the mechanical and biological properties of an injectable calcium phosphate cement-fibrin glue...
TRANSCRIPT

The Mechanical and Biological Properties of an InjectableCalcium Phosphate Cement-Fibrin Glue Composite forBone Regeneration
Geng Cui,1 Jie Li,2 Wei Lei,3 Long Bi,3 Peifu Tang,1 Yutian Liang,1 Sheng Tao,1 Yan Wang1
1 Institute of Orthopedics, General Hospital of PLA, Beijing 100853, People’s Republic of China
2 Department of Gynecology and Obstetrics, General Hospital of PLA, Beijing 100853, People’s Republic of China
3 Institute of Orthopaedics and Traumatology, Xijing Hospital, The Fourth Military Medical University, Xi’an 710032,People’s Republic of China
Received 24 March 2009; revised 2 July 2009; accepted 1 August 2009Published online 10 November 2009 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/jbm.b.31525
Abstract: Calcium phosphate cement (CPC) that can be injected to form a scaffold in situ
has promise for the repair of bone defects. However, its low-strength limits the CPC to non-
stress-bearing repairs. Fibrin glue (FG) with good sticking property and biocompatibility is
possible used to reinforce the CPC. The objective of this study was to investigate the effects of
FG on the mechanical and biological properties of CPC in an injectable CPC-FG composite.
The initial setting time of this CPC-FG was delayed compared with the CPC control at
different powder/liquid (P/L) mass ratio (p > 0.05). At a P/L of 5, the strength was (38.41 64.32) MPa for the CPC-FG, much higher than (27.42 6 2.85) MPa for the CPC alone (p <0.05). SEM showed bone marrow stromal cells (BMSCs) with healthy spreading and anchored
on the CPC-FG composite. After 14 days, the alkaline phosphatase (ALP) activity was (538 633) for the BMSCs on the CPC-FG and (517 6 27) for the BMSCs on the CPC alone. Both
ALPs were higher than the baseline ALP (93 6 10) for the undifferentiated BMSCs (p < 0.05).
The results demonstrate that this stronger CPC-FG scaffold may be useful for stem cell-based
bone regeneration in moderate load-bearing orthopedic applications. ' 2009 Wiley Periodicals,
Inc. J Biomed Mater Res Part B: Appl Biomater 92B: 377–385, 2010
Keywords: calcium phosphate(s); fibrin; biomechanics; cell proliferation; cell differentiation
INTRODUCTION
Treatments of osseous defects, delayed healing, and nonun-
ion, for example, from trauma, infection or tumor, remain
major problems in orthopedic surgery.1–3 Autografts and
allografts represent the current strategies for surgical inter-
vention and subsequent bone repair, but each possesses
limitations, such as donor-site morbidity with the use of
autografts and the risk of disease transmission with the use
of allografts.2–4 Tissue engineering is a promising approach
for the repair and regeneration of defective or damaged tis-
sues and organs. The basic principles involved in tissue-
engineered bone are the isolation and cultivation of cells,
the use of osteoinducing substances or growth factors, and
the placement of cells within suitable matrices or on scaf-
folds to support their growth.5 Two different types of scaf-
folds are used in tissue engineering for growth factor
delivery and cell adhesion, namely scaffolds made from
solid, prefabricated materials and scaffolds made from
materials that are injectable and hardened in situ.6
Injectable materials hold promise for tissue engineering
applications because they offer some advantages over solid
materials for certain indications. Injectable materials elimi-
nate the need for surgical intervention for their delivery,
and the minimally invasive procedure of injection reduces
discomfort and complications for the patient.7 Moreover,
injectable materials are able to take the shape of the cavity
into which they are placed and can thus fill irregular
defects. Also, problems with cell adhesion and growth fac-
tor delivery are overcome because, under the proper condi-
tions, the materials can be easily incorporated into the
solution by mixing prior to the injection.7,8 Candidates for
injectable materials include natural polymers, synthetic
polymers, and inorganic materials.6 Because of their simi-
larity to human bone, inorganic materials such as calcium
Correspondence to: Y. Wang (e-mail: [email protected])
' 2009 Wiley Periodicals, Inc.
377

phosphate ceramics and cements were, and still are, popu-
lar implant materials for diverse clinical applications.9–11
Different types of Ca-P ceramics are available and can be
classified as hydroxyapatite (HA), beta-tricalcium phos-
phate (b-TCP), or biphasic calcium phosphate (BCP).9
However, because they are made from sintered Ca-P
ceramics, they cannot be injected and must be shaped to
the defect site during operation, which makes the process
very labor intensive. A less than optimal tissue-to-implant
contact is often obtained. Because of the low-processing
temperature, calcium phosphate cements (CPCs), do not
comply with the original definition of calcium phosphate
ceramics, although the powder phase predominantly con-
tains TTCP with minor amounts of a-tricalcium phosphate
and HA.12,13 The main difference between cements and
ceramics is the injectability and in situ hardening of the
cement, which makes it easy to handle from a clinical point
of view.13,14 CPCs are obtained by mixing one or several
reactive calcium phosphate powders with an aqueous solu-
tion to form a paste that hardens within a restricted period
of time (e.g., 15 min). Two main approaches can be used
to make a CPC via an acid–base reaction or via a conver-
sion reaction of a metastable compound, either a-tricalcium
phosphate or a so-called amorphous calcium phosphate.13
However, due to its brittleness and weakness, the use of
CPC was limited to the reconstruction of non-stress-bearing
bone.15–17 Other injectable materials like chitosan, gelatin
and collagen are introduced to CPC to improve its mechan-
ical properties.18–20 However, studies have seldom been
done on the composite of CPC incorporated with fibrin
glue (FG) and its properties.21 FG is another type of inject-
able biomaterial approved by the Chinese State Food and
Drug Administration (SFDA) and is widely used in surgery
for repairing tissue damage or blood vessel injury.22–24 The
formation of FG involves the formation of a covalent iso-
peptide bridge between Gln and Lys residues by the enzy-
matic action of the transglutaminase factor XIIIa.24 FG
contains high concentrations of fibrinogen, which can pro-
duce a dense fibrin clot with sufficient adhesive strength to
maintain a required configuration for tissue adhesion and
cell ingrowth.25,26 Both CPC and FG have shown great
properties for the proliferation and differentiation of cells;
thus, the incorporation of FG was expected to increase the
strength without decreasing the biocompatibility of CPC.
