the journal of the irish practice nurses...
TRANSCRIPT

The Journal of the Irish Practice Nurses AssociationIssue 5 Volume 6 September/October 2013
RevIew Of GINA ASThmA GuIdelINeS IN STAble AdulT ASThmARuth Morrow
PRAcTIce NuRSeS’ quAlITy Of Ife
Lisa Nolan
The mANAGemeNT Of hyPeRTeNSION
Aoife Morris, Alma Murphy, and
Dr John Clarke
ROle Of The PN IN The NATIONAl cANceR cONTROl PROGRAmmeHilary Murphy
Are your patients at risk?
Pneumococcal DiseaseVaccinate your at-risk patients and those 65 years and over against serious pneumococcal disease.
08/12 IR00150b
age 65+
chronic lung, heart or renal
disease
weakenedimmunesystem
other at-risk groups*smoker
diabetes
Marketing authorisation holder: Sanofi Pasteur MSD Limited, Block A, Second Floor, Cookstown Court, Old Belgard Road, Tallaght, Dublin 24. Marketing authorisation number: PA 544/21/3 Legal category: POM
Information about adverse event reporting can be found at www.imb.ie. Adverse events and inadvertent vaccination during pregnancy should also be reported to Sanofi Pasteur MSD by calling 00 44 1628 785291.Further information is available on request or in the SPC.
* See Immunisation Guidelines for Ireland www.immunisation.ie
v is i t pneumo. ie
SPMSD1192 pneumovax reminder NIGP strip 90x210 v4.indd 1 27/09/2013 12:16

NEW
5 Hours
of learning...
Limited Offer
On-line Course
Ultimate Cholesterol Lowering Plan©
Available now & FREE to all Health Professionals
HEART UK – the UK’s cholesterol charity, has just launched its Ultimate Cholesterol Lowering Plan© (UCLP©)on-line course – AVAILABLE NOW to all health professionals.
The UCLP© course is a must for health professionals searching for a credible, practical and realistic step-by-stepapproach to helping all patients lower their cholesterol.
The UCLP© is HEART UK’s very own cholesterol-lowering plan developed with support from seven leading healthexperts and an education grant from Alpro UK Ltd.
The UCLP© course will take you step-by-step through the UCLP© process. Each module covers the scientificevidence and, more importantly, how these learnings translate into daily practice for when advising your patient.
Supported by an education grant from Alpro UK Ltd
Learn about the UCLP© and how to apply itin your everyday practice:
Step 1 - Motivational InterviewingStep 2 - Heart-healthy foundation dietStep 3 - The four cholesterol-busting foods
Refresh your heart health and cholesterolknow-how:
Heart health status of the nationCholesterol metabolism basicsHealth screening and lipid-lowering drugs
Take it at your own pace
www.heartuk.org.uk/uclp
Pause and resume the courseat your convenience
No time constraints
For your FREE access visit us now at:
UCLP A4 AD v2_210x297mm 08/08/2013 13:55 Page 1

1
editorial
PNs pivotal for the success of clinical care Programmes
An article in the Sunday Business Post (5th May 2013), The Patient Is Improving, outlined the improvements to patient care since the inception of the Clinical Care Programme. Firstly, the Stroke Programme states that more people who have a stroke are more likely to live than 3 years ago. Most hospitals now offer thrombolysis compared to only half of the hospitals offering it in
2009. Secondly, in relation to COPD, the length of stay of patients who experience an exacerbation has been reduced from 9.1 days in 2009 to 7.6 days in 2012 as a result of COPD Outreach teams being put in place as part of the COPD Clinical Care Programme. The COPD Outreach teams are designed to reduce the severity of COPD, stop patients smoking and manage co-morbidities such as osteoporosis, chronic muscle loss and heart disease. It was enlightening to see a positive article on the health service being published as its usually the negative stories that make the headlines.
Despite all the cuts in the health service, many of which were necessary, it is a challenging time, in a positive sense, to work in an area which is changing rapidly for the betterment of patient care. It is enlightening to see the recognition of primary care as being the more appropriate environment for the management of chronic conditions. However, if this transition is to be successful, resources need to be channelled into primary care. Practice nurses are ideally positioned to support chronic disease management but require ongoing education and support. The practice nurse workload is currently overloaded with little time for chronic disease management. Research has suggested that long term conditions are best managed by nurses with medical support. The HSE needs to look at supporting additional practice nurses to take on this additional workload if the outcomes of the clinical care programmes are to be achieved.
