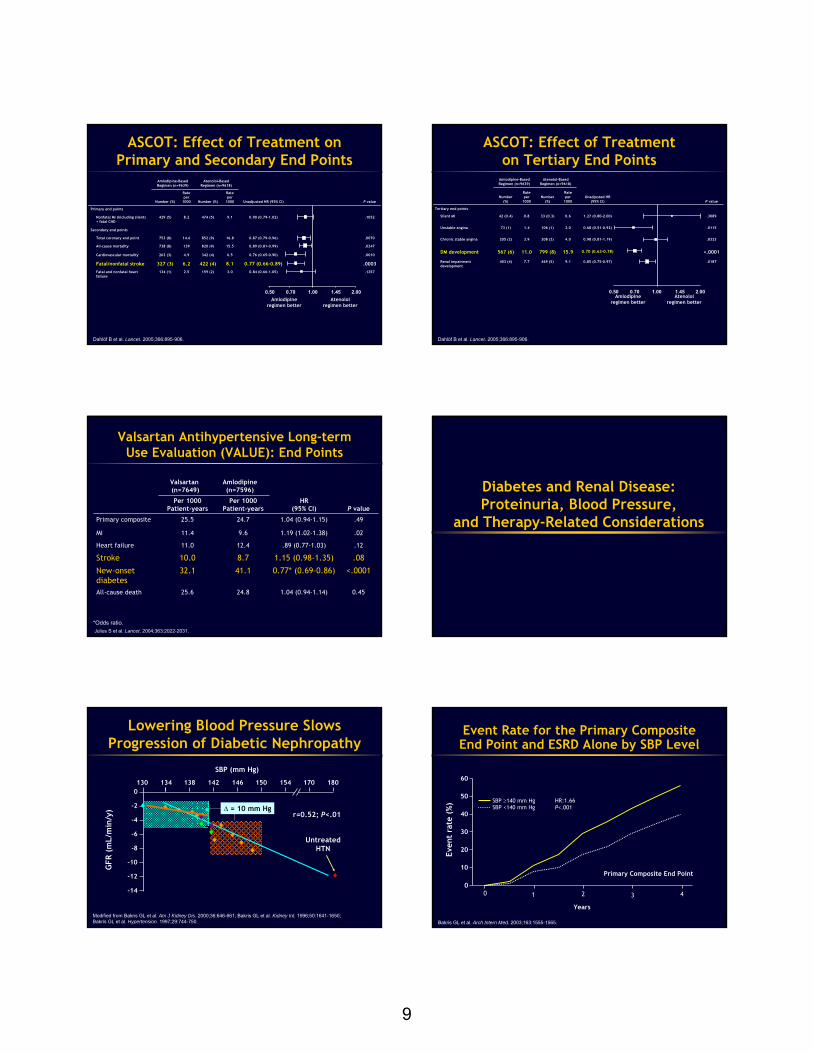
Dahlöf B et al. Lancet. 2005;366:895-906.
ASCOT: Effect of Treatment on Primary and Secondary End Points
Amlodipine-Based Regimen (n=9639)
Atenolol-Based Regimen (n=9618)
Number (%)
Rate per
1000 Number (%)
Rate per
1000 Unadjusted HR (95% CI) P value
Primary end points
Nonfatal MI (including silent) + fatal CHD
429 (5) 8.2 474 (5) 9.1 0.90 (0.79-1.02) .1052
Secondary end points
Total coronary end point 753 (8) 14.6 852 (9) 16.8 0.87 (0.79-0.96) .0070
All-cause mortality 738 (8) 139 820 (9) 15.5 0.89 (0.81-0.99) .0247
Cardiovascular mortality 263 (3) 4.9 342 (4) 6.5 0.76 (0.65-0.90) .0010
Fatal/nonfatal stroke 327 (3) 6.2 422 (4) 8.1 0.77 (0.66-0.89) .0003Fatal and nonfatal heart failure
134 (1) 2.5 159 (2) 3.0 0.84 (0.66-1.05) .1257
0.50 0.70 1.00 1.45 2.00Amlodipine
regimen betterAtenolol
regimen better
Amlodipine-Based Regimen (n=9639)
Atenolol-Based Regimen (n=9618)
Number (%)
Rate per
1000Number
(%)
Rate per
1000Unadjusted HR
(95% CI) P value
Tertiary end points
Silent MI 42 (0.4) 0.8 33 (0.3) 0.6 1.27 (0.80-2.00) .3089
Unstable angina 73 (1) 1.4 106 (1) 2.0 0.68 (0.51-0.92) .0115
Chronic stable angina 205 (2) 3.9 208 (2) 4.0 0.98 (0.81-1.19) .8323
DM development 567 (6) 11.0 799 (8) 15.9 0.70 (0.63-0.78) <.0001
Renal impairment development
403 (4) 7.7 469 (5) 9.1 0.85 (0.75-0.97) .0187
ASCOT: Effect of Treatment on Tertiary End Points
0.50 0.70 1.00 1.45 2.00Amlodipine
regimen betterAtenolol
regimen better
Dahlöf B et al. Lancet. 2005;366:895-906.