We presented an injectable composite by combined FG
with CPC for the repair of bone defects. The objectives of
this study were to investigate the mechanical and biological
properties of this CPC-FG composite. The hypotheses are
as follows: (1) FG can increase the strength of this CPC-
FG composite compared with CPC, with little influence on
its setting process; (2) bone marrow stromal cells (BMSCs)
derived from rabbit bone marrow will attach to this CPC-
FG scaffold with a high-proliferation rate; and (3) the
CPC-FG scaffold will support the osteogenic differentiation
of BMSCs, yielding an elevated expression of alkaline
phosphatase (ALP) and collagen I (Col I).
MATERIALS AND METHODS
Preparation of the CPC-FG Composite
Preparation of the CPC powder was done according to
Ref. 18. Briefly, TTCP was synthesized from a solid-state
reaction between equimolar amounts of DCPA and CaCO3,
which were mixed and heated at 15008C for 6 h in a fur-
nace. The heated mixture was quenched to room tempera-
ture, ground in a ball mill, and sieved to obtain TTCP
particles with sizes ranging from �1 to 80 lm, with a me-
dian of 17 lm. DCPA was ground for 24 h to obtain parti-
cle sizes ranging from about 0.4 to 3 lm, with a median of
1 lm. The TTCP and DCPA powders were then mixed in
a blender at a molar ratio of 1:1 to form the CPC powder.
A commercially available SFDA-approved FG (Hualan
Biological Engineering, China) was used. The CPC powder
and FG solution were mixed at three different powder/liq-
uid mass ratios (P/L) (g/mL): 5/1, 3, and 1 in sterile injec-
tion syringes. Each CPC-FG paste was immediately
injected into a circular mold of 10-mm diameter and 2-mm
thickness to make disks for the setting time and cell studies
and a circular mold of 10-mm diameter and 20-mm high to
make cylinders for mechanical testing. Each specimen was
set in a humidor with 100% relative humidity at 378C for
4 h and then demolded and immersed in distilled water
378C for 20 h. The SFDA-approved CPC (Shanghai
Rebone, China) made using the same CPC powder but
using water as the liquid without the FG, was also fabri-
cated to serve as a control.
Setting Time with Gillmore Needles
Gillmore needles standard27 was used to compare the set-
ting time of the CPC-FG with that of the CPC (n 5 5).
Briefly, after the CPC-FG and CPC of different P/L ratios
were made in moulds (according to M&M 2.1), needles
were used to scrub the paste gently according to the refer-
ence. The initial setting time is defined as the time when a
0.3 MPa static pressure does not leave a visible print on
the surface of the cement. The final setting time is the cor-
responding time for a static pressure of 5 MPa. Each speci-
men was set with 100% relative humidity at 378C.
Mechanical Testing
The entire specimens were cylinders of 10-mm diameter
and 20-mm height (n 5 5). The mechanical testing was
performed after the specimens were left at room tempera-
ture for 24 h. The mechanical properties of the specimens
were analyzed in a materials testing machine (MTS-858,
MTS System, USA) by compression in the cranial-caudal
direction at a deformation rate of 5 mm/min until failure.
The compressive strength was calculated by S 5 Fmax/A,where Fmax is the maximum load on the load-deformation
curve and A is the cross-sectional area of each specimen.
The elastic modulus was calculated by E 5 S/(L/H), where
378 GENG ET AL.
Journal of Biomedical Materials Research Part B: Applied Biomaterials

L is the load deformation value and H is the initial height
of the specimen.
BMSCs Culture on CPC and CPC-FG
The BMSCs were prepared as described previously.28
Briefly, BMSCs were obtained from the os longum of
female white New Zealand rabbits aged between 8 months
and 1 year. All animal procedures used in this study were
approved by our institutional animal care committee. The
cells were cultured at 378C in a humidified atmosphere of
5% CO2 in flasks containing Dulbecco’s modified Eagle’s
medium (DMEM; Gibco, USA), 10% fetal bovine serum
(FBS; HyClone, USA), and 1% penicillin/streptomycin.
The medium was changed every third day. Cell subcultures
of third passages were used in the experiments. Osteogenic
differentiation was induced by culturing the BMSCs in an
osteogenic medium (OM) consisting of DMEM supple-
mented with 10% FBS, 1028 M DEX, 1023 M b-glycerolphosphate, and 50 mg/mL L-ascorbic acid. Prior to the cell
culture, the CPC control and the CPC-FG disks were steri-
lized by gamma radiation at 25 KGy. The disks were rinsed
in Dulbecco’s phosphate buffered saline. Upon reaching
90% confluence, cells adhesive to the flasks were detached
with 0.25 wt % trypsin (Type XI; Sigma Chemical, USA)
in 0.1M PBS. A total of 5 3 104 cells were diluted into
2 mL of OM and added to each well of a 24-well plate.
Each of the wells contained a disk of either CPC-FG or
CPC control.
SEM Observation
After being cultured for days 3 and 7, the specimens were
removed from the plates and gently washed with PBS three
times. The specimens were then fixed with 3% glutaralde-
hyde in PBS for 24 h at 48C. After being thoroughly
washed with PBS, the specimens were dehydrated sequen-
tially in 30, 50, 70, 80, 90, 95, and 100% ethanol. The
specimens were dehydrated twice in each ethanol concen-
tration for 15 min each time. The specimens were freeze
dried, sputter coated with gold, and examined under a SEM
(S-3000N, Japan) operated at 20 kV.
BMSCs Proliferation Assay
The number of BMSCs in the scaffold was determined
after 1, 7, and 14 days of triplicate culturing. In brief, at
these predetermined times, five specimens of each group
were gently washed with PBS to remove unattached cells.
The adherent cells were removed from the specimens by
incubation for 5 min in 2 mL 0.25 wt % trypsin in 0.1MPBS. Then, the suspension was collected and centrifuged at
300 g for 10 min. The sediment cells were resuspended in
fresh medium. One drop of this cell suspension was com-
bined with an equal amount of 0.4% (w/v) trypan blue
(Sigma Chemical, USA) and counted using a hemocytome-
ter under phase-contrast light microscopy.
