the liver - medinfo2.psu.ac.ththe liver. lobar and segmental anatomy. ... treatment. 1. abscess >...
TRANSCRIPT

THE LIVERTHE LIVER

Lobar and segmental anatomyLobar and segmental anatomy

Vascular anatomy (dual blood supplies)
75% 25%

Infectious disease of liverInfectious disease of liver

�� PyogenicPyogenic liver abscess liver abscess
�� Amebic liver abscessAmebic liver abscess

�� PyogenicPyogenic liver abscess liver abscess
�� Amebic liver abscessAmebic liver abscess

EtiologyEtiology
Liver invasion by bacteria:Liver invasion by bacteria:
�� Ascending infection in Ascending infection in
the the biliarybiliary tracttract
�� Vascular seeding Vascular seeding
(portal or arterial)(portal or arterial)
�� Direct invasion from a Direct invasion from a
nearby sourcenearby source
�� Traumatic implantationTraumatic implantation

Origins and causes of Origins and causes of pyogenicpyogenic liver abscessliver abscess
BiliaryBiliary tracttract LithiasisLithiasis
CholangiocarcinomaCholangiocarcinoma
StricturesStrictures
BiliaryBiliary--enteric enteric anastomosisanastomosis
BiliaryBiliary proceduresprocedures
Portal veinPortal vein AppendicitisAppendicitis
DiverticulitisDiverticulitis
Crohn'sCrohn's diseasedisease
Hepatic arteryHepatic artery Bacterial Bacterial endocarditisendocarditis
Dental infectionDental infection
Direct extensionDirect extension Gall bladder Gall bladder empyemaempyema
Perforated peptic ulcerPerforated peptic ulcer
SubphrenicSubphrenic abscessabscess
TraumaTrauma Abdominal traumaAbdominal trauma
ChemoembolizationChemoembolization
Ethanol injection or radiofrequency Ethanol injection or radiofrequency
ablationablation
CryptogenicCryptogenic
EtiologyEtiology

Depended on cause of abscessDepended on cause of abscess
�� BiliaryBiliary
gramgram--negative aerobic bacilli and negative aerobic bacilli and enterococcienterococci
�� Pelvic/Pelvic/intraperitonealintraperitoneal
Mixed aerobic and anaerobic (Mixed aerobic and anaerobic (BacteroidesBacteroides fragilisfragilis))
�� HematogenousHematogenous/trauma/trauma
Single (Single (StaphStaph aureusaureus, Strep, Strep))
MicrobiologyMicrobiology

Fever (90%)Fever (90%)
RUQ, RUQ, epigastricepigastric painpain
Jaundice (25%)Jaundice (25%)
ChillsChills
AnorexiaAnorexia
Weight lossWeight loss
Nausea, vomitingNausea, vomiting
Weakness, malaiseWeakness, malaise
Clinical manifestationClinical manifestation

↑↑ alkaline alkaline phosphatasephosphatase (80%)(80%)
↑↑ bilirubinbilirubin (20(20--50%)50%)
leukocytosisleukocytosis (70(70--90%)90%)
CXRCXR
�� R R hemidiaphragmhemidiaphragm elevationelevation
�� R basilar infiltrateR basilar infiltrate
�� Unilateral pleural effusionUnilateral pleural effusion
Clinical manifestationClinical manifestation

1.Imaging1.Imaging
�� Ultrasound : initial testUltrasound : initial test
�� CT : If suspected CT : If suspected intraabdominalintraabdominal pathologypathology
�� MRI : no benefit over CT scanMRI : no benefit over CT scan
2.Microbial cultures2.Microbial cultures (aerobic, anaerobic)(aerobic, anaerobic)
�� AspirationAspiration
3.Serology3.Serology
�� R/O AmebicR/O Amebic
DiagnosisDiagnosis



1.Abscess management1.Abscess management
2.Underlying cause management2.Underlying cause management
TreatmentTreatment

1.Abscess management1.Abscess management
(1) IV ATB(1) IV ATB
33rdrd gengen cephalosporinscephalosporins+ + metronidazolemetronidazole
oror ampicillin+gentamicin+metronidazoleampicillin+gentamicin+metronidazole
x 10x 10--14 days14 days then then
continue oral ATB until continue oral ATB until 44--6 weeks6 weeks
(2) Drain abscess(2) Drain abscess
-- PercutaneousPercutaneous drainage**drainage**
-- PercutaneousPercutaneous needle aspirationneedle aspiration
-- Surgical drainageSurgical drainage

PCD success rate > PNAPCD success rate > PNA
But PNA may consider in But PNA may consider in unilocularunilocular
abscess < 5 cmabscess < 5 cm
SurgerySurgery
1.Tx primary pathologic process1.Tx primary pathologic process
2.Failed PCD2.Failed PCD

�� PyogenicPyogenic liver abscessliver abscess
�� Amebic liver abscessAmebic liver abscess

