the magnitude, persistence and public health significance of cognitive effects of environmental lead...
TRANSCRIPT

JOURNAL OF ENVIRONMENTAL MEDICINEORIGINAL ARTICLE J. Environ. Med.1: 103–110 (1999)
The Magnitude, Persistence and Public HealthSignificance of Cognitive Effects of Environmental LeadExposure in Childhood
Shilu Tong,1* Anthony J. McMichael2
1Centre for Public Health Research, Queensland University of Technology, Kelvin Grove, Qld. 4059, Australia2Department of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, LondonWC1E 7HT, UK
KEY WORDS Although much research has been done on the effects of lead exposure on cogni-tive development, the magnitude, persistence and public health implications ofsuch effects remain controversial. A literature search, in conjunction with ourown work, was conducted to review these issues. Currently available evidencesuggests that early exposure to environmental lead may cause a discernibleeffect on cognitive development, and this effect seems to persist into later child-hood. No threshold is evident down to a blood lead concentration of 5 mg dl21,although there is a paucity of epidemiological data at these lower levels. Aneconomic loss could be serious for children exposed to an excess of lead in theirenvironment. The environmental lead problem is preventable, or, where it isalready established, is remediable. It should therefore be addressed, especiallyin developing countries where rapid industrialisation and increased use of motorvehicles are occurring. There is clear evidence that excessive lead exposure isstill a significant public health issue in most countries, particularly developingcountries. The formulation of a public health strategy should seek a balancebetween consideration of the nature and extent of the risk to human populationhealth, knowledge of any dose-effect threshold, estimation of socio-environ-mental benefits, and commitment to making the best use of existing resources.The development of such a strategy should take into account the views andpriorities of all interested parties, and—most certainly—those of communitiesdirectly at risk from lead exposure.Copyright 1999 John Wiley & Sons, Ltd.
Introduction
Lead is the most abundant of the heavy metals on earth,and its crustal abundance varies from 7 to 20 parts permillion in different areas.1 The use of lead since prehistorictimes, and its massive mobilisation into the environment,has resulted in increased exposure to this heavy metal byhumans.2 Lead is a well-known toxin. It can cause adverseeffects on various organ systems, most importantly the cen-tral nervous system, kidneys and blood.3–5 Although thehealth effects of exposure to high levels of lead have longbeen recognised, there has been a debate over the nature,
*Correspondence to: Dr S. Tong, Centre for Public Health Research,Queensland University of Technology, Kelvin Grove, Qld, 4059AustraliaE-mail: s.tongKqut.edu.au
CCC/0885–6087/99/020103–08$17.50 Received 6 April 1999Copyright 1999 John Wiley & Sons, Ltd. Accepted 4 June 1999
magnitude and persistence of the adverse effects on humanhealth of low-level exposure to lead.
The accumulated epidemiological evidence indicatesthat low-level exposure to lead in early childhoodcauses a deficit in cognitive development during theimmediately ensuing childhood years.6–9 However, thequantitative assessment of the risk of developmentalneurotoxicity due to low-level lead exposure is noteasy. In this paper, we discuss the following issues inrelation to that quantitative assessment task:
(1) Lead contamination of the global environment(2) Magnitude of the effect of early-life low-level lead
exposure upon cognition(3) Reversibility of the lead effect(4) Threshold of lead exposure below which there is
no neurotoxicological effect(5) Public health implications of the effects of lead
upon cognitive development
104 S. TONG AND A.J. McMICHAEL
Although these questions have received some attentionin the scientific community, they have not been wellanswered yet.
Lead Contamination of GlobalEnvironment
Lead may have been the first metal to have beensmelted by human beings. Lead beads have been found,together with gold and copper ornaments, in Anatoliadating from 7000 to 6500 BC. Lead has been found ina sixth millennium BC setting at Yarum Tepe in Iraq,at the fifth millennium BC site of Arpachiyeh in Iraqand at the fourth millennium BC sites of Anau I inTurkestan, Hissar III in Iraq and Naqada in Egypt.10–
12 These findings suggest that lead smelting, albeit ona small scale, began as early as 8000 to 9000 yearsago.10,11References to lead in the Old Testament of theChristian Bible include the use of lead in the construc-tion of the Hanging Gardens of Babylon, and lead min-ing by the Phoenicians in Spain from about 2000BC.11,12 In China, lead metal, pigments, and lead glasswere known at least as early as the Chou Dynasty (5thcentury BC).13
The elemental symbol for lead, Pb, is from the latin‘plumbum’ from which the word ‘plumber’ isderived—a reference to the importance of lead inplumbing practice (until very recently). The alchemicalsymbol for lead was Saturn, because the medievalalchemists considered lead to be the father of metalsdue to the ease with which the nobler metals, such assilver and gold, dissolved in molten lead.10 Plumbismand Saturnism are both old medical names used forclinical lead poisoning.