Type-I Collagen (Col I) Immunohistochemistry Staining
The expression of Col I in the BMSCs was determined at
14 days by the Avidin-biotin peroxidase complex (ABC)
method. Briefly, the BMSCs on each specimen were
detached with 0.25 wt % trypsin (in 0.1M PBS) at 378C for
10 min. Then the specimens were extracted, and the cells
were centrifuged. The deposit of cells were resuspended in
PBS containing 10% fetal calf serum and the suspended cells
were incubated on 10 mm 3 10 mm sterile glass slides in
OM until adherence. Then the OM was removed. After speci-
mens were fixed with acetone at 48C for 10 min, they were
incubated in a moist chamber at 308C for 2 h with a primary
antibody, monoclonal rabbit anti-rat Col I diluted in PBS
with 1% BSA to 1:800. A horseradish peroxidase-3,30-diami-
nobenzidine tetrahydrochloride (HRP-DAB) system kit
(R&D System, USA) was used, including a secondary anti-
body, ABC reagent, and DAB system. The cells were incu-
bated with biotinylated secondary antibodies (rat anti-rabbit)
at room temperature for 30 min and incubated with the ABC/
HRP for 30 min. The results were observed by light micros-
copy at high magnification. BMSCs cultured in OM without
any specimen were incubated on the sterile glass slides and
regarded as positive control. On the other hand, BMSCs cul-
tured without OM and specimen were incubated on the ster-
ile glass slides, and were regarded as negative control.
ALP Measurement
The ALP activity was determined at 7 and 14 days of cul-
turing according to Ref. 18. Briefly, the medium was
removed and at the predetermined time point, five speci-
mens of each group were transferred to a new well plate.
Then, 0.5 mL of Triton X-100 was added to each well. A
cell scraper was used to remove the BMSCs from the disk
surface. The disk and 0.5 mL of cell lysate were placed in
a 1.5 mL centrifuge tube. The samples were then processed
through two freeze–thaw cycles (2808C and room tempera-
ture, 45-min each) to rupture the cell membranes and
extract the proteins and DNA from the cells. A p-nitro-phenyl phosphate (pNPP) liquid substrate system (Nanjing
Jiancheng, China) was used to analyze the ALP concentra-
tion from the cells on each disk. Five milliliters of each
cell lysate solution was added to 195 lL of pNPP substrate
and incubated in the dark at room temperature for 1 min.
The absorbance was read using a plate reader (Molecular
Devices, USA) at 405 nm and normalized to the PicoGreen
assay.29 The DNA was quantified using the PicoGreen Kit
(Invitrogen, USA) following standard protocols. Briefly,
100 lL of each cell lysate solution was added to 100 lL of
PicoGreen reagent and incubated in the dark at room tem-
perature for 5 min. The absorbance was read at an excita-
tion/emission of 480–520 nm on the plate reader.
Statistical Analysis
Statistical analyses were performed using SPSS software,
version 12.0 (SPSS, USA). The data were presented as the
379CPC-FG COMPOSITE FOR BONE REGENERATION
Journal of Biomedical Materials Research Part B: Applied Biomaterials
mean 6 SD, and levels were compared by the nonparamet-
ric Mann–Whitney U test or Student’s t-test. P-values less
than 0.05 were considered significant.
RESULTS
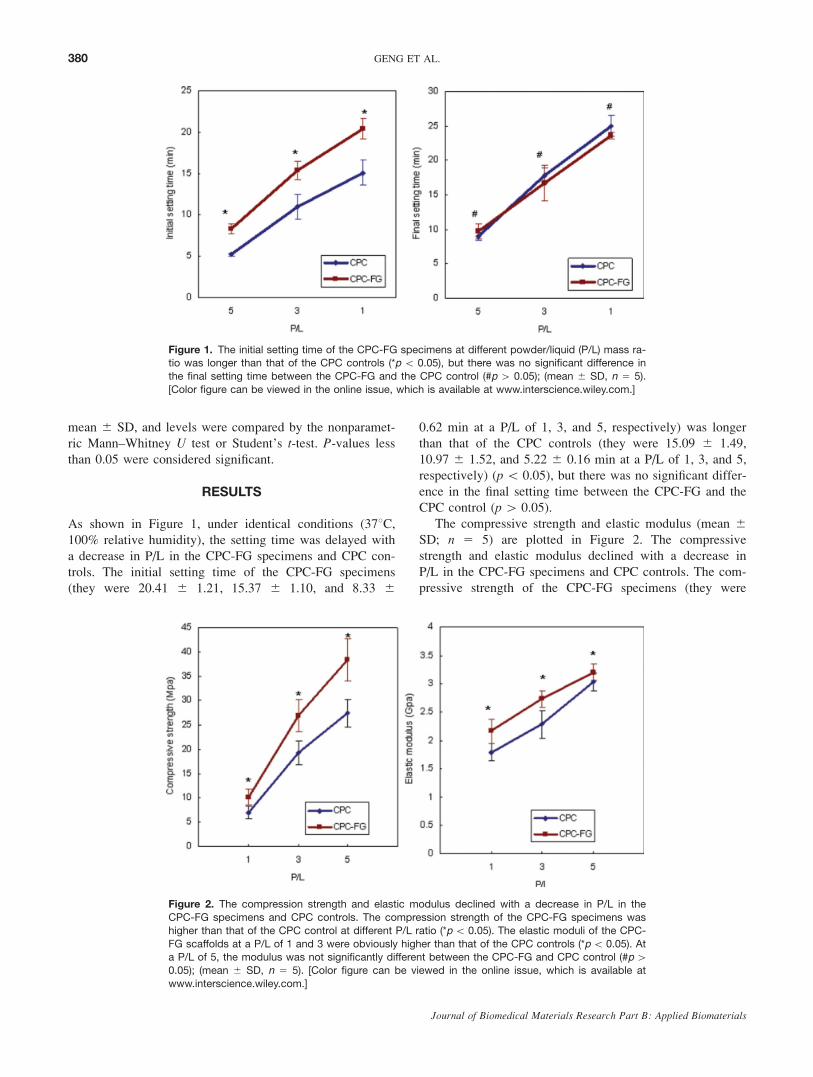
As shown in Figure 1, under identical conditions (378C,100% relative humidity), the setting time was delayed with
a decrease in P/L in the CPC-FG specimens and CPC con-
trols. The initial setting time of the CPC-FG specimens
(they were 20.41 6 1.21, 15.37 6 1.10, and 8.33 6
0.62 min at a P/L of 1, 3, and 5, respectively) was longer
than that of the CPC controls (they were 15.09 6 1.49,
10.97 6 1.52, and 5.22 6 0.16 min at a P/L of 1, 3, and 5,
respectively) (p\ 0.05), but there was no significant differ-
ence in the final setting time between the CPC-FG and the
CPC control (p[ 0.05).