EntamoebaEntamoeba histolyticahistolytica
Trophozoite Cyst

PathogenesisPathogenesis

Symptoms like Symptoms like pyogenicpyogenic liver abscessliver abscess but but
delay onset and less sepsisdelay onset and less sepsis
Male : female = 10 : 1, Age < 50 yrsMale : female = 10 : 1, Age < 50 yrs
1/3 diarrhea but 70% of pt : stool exam 1/3 diarrhea but 70% of pt : stool exam negneg
CBC : CBC : leucocytosisleucocytosis without without eosinophiliaeosinophilia
LFT : elevate ALP, LFT : elevate ALP, transminasestransminases
Clinical manifestationClinical manifestation

1.circulating amebic antibody 1.circulating amebic antibody (sens&spec95%)(sens&spec95%)
+ +
2.Imaging study : 2.Imaging study : USG USG
CT scan whenCT scan when
No response to medicationNo response to medication
Diagnosis uncertainDiagnosis uncertain
Suspicious complicationSuspicious complication
DiagnosisDiagnosis
MetronidazoleMetronidazole 750 mg 750 mg popo tidtid x 10 days x 10 days
IntraluminalIntraluminal amebicidalamebicidal agentsagents
((IodoquinolIodoquinol, , paromomycinparomomycin ,,diloxanidediloxanide furoatefuroate))
PNA not indicate in every patients but PNA not indicate in every patients but
selected inselected in
TreatmentTreatment

1.1.abscess > 5 cmabscess > 5 cm
2.2.abscess at Lt lobe liverabscess at Lt lobe liver
3.3.secondary bacterial infectionsecondary bacterial infection
4.4.clinical not improve in 3clinical not improve in 3--5 days after 5 days after
medicationmedication
5.5.amebic cytology inconclusive amebic cytology inconclusive
(cannot R/O (cannot R/O pyogenicpyogenic))
6.6.pregnancy pregnancy
(contraindication for (contraindication for metronidazolemetronidazole))


GI portal veinGI portal veinbiliarybiliary tract tract
infectioninfection
Cause Cause
amebaamebabacteria bacteria OrganismOrganism
imaging, imaging,
serologyserology
history, imaging history, imaging
aspiration, aspiration,
hemoculturehemoculture
DiagnosisDiagnosis
amebicidalamebicidalantibiotic + antibiotic +
drainage drainage
Treatment Treatment
right loberight loberight loberight lobeLocationLocation
> 80 % > 80 % 50 % 50 % Solitary Solitary
10 : 110 : 12 : 12 : 1M : FM : F
2020--4040> 50 > 50 Age ( yr)Age ( yr)
ALAALAPLAPLA

Benign liver tumorsBenign liver tumors

Benign liver tumorBenign liver tumor
HepatocyteHepatocyte : hepatic adenoma: hepatic adenoma
: focal nodular hyperplasi: focal nodular hyperplasia a
MesenchymalMesenchymal tissue : tissue : hamartomahamartoma
: : hemangiomahemangioma
HeterotopicHeterotopic tissue : adrenal resttissue : adrenal rest
: pancreatic rest: pancreatic rest

Cavernous Cavernous hemangiomahemangioma

The most common benign tumor of liverThe most common benign tumor of liver
Mean age 50 years; female predominant Mean age 50 years; female predominant
““Giant Giant HemangiomaHemangioma”” –– size size ≥≥ 10 cm10 cm
Pathogenesis Pathogenesis –– not well understoodnot well understood



AsymptomAsymptom
Symptom :Symptom :
-- RuptureRupture
-- CompressionCompression
-- KasabachKasabach Merritt syndromeMerritt syndrome

““Whatever the size, there is Whatever the size, there is no treatment for no treatment for
asymptomatic asymptomatic hemangiomahemangioma””
Rare growth and complicationRare growth and complication
TreatmentTreatment

Indications for surgical resectionIndications for surgical resection
�� Severe abdominal painSevere abdominal pain
�� Rapid enlargement of tumorRapid enlargement of tumor
�� Rupture or potential ruptureRupture or potential rupture
�� Indeterminate diagnosisIndeterminate diagnosis
�� ComplicationComplication
SurgerySurgery : : enucleationenucleation, liver resection or liver, liver resection or liver
transplantation transplantation