Annual conferenceIt’s IPNA Annual Conference and AGM time of year once again. This year the North Dublin Branch will host the conference in Athlone on 11th/12th October. The branch, who are not long in operation, have come up with a wide and varied conference programme entitled, Old Issues, New Ideas. The diverse nature of the conference illustrates perfectly the broad role the practice nurse plays in the practice. The conference opens on Friday afternoon with speakers on migrant women’s sexual and reproductive health, substance abuse in adolescence and substance abuse in pregnancy. The keynote speaker on Friday night is Mary Scott’s, Good Sexual History. Saturday topics include obesity and metabolism, hypertension and dermatology. In addition, the IPNA conference offers a prime opportunity for members and non-members to network, support and share experiences with each other. For new members, it gives a great opportunity to meet up with experienced practice nurses, some of whom have over 25 years experience behind them. For the more experienced practice nurse, it is an opportunity to continue developing and enhancing our professional development. The large pharmaceutical exhibition provides us with ample opportunity to keep abreast of new research and developments which gives us the knowledge to improve our practice and for the betterment of patient care.
See you in Athlone!
Ruth Morrow
NEW
5 Hours
of learning...
Limited Offer
On-line Course
Ultimate Cholesterol Lowering Plan©
Available now & FREE to all Health Professionals
HEART UK – the UK’s cholesterol charity, has just launched its Ultimate Cholesterol Lowering Plan© (UCLP©)on-line course – AVAILABLE NOW to all health professionals.
The UCLP© course is a must for health professionals searching for a credible, practical and realistic step-by-stepapproach to helping all patients lower their cholesterol.
The UCLP© is HEART UK’s very own cholesterol-lowering plan developed with support from seven leading healthexperts and an education grant from Alpro UK Ltd.
The UCLP© course will take you step-by-step through the UCLP© process. Each module covers the scientificevidence and, more importantly, how these learnings translate into daily practice for when advising your patient.
Supported by an education grant from Alpro UK Ltd
Learn about the UCLP© and how to apply itin your everyday practice:
Step 1 - Motivational InterviewingStep 2 - Heart-healthy foundation dietStep 3 - The four cholesterol-busting foods
Refresh your heart health and cholesterolknow-how:
Heart health status of the nationCholesterol metabolism basicsHealth screening and lipid-lowering drugs
Take it at your own pace
www.heartuk.org.uk/uclp
Pause and resume the courseat your convenience
No time constraints
For your FREE access visit us now at:
UCLP A4 AD v2_210x297mm 08/08/2013 13:55 Page 1

2
Issue 5 Volume 2 September / October2009
ContentsThe Journal of the Irish Practice Nurses Association
Issue 5 Volume 6 September / October 2013
Nursing in General Practice is published by GreenCross Publishing Ltd., 7 Upper Leeson Street, Dublin 4. Tel: 01 4410024 Fax: 01 547 2388Email: [email protected]
DisclaimerThe views expressed in Nursing in General Practice are not necessarily those of the publishers, editor or editorial advisory board. While the publishers, editor and editorial advisory board have taken every care with regard to accuracy of editorial and advertisement contributions, they cannot be held responsible for any errors or omissions contained.
*GreenCross Publishing was established in 2007 and is jointly owned by Graham Cooke and Maura Henderson.