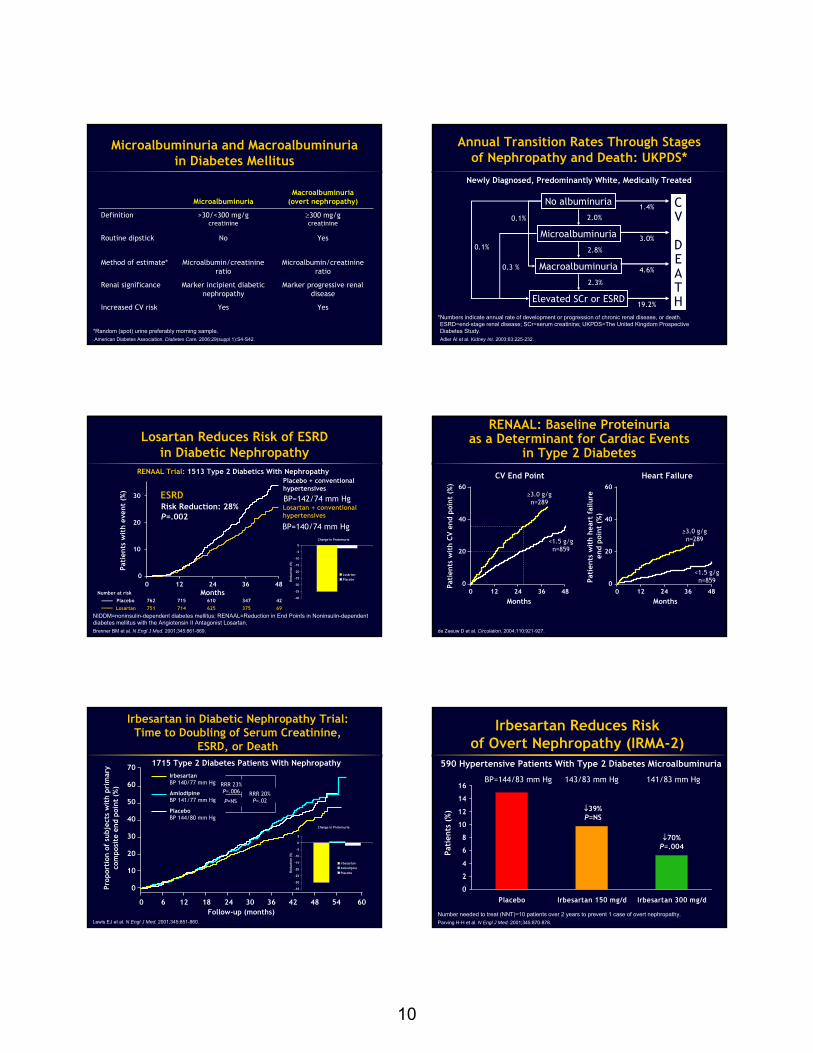
Valsartan Antihypertensive Long-term Use Evaluation (VALUE): End Points
Valsartan(n=7649)
Amlodipine(n=7596)
Per 1000 Patient-years
Per 1000 Patient-years
HR(95% CI) P value
Primary composite 25.5 24.7 1.04 (0.94-1.15) .49
MI 11.4 9.6 1.19 (1.02-1.38) .02
Heart failure 11.0 12.4 .89 (0.77-1.03) .12
Stroke 10.0 8.7 1.15 (0.98-1.35) .08
New-onset diabetes
32.1 41.1 0.77* (0.69-0.86) <.0001
All-cause death 25.6 24.8 1.04 (0.94-1.14) 0.45
*Odds ratio.Julius S et al. Lancet. 2004;363:2022-2031.