The useful physical properties of elemental lead, i.e.its malleability, ductility, corrosion resistance and poorconductance, have resulted in a multiplicity of uses ofthe metal for over a thousand years. The ancient civiliz-ations of Phoenicia, Egypt, Greece, China and India areknown to have smelted and used lead for vessels, roofs,water ducts, utensils, ornaments and weights. TheRomans used lead throughout their empire for the con-struction of aqueducts and cisterns. In Roman times,cooking utensils were made of lead and copper, andpewter was made of a lead–tin alloy.10,14 Although itsimportance initially lay in its close association with sil-ver, lead emerged from the background and assumeda dominant role in the technology of the developingRoman Empire. One reason for the Roman invasion ofBritain in the first century was to exploit the mines oflead (and other minerals) in England in order to satisfythe Roman enthusiasm for sanitation and bathing.11,14
Following the fall of the Roman Empire in the fourthcentury, the use of lead diminished considerably andwas mainly confined to products such as sheeting, tub-ing, vessels, glazes, pigments and alloys until theIndustrial Revolution.12,15 There was a great upsurge
Copyright 1999 John Wiley & Sons, Ltd. J. Environ. Med.1: 103–110 (1999)
in the use of lead during the period of the IndustrialRevolution. The advent of mass industrialization and,in particular, the motor vehicle, brought about dramaticincreases in lead usage: as a component of the lead-acid storage battery and (from 1922) as the ‘anti-knock’additive (tetraethyl-and tetra-methyl lead) in gasoline.Even today, lead is still the most widely used nonfer-rous metal.12,15,16
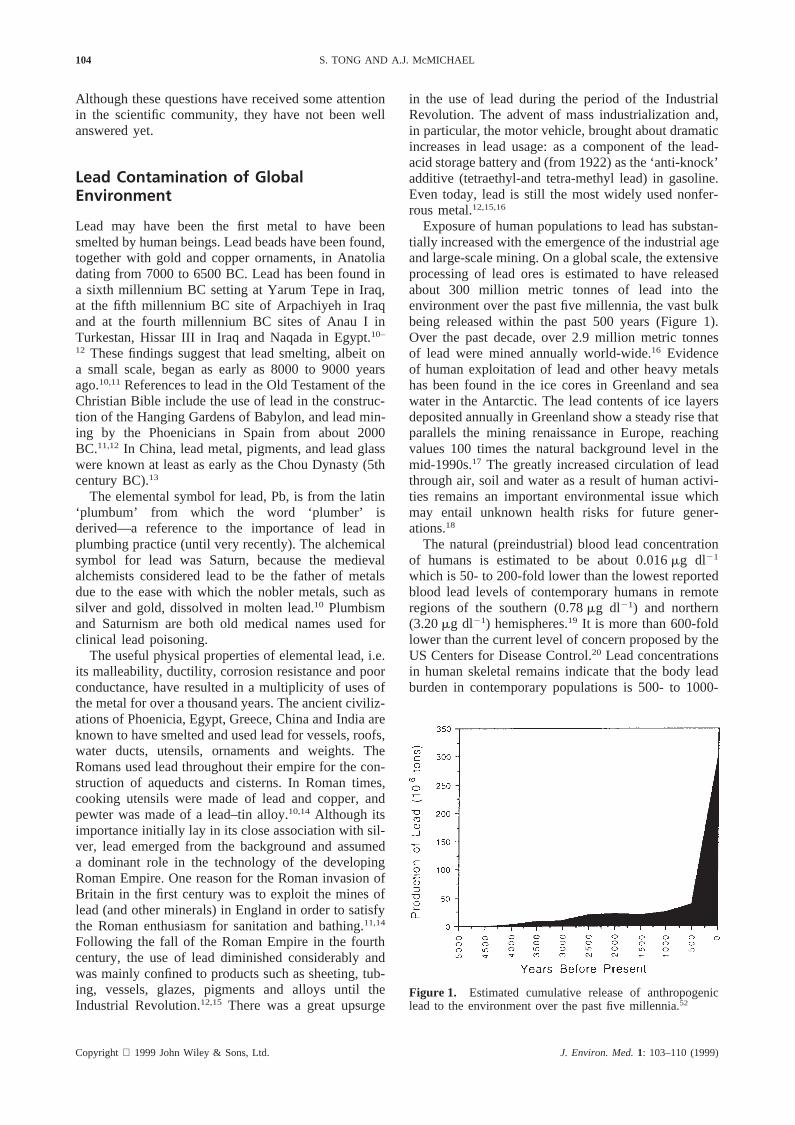
Exposure of human populations to lead has substan-tially increased with the emergence of the industrial ageand large-scale mining. On a global scale, the extensiveprocessing of lead ores is estimated to have releasedabout 300 million metric tonnes of lead into theenvironment over the past five millennia, the vast bulkbeing released within the past 500 years (Figure 1).Over the past decade, over 2.9 million metric tonnesof lead were mined annually world-wide.16 Evidenceof human exploitation of lead and other heavy metalshas been found in the ice cores in Greenland and seawater in the Antarctic. The lead contents of ice layersdeposited annually in Greenland show a steady rise thatparallels the mining renaissance in Europe, reachingvalues 100 times the natural background level in themid-1990s.17 The greatly increased circulation of leadthrough air, soil and water as a result of human activi-ties remains an important environmental issue whichmay entail unknown health risks for future gener-ations.18
The natural (preindustrial) blood lead concentrationof humans is estimated to be about 0.016mg dl21
which is 50- to 200-fold lower than the lowest reportedblood lead levels of contemporary humans in remoteregions of the southern (0.78mg dl21) and northern(3.20mg dl21) hemispheres.19 It is more than 600-foldlower than the current level of concern proposed by theUS Centers for Disease Control.20 Lead concentrationsin human skeletal remains indicate that the body leadburden in contemporary populations is 500- to 1000-