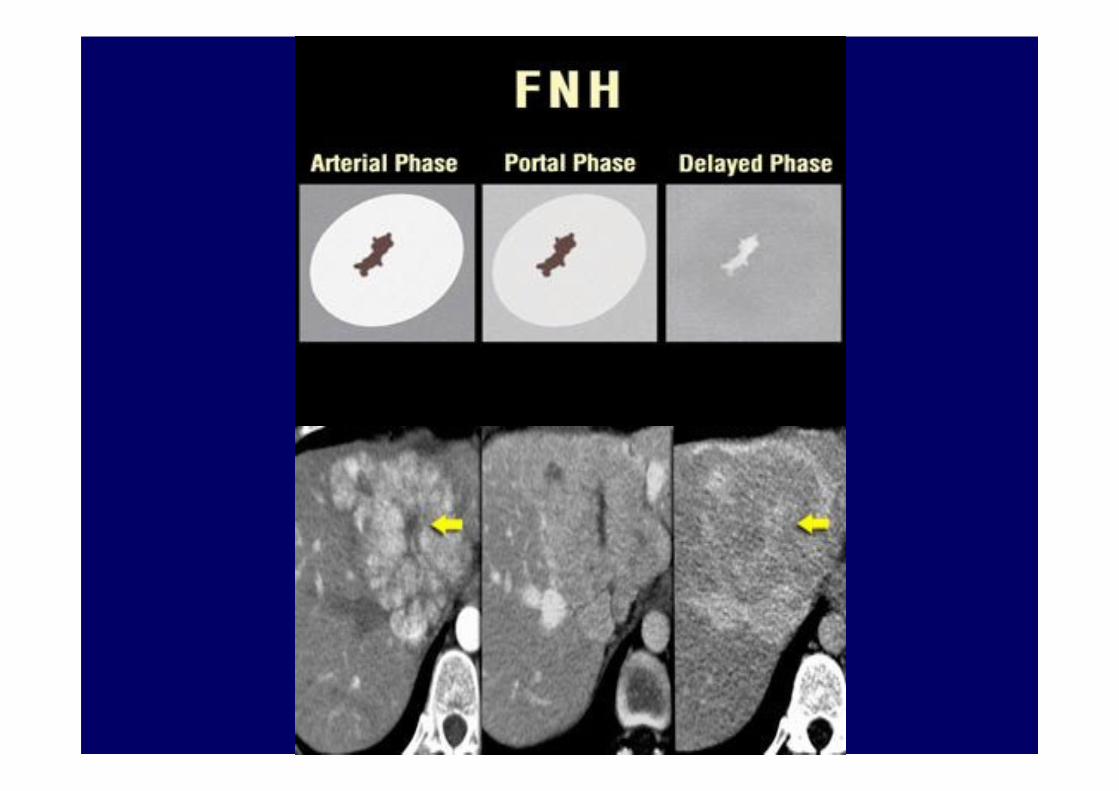
Focal nodular hyperplasiaFocal nodular hyperplasia

Benign tumor like lesionBenign tumor like lesion
Hyperplasia/regeneration processHyperplasia/regeneration process
No malignant potentialNo malignant potential
Rarely complicationRarely complication


Asymptomatic pt : no Asymptomatic pt : no TxTx
Indication for surgeryIndication for surgery
Indeterminate diagnosisIndeterminate diagnosis
Severe abdominal pain (R/O other causes)Severe abdominal pain (R/O other causes)
Prefer resection > Prefer resection > enucleationenucleation
TreatmentTreatment

Hepatic adenomaHepatic adenoma

Associated oral contraceptive use Associated oral contraceptive use
Risk of hemorrhage or rupture ~20Risk of hemorrhage or rupture ~20--40%40%
Increase risk of bleedingIncrease risk of bleeding
�� Women taking oral contraceptives Women taking oral contraceptives
�� During pregnancyDuring pregnancy
�� Tumor >4Tumor >4--5 cm5 cm

Risk of malignant transformationRisk of malignant transformation –– 10%10%



size < 4 cm cessation of pill + avoidance size < 4 cm cessation of pill + avoidance
pregnancypregnancy
indication for surgeryindication for surgery
: size > 4 cm: size > 4 cm
: don: don’’t shrink after cessation of pillt shrink after cessation of pill
: can: can’’t stop pill t stop pill
: plan become pregnancy: plan become pregnancy
: rupture: rupture
Procedure of choice = resectionProcedure of choice = resection
TreatmentTreatment

Simple hepatic cystSimple hepatic cyst



Asymptomatic : F.U.Asymptomatic : F.U.
TxTx when only symptomatic ptwhen only symptomatic pt
aspiration only recurrence 100 %aspiration only recurrence 100 %
Choice of treatmentChoice of treatment
1.PAIR (1.PAIR (percutaneouspercutaneous aspiration instillation and aspiration instillation and
reaspirationreaspiration))
2.Unroofing or fenestration 2.Unroofing or fenestration
3.Cystectomy or 3.Cystectomy or hepatectomyhepatectomy : rarely required: rarely required
TreatmentTreatment