© Copyright GreenCross Publishing Ltd. 2013The contents of Nursing in General Practice are protected by copyright. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form by any means – electronic, mechanical or photocopy recording or otherwise – whole or in part, in any form whatsoever for advertising or promotional purposes without the prior written permission of the editor or publishers
1 edITORIAl
4 NewS
8 bRANch NewS
RevIewS
10 The mANAGemeNT Of hyPeRTeNSION Aoife morris, Alma murphy, and dr John clarke
15 RevIew Of GINA ASThmA GuIdelINeS IN STAble AdulT ASThmA Ruth morrow
20 ROle Of The PN IN The NATIONAl cANceR cONTROl PROGRAmme hilary murphy
TRAINING
25 uNdeRSTANdING ANd SuPPORTING cOuPle RelATIONShIPS dr maeve hurley
24 ANNuAl cONfeReNce AGeNdA
27 TechNOlOGy
PRAcTIce NuRSeS’ quAlITy Of Ife lisa Nolan
meeTING RePORT
30 fOuR TyPeS Of ASThmA PATIeNT
32 AbSTRAcTS
34 PROducTS
37 cROSSwORd
EDITORMaura Henderson
CONSulTING EDITORSDarina lane and Ruth Morrow
DESIGNERBarbara Vasic
PuBlISHERSGraham CookeMaura Henderson

Over 350 million patients treated with Clexane worldwide2
NOT ACTUAL SIZE
Clear visibility of expiry date
Colour-coded labelling and clear identification of CLEXANE® syringes by dose
Needle completely covered by the protection cap immediately after the injection
Automatic release of the safety mechanism when the plunger is fully depressed
Clear product identification
Designed to
protect against
needle stick
injuries1
References:1. CLEXANE® Summary of Product Characteristics. sanofi 2. Sanofi IMS data on file April 2012
CLEXANE® CONFIDENCE AT YOUR FINGERTIPS
New Clexane® and Clexane® Fortesafety lock syringes
CLEXANE® SYRINGES AND CLEXANE® FORTE SYRINGES PRESCRIBING INFORMATIONPresentation: Clear, colourless to pale yellow solution of either 100mg enoxaparin per 1ml (anti-factor Xa activity of 10,000IU/ml with reference to the WHO First International LMW Heparin Reference Standard) or 150mg enoxaparin per 1ml (anti-factor Xa activity of 15,000IU/ml). Clexane® Syringes: single dose pre-filled syringes containing either: 20mg enoxaparin in 0.2ml (2,000IU), 40mg enoxaparin in 0.4ml (4,000IU), 60mg enoxaparin in 0.6ml (6,000IU), 80mg in 0.8ml (8,000IU) or 100mg in 1ml (10,000IU). Clexane® Forte Syringes: single dose pre-filled syringes containing either: 120mg enoxaparin in 0.8ml (12,000IU) or 150mg in 1ml (15,000IU). Indications: Prophylaxis of thromboembolic disorders of venous origin, in particular those associated with orthopaedic or general surgery and in medical patients bedridden due to acute illness. Treatment of venous thromboembolic disease presenting with deep vein thrombosis, pulmonary embolism or both. Treatment of unstable angina and non-Q-wave myocardial infarction, administered concurrently with aspirin. Prevention of thrombus formation in the extracorporeal circulation during haemodialysis. Clexane 100mg/ml syringes only: Treatment of acute ST-segment Elevation Myocardial Infarction (STEMI) including patients to be managed medically or with subsequent Percutaneous Coronary Intervention (PCI) in conjunction with thrombolytic drugs (fibrin or non-fibrin specific). Dosage & Administration: Prophylaxis: Patients with low to moderate risk of thromboembolism, e.g. general surgery, recommended dose of Clexane® is 20mg (2,000IU) once daily subcutaneously. Clexane® should be continued for 7 to 10 days or until risk of thromboembolism has diminished. Longer durations may be appropriate in some patients following hip replacement. Patients undergoing surgery, initial dose approximately 2 hours preoperatively. Patients with high risk of venous thromboembolism, e.g. orthopaedic surgery, the recommended dose is 40mg (4,000IU) once daily subcutaneously, initial dose being given approximately 12 hours preoperatively. Medical patients bedridden due to acute illness, the recommended dose is 40mg (4,000IU) once daily for a minimum of 6 days until return to full ambulation, for a maximum of 14 days. Longer durations may necessary if it is there is an ongoing significant risk of thromboembolic events beyond 14 days. Treatment: Subcutaneous administration either as a single injection of 1.5mg/kg (150 IU/kg) or as a twice daily injection of 1 mg /kg (100 IU/kg) usually for 5 days and until adequate oral anticoagulation is established. Unstable angina and non-Q-wave myocardial infarction recommended dose is 1mg/kg (100IU/kg) every 12 hours subcutaneously, administered concurrently with oral aspirin 100 to 325mg once daily. Treatment should be for minimum of 2 days and continued until clinical stabilisation, usual duration 2 to 8 days. Clexane 100mg/ml syringes only: Treatment of STEMI, the recommended dose is a single IV bolus of 30mg, plus a 1mg/kg SC dose followed by 1mg/kg administered SC every 12 hours (max 100mg for the first two doses only, followed by 1mg/kg dosing for the remaining doses) for 8 days or until hospital discharge, whichever comes first. For dosage in patients ≥75 years of age, see elderly section. When used with a thrombolytic (fibrin specific or non-fibrin specific) Clexane® should be given between 15 minutes before and 30 minutes