Figure 1. Estimated cumulative release of anthropogeniclead to the environment over the past five millennia.52
105RISK ASSESSMENT OF LEAD EXPOSURE
fold greater than that in their preindustrial counter-parts.21,22Since the most substantial evidence from epi-demiological studies of populations with blood leadlevels as low as 10–15mg dl21 relates to decrementsin intelligence quotient, many developed countries,including the United States and Australia, have recentlyset new, lower standards on environmental leadexposure.20,23 However, childhood lead poisoning—aphrase now widely used to refer to any adverse healthconsequences of lead exposure—is a growing publichealth problem in most developing countries. Forexample, the lead content of gasoline sold in Africa isthe highest in the world, with an estimated lead contentof 0.5–0.8 g l21 in most African countries. Averagelead concentrations reached 0.5–3.0mg m23 in theatmosphere and.1000mg g21 in dust and soils. Inaddition to automotive and industrial sources, cottageindustries and the burning of paper products, discardedrubber, battery castings and painted woods for cookingand heating represent additional hazards to individualhouseholds. Childhood lead poisoning is a widespreadproblem in Africa.17,24 Recent data show that, forexample, over 90% of the children in the Cape Prov-ince, South Africa, had blood lead levels$ 10 mgdl21.17 Lead poisoning also prevails in many otherdeveloping countries. In Dhaka City, the lead concen-tration in airborne particulate matter is one of the high-est recorded in the world: it is 453 ng m23 during thelow rainfall season (November–January).25 The meanblood lead concentration in 93 randomly chosen rick-shaw-pullers was 53mg dl21,26 which is more than five
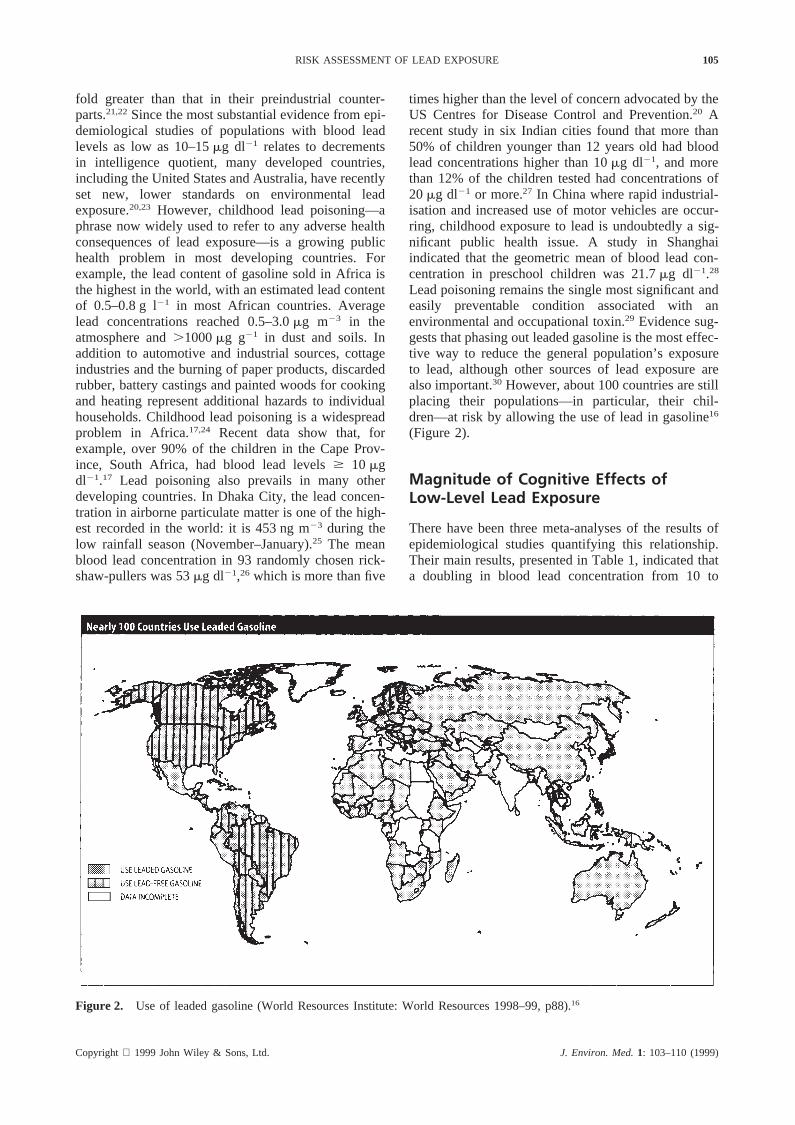
Figure 2. Use of leaded gasoline (World Resources Institute: World Resources 1998–99, p88).16
Copyright 1999 John Wiley & Sons, Ltd. J. Environ. Med.1: 103–110 (1999)
times higher than the level of concern advocated by theUS Centres for Disease Control and Prevention.20 Arecent study in six Indian cities found that more than50% of children younger than 12 years old had bloodlead concentrations higher than 10mg dl21, and morethan 12% of the children tested had concentrations of20mg dl21 or more.27 In China where rapid industrial-isation and increased use of motor vehicles are occur-ring, childhood exposure to lead is undoubtedly a sig-nificant public health issue. A study in Shanghaiindicated that the geometric mean of blood lead con-centration in preschool children was 21.7mg dl21.28
Lead poisoning remains the single most significant andeasily preventable condition associated with anenvironmental and occupational toxin.29 Evidence sug-gests that phasing out leaded gasoline is the most effec-tive way to reduce the general population’s exposureto lead, although other sources of lead exposure arealso important.30 However, about 100 countries are stillplacing their populations—in particular, their chil-dren—at risk by allowing the use of lead in gasoline16
(Figure 2).