BiliaryBiliary cystadenomacystadenoma
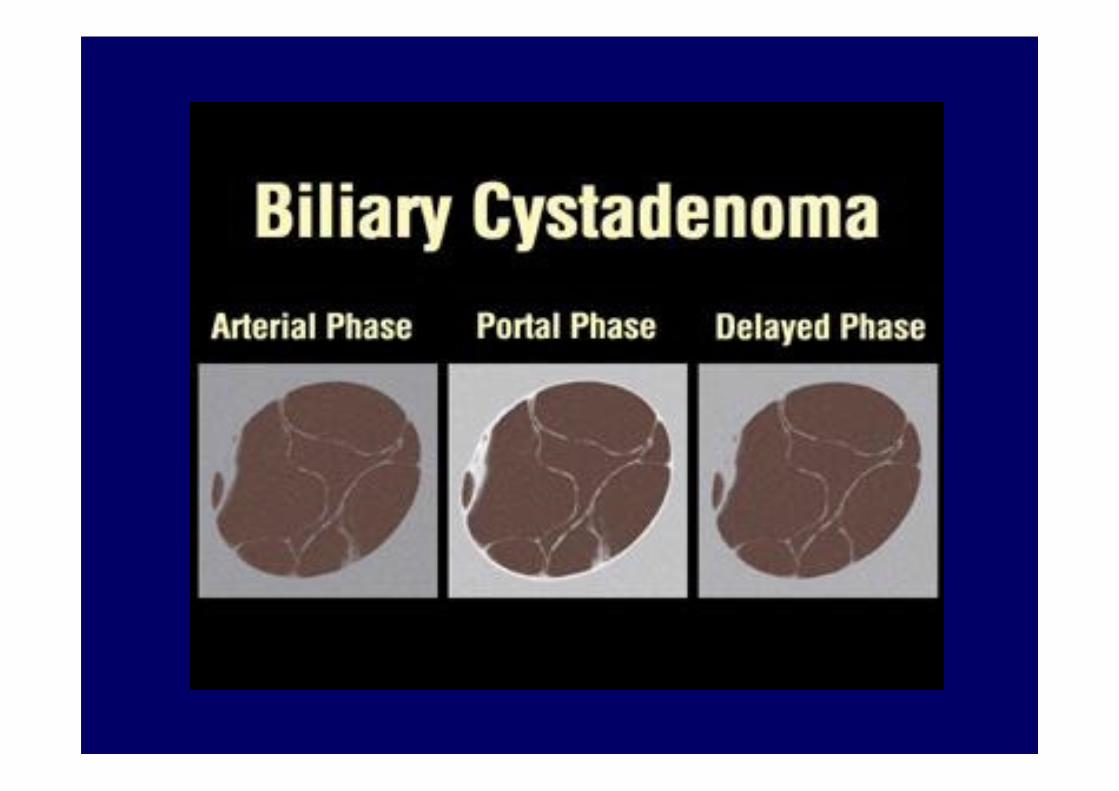

multimulti--loculationloculation , internal , internal septationseptation, calcification , papillary , calcification , papillary
projection, thick nodular wall.projection, thick nodular wall.

CystadenomaCystadenoma : : malignant 25 %malignant 25 %
TxTx of choice : of choice : resectionresection
TreatmentTreatment

Malignant liver tumorMalignant liver tumor

�� HepatocellularHepatocellular carcinomacarcinoma
�� CholangiocarcinomaCholangiocarcinoma
�� MetastaticMetastatic liver tumorliver tumor

HepatocellularHepatocellular carcinomacarcinoma

-- Liver cirrhosisLiver cirrhosis
-- Hepatitis B, CHepatitis B, C
-- AflatoxinAflatoxin
-- AlcoholAlcohol
-- HemochromatosisHemochromatosis
-- WilsonWilson’’s diseases disease
Risk factorsRisk factors

-- Symptom of cirrhosisSymptom of cirrhosis
-- Abdominal pain/mass, jaundice, feverAbdominal pain/mass, jaundice, fever
-- AsymptomAsymptom but incidental findingsbut incidental findings
Clinical manifestationClinical manifestation

DiagnosisDiagnosis

AASLDAASLD
(American Association for the Surgery of (American Association for the Surgery of
Liver Disease)Liver Disease)
Diagnosis Diagnosis guided by the size of the lesionguided by the size of the lesion

Lesion < 1 cm in diameterLesion < 1 cm in diameter
�� Follow with US q 3 Follow with US q 3 –– 6 months x 2 yrs6 months x 2 yrs
-- Stable lesion Stable lesion �������� revert to routine surveillancerevert to routine surveillance
-- Enlarging lesion Enlarging lesion �������� proceed according to sizeproceed according to size
Lesion 1 Lesion 1 –– 2 cm in diameter2 cm in diameter
�� 2 dynamic imaging studies2 dynamic imaging studies
-- Typical HCC x 2 technique Typical HCC x 2 technique �������� DxDx HCCHCC
-- Others Others �������� liver biopsyliver biopsy

Lesion > 2 cm in diameterLesion > 2 cm in diameter
�� One dynamic imagingOne dynamic imaging
-- Typical features of HCC Typical features of HCC �������� DiagnosisDiagnosis
-- AFP > 200 AFP > 200 ng/mLng/mL �������� DiagnosisDiagnosis
-- Atypical vascular pattern Atypical vascular pattern �������� BiopsyBiopsy


HCCHCC

TreatmentTreatment

The BarcelonaThe Barcelona--ClinicClinic-- LiverLiver--Cancer (BCLC) Cancer (BCLC)
staging systemstaging system
Includes variables related to Includes variables related to
�� Tumor stage (Okuda)Tumor stage (Okuda)
�� Liver functional status (ChildLiver functional status (Child’’s s pughpugh))
�� Physical status (WHO)Physical status (WHO)
TreatmentTreatment

Okuda classificationOkuda classificationStageStage Tumor SizeTumor Size AscitesAscites AlbuminAlbumin BilirubinBilirubin
> 50 %> 50 %
( + )( + )< 50%< 50%
( ( -- ))( + )( + ) ( ( -- )) < 3 g/dl< 3 g/dl
( + )( + )> 3 g/dl> 3 g/dl
( ( -- ))> 3 mg/dl> 3 mg/dl
( + )( + )< 3 mg/dl< 3 mg/dl
( ( -- ))
II ( ( -- )) ( ( -- )) ( ( -- )) ( ( -- ))
IIII 1 or 2 ( + )1 or 2 ( + )
IIIIII 3 or 4 ( + )3 or 4 ( + )