The compressive strength and elastic modulus (mean 6SD; n 5 5) are plotted in Figure 2. The compressive
strength and elastic modulus declined with a decrease in
P/L in the CPC-FG specimens and CPC controls. The com-
pressive strength of the CPC-FG specimens (they were
Figure 1. The initial setting time of the CPC-FG specimens at different powder/liquid (P/L) mass ra-tio was longer than that of the CPC controls (*p \ 0.05), but there was no significant difference in
the final setting time between the CPC-FG and the CPC control (#p [ 0.05); (mean 6 SD, n 5 5).
[Color figure can be viewed in the online issue, which is available at www.interscience.wiley.com.]
Figure 2. The compression strength and elastic modulus declined with a decrease in P/L in the
CPC-FG specimens and CPC controls. The compression strength of the CPC-FG specimens was
higher than that of the CPC control at different P/L ratio (*p\ 0.05). The elastic moduli of the CPC-
FG scaffolds at a P/L of 1 and 3 were obviously higher than that of the CPC controls (*p\ 0.05). Ata P/L of 5, the modulus was not significantly different between the CPC-FG and CPC control (#p[0.05); (mean 6 SD, n 5 5). [Color figure can be viewed in the online issue, which is available at
www.interscience.wiley.com.]
380 GENG ET AL.
Journal of Biomedical Materials Research Part B: Applied Biomaterials
10.15 6 1.59, 26.93 6 3.26, and 38.41 6 4.32 MPa at a
P/L of 1, 3, and 5, respectively) was higher than that of the
CPC control (they were 7.00 6 1.33, 19.32 6 2.40, and
27.42 6 2.85 MPa at a P/L of 1, 3, and 5, respectively) (p\ 0.05). The elastic moduli of the CPC-FG scaffolds at a
P/L of 1, 3, and 5 (2.16 6 0.16, 2.73 6 0.24, and 3.20 60.16 GPa) were higher than that of the CPC controls (1.79
6 0.21, 2.28 6 0.14, and 3.03 6 0.14 GPa) (p\ 0.05).
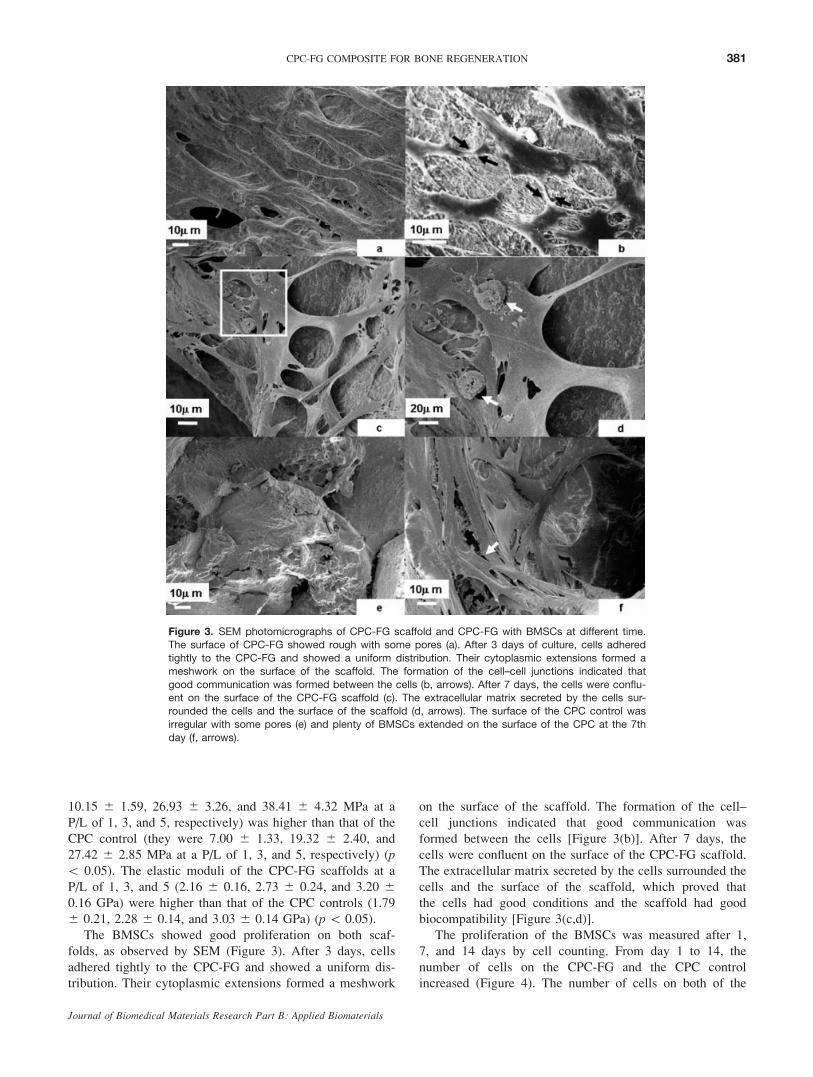
The BMSCs showed good proliferation on both scaf-
folds, as observed by SEM (Figure 3). After 3 days, cells
adhered tightly to the CPC-FG and showed a uniform dis-
tribution. Their cytoplasmic extensions formed a meshwork
on the surface of the scaffold. The formation of the cell–
cell junctions indicated that good communication was
formed between the cells [Figure 3(b)]. After 7 days, the
cells were confluent on the surface of the CPC-FG scaffold.