Magnitude of Cognitive Effects ofLow-Level Lead Exposure
There have been three meta-analyses of the results ofepidemiological studies quantifying this relationship.Their main results, presented in Table 1, indicated thata doubling in blood lead concentration from 10 to
106 S. TONG AND A.J. McMICHAEL
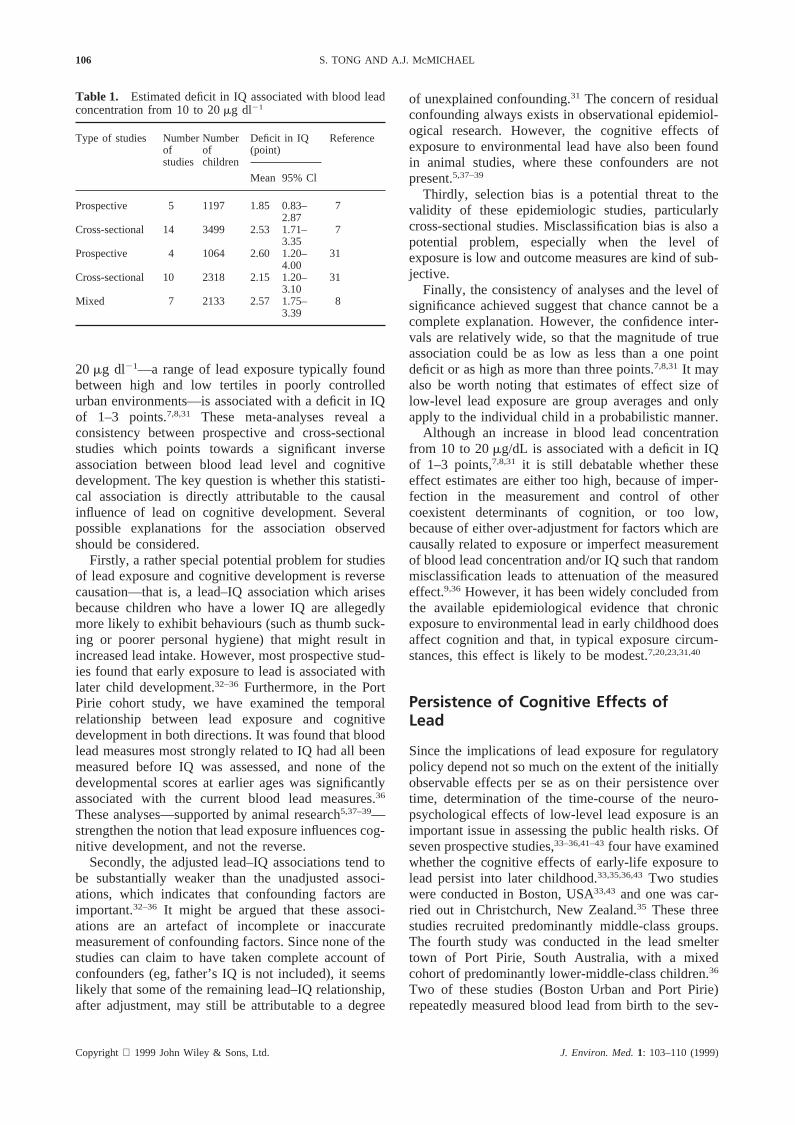
Table 1. Estimated deficit in IQ associated with blood leadconcentration from 10 to 20mg dl21
Type of studies Number Number Deficit in IQ Referenceof of (point)studies children
Mean 95% Cl
Prospective 5 1197 1.85 0.83– 72.87
Cross-sectional 14 3499 2.53 1.71– 73.35
Prospective 4 1064 2.60 1.20– 314.00
Cross-sectional 10 2318 2.15 1.20– 313.10
Mixed 7 2133 2.57 1.75– 83.39
20 mg dl21—a range of lead exposure typically foundbetween high and low tertiles in poorly controlledurban environments—is associated with a deficit in IQof 1–3 points.7,8,31 These meta-analyses reveal aconsistency between prospective and cross-sectionalstudies which points towards a significant inverseassociation between blood lead level and cognitivedevelopment. The key question is whether this statisti-cal association is directly attributable to the causalinfluence of lead on cognitive development. Severalpossible explanations for the association observedshould be considered.
Firstly, a rather special potential problem for studiesof lead exposure and cognitive development is reversecausation—that is, a lead–IQ association which arisesbecause children who have a lower IQ are allegedlymore likely to exhibit behaviours (such as thumb suck-ing or poorer personal hygiene) that might result inincreased lead intake. However, most prospective stud-ies found that early exposure to lead is associated withlater child development.32–36 Furthermore, in the PortPirie cohort study, we have examined the temporalrelationship between lead exposure and cognitivedevelopment in both directions. It was found that bloodlead measures most strongly related to IQ had all beenmeasured before IQ was assessed, and none of thedevelopmental scores at earlier ages was significantlyassociated with the current blood lead measures.36
These analyses—supported by animal research5,37–39—strengthen the notion that lead exposure influences cog-nitive development, and not the reverse.
Secondly, the adjusted lead–IQ associations tend tobe substantially weaker than the unadjusted associ-ations, which indicates that confounding factors areimportant.32–36 It might be argued that these associ-ations are an artefact of incomplete or inaccuratemeasurement of confounding factors. Since none of thestudies can claim to have taken complete account ofconfounders (eg, father’s IQ is not included), it seemslikely that some of the remaining lead–IQ relationship,after adjustment, may still be attributable to a degree
Copyright 1999 John Wiley & Sons, Ltd. J. Environ. Med.1: 103–110 (1999)
of unexplained confounding.31 The concern of residualconfounding always exists in observational epidemiol-ogical research. However, the cognitive effects ofexposure to environmental lead have also been foundin animal studies, where these confounders are notpresent.5,37–39
Thirdly, selection bias is a potential threat to thevalidity of these epidemiologic studies, particularlycross-sectional studies. Misclassification bias is also apotential problem, especially when the level ofexposure is low and outcome measures are kind of sub-jective.
Finally, the consistency of analyses and the level ofsignificance achieved suggest that chance cannot be acomplete explanation. However, the confidence inter-vals are relatively wide, so that the magnitude of trueassociation could be as low as less than a one pointdeficit or as high as more than three points.7,8,31 It mayalso be worth noting that estimates of effect size oflow-level lead exposure are group averages and onlyapply to the individual child in a probabilistic manner.