ChildChild’’s s pughpugh classificationclassification
Clinical or laboratory Clinical or laboratory
featurefeature1 point1 point 2 points2 points 3 points3 points
Encephalopathy (grade)Encephalopathy (grade) 0 (absent)0 (absent) 1 1 –– 22 3 3 –– 44
AscitesAscites AbsentAbsent SlightSlight PoorlyPoorly
BilirubinBilirubin (mg/dl)(mg/dl) < 2.0< 2.0 2.0 2.0 –– 3.03.0 > 3.0> 3.0
Albumin (g/dl)Albumin (g/dl) > 3.5> 3.5 2.8 2.8 –– 3.53.5 < 2.8< 2.8
INRINR < 1.7< 1.7 1.7 1.7 –– 2.22.2 > 2.3> 2.3
Each feature is assigned 1, 2, or 3 points.Class A: 5 – 6 points; Class B: 7 – 9 points; Class C: 10 – 15 points

WHO performance statusWHO performance statusWorld Health Organization Performance Status gradesWorld Health Organization Performance Status grades
Stage 0Stage 0 Fully active, normal life, no symptomsFully active, normal life, no symptoms
Stage 1Stage 1 Minor symptoms, able to do light activityMinor symptoms, able to do light activity
Stage 2Stage 2 Capable of selfCapable of self--care but unable to carry out work activitiescare but unable to carry out work activities
Up for more than 50% waking hoursUp for more than 50% waking hours
Stage 3Stage 3 Limited self care capacityLimited self care capacity
Confined to bed or chair > 50% waking hoursConfined to bed or chair > 50% waking hours
Stage 4Stage 4 Completely disabledCompletely disabled
Confined to bed or chairConfined to bed or chair


Curative treatmentCurative treatment
1.Resection1.Resection
2.Liver transplantation2.Liver transplantation
3.Radiofrequency ablation3.Radiofrequency ablation

CholangiocarcinomaCholangiocarcinoma

-- Primary Primary sclerosingsclerosing cholangitischolangitis
-- CholedochalCholedochal cystcyst
-- HepatolithiasisHepatolithiasis
-- Liver flukesLiver flukes
-- Prior Prior biliarybiliary--enteric enteric anastomosisanastomosis
-- Toxic substances : nitric oxide Toxic substances : nitric oxide
: nitrosamine : nitrosamine
: : thorotrastthorotrast
-- Congenital hepatic fibrosisCongenital hepatic fibrosis
Risk factorsRisk factors

-- Fever, anorexia, weight loss, Fever, anorexia, weight loss,
abdominal massabdominal mass
--““cholestaticcholestatic jaundicejaundice””
-- Progressive jaundice, dark urine, pale Progressive jaundice, dark urine, pale
stool, stool, prurituspruritus
Clinical manifestationClinical manifestation

LFT : direct LFT : direct hyperbilirubinemiahyperbilirubinemia, elevated , elevated
ALPALP
USG : USG : intrahepaticintrahepatic mass, bile duct dilatationmass, bile duct dilatation
CT scan or MRICT scan or MRI
+ tumor marker CA 19+ tumor marker CA 19--99
DiagnosisDiagnosis

Mainstay : Liver resectionMainstay : Liver resection
Other modalities for Other modalities for noncurativenoncurative treatmenttreatment
but poor outcomebut poor outcome
TreatmentTreatment

BILIARY SYSTEMSBILIARY SYSTEMS

Gallstone diseasesGallstone diseases

Gallstone diseaseGallstone disease
Female : male = 3:1Female : male = 3:1
Risk factorsRisk factors
Pregnancy Pregnancy Terminal Terminal ilealileal resectionresection
ObesityObesity Gastric surgery Gastric surgery
Crohn'sCrohn's disease disease Hemolytic anemiaHemolytic anemia

Bile = Bile = bilebile salts, phospholipids, cholesterolsalts, phospholipids, cholesterol
Gallstones due to Gallstones due to imbalanceimbalance rendering rendering
cholesterol & calcium salts insolublecholesterol & calcium salts insoluble
Pathogenesis involves 3 stagesPathogenesis involves 3 stages::
�� 1. cholesterol 1. cholesterol supersaturationsupersaturation in bilein bile
�� 2. crystal nucleation2. crystal nucleation
�� 3. stone growth3. stone growth

Asymptomatic gallstoneAsymptomatic gallstone

3% risk of developing symptoms/ year
2/3 will remain symptom free at 20000 years
No require treatment

Study from Cochrane review 2007
No RCT/meta-analysis about treatment of
asymptomatic gallstone