Diabetes and Renal Disease: Proteinuria, Blood Pressure,
and Therapy-Related Considerations
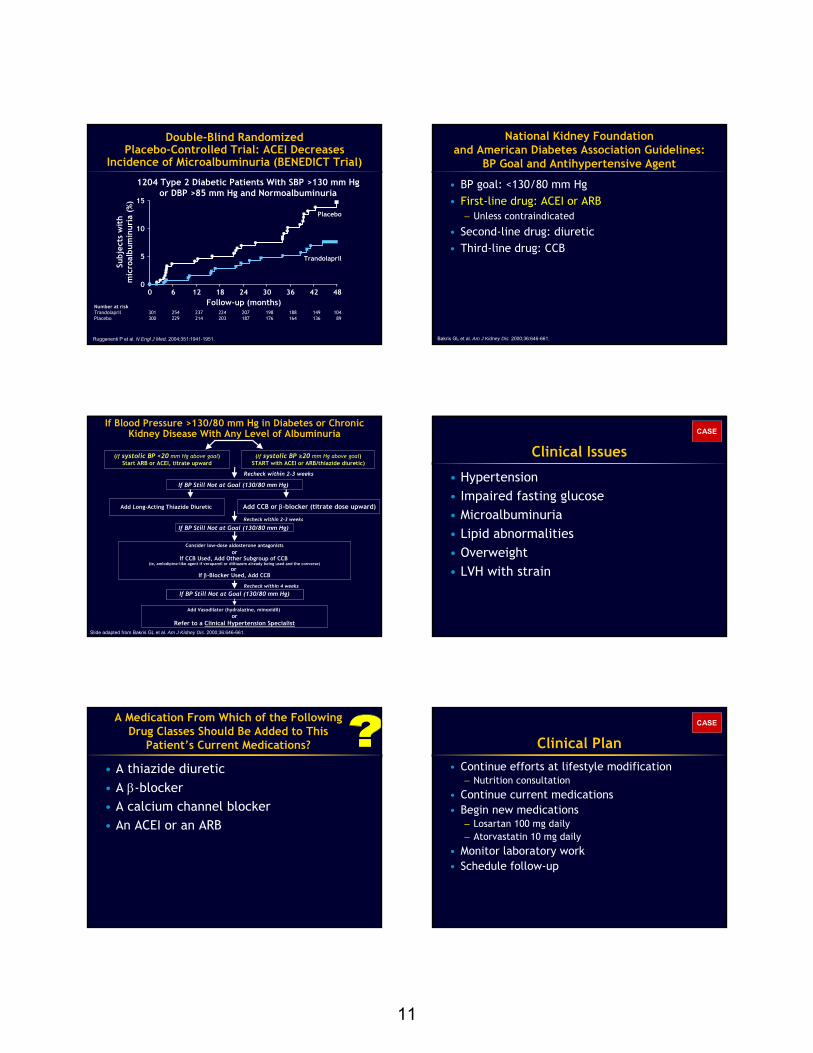
130 134 138 142 146 150 154 170 180
r=0.52; P<.01
SBP (mm Hg)
GFR
(m
L/m
in/y
)
UntreatedHTN
0
-2
-4
-6
-8
-10
-12
-14
∆ = 10 mm Hg
Modified from Bakris GL et al. Am J Kidney Dis. 2000;36:646-661; Bakris GL et al. Kidney Int. 1996;50:1641-1650; Bakris GL et al. Hypertension. 1997;29:744-750.
Lowering Blood Pressure SlowsProgression of Diabetic Nephropathy
Bakris GL et al. Arch Intern Med. 2003;163:1555-1565.