Although an increase in blood lead concentrationfrom 10 to 20mg/dL is associated with a deficit in IQof 1–3 points,7,8,31 it is still debatable whether theseeffect estimates are either too high, because of imper-fection in the measurement and control of othercoexistent determinants of cognition, or too low,because of either over-adjustment for factors which arecausally related to exposure or imperfect measurementof blood lead concentration and/or IQ such that randommisclassification leads to attenuation of the measuredeffect.9,36 However, it has been widely concluded fromthe available epidemiological evidence that chronicexposure to environmental lead in early childhood doesaffect cognition and that, in typical exposure circum-stances, this effect is likely to be modest.7,20,23,31,40
Persistence of Cognitive Effects ofLead
Since the implications of lead exposure for regulatorypolicy depend not so much on the extent of the initiallyobservable effects per se as on their persistence overtime, determination of the time-course of the neuro-psychological effects of low-level lead exposure is animportant issue in assessing the public health risks. Ofseven prospective studies,33–36,41–43four have examinedwhether the cognitive effects of early-life exposure tolead persist into later childhood.33,35,36,43Two studieswere conducted in Boston, USA33,43 and one was car-ried out in Christchurch, New Zealand.35 These threestudies recruited predominantly middle-class groups.The fourth study was conducted in the lead smeltertown of Port Pirie, South Australia, with a mixedcohort of predominantly lower-middle-class children.36
Two of these studies (Boston Urban and Port Pirie)repeatedly measured blood lead from birth to the sev-

107RISK ASSESSMENT OF LEAD EXPOSURE
eral ages of cognitive assessment, while the other two(Boston Suburban and Christchurch) used dentine leadas an indicator of lead exposure. All the studies gaveclose attention to potential confounders, includingmaternal intelligence, quality of home environment andsocial class.
In the Boston (suburban) study by Needleman andcolleagues,43 132 subjects from the original sample of270 children were re-examined 11 years later. Com-pared with those with dentine lead levels below10 ppm, the subjects with dentine lead levels above20 ppm had a markedly higher risk of dropping out ofhigh school (adjusted odds ratio= 7.4; 95% confidenceinterval: 1.4 to 40.7) and of having a reading disability(odds ratio= 7.4; 5.8; 95% confidence interval: 1.7 to19.7). Higher dentine lead levels were also associatedwith the results of some other neurobehavioural indi-ces. It was concluded from this study that exposure tolead in childhood is associated with deficits in centralnervous system functioning that persist into youngadulthood.
In the Christchurch Study,35 the relationship betweendentine lead levels and the development of word recog-nition abilities was examined at ages 8 to 12 years ina sample of 636 children of the initial cohort of 1265infants. The mean reading test score was found to beconsistently three points lower in children with dentinelead levels above 8 ppm than in those with dentine leadlevels below 3 ppm.
Dentine lead level, however, cannot describe thechronology of change in exposure status with increas-ing age. In contrast, the two long-term follow-up stud-ies in Boston (urban) and Port Pirie, both used serialblood lead concentrations as indices of exposure. In theBoston (urban) study,33 249 infants were recruited atbirth and 148 children were re-assessed at age 10 years.The study shows that slightly elevated blood lead levelsaround age 2 years (mean value: 6.5mg dl21) wereassociated with deficits in intellectual performance atage 10 years. In the Port Pirie study, 375 children ofthe original sample of 723 infants were re-evaluated atage 11–13 years.36 The results indicate that the associ-ation between early-life exposure to environmental leadand impaired cognitive development persists into laterchildhood, even though blood lead concentrations inthese children had declined substantially since theirthird year of life (mean blood lead concentrations atages 2 and 11–13 years were 21.3 and 7.9mg dl21.respectively).
Ruff and colleagues44,45 reported that therapeuticallyreduced blood lead levels were associated with cogni-tive improvement in moderately lead-poisoned childrenaged 13 to 87 months. Participants in their study allhad initial blood lead levels between 1.21 and2.66mmol l21 (22 and 55mg dl21) and reductions wereachieved with the chelating agent calcium sodiumEDTA. However, this study was of small size (126children), and only provided information on the short-
Copyright 1999 John Wiley & Sons, Ltd. J. Environ. Med.1: 103–110 (1999)
term (6 months) impact of clinical intervention onmoderately lead-poisoned children. Hence, it is difficultto appraise the long-term implications and the potentialfor children in non-clinical settings from these data.Moreover, this study has been criticised for its potentialresidual confounding by age of the child and outcomemeasures.46 Recently, it was found that, in the PortPirie cohort study, cognitive scores in children whoseblood lead concentration declined most were generallynot improved relative to the scores of children whoseblood lead levels declined least. Changes in IQ anddeclines in blood lead levels that occurred between theages of 7 and 11 to 13 years (r = 0.12,p = 0.09) sug-gested only slightly better cognition among childrenwhose blood lead levels declined most. Thus, theresults of the Port Pirie cohort study indicate that thecognitive deficits associated with exposure to environ-mental lead in early childhood appear to be only par-tially, at most, reversed by a subsequent decline inblood lead levels.9
In summary, the currently available epidemiologicalevidence suggests that cognitive deficits associatedwith early life exposure to environmental lead persistinto late childhood and early adulthood. We haverecently hypothesised that both the magnitude of theinitial effect of environmental lead exposure and thepersistence of the effect may depend not only on theextent of exposure but also on the timing and chronicityof exposure and on other social and familial factors (egnutrition, stimulating environment, and socioeconomicstatus) that modulate the effect of the lead exposure.36
Threshold Issue
Given the evidence of a persistent effect of chronicexposure to environmental lead, a critical issue iswhether there is a level of exposure below which thisneurotoxicological effect may not occur. Lead has noknown biological role, so, theoretically, the ideal levelof exposure is zero. In practice, a lead-free environmentis impossible to attain, first, because lead is a constitu-ent of the natural environment, and second, the magni-tude and dispersal of lead contamination in the environ-ment that has occurred since the emergence of theindustrial age precludes a return to the levels of thepre-industrial era. However, the goal of zero exposurewould be unnecessary if it were known that there is athreshold for lead-induced effects.