after the start of fibrinolytic therapy. All patients should receive aspirin 75 to 325mg once daily unless contraindicated. For patients managed with PCI: If the last Clexane® SC administration was given less than 8 hours before balloon inflation, no additional dosing is needed. If the last SC administration was given more than 8 hours before balloon inflation, an IV bolus of 0.3mg/kg of Clexane® should be administered. During haemodialysis: 1mg/kg (100IU/kg) Clexane® introduced into arterial line of the circuit at beginning of dialysis. This dose is usually sufficient for a 4 hour session. If fibrin rings are found, e.g. after a longer session, a further 0.5 to 1mg/kg (50 to 100IU/kg) may be given. In patients with high risk of haemorrhage reduce the dose to 0.5mg/kg (50IU/kg) (double vascular access) or 0.75mg/kg (75IU/kg) (single vascular access). Elderly: Clexane 100mg/ml syringes only: For treatment of STEMI in patients ≥75 years of age, do not use an initial IV bolus. Initiate dosing with 0.75mg/kg SC every 12 hours (maximum 75mg for the first two doses only, followed by 0.75mg/kg dosing for the remaining doses). For other indications, no dosage adjustment necessary unless kidney function is impaired. Children: Not recommended. Renal impairment: Dosage adjustment required for patients with severe renal impairment. Contraindications: Acute bacterial endocarditis; active major bleeding and conditions with a high risk of uncontrolled haemorrhage, including recent haemorrhagic stroke or subdural haematoma; thrombocytopenia in patients with positive in vitro aggregation test in presence of Clexane®; in jaundice; active gastric/duodenal ulcer; hiatal ulceration; threatened abortion or retinopathy; hypersensitivity to enoxaparin, heparin or other LMWH. Warnings and Precautions: Clexane® must not be administered by the intramuscular route. Different low
molecular weight heparins may not be equivalent; alternative products should not be substituted during therapy. Neuraxial haematomas may occur when Clexane® is used concomitantly with spinal/epidural anaesthesia. Haemodynamically unstable patients with pulmonary embolism may require alternative treatment. Use in patients with prosthetic heart valves has not been adequately studied and is not recommended. Clexane® should be used with care in hepatic insufficiency, history of thrombocytopenia, and conditions or patients with increased bleeding potential (such as those with peptic ulcers, recent ischaemic stroke, uncontrolled severe arterial hypertension, diabetic retinopathy, renal impairment, elderly and extremes of weight). Platelet counts should be measured prior to initiation of Clexane® and regularly during treatment. Heparins can suppress adrenal secretion of aldosterone leading to hyperkalaemia. Following vascular instrumentation adhere precisely to recommended dose intervals. If a closure device is used, the sheath can be removed immediately. If a manual compression method is used, sheath should be removed 6 hours after the last IV/SC enoxaparin sodium injection. If treatment is to be continued, the next scheduled dose should be given no sooner than 6 to 8 hours after sheath removal. The site of the procedure should be observed for signs of bleeding or haematoma formation. Pregnancy: Clexane® should be used during pregnancy only if the physician has established a clear need. Lactation: Advise avoidance of breast-feeding. Interactions: Discontinue unless essential agents affecting haemostasis, e.g. oral anticoagulants, thrombolytics, systemic glucocorticoids, NSAIDs, aspirin, clopidogrel. If the combination cannot be avoided, careful clinical and laboratory monitoring is recommended. Adverse Reactions: Bleeding, including retroperitoneal and intracranial, with or without the presence of associated risk factors, such as invasive procedures or use of medications affecting haemostasis. Thrombocytopenia, including rare cases of immuno-allergic thrombocytopenia with thrombosis. Elevation of liver enzyme levels and platelet count, and cutaneous or systemic allergic reactions (including anaphylactic/anaphylactoid reactions, and very rarely cutaneous vasculitis) have been reported. At site of injection: pain, haematoma, irritation, rarely hard inflammatory nodules and skin necrosis. Heparins can cause hypoaldsteronism which can increase in plasma potassium, and rarely, clinically significant hyperkalaemia. Rare reports of neuraxial haematoma when using spinal/epidural anaesthesia and post-operative indwelling catheter. Please consult SPC for full details of the recognised side effects with Clexane. Pharmaceutical Precautions: Do not mix with other injections or infusions. Do not store above 25°C. Do not refrigerate or freeze. PI revision: November 2012Product Licence numbers: PA 540/97/1: Clexane® Syringes; PA 540/97/2: Clexane® Forte Syringes.Legal category: POMMarketing Authorisation Holder: Sanofi-Aventis Ireland Ltd., Citywest Business Campus, Dublin 24, Ireland.Further information is available from: Sanofi 18 Riverwalk, Citywest Business Campus, Dublin 24 or contact [email protected] Tel.: (01) 4035600.