The extracellular matrix secreted by the cells surrounded the
cells and the surface of the scaffold, which proved that
the cells had good conditions and the scaffold had good
biocompatibility [Figure 3(c,d)].
The proliferation of the BMSCs was measured after 1,
7, and 14 days by cell counting. From day 1 to 14, the
number of cells on the CPC-FG and the CPC control
increased (Figure 4). The number of cells on both of the
Figure 3. SEM photomicrographs of CPC-FG scaffold and CPC-FG with BMSCs at different time.The surface of CPC-FG showed rough with some pores (a). After 3 days of culture, cells adhered
tightly to the CPC-FG and showed a uniform distribution. Their cytoplasmic extensions formed a
meshwork on the surface of the scaffold. The formation of the cell–cell junctions indicated that
good communication was formed between the cells (b, arrows). After 7 days, the cells were conflu-ent on the surface of the CPC-FG scaffold (c). The extracellular matrix secreted by the cells sur-
rounded the cells and the surface of the scaffold (d, arrows). The surface of the CPC control was
irregular with some pores (e) and plenty of BMSCs extended on the surface of the CPC at the 7th
day (f, arrows).
381CPC-FG COMPOSITE FOR BONE REGENERATION
Journal of Biomedical Materials Research Part B: Applied Biomaterials
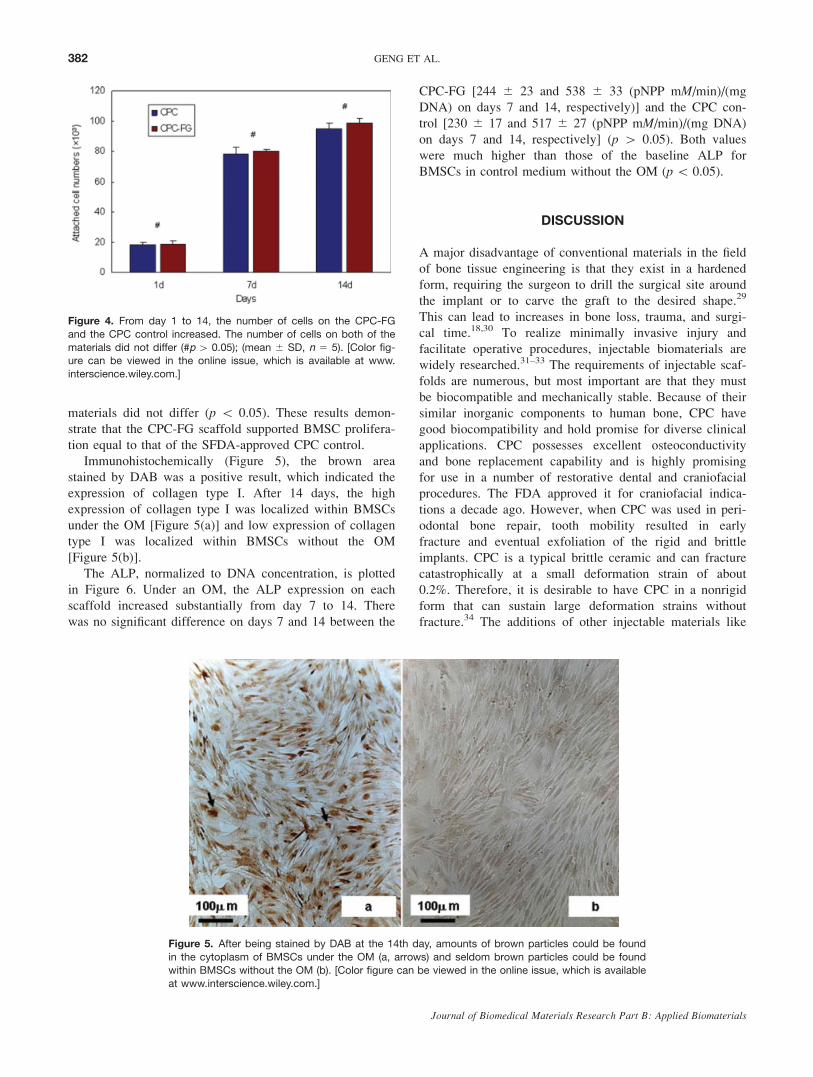
materials did not differ (p \ 0.05). These results demon-
strate that the CPC-FG scaffold supported BMSC prolifera-
tion equal to that of the SFDA-approved CPC control.
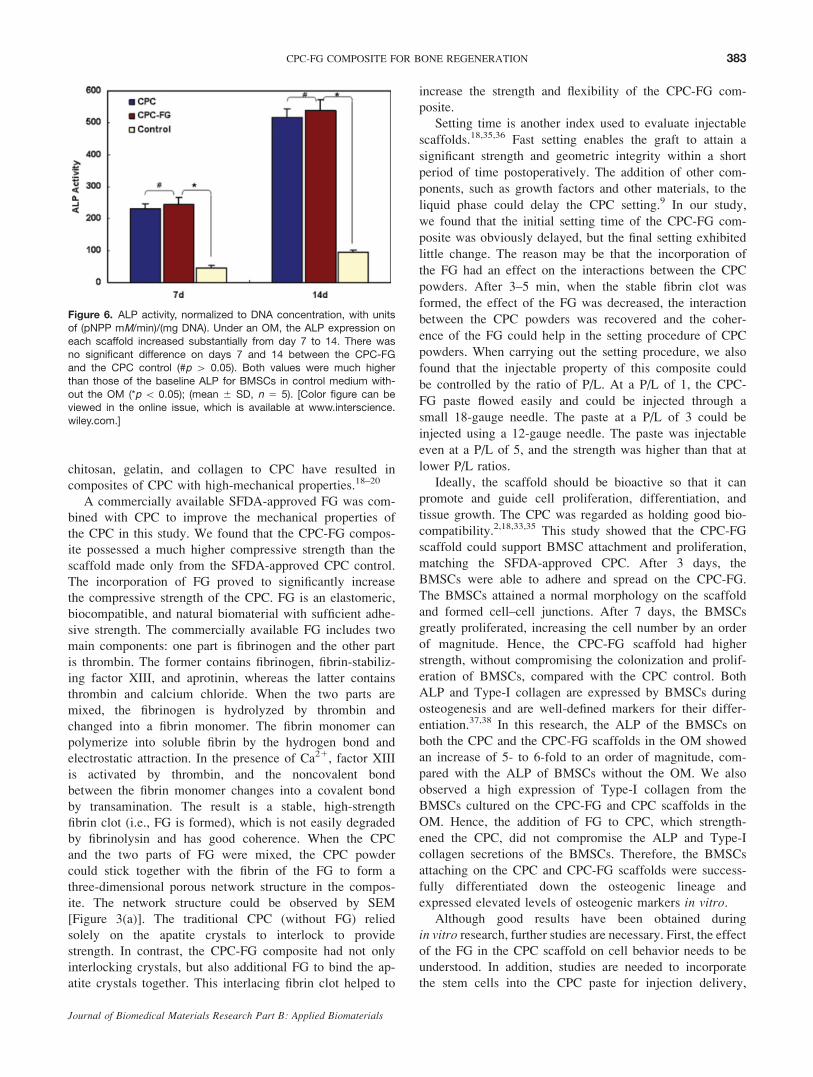
Immunohistochemically (Figure 5), the brown area
stained by DAB was a positive result, which indicated the
expression of collagen type I. After 14 days, the high
expression of collagen type I was localized within BMSCs
under the OM [Figure 5(a)] and low expression of collagen
type I was localized within BMSCs without the OM
[Figure 5(b)].