Evidence of a threshold for the neurotoxicity of leadhas been sought. However, the association betweenblood lead and IQ continues even at blood lead levelsbelow 5mg dl21,8,47 although there is a paucity of epid-emiological data at those lower levels. There is specu-lation that no threshold is evident down to a blood leadconcentration of 1mg dl21,8 but it is questionablewhether there is any evidence at such low exposurelevel. Recently, a study of 313 children with a mean

108 S. TONG AND A.J. McMICHAEL
blood lead level of 4.4 (mg dl21) did not find an associ-ation between blood lead level and any of the cognitivefactors.48 Therefore, the authors concluded that theirstudy, despite being designed to maximize the chanceof finding an effect of lead in asymptomatic children,does not support a relationship between lead at verylow doses and cognition in school children. However,it should be noted that no data were provided on qualityassurance and quality control for their blood leadmeasurement.
Toxicological data indicate that lead interferes withhippocampal function, dopamine neurotransmissionand N-methyl-D-aspartate receptor.38,39,49 Picomolarconcentrations of lead also significantly activate proteinkinase C which was partially purified from rat brainand interfere with calcium second messenger systemswhich regulate neurotransmission.37 This pathway maybe critical for learning processes. However, it remainsunclear how to infer these animal data to humans inthe assessment of a threshold of lead exposure.
At present, there is insufficient evidence to draw afirm conclusion about the possible existence of a thres-hold since few data are available in the range that isnow regarded as a very low level of exposure (eg bloodlead level less than 0.24mmol l21 (5 mg dl21). There-fore, further reductions of environmental lead exposuremay be required before we can determine, with epi-demiological studies, if there is a threshold level forneurotoxicity within this low exposure range. Suchresearch would require the study of a large number ofsubjects at these lower exposure levels, either byplanned multi-centre collaboration or by subsequentmeta-analysis.
Public Health Implications of CognitiveEffects of Lead
The finding that the association between early-lifeexposure to environmental lead and impaired cognitivedevelopment persists through and beyond childhoodstrengthens the rationale for public health measures toprevent neurotoxicological effects of environmentallead exposure in early childhood. Formal assessmentof the population health risk can assist the making ofpublic health policy.
Since lead is ubiquitous in the environment, a mod-est health impact upon each exposed individual withina population would result in a substantial aggregateimpact for the total population. It is undesirable for anentire community of exposed individuals to undergo asmall downward shift in the distribution of cognitiveperformance, even though for the great majority ofchildren the cognitive deficits would be neither clini-cally identifiable nor environmentally attributable at theindividual level. For example, in a hypothetical popu-lation of 100 000 persons with a Gaussian distributionof IQ, 2300 would have an IQ above 130, based on the
Copyright 1999 John Wiley & Sons, Ltd. J. Environ. Med.1: 103–110 (1999)
population mean IQ score of 100 and standard devi-ation of 15. If, because of the effects of lead exposure,the population mean IQ score declined to 97, the num-ber of individuals scoring above 130 in a total popu-lation of 100 000 would drop by 38.4% from 2300 to1400. The number of individuals with IQ below 70would correspondingly increase from 2300 to 3200.
An alternative mode of impact assessment has beenproposed by Ostro.50 To estimate the attributable lossof IQ points in, for example, 40 000 young childrenexposed to an (avoidable) excess of 4mg m23 of leadin air (PbAir), he uses the following equation:
Aggregate loss of IQ= 0.9753 4 3 40 000= 156 000IQ points
Ostro points out that, while the predominant measureof ‘exposure’ used in epidemiological studies has beenPbB, the conversion factor of PbAir/PbB can be esti-mated as 3.9 (ie as air lead increases 1mg m23, therewill be an increase of 3.9mg dl21 in PbB for children).From the literature-based dose-response relationship,he derives an estimate of a 0.25 IQ point deficit per1 mg dl21 increase in PbB, which becomes 0.253 3.9= 0.975 IQ point deficit per 1mg m23 PbAir.
If the aggregate loss of IQ is 156 000 IQ points for40 000 young children exposed to an excess of 4mgm23 of PbAir, we can convert this to an estimation ofthe total loss in the expected present value of lifetimeearnings from exposure to lead. From the figures pub-lished by the US Centers for Disease Control,20 thiscategory of economic loss would be $713 232 000 forthis hypothetical group of children. The details andimplied priorities of such economic impact calculationsare, of course, debatable. However, this example indi-cates how, in principle, a quantitative assessment ofpopulation health risk and its social consequences canbe made.
The effect of lead should also be viewed relative tothe effects of other determinants of cognitive develop-ment. The data from the Port Pirie Cohort Study9,32,36,51
show that, compared with other socio-environmentaland familial factors, the estimated proportion of thetotal variance in cognition attributable to lead is small.However, this should not overshadow two importantconsiderations. First, lead exposure is technically pre-ventable (or substantially reducible). Second, unrem-edied, persistent, environmental lead will affect suc-cessive generations of children.
Conclusions
The evidence appraised here indicates that exposure toenvironmental lead has a persistent effect on cognitivedevelopment in young children. The environmentallead problem is preventable, or, where it is alreadyestablished, is remediable (although this is expensive).

109RISK ASSESSMENT OF LEAD EXPOSURE
It should therefore be addressed, especially indeveloping countries where rapid industrialisation andincreased use of motor vehicles are occurring. How-ever, since lead continues to have some importantindustrial uses, the formulation of a public health strat-egy will, in reality, seek a balance between consider-ation of the nature and extent of the risk to humanpopulation health, knowledge of any dose-effect thres-hold, and making the best use of existing resources.The development of such a strategy should take intoaccount the views and priorities of all interested parties,and—most certainly—those of communities directly atrisk from lead exposure.