References:1. CLEXANE® Summary of Product Characteristics. sanofi 2. sanofi Data on file April 2012
Please refer to the Summary of Product Characteristics which can be found on IPHA @ http://www.medicines.ie/ before prescribing.
Information about adverse event reporting can be found at www.imb.ie Adverse events should be reported to the Sanofi Drug Safety Department
GBIE.ENO.13.06.01 Date of preparation July 2013
RRD01246 Clexane Sanofi A4 Ad_V6 (Resized).indd 1 8/8/13 3:00 PM

4
newsNEC NEwS
IPNA AwARdS 2013The following awards will be presented at the IPNA Conference on 11th-12th October.Practice Nurse of the Year 2013.Valerie Mangan IPNA loyalty Award 2013.IPNA Clinical Award 2013 (ESC CVD Prevention Guidelines 2012).
IPNA ANNuAl educATIONAl cONfeReNce/AGm 2013Friday 11th/Saturday 12th October in the Radisson Blu Hotel, Athlone; hosted by the IPNA North Dublin Branch. Theme: Old Issues –New Ideas. For more information and programme please see the IPNA website.Closing date for registrations is Friday 20th September 2013Exhibitor queries can be e-mailed to [email protected] AGM will take place on Saturday 12th October at 2.30pm.
Nec meeTINGS 2013 Friday 11th October 2013, 5-6pm, Radisson Blu Hotel, Athlone.
IPNA webSITeThe IPNA website, www.irishpracticenurses.ie is updated constantly, so please log in regularly to get the latest news on study days, education, new comments in the Discussion boards and more. You will also find IPNA Policies, Articles of Association and Minutes of all NEC meetings to date in the Members Area.
IPNA ON TwITTeRIf you have a Twitter account you can follow the handle @PracticeNurses to receive IPNA news, reminders and useful information that is retweeted from other groups – directly to your timeline.
lisa Nolan, IPNA Administrator Tel: 042-9692403 email: [email protected]
SUAS: new ankylosing spondylitis exercise app The Ankylosing Spondylitis Association of Ireland (ASAI) recently launched SUAS (Supporting and understanding Ankylosing Spondylitis) – a new iPhone application to support the 1 in 200 people in Europe currently living with Ankylosing Spondylitis (AS).
The SUAS app, developed in partnership with the waterford Regional Hospital Rheumatology team and supported by Pfizer Healthcare Ireland, is the first of its kind in Ireland and provides AS patients with educational information, guided exercise videos and the ability to monitor their progress over time.
The SUAS app is designed to support and empower patients take charge of their condition. As a flexible, on-the-go tool, SUAS helps those living with AS learn about all aspects of their condition while also teaching daily exercise techniques”
“In addition to providing information on all the frequently asked questions in relation to living with AS, SUAS users will also be prompted to take the BASFI test [Bath Ankylosing Spondylitis Functionality Index], to determine their degree of functional limitation and chart their ‘score’ over time as they exercise and improve strength and flexibility. They can keep a record of this to discuss with their healthcare professional to better inform their treatment regimen,” continued Dr Sheehy.
The app also contains support information and tips for those living with AS to manage key aspects of daily life, including condition symptoms, maintaining posture, working with AS and daily lifestyle.
Seoirse Smith, Secretary of the ASAI said: “whether you have AS or not, it can be difficult to stay motivated to exercise and know what the best exercises for you are. SUAS contains information on activities from walking to Pilates and has a library of over 30 guided exercises, shaped by healthcare professionals, to ensure people know what exercises can and should be done…and more importantly, how to do them. This allows people with AS to actively manage their condition
through a diverse range of guided exercises, ensuring they remain active between visits to their healthcare professionals.”