Event Rate for the Primary Composite End Point and ESRD Alone by SBP Level
Even
t ra
te (
%) HR:1.66
P<.001SBP ≥140 mm HgSBP <140 mm Hg
Primary Composite End Point
0
10
20
30
40
50
60
0 21 43
Years
10
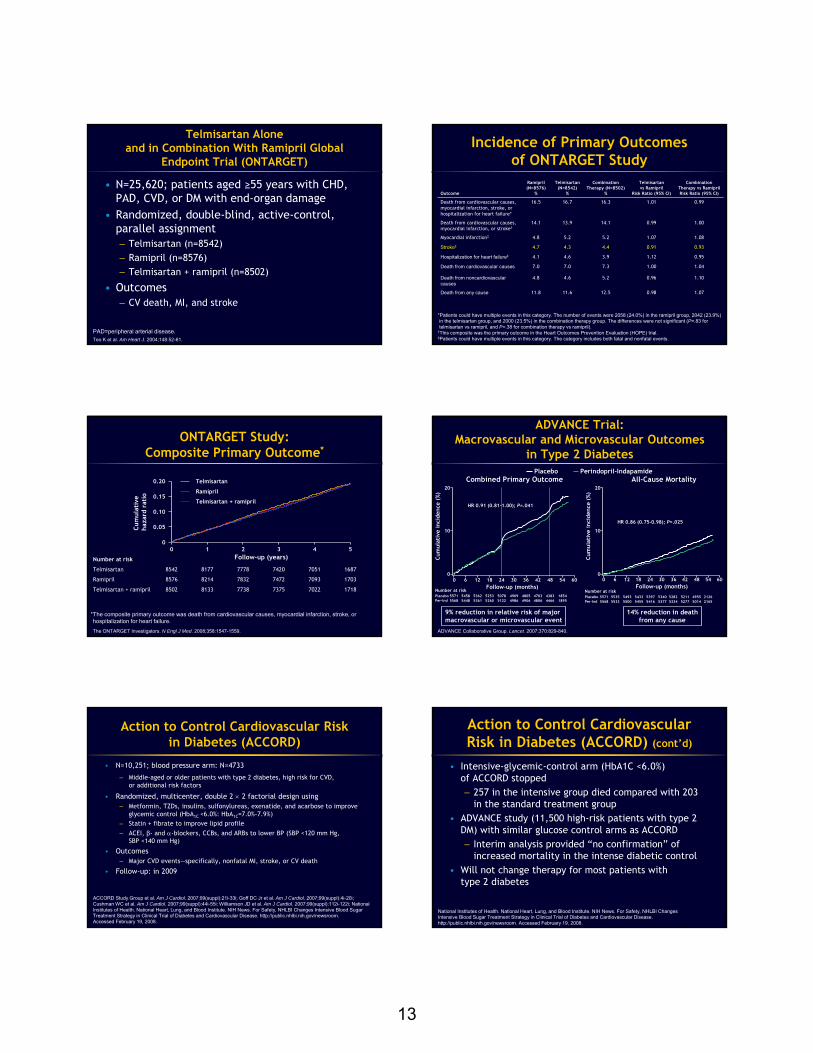
MicroalbuminuriaMacroalbuminuria
(overt nephropathy)
Definition >30/<300 mg/gcreatinine
≥300 mg/gcreatinine
Routine dipstick No Yes
Method of estimate* Microalbumin/creatinineratio
Microalbumin/creatinineratio
Renal significance Marker incipient diabetic nephropathy
Marker progressive renal disease
Increased CV risk Yes Yes
Microalbuminuria and Macroalbuminuriain Diabetes Mellitus
*Random (spot) urine preferably morning sample.American Diabetes Association. Diabetes Care. 2006;29(suppl 1):S4-S42.
Annual Transition Rates Through Stages of Nephropathy and Death: UKPDS*
Newly Diagnosed, Predominantly White, Medically Treated
*Numbers indicate annual rate of development or progression of chronic renal disease, or death.ESRD=end-stage renal disease; SCr=serum creatinine; UKPDS=The United Kingdom Prospective Diabetes Study.Adler AI et al. Kidney Int. 2003;63:225-232.
No albuminuria
Microalbuminuria
Macroalbuminuria
Elevated SCr or ESRD
CV
DEATH
1.4%
3.0%
4.6%
19.2%
2.0%
2.8%
2.3%
0.1%
0.3 %
0.1%
ESRD
Months
Pati
ents
wit
h ev
ent
(%)
0 12 24 36 480
10
20
30
P=.002Risk Reduction: 28%
PlaceboLosartan 751 714 625 375 69
762 715 610 347 42
NIDDM=noninsulin-dependent diabetes mellitus; RENAAL=Reduction in End Points in Noninsulin-dependent diabetes mellitus with the Angiotensin II Antagonist Losartan.Brenner BM et al. N Engl J Med. 2001;345:861-869.
RENAAL Trial: 1513 Type 2 Diabetics With Nephropathy
Losartan Reduces Risk of ESRD in Diabetic Nephropathy
Number at risk
BP=142/74 mm Hg
BP=140/74 mm HgChange in Proteinuria
-40
-35
-30
-25
-20
-15
-10
-5
0
Redu
ctio
n (%
)
LosartanPlacebo
Placebo + conventional hypertensives
Losartan + conventionalhypertensives
RENAAL: Baseline Proteinuriaas a Determinant for Cardiac Events
in Type 2 Diabetes
CV End Point Heart Failure
≥3.0 g/gn=289
<1.5 g/gn=859
≥3.0 g/gn=289
<1.5 g/gn=859
de Zeeuw D et al. Circulation. 2004;110:921-927.