A public health strategy to reduce the adverse effectsof lead exposure upon the cognitive development ofyoung children should include the following:
1. Systematic monitoring: A national surveillance sys-tem for monitoring exposure to, selected or sentinel,environmental contaminants, including lead, shouldbe established.
2. Identification of communities in need: Appropriateinterventions should be undertaken within the mostvulnerable communities. Some communities, suchas those with old housing with lead-based paint, orclose to highways, lead mines, lead smelting facili-ties, or battery factories, may have a large pro-portion of children exposed to lead.
3. Community education and public awareness: This isimportant for the successful implementation of anyintervention programme.
A wide range of surveillance and preventive actionshas been implemented in Australia in recent years, eg,a national survey of lead in children and severaldecontamination programmes in lead smelting com-munities such as Port Pirie, Boolaroo and Argenton.This Australian experience and resultant expertiseshould have potential for assisting developing countriesto solve their environmental lead problem.
There are two further considerations. First, anapproach that addresses the many social-environmentalinfluences on childhood development should beadopted, alongside specific measures to preventenvironmental lead exposure in young children.Second, although extensive data have been collectedon the health effect of lead exposure, several issuesremain unresolved. Further research will therefore berequired to determine the best measure of body leadburden at low levels of exposure; the most sensitiveindicator of the effects of lead; whether there is a thres-hold for lead-induced effects; And what is the mostcost- effective method for reducing and preventinglead exposure.
Meanwhile, the results of two decades of researchinto the childhood health consequences of environmen-tal lead exposure provide a clear justification for sys-tematic public health interventions to reduce this wide-spread environmental health problem.
Copyright 1999 John Wiley & Sons, Ltd. J. Environ. Med.1: 103–110 (1999)
References
1. Zimdahl RL, Hassett JJ. Lead in soil. InLead in theEnvironment, Boggess WR, Wixson BG (eds), CastleHouse Publications: Illinois, 1979.
2. Shy CM. Lead in petrol: the mistake of the 20th century.Wld Hlth Statist Quart1990; 43: 168–176.
3. US Environmental Protection Agency.Air Quality Cri-teria for Lead. (EPA/600/8–83/028aF) EnvironmentalCriteria and Assessment Office: NC, USA, 1986.
4. US Agency for Toxic Substances and Disease Registry.The Nature and Extent of Lead Poisoning in Children inthe United States: A report to Congress, Department ofHealth and Human Services: Atlanta, 1988.
5. Goldstein GW. Neurological concepts of lead poisoningin children.Pediatr. Annals1992; 21(6): 384–388.
6. Davis M. Risk assessment of the developmental neuro-toxicity of lead.Neuro. Toxicol.1990; 11: 285–292.
7. Pocock SJ, Smith M, Baghurst P. Environmental lead andchildren’s intelligence: a systematic review of the epide-miological evidence.BMJ 1994; 309: 1189–1197.
8. Schwartz J. Low-level lead exposure and children’s IQ:A meta-analysis and search for a threshold.Environ. Res.1994; 65: 42–55.
9. Tong S, Baghurst P, McMichael A, Sawyer M, MudgeJ. Declining blood lead levels and changes in cognitivefunction during childhood: the Port Pirie Cohort Study.JAMA 1998; 280: 1915–1919.
10. Winder C. The Developmental Neurotoxicity of Lead,MTP Press, Lancaster, 1984.
11. Smith MA. Lead in history. InThe Lead Debate: TheEnvironmental Toxicology and Child Health, LansdownR, Yule W (eds), Croom Helm: London, 1986.
12. Kazantzis G. Lead: Ancient metal—Modern menace? InLead Exposure and Child Development: An InternationalAssessment, Smith MA, Grant LD, Sors AI (eds), MTPPress: Lancaster, 1989; 119–128.
13. Rabinowitz MB. Stable isotopes of lead for source identi-fication. J. Toxicol.1995;33: 649–655.
14. Nriagu JO. Saturnine gout among Roman aristocrats: Didlead poisoning contribute to the fall of the Empire?N.Engl. J. Med.1983;308: 660–663.
15. Ratcliffe JM.Lead in Man and the Environment. ElisHorwood: Chichester, 1981.
16. World Resources Institute.1998–99 World Resources: AGuide to the Global Environment, World Resources Insti-tute: New York, 1998.
17. Nriagu JO, Blankson ML, Ocran K. Childhood lead poi-soning in Africa: a growing public health problem.Sci.Total Environ.1996; 181: 93–100.
18. Nriagu JO, Pacnya JM. Quantitative assessment of world-wide contamination of air, water and soils by trace met-als. Nature1988; 333: 134–139.
19. Flegal AR, Smith DR. Lead levels in preindustrialhumans.N. Engl. J. Med.1992b;326: 1293–1294.
20. US Centers for Disease Control.Strategic Plan for theElimination of Childhood Lead Poisoning. US Depart-ment of Health and Human Services: Washington, DC,1991.
21. Ericson JE, Shirahata H, Patterson CC. Skeletal concen-tration of lead in ancient Peruvians.N. Engl. J. Med.1979; 300: 946–951.
110 S. TONG AND A.J. McMICHAEL
22. Patterson CC, Ericson J, Manea-Krichten M, ShirahataH. Natural skeletal levels of lead inHomo sapiensuncon-taminated by technological lead.Sci. Total Environ.1991; 107: 205–230.
23. Australian Department of Health, Housing, LocalGovernment and Community Services.Reducing LeadExposure in Australia: Risk Assessment and Analysis ofEconomic, Social and Environmental Impacts. AustralianGovernment Publishing Service: Canberra, 1994.