The free SUAS – Supporting and understanding Ankylosing Spondylitis iPhone application is part of a newly-developed suite of support and information resources for patients living with AS and is available to download from the iTunes store. In addition to the SUAS app, an educational booklet has also been developed, as well as an updated patient site, www.ankylosing-spondylitis.ie.
dr claire Sheehy of waterford Regional hospital with Nathan hennessy and Seoirse Smith, Secretary of the ASAI

5
newsA quarter of people would get the pneumococcal vaccination if recommended by their GPRTE radio presenter Ronan Collins was joined by five patient organisations to encourage those at risk, including those over 65, to get vaccinated from pneumococcal disease. Only 16% of over 65s indicated that they received the vaccination which suggests that over 400,000 people over 65 could be at risk of contracting pneumonia, meningitis or septicaemia.
Research conducted by Millward Browne, on behalf of Sanofi Pasteur MSD, to coincide with the ‘Seven Reasons You Should Know Pneumo’ health promotion campaign shows that only 46% of Irish people have heard of pneumococcal disease and 89% indicated they have never been vaccinated1 even though a vaccine is readily available from GPs. The research suggests that the GP’s recommendation is a key influence as almost half of those vaccinated say it was due to their doctor’s advice. A recent study indicated that proactive contact about the pneumo vaccine from the GP office to at risk patients promotes better awareness and increased participation in the vaccination process.
The broadcaster – who has diabetes,
putting him in the at risk group for the pneumo bug – helped launch Sanofi Pasteur MSD’s campaign, joining representatives from five different patient organisations.
This year the existing coalition of Diabetes Ireland, Asthma Society of Ireland, Age Action and the Irish Patients’ Association has been bolstered by the addition of Meningitis Research Foundation.
Ronan Collins said, “I’m very proud to support this campaign for a second year. we need to get the word out that pneumococcal is a serious condition that can be avoided by getting a vaccine from a GP. The fact that five different groups are involved in this campaign really highlights the fact that
pneumococcal disease affects such a large part of our society.
“Only a third of people have actually heard of the pneumococcal vaccine so I’m hoping that this campaign will drive the message home and raise awareness amongst the Irish public. If you are at risk, or you know some who is, then a vaccination should be your top priority.”
bon Secours hospital cork host Practice Nurse conferenceThe first annual Practice Nurse Conference was hosted by Bon Secours Hospital Cork in the River lee Hotel on Saturday 21st September.
The aim of the Practice Nurse conference hosted by Bon Secours Hospital Cork recently was to acknowledge the vitally important role that the Practice Nurse plays within the GP Surgery. The conference programme was devised to comple-ment the successful and long-running GP Study Day which is hosted annually by the Bon Secours hospital. The conference was accredited by An Bord Altranais (8 CEus) and was very well attended.
Ms Ber Mulchay, Director of Nursing, opened the conference with an informative talk which highlighted the importance of maintaining good links between the hospital and those working in the community. Ms Mulcahy was followed by guest speaker, Professor Josephine Hegarty from university College Cork, who mapped the history of nursing from its beginnings in the 19th century up to the present day. Professor Hegarty also emphasised the need for continuing education for nursing practitioners.
Participants had the opportunity to attend 10 education ses-sions throughout the day which were delivered by Nurse Spe-cialists and members of the multi-disciplinary team. Delegates also had the opportunity to meet with the various speakers on a one-to-one basis, outside of the formal conference setting.
mary connor, cardiac Nurse, mary ford, Practise development co-ordinator, Ann mccarthy, Rapid Access chest Pain Nurse, Sr. marie cuffe, harry canning, hospital manager, dr. Josephine hegarty, Professor of Nursing in ucc, and ber mulcahy, director of Nursing, bon Secours cork, pictured at the bon Secours hospital Practise Nurse conference in the River lee hotel in cork city.

6
newsNew guide launched to empower patients with chronic kidney disease
A new guide is now available to aid patients in Ireland who have been diagnosed with chronic kidney disease to assist them in understanding and taking control of their illness thereby protecting their remaining kidney function, overall general health and quality of life.