Pati
ents
wit
h CV
end
poi
nt (
%)
0 12 24 36 48Months
0
20
40
60
Pati
ents
wit
h he
art
failu
re
end
poin
t (%
)0 12 24 36 48
Months
0
20
40
60
Irbesartan in Diabetic Nephropathy Trial: Time to Doubling of Serum Creatinine,
ESRD, or Death
Lewis EJ et al. N Engl J Med. 2001;345:851-860.
Prop
orti
on o
f su
bjec
ts w
ith
prim
ary
com
posi
te e
nd p
oint
(%
)
0 6 12 18 24 30 36 42 48 54Follow-up (months)
60
0
10
20
30
40
50
60
70
RRR 20%P=.02P=NS
RRR 23%P=.006
Change in Proteinuria
-35
-30
-25
-20
-15
-10
-5
0
5
Red
ucti
on (
%)
IrbesartanAmlodipinePlacebo
PlaceboBP 144/80 mm Hg
IrbesartanBP 140/77 mm Hg
AmlodipineBP 141/77 mm Hg
1715 Type 2 Diabetes Patients With Nephropathy
Irbesartan Reduces Risk of Overt Nephropathy (IRMA-2)
0
2
4
6
8
10
12
14
16
Placebo Irbesartan 150 mg/d Irbesartan 300 mg/d
↓39%P=NS
↓70%P=.004
Pati
ents
(%
)
Number needed to treat (NNT)=10 patients over 2 years to prevent 1 case of overt nephropathy.Parving H-H et al. N Engl J Med. 2001;345:870-878.
BP=144/83 mm Hg 143/83 mm Hg 141/83 mm Hg
590 Hypertensive Patients With Type 2 Diabetes Microalbuminuria
11
Double-Blind Randomized Placebo-Controlled Trial: ACEI Decreases
Incidence of Microalbuminuria (BENEDICT Trial)
Ruggenenti P et al. N Engl J Med. 2004;351:1941-1951.
1204 Type 2 Diabetic Patients With SBP >130 mm Hg or DBP >85 mm Hg and Normoalbuminuria
15
10
5
0
Subj
ects
wit
hm
icro
albu
min
uria
(%)
0 6 12 18 24 30 36 42 48Follow-up (months)
Trandolapril
Placebo
Number at riskTrandolapril 301 254 237 224 207 198 188 149 104Placebo 300 229 214 203 187 176 164 136 89
National Kidney Foundation and American Diabetes Association Guidelines:
BP Goal and Antihypertensive Agent
• BP goal: <130/80 mm Hg• First-line drug: ACEI or ARB
– Unless contraindicated
• Second-line drug: diuretic• Third-line drug: CCB
Bakris GL et al. Am J Kidney Dis. 2000;36:646-661.
(If systolic BP ≥20 mm Hg above goal)START with ACEI or ARB/thiazide diuretic)
If BP Still Not at Goal (130/80 mm Hg)
If BP Still Not at Goal (130/80 mm Hg)
orIf CCB Used, Add Other Subgroup of CCB
(ie, amlodipine-like agent if verapamil or diltiazem already being used and the converse)or
If β-Blocker Used, Add CCB
Add Vasodilator (hydralazine, minoxidil) or
Refer to a Clinical Hypertension Specialist
If BP Still Not at Goal (130/80 mm Hg)
Add Long-Acting Thiazide Diuretic
Recheck within 2-3 weeks
Recheck within 2-3 weeks
Recheck within 4 weeks
(If systolic BP <20 mm Hg above goal)Start ARB or ACEI, titrate upward
Add CCB or β-blocker (titrate dose upward)
Slide adapted from Bakris GL et al. Am J Kidney Dis. 2000;36:646-661.
Consider low-dose aldosterone antagonists
If Blood Pressure >130/80 mm Hg in Diabetes or Chronic Kidney Disease With Any Level of Albuminuria
Clinical Issues
• Hypertension• Impaired fasting glucose• Microalbuminuria• Lipid abnormalities• Overweight• LVH with strain
CASE
A Medication From Which of the Following Drug Classes Should Be Added to This
Patient’s Current Medications?