The ALP, normalized to DNA concentration, is plotted
in Figure 6. Under an OM, the ALP expression on each
scaffold increased substantially from day 7 to 14. There
was no significant difference on days 7 and 14 between the
CPC-FG [244 6 23 and 538 6 33 (pNPP mM/min)/(mg
DNA) on days 7 and 14, respectively)] and the CPC con-
trol [230 6 17 and 517 6 27 (pNPP mM/min)/(mg DNA)
on days 7 and 14, respectively] (p [ 0.05). Both values
were much higher than those of the baseline ALP for
BMSCs in control medium without the OM (p\ 0.05).
DISCUSSION
A major disadvantage of conventional materials in the field
of bone tissue engineering is that they exist in a hardened
form, requiring the surgeon to drill the surgical site around
the implant or to carve the graft to the desired shape.29
This can lead to increases in bone loss, trauma, and surgi-
cal time.18,30 To realize minimally invasive injury and
facilitate operative procedures, injectable biomaterials are
widely researched.31–33 The requirements of injectable scaf-
folds are numerous, but most important are that they must
be biocompatible and mechanically stable. Because of their
similar inorganic components to human bone, CPC have
good biocompatibility and hold promise for diverse clinical
applications. CPC possesses excellent osteoconductivity
and bone replacement capability and is highly promising
for use in a number of restorative dental and craniofacial
procedures. The FDA approved it for craniofacial indica-
tions a decade ago. However, when CPC was used in peri-
odontal bone repair, tooth mobility resulted in early
fracture and eventual exfoliation of the rigid and brittle
implants. CPC is a typical brittle ceramic and can fracture
catastrophically at a small deformation strain of about
0.2%. Therefore, it is desirable to have CPC in a nonrigid
form that can sustain large deformation strains without
fracture.34 The additions of other injectable materials like
Figure 4. From day 1 to 14, the number of cells on the CPC-FG
and the CPC control increased. The number of cells on both of the
materials did not differ (#p [ 0.05); (mean 6 SD, n 5 5). [Color fig-ure can be viewed in the online issue, which is available at www.
interscience.wiley.com.]
Figure 5. After being stained by DAB at the 14th day, amounts of brown particles could be found
in the cytoplasm of BMSCs under the OM (a, arrows) and seldom brown particles could be found
within BMSCs without the OM (b). [Color figure can be viewed in the online issue, which is available
at www.interscience.wiley.com.]
382 GENG ET AL.
Journal of Biomedical Materials Research Part B: Applied Biomaterials
chitosan, gelatin, and collagen to CPC have resulted in
composites of CPC with high-mechanical properties.18–20
A commercially available SFDA-approved FG was com-
bined with CPC to improve the mechanical properties of
the CPC in this study. We found that the CPC-FG compos-
ite possessed a much higher compressive strength than the
scaffold made only from the SFDA-approved CPC control.
The incorporation of FG proved to significantly increase
the compressive strength of the CPC. FG is an elastomeric,
biocompatible, and natural biomaterial with sufficient adhe-
sive strength. The commercially available FG includes two
main components: one part is fibrinogen and the other part
is thrombin. The former contains fibrinogen, fibrin-stabiliz-
ing factor XIII, and aprotinin, whereas the latter contains
thrombin and calcium chloride. When the two parts are
mixed, the fibrinogen is hydrolyzed by thrombin and
changed into a fibrin monomer. The fibrin monomer can
polymerize into soluble fibrin by the hydrogen bond and
electrostatic attraction. In the presence of Ca21, factor XIII
is activated by thrombin, and the noncovalent bond
between the fibrin monomer changes into a covalent bond
by transamination. The result is a stable, high-strength
fibrin clot (i.e., FG is formed), which is not easily degraded
by fibrinolysin and has good coherence. When the CPC
and the two parts of FG were mixed, the CPC powder
could stick together with the fibrin of the FG to form a
three-dimensional porous network structure in the compos-
ite. The network structure could be observed by SEM
[Figure 3(a)]. The traditional CPC (without FG) relied
solely on the apatite crystals to interlock to provide
strength. In contrast, the CPC-FG composite had not only
interlocking crystals, but also additional FG to bind the ap-
atite crystals together. This interlacing fibrin clot helped to
increase the strength and flexibility of the CPC-FG com-
posite.