The guide, sponsored by the global biopharmaceutical company AbbVie, is a collaboration between the Irish Kidney Association and Consultant Nephrologist Professor Austin Stack, Chairman of Medicine at university Hospital limerick and Graduate Entry Medical School, university of limerick. The book entitled ‘living with Chronic Kidney Disease – A Guide for Patients’ was launched by Prof. Austin Stack at the Irish Kidney Association’s Renal Support Centre, Beaumont Hospital.
Speaking about the book Prof. Stack said, “This new addition to the Irish Kidney Association kidney book series will be a fantastic reservoir of knowledge and advice for our patients in Ireland. The Guide will not only enlighten and inform patients who have been diagnosed with kidney disease in our community; it will also empower them to better manage their overall kidney health.”
Mark Murphy, the Chief Executive of The Irish Kidney Association said, “we are pleased that a resource gap which specifically targets recently diagnosed kidney patients with CKD has now been filled with this comprehensive book. we hope that it will help patients come to terms with and take control of their silent disease, improving their health outcome to prolong their overall quality of life. This practical guide explains the medical terms surrounding CKD as well as the benefits of early intervention. It lays out simple steps to ensure the best possible outcome with advice on nutrition, overall physical and emotional health and medication. It will also inform patients on other conditions, such as diabetes, obesity, high blood pressure and heart disease, which can be a catalyst for kidney disease and vice versa.”
At the launch of living with chronic Kidney disease – A Guide for Patients which took place at the Irish Kidney Association’s Renal Support centre at beaumont hospital were: mr. mark murphy, chief executive Irish Kidney Association; dr. michelle costello Smith, medical director in Ireland for biopharmaceutical company Abbvie limited; and Prof. Austin Stack, chairman of medicine at the university hospital limerick and Graduate entry medical School, university of limerick.
word of mouth offers support to patients with mouth cancerTo mark National Mouth Cancer Awareness Day which takes place on 18th September, the School of Dental Science at Trinity College Dublin launched a book of memoirs, thoughts and advice from mouth, head and neck cancer survivors and healthcare professionals involved in their care. The book is entitled Word of Mouth – Coping with and Surviving Mouth, Head and Neck Cancers.
Word of Mouth includes both professional healthcare advice and stories from people with direct experience of diagnosis, treatment and recovery. Full of accessible, humorous, poignant, practical and inspiring advice and suggestions, it is particularly relevant for people who have been diagnosed with mouth, head and neck cancers and their families and is designed to help them to understand and cope with their own diagnosis, treatment and recovery.
“It is possible to be happy and live a good life even with the concerns that come with a diagnosis. I like to think of it this way: even without cancer I would have had other things to worry about. I like to think that at the very least the quality of my worries has improved.” Edward Naessens, a contributor to Word of Mouth – Coping with and Surviving Mouth, Head and Neck Cancers.
There are more than 300 cases of cancer of the mouth (oral cavity and pharynx) reported in Ireland every year. The incidence is growing, especially among younger people; yet many people only hear about these diseases for the first time when they get their own diagnosis. The stories in the book are written by men and women, young and old and reflect the varied profile of people who have been affected by these cancers.
Speaking about the book, Dr Denise MacCarthy, Associate Professor in Restorative Dentistry at the School of Dental Science, and one of the editors of Word of Mouth said, “It has been a privilege to work on this project, with the authors of the memoirs, the professionals who provide care and the inimitable Molar Rollers. I hope the information therein will be of practical use.”
cystic fibrosis e-learning website launched
Irish healthcare professionals working with CF patients now have access to the latest expert-led CF meeting content through a dedicated e-learning platform, www.expertviewpoints.org.
users of the website, which showcases content from a variety of CF meetings, can follow the presentations flexibly and at their own pace. There is also the opportunity to earn up to 2 CPD points, awarded by the Royal College of Physicians, london.
The website was launched in Ireland at the first ever Irish Expert viewpoints in cystic fibrosis meeting, held at the Royal College of Physicians of Ireland in Dublin on wednesday 3 July 2013.
The educational meeting was attended by over 70 CF healthcare professionals from centres across Ireland, and featured topical presentations by an expert faculty, which included, among others, Prof Charles Gallagher and Dr Ed McKone from St Vincent’s university Hospital, and Dr Barry Plant from Cork university Hospital.