• A thiazide diuretic• A β-blocker• A calcium channel blocker• An ACEI or an ARB
Clinical Plan• Continue efforts at lifestyle modification
– Nutrition consultation
• Continue current medications• Begin new medications
– Losartan 100 mg daily– Atorvastatin 10 mg daily
• Monitor laboratory work• Schedule follow-up
CASE

12
Patient Visit at 1 Month
• Patient without specific complaints. He has been adhering to the nutritional plan and walking 20 minutes most days of the week. He reports weight loss of 4 lb, improved exercise tolerance, and generally feels better
CASE
• Height: 5 ft, 10 in (178 cm)• Weight: 191 lb (86.6 kg) (↓ 4 lb) • BMI: 27 kg/m2 (↓ 1 kg/m2)
– Overweight BMI=25.0-29.9 kg/m2
• BP: 127/78 mm Hg (↓ 23/16 mm Hg)
Patient Physical ExaminationCASE
Patient Laboratory Test Results
ACR=urinary albumin to creatinine ratio.
CASE
Old New Change
FPG 116 mg/dL 107 mg/dL -9 mg/dL
A1C 6.3%
TC 230 mg/dL 175 mg/dL -55 mg/dL
LDL-C 165 mg/dL 110 mg/dL -55 mg/dL
HDL-C 38 mg/dL 41 mg/dL +3 mg/dL
TG 135 mg/dL 118 mg/dL -17 mg/dL
ACR ratio 84 mg/g Cr (N<30 mg/g)
39 mg/g Cr (N<30 mg/g)
-45 mg/g Cr
SCr 1.1 mg/dL 1.1 mg/dL
LFTs Normal Normal
Clinical Trials
ACCOMPLISH, ONTARGET, and ACCORD
Avoiding Cardiovascular Events Through Combination Therapy in Patients Living With
Systolic Hypertension (ACCOMPLISH)
• N=11,454; high-risk hypertensives, ≥60 years, SBP ≥160 mm Hg
• Multicenter, randomized, double-blind, controlled trial comparing antihypertensive efficacy of– Benazepril + amlodipine
– Benazepril + HCTZ
• Outcomes– Fatal and nonfatal cardiovascular events
• Follow-up: 5 years (2003-2008)
HCTZ=hydrochlorothiazide.Weber MA et al. Blood Press. 2007;16:13-19; Jamerson KA et al. Am J Hypertens. 2004;17:793-801.
Summary of Results for ACCOMPLISH TRIAL
• Amlodipine/benazepril was found to be superior to benazepril/HCTZ
• CV morbidity/mortality was reduced by 20% in amlodipine/benazepril group compared with benazepril/HCTZ group (P<.002)
• CV death, stroke, and MI were reduced by 20% in amlodipine/benazepril group compared with benazepril/HCTZ group (P<.007)
Avoiding Cardiovascular Events Through Combination Therapy in Patients Living With Systolic Hypertension (ACCOMPLISH). Presented at: SCAI-ACC i2 Summit/American College of Cardiology Annual Scientific Session; March/April, 2008; Chicago, IL.
13
Telmisartan Alone and in Combination With Ramipril Global
Endpoint Trial (ONTARGET)
• N=25,620; patients aged ≥55 years with CHD, PAD, CVD, or DM with end-organ damage
• Randomized, double-blind, active-control, parallel assignment– Telmisartan (n=8542)– Ramipril (n=8576)– Telmisartan + ramipril (n=8502)
• Outcomes– CV death, MI, and stroke
PAD=peripheral arterial disease.Teo K et al. Am Heart J. 2004;148:52-61.
Incidence of Primary Outcomes of ONTARGET Study
Outcome
Ramipril(N=8576)
%
Telmisartan(N=8542)
%
Combination Therapy (N=8502)
%
Telmisartanvs Ramipril
Risk Ratio (95% CI)
Combination Therapy vs RamiprilRisk Ratio (95% CI)
Death from cardiovascular causes, myocardial infarction, stroke, or hospitalization for heart failure*
16.5 16.7 16.3 1.01 0.99
Death from cardiovascular causes, myocardial infarction, or stroke†
14.1 13.9 14.1 0.99 1.00
Myocardial infarction‡ 4.8 5.2 5.2 1.07 1.08
Stroke‡ 4.7 4.3 4.4 0.91 0.93
Hospitalization for heart failure‡ 4.1 4.6 3.9 1.12 0.95
Death from cardiovascular causes 7.0 7.0 7.3 1.00 1.04
Death from noncardiovascularcauses
4.8 4.6 5.2 0.96 1.10
Death from any cause 11.8 11.6 12.5 0.98 1.07
*Patients could have multiple events in this category. The number of events were 2058 (24.0%) in the ramipril group, 2042 (23.9%) in the telmisartan group, and 2000 (23.5%) in the combination therapy group. The differences were not significant (P=.83 for telmisartan vs ramipril, and P=.38 for combination therapy vs ramipril).