Some indication for prophylactic Some indication for prophylactic
cholecystectmycholecystectmy
1. Gallstone > 3 cm1. Gallstone > 3 cm
2. Calcified ( porcelain ) gallbladder2. Calcified ( porcelain ) gallbladder
3. Gallbladder polyp > 1 cm3. Gallbladder polyp > 1 cm
4. 4. SplenectomySplenectomy in hemolytic anemia patientin hemolytic anemia patient
5. 5. BariatricBariatric surgery surgery
6. Long term TPN6. Long term TPN
7. Transplant patient needed7. Transplant patient needed
immunosuppressive drug immunosuppressive drug
8. No access to medical care8. No access to medical care

Chronic Chronic cholecystitischolecystitis

Recurrent attack of Recurrent attack of biliarybiliary colic from colic from
recurrent cystic obstruction (from stone)recurrent cystic obstruction (from stone)
Aggravate by fatty meal/supine position Aggravate by fatty meal/supine position
when sleepwhen sleep
Diagnosis : Diagnosis : USUS
Clinical manifestationClinical manifestation
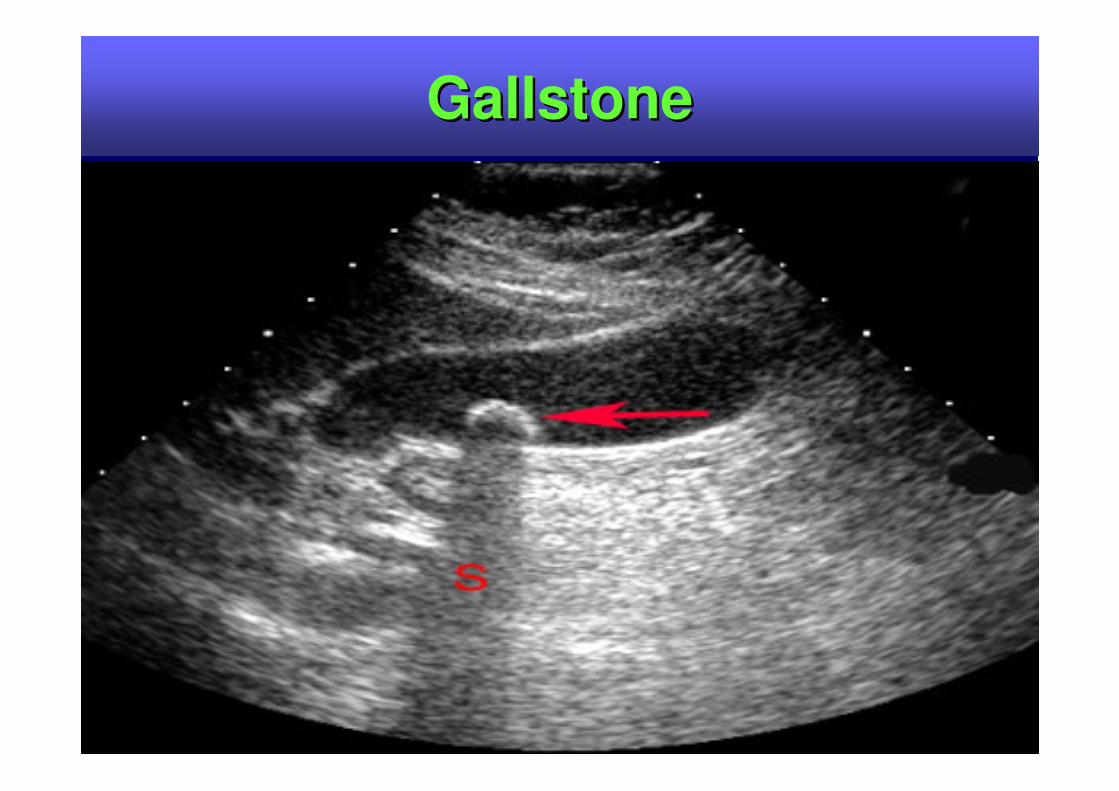
GallstoneGallstone

Procedure of choice :Procedure of choice :
Laparoscopic Laparoscopic cholecystectomycholecystectomy
TreatmentTreatment

Acute Acute cholecystitischolecystitis

-- Persistent cystic duct obstruction Persistent cystic duct obstruction leads to leads to
GB distension, wall inflammation & edemaGB distension, wall inflammation & edema
-- Can lead to: Can lead to: empyemaempyema, gangrene, rupture, gangrene, rupture

EpigastriumEpigastrium/RUQ pain /RUQ pain >24hr>24hr
Radiate to Radiate to interscapularinterscapular or or RtRt
scapular areascapular area
Anorexia, nausea/vomiting and fever Anorexia, nausea/vomiting and fever
Palpable/tender or even Palpable/tender or even visiblevisible RUQ massRUQ mass
Positive Murphy's signPositive Murphy's sign
( ( inspiratoryinspiratory arrest with deep palpation in the right arrest with deep palpation in the right subcostalsubcostal area) area)
Clinical manifestationClinical manifestation

LabLab : :
Moderate Moderate leucocytosisleucocytosis
(WBC 12,000(WBC 12,000--15,000 cells/mm3) 15,000 cells/mm3)
If WBC > 20,000 cells/mm3 : complicated If WBC > 20,000 cells/mm3 : complicated
cholecystitischolecystitis
Mild abnormal LFT, jaundice Mild abnormal LFT, jaundice no more than 4 no more than 4
mg/dlmg/dl