Setting time is another index used to evaluate injectable
scaffolds.18,35,36 Fast setting enables the graft to attain a
significant strength and geometric integrity within a short
period of time postoperatively. The addition of other com-
ponents, such as growth factors and other materials, to the
liquid phase could delay the CPC setting.9 In our study,
we found that the initial setting time of the CPC-FG com-
posite was obviously delayed, but the final setting exhibited
little change. The reason may be that the incorporation of
the FG had an effect on the interactions between the CPC
powders. After 3–5 min, when the stable fibrin clot was
formed, the effect of the FG was decreased, the interaction
between the CPC powders was recovered and the coher-
ence of the FG could help in the setting procedure of CPC
powders. When carrying out the setting procedure, we also
found that the injectable property of this composite could
be controlled by the ratio of P/L. At a P/L of 1, the CPC-
FG paste flowed easily and could be injected through a
small 18-gauge needle. The paste at a P/L of 3 could be
injected using a 12-gauge needle. The paste was injectable
even at a P/L of 5, and the strength was higher than that at
lower P/L ratios.
Ideally, the scaffold should be bioactive so that it can
promote and guide cell proliferation, differentiation, and
tissue growth. The CPC was regarded as holding good bio-
compatibility.2,18,33,35 This study showed that the CPC-FG
scaffold could support BMSC attachment and proliferation,
matching the SFDA-approved CPC. After 3 days, the
BMSCs were able to adhere and spread on the CPC-FG.
The BMSCs attained a normal morphology on the scaffold
and formed cell–cell junctions. After 7 days, the BMSCs
greatly proliferated, increasing the cell number by an order
of magnitude. Hence, the CPC-FG scaffold had higher
strength, without compromising the colonization and prolif-
eration of BMSCs, compared with the CPC control. Both
ALP and Type-I collagen are expressed by BMSCs during
osteogenesis and are well-defined markers for their differ-
entiation.37,38 In this research, the ALP of the BMSCs on
both the CPC and the CPC-FG scaffolds in the OM showed
an increase of 5- to 6-fold to an order of magnitude, com-
pared with the ALP of BMSCs without the OM. We also
observed a high expression of Type-I collagen from the
BMSCs cultured on the CPC-FG and CPC scaffolds in the
OM. Hence, the addition of FG to CPC, which strength-
ened the CPC, did not compromise the ALP and Type-I
collagen secretions of the BMSCs. Therefore, the BMSCs
attaching on the CPC and CPC-FG scaffolds were success-
fully differentiated down the osteogenic lineage and
expressed elevated levels of osteogenic markers in vitro.Although good results have been obtained during
in vitro research, further studies are necessary. First, the effectof the FG in the CPC scaffold on cell behavior needs to be
understood. In addition, studies are needed to incorporate
the stem cells into the CPC paste for injection delivery,
Figure 6. ALP activity, normalized to DNA concentration, with units
of (pNPP mM/min)/(mg DNA). Under an OM, the ALP expression on
each scaffold increased substantially from day 7 to 14. There wasno significant difference on days 7 and 14 between the CPC-FG
and the CPC control (#p [ 0.05). Both values were much higher
than those of the baseline ALP for BMSCs in control medium with-
out the OM (*p \ 0.05); (mean 6 SD, n 5 5). [Color figure can beviewed in the online issue, which is available at www.interscience.
wiley.com.]
383CPC-FG COMPOSITE FOR BONE REGENERATION
Journal of Biomedical Materials Research Part B: Applied Biomaterials
instead of seeding the cells on the surface of a prehardened
CPC. Furthermore, because the in vitro cell culture is a
closed static system and differs from the dynamic circula-
tion in vivo, animal studies are needed to investigate the
bone regeneration efficacy of the CPC-FG-stem cell
construct.
CONCLUSIONS
The CPC-FG scaffold possessed compressive strength
higher than the CPC control. The CPC-FG composite sup-
ported BMSC attachment and proliferation. Although the
initial setting time of the CPC-FG composite was obviously
delayed compared with the CPC control, the final setting
time had little change. The expression of ALP and Type-I
collagen of the BMSCs in this CPC-FG in the OM was
also increased compared with the BMSCs in control me-
dium without osteogenic factors. Therefore, the addition of
FG to CPC, which strengthened the CPC, did not compro-
mise the proliferation and differentiation of BMSCs.
Hence, the CPC-FG scaffold may have potential for BMSC
delivery and bone regeneration in moderate stress-bearing
orthopedic applications.
REFERENCES
1. Schmidmaier G, Schwabe P, Wildemann B, Haas NP. Use ofbone morphogenetic proteins for treatment of non-unions andfuture perspectives. Injury 2007;38 (Suppl 4):S35–S41.
2. Khan Y, Yaszemski MJ, Mikos AG, Laurencin CT. Tissue en-gineering of bone: Material and matrix considerations. J BoneJoint Surg Am 2008;90 (Suppl 1):36–42.
3. Bishop GB, Einhorn TA. Current and future clinical applica-tions of bone morphogenetic proteins in orthopaedic traumasurgery. Int Orthop 2007;31:721–727.
4. Liu G, Zhao L, Zhang W, Cui L, Liu W, Cao Y. Repair ofgoat tibial defects with bone marrow stromal cells and beta-tricalcium phosphate. J Mater Sci Mater Med 2008;19:2367–2376.
5. Langer R, Vacanti JP. Tissue engineering. Science 1993;260:920–926.
6. Tessmar JK, Gopferich AM. Matrices and scaffolds forprotein delivery in tissue engineering. Adv Drug Deliv Rev2007;59:274–291.
7. Kretlow JD, Klouda L, Mikos AG. Injectable matrices andscaffolds for drug delivery in tissue engineering. Adv DrugDeliv Rev 2007;59:263–273.
8. Jayabalan M, Shalumon KT, Mitha MK. Injectable biomateri-als for minimally invasive orthopedic treatments. J Mater SciMater Med 2009;20:1379–1387.
9. Habraken WJ, Wolke JG, Jansen JA. Ceramic composites asmatrices and scaffolds for drug delivery in tissue engineering.Adv Drug Deliv Rev 2007;59:234–248.
10. Habibovic P, Kruyt MC, Juhl MV, Clyens S, Martinetti R,Dolcini L, Theilgaard N, van Blitterswijk CA. Comparative invivo study of six hydroxyapatite-based bone graft substitutes.J Orthop Res 2008;26:1363–1370.
11. Bajammal SS, Zlowodzki M, Lelwica A, Tornetta P III, Ein-horn TA, Buckley R, Leighton R, Russell TA, Larsson S,Bhandari M. The use of calcium phosphate bone cement infracture treatment. A meta-analysis of randomized trials.J Bone Joint Surg Am 2008;90:1186–1196.