†This composite was the primary outcome in the Heart Outcomes Prevention Evaluation (HOPE) trial.‡Patients could have multiple events in this category. The category includes both fatal and nonfatal events.
ONTARGET Study: Composite Primary Outcome*
*The composite primary outcome was death from cardiovascular causes, myocardial infarction, stroke, or hospitalization for heart failure.
The ONTARGET Investigators. N Engl J Med. 2008;358:1547-1559.
0 1 2 3 4 50
0.05
0.10
0.15
0.20
Follow-up (years)
Cum
ulat
ive
haza
rd r
atio
Telmisartan
Ramipril
Telmisartan + ramipril
8542 8177 7778 7420 7051 1687
8576 8214 7832 7472 7093 1703
8502 8133 7738 7375 7022 1718
Telmisartan
Ramipril
Telmisartan + ramipril
Number at risk
ADVANCE Trial: Macrovascular and Microvascular Outcomes
in Type 2 Diabetes
ADVANCE Collaborative Group. Lancet. 2007;370:829-840.
20
10
0
Cum
ulat
ive
inci
denc
e (%
)
HR 0.91 (0.81-1.00); P=.041
Placebo Perindopril-IndapamideCombined Primary Outcome
PlaceboPer-Ind
Number at risk5571 5458 5362 5253 5078 4909 4805 4703 4383 18545568 5448 5361 5260 5122 4986 4906 4806 4466 1895
20
10
0
Cum
ulat
ive
inci
denc
e (%
)
HR 0.86 (0.75-0.98); P=.025
All-Cause Mortality
PlaceboPer-Ind
Number at risk5571 5535 5493 5433 5397 5340 5282 5211 4955 21265568 5533 5500 5455 5416 5377 5334 5277 5014 2165
0 6 12 18 24 30 36 42 48 54 60Follow-up (months)
9% reduction in relative risk of major macrovascular or microvascular event
14% reduction in deathfrom any cause
0 6 12 18 24 30 36 42 48 54 60Follow-up (months)
Action to Control Cardiovascular Risk in Diabetes (ACCORD)
• N=10,251; blood pressure arm: N=4733
– Middle-aged or older patients with type 2 diabetes, high risk for CVD, or additional risk factors
• Randomized, multicenter, double 2 × 2 factorial design using – Metformin, TZDs, insulins, sulfonylureas, exenatide, and acarbose to improve
glycemic control (HbA1C <6.0%: HbA1C=7.0%-7.9%)– Statin + fibrate to improve lipid profile– ACEI, β- and α-blockers, CCBs, and ARBs to lower BP (SBP <120 mm Hg,
SBP <140 mm Hg)
• Outcomes– Major CVD events—specifically, nonfatal MI, stroke, or CV death
• Follow-up: in 2009
ACCORD Study Group et al. Am J Cardiol. 2007;99(suppl):21i-33i; Goff DC Jr et al. Am J Cardiol. 2007;99(suppl):4i-20i; Cushman WC et al. Am J Cardiol. 2007;99(suppl):44i-55i; Williamson JD et al. Am J Cardiol. 2007;99(suppl):112i-122i; National Institutes of Health. National Heart, Lung, and Blood Institute. NIH News. For Safety, NHLBI Changes Intensive Blood Sugar Treatment Strategy in Clinical Trial of Diabetes and Cardiovascular Disease. http://public.nhlbi.nih.gov/newsroom. Accessed February 19, 2008.
Action to Control Cardiovascular Risk in Diabetes (ACCORD) (cont’d)
• Intensive-glycemic-control arm (HbA1C <6.0%)of ACCORD stopped– 257 in the intensive group died compared with 203
in the standard treatment group• ADVANCE study (11,500 high-risk patients with type 2
DM) with similar glucose control arms as ACCORD– Interim analysis provided “no confirmation” of
increased mortality in the intense diabetic control • Will not change therapy for most patients with
type 2 diabetes
National Institutes of Health. National Heart, Lung, and Blood Institute. NIH News. For Safety, NHLBI ChangesIntensive Blood Sugar Treatment Strategy in Clinical Trial of Diabetes and Cardiovascular Disease.http://public.nhlbi.nih.gov/newsroom. Accessed February 19, 2008.