Study of choice = Study of choice = USUS
Gallstones, Gallstones, sonographicsonographic MurphyMurphy’’s signs sign
gallbladder wall thickening, distended gallbladder wall thickening, distended
gallbladder, gallbladder, pericholecysticpericholecystic fluidfluid
DiagnosisDiagnosis


-- NPONPO
-- IV fluid resuscitationIV fluid resuscitation
-- IV ATB cover gram IV ATB cover gram negneg aerobe/anaerobeaerobe/anaerobe
(3(3rdrd generation generation cephalosporinscephalosporins with good with good
anaerobic coverage or 2anaerobic coverage or 2ndnd generation generation
cephalosporinscephalosporins plus plus metronidazolemetronidazole))
TreatmentTreatment
Every patients must surgery Every patients must surgery except except
medically unfit patientsmedically unfit patients
Timing of surgeryTiming of surgery
Early VS. delayed Early VS. delayed cholecystectomycholecystectomy
(early = (early = SxSx in 3 days, in 3 days,
delayed = delayed = SxSx in 6in 6--10 wks after disease)10 wks after disease)

If patients present If patients present within 3 dayswithin 3 days of onset prefer of onset prefer
early early cholecystectomycholecystectomy
If patients present If patients present > 3 days> 3 days of onset prefer of onset prefer
delayed delayed cholecystectomycholecystectomy except in except in unresponseunresponse
to ATB or complicated to ATB or complicated cholecystitischolecystitis
Medically unfit patientsMedically unfit patients considerconsider
cholecystostomycholecystostomy and delayed and delayed cholecystectomycholecystectomy
if patients recover and fit for surgeryif patients recover and fit for surgery
CholedocholithiasisCholedocholithiasis

66--12% of gallstone patients12% of gallstone patients
Classified intoClassified into
(1) Primary CBD stone(1) Primary CBD stone
(2) Secondary CBD stone(2) Secondary CBD stone

Obstructive jaundice, Obstructive jaundice, cholangitischolangitis, gallstone , gallstone
pancreatitispancreatitis
Clinical manifestationClinical manifestation

LFTLFT : direct : direct hyperbilirubinemiahyperbilirubinemia, elevated , elevated
ALP ALP
USUS : CBD obstruction, proximal BD: CBD obstruction, proximal BD
dilatationdilatation
DiagnosisDiagnosis

Sensitivity Specificity AccuracySensitivity Specificity Accuracy
TUSTUS 2020--80% 80% 95%95%
CT CT 2323--85% 85% 95% 95% 71% 71%
ERCP ERCP 7979--95% 95% 9292--100% 100% 97%97%
MRCPMRCP 7171--100% 100% 9393--100% 100%
EUSEUS 8888--96% 96% 9696--100% 100% 95%95%
IOC IOC 93.5% 93.5% 93.3%93.3%
DiagnosisDiagnosis



CholangitisCholangitis

PathogenesisPathogenesis
BacteribiliaBacteribilia + + intraductalintraductal hypertensionhypertension

MicrobiologyMicrobiology
Escherichia coliEscherichia coli
KlebsiellaKlebsiella pneumoniaepneumoniae
Streptococcus Streptococcus faecalisfaecalis
BacteroidesBacteroides fragilisfragilis

1.Fever with chills1.Fever with chills
2.RUQ pain2.RUQ pain
3.Jaundice3.Jaundice
��CharcotCharcot’’s triads triad
5% of patients = acute toxic 5% of patients = acute toxic cholangitischolangitis
(Charcot(Charcot’’s triad + hypotension + mental s triad + hypotension + mental
status change = status change = ReynoldReynold’’ss pentadpentad))
Clinical manifestationClinical manifestation

CBC : CBC : leucocytosisleucocytosis
LFT : LFT : hyperbilirubinemiahyperbilirubinemia, elevation of ALP and , elevation of ALP and
transaminasestransaminases
Initial imaging : US Initial imaging : US
Definite diagnosis :Definite diagnosis : ERC or PTCERC or PTC
If suspected cancer : CT or MRIIf suspected cancer : CT or MRI
DiagnosisDiagnosis

-- NPONPO
-- IV fluid resuscitationIV fluid resuscitation
-- IV ATBIV ATB
-- ERCP with drainage or PTBDERCP with drainage or PTBD
ATC : emergency ATC : emergency biliarybiliary drainagedrainage
TreatmentTreatment

Malignant neoplasm Malignant neoplasm

�� Gallbladder carcinomaGallbladder carcinoma
�� ExtrahepaticExtrahepatic cholangiocarcinomacholangiocarcinoma

Gallbladder carcinoma Gallbladder carcinoma

IncidenceIncidence
-- 55thth common GI cancercommon GI cancer
-- elderly ( > 70 yrs)elderly ( > 70 yrs)
-- F : M = 2F : M = 2--3 : 13 : 1
-- 7070--90 % +90 % +veve GSGS
-- < 0.5% GS +< 0.5% GS +veve GB cancerGB cancer
-- adenoadeno. CA.. CA. 90%90%