24. Alliance to End Childhood Lead Poisoning.The GlobalDimensions of Lead Poisoning, Washington DC, 1994.
25. Khaliquzzman M, Biswas SK, Tarafdar SA, Islam A,Khan AH. Trace Element Composition of Size Fraction-ated Airborne Particulate Matter in Urban and RuralAreas in Bangladesh—Report. Accelerator FacilitiesDivision and Chemistry Division, Atomic Energy Center:Dhaka, 1997.
26. Viswanathan P, Patrikh DJ, Nath R, Chandra SV, PitchaiR, Chatterjee GC. Biological monitoring and lead andcadmium. InToxic Metals in the Indian Environment,Krishna Murti CR, Viswanathan P (eds), Tata McGraw-Hill: New Delhi, 1991; 212–235.
27. Sharma D. Alarming amounts of lead found in Indianchildren.Lancet1999;353: 647.
28. Shen XM, Guo D, Xu JD. The adverse efect of mar-ginally higher lead level on intelligence development ofchildren: a Shanghai study.Indian J. Pediatr.1992; 59:233–238.
29. Silbergeld E, Tonat K. Investing in prevention: Opport-unities to prevent disease and reduce health care costsby identifying environmental and occupational causes ofnoncancer disease.Toxicol. Indust. Health1994;10: 677.
30. Silbergeld E. The international dimensions of leadexposure.Int. J. Occup. Environ. Health1995;338: 340.
31. IPCS Inorganic Lead. Environmental Health Criteria165. World Health Organisation; Geneva, 1995.
32. McMichael AJ, Baghurst PA, Wigg NR, Vimpani GV,Robertson EF, Roberts RJ. Port Pirie cohort study:Environmental exposure to lead and children’s abilitiesat the age of four years.N. Engl. J. Med.1988; 319:468–475.
33. Bellinger D, Stiles KM, Needleman H. Low-level leadexposure, intelligence and academic achievement: Along-term follow-up study.Pediatrics 1992; 90: 855–861.
34. Dietrich KN, Succop PA, Berger OG, Keith RW. Leadexposure and the central auditory processing abilities andcognitive development of Urban children: the Cincinnatilead study cohort at age 5 years.Neurotoxicol. Teratol.1992; 14: 51–56.
35. Fergusson DM, Horwood LJ. The effects of lead levelson the growth of word recognition in middle childhood.Int. J. Epidemiol.1993; 22: 891–897.
36. Tong S, Baghurst P, McMichael A, Sawyer M, MudgeJ. Lifetime exposure to environmental lead and children’sintelligence at 11–13 years: the Port Pirie cohort study.BMJ 1996;312: 1569–1575.
Copyright 1999 John Wiley & Sons, Ltd. J. Environ. Med.1: 103–110 (1999)
37. Markovac J, Goldstein GW. Picomolar concentrations oflead stimulate brain protein kinase C.Nature1988;334:71–73.
38. Alkondon M, Costa ACS, Radhakrishnan V. Selectiveblockade of NMDA-activated channel currents may beimplicated in learning deficits caused by lead.FEBS Lett.1990; 261: 124–130.
39. Jett DA, Kuhlmann AC, Guilarte TR. Lead impairs spa-tial learning in the Morris water maze: Studies usingchronic developmental exposure and acute intra-hippo-campal microinjection.Fund. Appl. Toxicol. (Suppl.)1996; 30: 25.
40. Needleman H, Gatsonis C. Low-level lead exposure andthe IQ of children.JAMA 1990; 263: 673–678.
41. Ernhart CB, Morrow-Tlucak M, Wolf AW, Super D,Drotar D. Low-level lead exposure in the prenatal andearly preschool periods: Intelligence prior to schoolentry. Neurotoxicol. Teratol.1989; 11: 161–170.
42. Cooney GH, Bell A, McBride W, Carter C. Low leadexposure to lead: the Sydney lead study.Dev. Med.Child. Neurol1989; 31: 640–649.
43. Needleman H, Schell A, Bellinger D, Leviton A, AllredE. The long-term effects of exposure to low doses of leadin childhood: An 11-year follow-up report.N. Engl. J.Med. 1990; 322: 83–88.
44. Ruff HA, Bijur PE, Markowitz M, Ma Y, Rosen JF.Declining blood lead levels and cognitive changes inmoderately lead-poisoned children.JAMA 1993; 269:1641–1646.
45. Ruff HA, Markowitz M, Bijur PE, Rosen JF. Relation-ships among blood lead levels, iron deficiency, and cog-nitive development in two-year-old children.Environ.Health Perspect.1996; 104: 180–185.
46. Binder S, Matte T. Childhood lead poisoning: the impactof prevention.JAMA 1993; 269: 1679–1681.
47. Schwartz J. Beyond LOEL’s, p values, and vote coun-ting: methods for looking at the shapes and strengths ofassociations.Neurotoxicology1993; 14: 237–246.
48. Minder B, Das-Smaal EA, Orlebeke JE. Cognition inchildren does not suffer from very low lead exposure.J.Learning Disabilities1998; 31(5): 492–502.
49. Cory-Slechta DA, Widzowski DV. Low-level leadexposure increases sensitivity to the stimulus propertiesof dopamine D1 and D2 agonists.Brain Res.1991;553:65–74.
50. Ostro B.Estimating the Health Effects of Air Pollutants.Policy Research Working Paper 1301, World Bank:Washington, DC, 1994.
51. Baghurst PA, McMichael AJ, Wigg NRet al. Environ-mental exposure to lead and children’s intelligence at theage of seven years: the Port Pirie cohort study.N. Engl.J. Med.1992;327: 1279–1284.
52. Flegal AR, Smith DR. Current needs for increased accu-racy and precision in measurements of low levels of leadin blood. Environ. Res.1992a;58: 125–133.