14
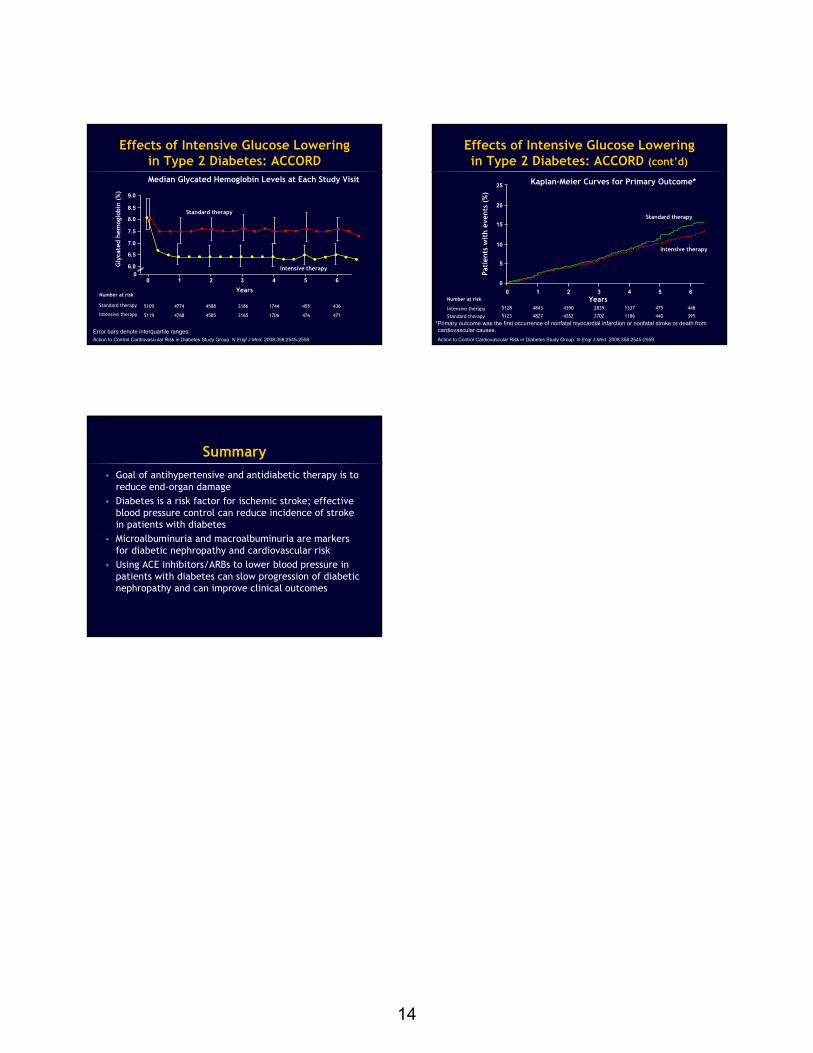
Effects of Intensive Glucose Lowering in Type 2 Diabetes: ACCORD
Error bars denote interquartile ranges.Action to Control Cardiovascular Risk in Diabetes Study Group. N Engl J Med. 2008;358:2545-2559.
9.0
8.5
8.0
7.5
7.0
6.5
6.00
0 1 2 3 4 5 6
Gly
cate
dhe
mog
lobi
n (%
)
Years
Standard therapy
Intensive therapy
Number at risk
Standard therapy 5109
5119
4774
4768
4588
4585
3186
3165
1744
1706
455
476
436
471Intensive therapy
Median Glycated Hemoglobin Levels at Each Study Visit
Effects of Intensive Glucose Lowering in Type 2 Diabetes: ACCORD (cont’d)
25
20
15
10
5
00 1 2 3 4 5 6
Pati
ents
wit
h ev
ents
(%
)
Years
Standard therapy
Intensive therapy
Kaplan-Meier Curves for Primary Outcome*
Number at risk
Intensive therapy
Standard therapy
5128
5123
4843
4827
4390
4262
2839
2702
1337
1186
475
440
448
395
*Primary outcome was the first occurrence of nonfatal myocardial infarction or nonfatal stroke or death from cardiovascular causes.Action to Control Cardiovascular Risk in Diabetes Study Group. N Engl J Med. 2008;358:2545-2559.
Summary• Goal of antihypertensive and antidiabetic therapy is to
reduce end-organ damage• Diabetes is a risk factor for ischemic stroke; effective
blood pressure control can reduce incidence of stroke in patients with diabetes
• Microalbuminuria and macroalbuminuria are markers for diabetic nephropathy and cardiovascular risk
• Using ACE inhibitors/ARBs to lower blood pressure in patients with diabetes can slow progression of diabetic nephropathy and can improve clinical outcomes