12. Takagi S, Chow LC, Markovic M, Friedman CD, CostantinoPD. Morphological and phase characterizations of retrievedcalcium phosphate cement implants. J Biomed Mater Res2001;58:36–41.
13. Bohner M, Gbureck U, Barralet JE. Technological issues forthe development of more efficient calcium phosphate bonecements: A critical assessment. Biomaterials 2005;26:6423–6429.
14. Jansen J, Ooms E, Verdonschot N, Wolke J. Injectable cal-cium phosphate cement for bone repair and implant fixation.Orthop Clin North Am 2005;36:89–95.
15. Shindo ML, Costantino PD, Friedman CD, Chow LC. Facialskeletal augmentation using hydroxyapatite cement. Arch Oto-laryngol Head Neck Surg 1993;119:185–190.
16. Friedman CD, Costantino PD, Takagi S, Chow LC. Bonesource hydroxyapatite cement: A novel biomaterial for cranio-facial skeletal tissue engineering and reconstruction. J BiomedMater Res 1998;43:428–432.
17. Xu HH, Quinn JB, Takagi S, Chow LC, Eichmiller FC.Strong and macroporous calcium phosphate cement: Effectsof porosity and fiber reinforcement on mechanical properties.J Biomed Mater Res 2001;57:457–466.
18. Moreau JL, Xu HH. Mesenchymal stem cell proliferation anddifferentiation on an injectable calcium phosphate-chitosancomposite scaffold. Biomaterials 2009;30:2675–2682.
19. Link DP, van den Dolder J, van den Beucken JJ, Wolke JG,Mikos AG, Jansen JA. Bone response and mechanicalstrength of rabbit femoral defects filled with injectable CaPcements containing TGF-b1 loaded gelatin microspheres. Bio-materials 2008;29:675–682.
20. Moreau JL, Weir MD, Xu HHK. Self-setting collagen-calciumphosphate bone cement: Mechanical and cellular properties.J Biomed Mater Res A 2008;91:605–613.
21. Hu YS, Fan QY, Ma BA, Zhou Y, Hu ZQ, Ye XX. Structuraland mechanical properties of the compound scaffold of cal-cium phosphate cement and fibrin glue. J Funct Mater2006;37:607–610.
22. Menovsky T, Bartels RH. Stabilization and accurate trimmingof nerve ends: Practical use of fibrin glue. Neurosurgery1999;44:224–225; discussion 225–226.
23. Findikcioglu K, Findikcioglu F, Yavuzer R, Elmas C, AtabayK. Effect of platelet-rich plasma and fibrin glue on healing ofcritical-size calvarial bone defects. J Craniofac Surg 2009;20:34–40.
24. Weisel JW. Fibrinogen and fibrin. Adv Protein Chem 2005;70:247–299.
25. Ehrbar M, Rizzi SC, Schoenmakers RG, Miguel BS, HubbellJA, Weber FE, Lutolf MP. Biomolecular hydrogels formedand degraded via site-specific enzymatic reactions. Biomacro-molecules 2007;8:3000–3007.
26. Zhu SJ, Choi BH, Jung JH, Lee SH, Huh JY, You TM, LeeHJ, Li J. A comparative histologic analysis of tissue-engi-neered bone using platelet-rich plasma and platelet-enrichedfibrin glue. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2006;102:175–179.
27. Nilsson M, Carlson J, Fernandez E, Planell JA. Monitoringthe setting of calcium-based bone cements using pulse-echoultrasound. J Mater Sci Mater Med 2002;13:1135–1141.
28. Kim H, Lee JH, Suh H. Interaction of mesenchymal stemcells and osteoblasts for in vitro osteogenesis. Yonsei Med J2003;44:187–197.
29. Laurencin CT, Ambrosio AM, Borden MD, Cooper JA, Jr.Tissue engineering: Orthopedic applications. Annu Rev BiomedEng 1999;1:19–46.
30. Betz MW, Modi PC, Caccamese JF, Coletti DP, Sauk JJ,Fisher JP. Cyclic acetal hydrogel system for bone marrowstromal cell encapsulation and osteodifferentiation. J BiomedMater Res A 2008;86:662–670.
384 GENG ET AL.
Journal of Biomedical Materials Research Part B: Applied Biomaterials

31. Arnold JC, Venditti NP. Prediction of the long-term creepbehaviour of hydroxyapatite-filled polyethylmethacrylate bonecements. J Mater Sci Mater Med 2007;18:1849–1858.
32. Xu HH, Burguera EF, Carey LE. Strong, macroporous, and insitu-setting calcium phosphate cement-layered structures. Bio-materials 2007;28:3786–3796.
33. del Valle S, Mino N, Munoz F, Gonzalez A, Planell JA,Ginebra MP. In vivo evaluation of an injectable macroporouscalcium phosphate cement. J Mater Sci Mater Med 2007;18:353–361.
34. Xu HH, Takagi S, Sun L, Hussain L, Chow LC, Guthrie WF,Yen JH. Development of a nonrigid, durable calcium phos-phate cement for use in periodontal bone repair. J Am DentAssoc 2006;137:1131–1138.
35. Weir MD, Xu HH. High-strength, in situ-setting calciumphosphate composite with protein release. J Biomed MaterRes A 2008;85:388–396.
36. Sun L, Xu HH, Takagi S, Chow LC. Fast setting calciumphosphate cement-chitosan composite: Mechanical propertiesand dissolution rates. J Biomater Appl 2007;21:299–315.
37. Guo L, Kawazoe N, Hoshiba T, Tateishi T, Chen G, ZhangX. Osteogenic differentiation of human mesenchymal stemcells on chargeable polymer-modified surfaces. J Biomed MaterRes A 2008;87:903–912.
38. Wang H, Li Y, Zuo Y, Li J, Ma S, Cheng L. Biocompatibilityand osteogenesis of biomimetic nano-hydroxyapatite/polyam-ide composite scaffolds for bone tissue engineering. Biomate-rials 2007;28:3338–3348.
385CPC-FG COMPOSITE FOR BONE REGENERATION
Journal of Biomedical Materials Research Part B: Applied Biomaterials