1) large GS > 3 cm1) large GS > 3 cm
2) calcified GB wall ( porcelain GB ) 2) calcified GB wall ( porcelain GB )
3) 3) choledochalcholedochal cystcyst
4) chronic inflammatory state : typhoid 4) chronic inflammatory state : typhoid
,,H.pyloriH.pylori
5) GB polyp > 1 cm5) GB polyp > 1 cm
6) anomalous 6) anomalous pancreaticobiliarypancreaticobiliary duct duct
junction ( APBDJ )junction ( APBDJ )
7) carcinogen : 7) carcinogen : azotolueneazotoluene , nitrosamine, nitrosamine
Risk factorsRisk factors

Porcelain gallbladderPorcelain gallbladder

CholedochalCholedochal cystcyst

SimilarSimilar cholecystitischolecystitis or or cholelithiasischolelithiasis
May May asymptomasymptom
2525--50% : jaundice50% : jaundice
50% of patients cannot 50% of patients cannot DxDx GB CA before GB CA before
surgerysurgery
Clinical manifestationClinical manifestation
Initial test : USInitial test : US
Imaging before Imaging before TxTx : MRCP: MRCP
CTCT
Tumor marker : CA 19Tumor marker : CA 19--99
PreopPreop tissue tissue DxDx : not necessary except : not necessary except
in advance CA before chemoin advance CA before chemo
DiagnosisDiagnosis

Gallbladder carcinomaGallbladder carcinoma

Tumor not beyond Tumor not beyond muscularismuscularis propriapropria
TTxx : : Simple Simple cholecystectomycholecystectomy
TreatmentTreatment

Tumor beyond Tumor beyond muscularismuscularis propriapropria but not but not
beyond beyond serosaserosa
TTxx : : Extended Extended cholecystectomycholecystectomy
(simple (simple cholcystecomycholcystecomy + segment IVb,5 + segment IVb,5
resection + regional resection + regional lymphadenectomylymphadenectomy))
TreatmentTreatment

Tumor perforate Tumor perforate serosaserosa, invade liver or , invade liver or
adjacent organsadjacent organs
TTxx :: Extended RT. Extended RT. HepatectomyHepatectomy
(IV(IV--VIII)VIII)
TreatmentTreatment

MetastaticMetastatic diseasesdiseases
TTxx : : palliation for pain or jaundicepalliation for pain or jaundice
(ERCP/PTBD)(ERCP/PTBD)
TreatmentTreatment

CholangiocarcinomaCholangiocarcinoma

Classified intoClassified into
1)1) HilarHilar : : KlatskinKlatskin’’ss tumor, 2/3tumor, 2/3
2)2) MiddleMiddle
3)3) LowerLower

CholestaticCholestatic jaundice (painless) jaundice (painless)
Clinical Clinical cholangitischolangitis
Anorexia, weight lossAnorexia, weight loss
Clinical manifestationClinical manifestation

Initial test : USInitial test : US
Imaging before Imaging before TxTx : MRCP: MRCP
CT + ERCP/PTCCT + ERCP/PTC
Tumor marker : CA 19Tumor marker : CA 19--99
PreopPreop tissue tissue DxDx : not necessary except : not necessary except
in advance CA before chemoin advance CA before chemo
DiagnosisDiagnosis

HilarHilar lesionlesion : Bismuth: Bismuth--CorletteCorlette
TreatmentTreatment

Type I bile duct resection Type I bile duct resection ±± segment 1segment 1
Type II bile duct resection Type II bile duct resection ++ segment 1segment 1
Type Type IIIaIIIa Rt. Rt. hepatectomyhepatectomy
Type Type IIIbIIIb Lt. Lt. hepatectomyhepatectomy
Type IV palliationType IV palliation
TreatmentTreatment

Middle lesion : major common bile duct Middle lesion : major common bile duct
resectionresection
Distal lesion : Whipple operationDistal lesion : Whipple operation
TreatmentTreatment

Approach to jaundiceApproach to jaundice

JaundiceJaundice
Jaundice
Prehepatic Hepatic Posthepatic
Jaundice
Unconjugated ConjugatedHyperbilirubinemia Hyperbilirubinemia
Jaundice
Hemolytic Hepatocellular Cholestatic

JaundiceJaundice
Medical jaundice Surgical jaundice

Symptoms/signs of surgical jaundiceSymptoms/signs of surgical jaundice
Jaundice with dark urine, pale stool and Jaundice with dark urine, pale stool and prurituspruritus
Abdominal painAbdominal pain
History of previous History of previous biliarybiliary tract surgerytract surgery
Abdominal mass/RUQ mass/CourvoisierAbdominal mass/RUQ mass/Courvoisier’’s law s law
LFT : direct LFT : direct hyperbilirubinemiahyperbilirubinemia, elevated ALP, elevated ALP
UA : Bile+, UA : Bile+, urobilinogenurobilinogen --

Suspicion surgical jaundice Suspicion surgical jaundice ��������
USUS then then
ERCP/PTCERCP/PTC


THANK YOUTHANK YOU