Over 20 years and 3 million patient-years collective clinical experience 9,10
Enbrel (etanercept) Abbreviated Prescribing Information
Before prescribing Enbrel® please refer to full Summary of Product Characteristics (SmPC). Presentation: Enbrel Pre-filled Syringe: Enbrel 25 mg and 50 mg solution for injection in pre-filled syringe. Each pre-filled syringe contains either 25 mg or 50 mg etanercept. Enbrel Pre-filled Pen (MYCLIC®): Enbrel 50 mg solution for injection in pre-filled pen. Each pre-filled pen contains 50 mg etanercept. Enbrel Powder: Enbrel 25 mg powder and solvent for solution for injection. Each vial contains 25 mg etanercept and each pre-filled syringe contains 1 ml water for injections. Enbrel Paediatric: Enbrel 10 mg powder and solvent for solution for injection for paediatric use. Each vial contains 10 mg etanercept and each pre-filled syringe contains 1 ml water for injections.
Uses: Adults: Moderate to severe active rheumatoid arthritis (RA), in combination with methotrexate, when response to disease-modifying anti-rheumatic drugs DMARDs, including methotrexate (unless contraindicated), has been inadequate. Enbrel can be given as monotherapy in the case of intolerance to methotrexate or when continued treatment with methotrexate is inappropriate. Severe, active and progressive RA without prior methotrexate treatment.
Enbrel alone or with methotrexate has been shown to reduce the rate of progression of joint damage measured by X-ray and to improve physical function. Patients with moderate to severe plaque psoriasis (PP) who failed to respond to, or who have a contraindication to, or are intolerant to other systemic therapy including ciclosporine, methotrexate or PUVA. Active and progressive psoriatic arthritis (PsA) when response to DMARDs has been inadequate. Enbrel has been shown to improve physical function in PsA patients, and to reduce the progression rate of peripheral joint damage as measured by X-ray in patients with polyarticular symmetrical subtypes of PsA. Severe active ankylosing spondylitis (AS) when response to conventional therapy has been inadequate. Children aged 2-17 years: Juvenile idiopathic arthritis (JIA). Polyarthritis (rheumatoid factor positive or negative) and extended oligoarthritis from the age of 2 years when inadequate response to, or intolerant of methotrexate. Psoriatic arthritis from the age of 12 years when inadequate response to, or intolerant of methotrexate. Enthesitis-related arthritis from the age of 12 years when inadequate response to, or intolerant of, conventional therapy. Children aged 6-17 years: Chronic severe psoriasis when inadequately controlled by, or intolerant to, other systemic therapies or phototherapies. Dosage: By subcutaneous injection. Adults: RA – 25 mg twice weekly or 50 mg once weekly PP – 25 mg twice weekly or 50 mg once weekly for up to 24 weeks, or 50 mg twice weekly for up to 12 weeks followed by 25 mg twice weekly or 50 mg once weekly for a further 12 weeks if needed. Continuous therapy may be appropriate for some adult patients. Discontinue if no response after 12 weeks. For re-treatment: 25 mg twice weekly or 50 mg once weekly for up to 24 weeks. AS and PsA – 25 mg twice weekly or 50 mg once weekly. Children aged 2-17 years: JIA – 0.4 mg/kg (maximum per dose 25 mg) twice weekly with an interval of 3 - 4 days or 0.8 mg/kg (maximum per dose 50 mg) once weekly. Discontinuation of treatment should be considered in patients who show no response after 4 months. Children aged 6-17 years: Plaque psoriasis in children aged 6-17 years – 0.8 mg/kg (maximum per dose 50 mg) once weekly for up to 24 weeks. Discontinue if no response after 12 weeks. For re-treatment: 0.8 mg/kg (maximum per dose 50 mg) once weekly for up to 24 weeks. Contra-indications: Hypersensitivity to any of the ingredients, sepsis or risk of sepsis, active infections. Warnings and Precautions: Enbrel should be initiated and supervised by specialist physicians experienced in the diagnosis and treatment of RA, JIA, PsA,
AS, PP or Paediatric PP. Patients treated with Enbrel should be given the Patient Alert Card. Use carefully in patients predisposed to, or with history of, infection due to underlying diseases other than RA (e.g. advanced or poorly controlled diabetes) or with history of blood dyscrasias, pre-existing or predisposition to demyelinating disease or congestive heart failure. Cases of active tuberculosis have been reported, therefore all patients should be evaluated for both active and inactive TB prior to being treated with Enbrel. If active TB is diagnosed, Enbrel should not be initiated. Caution should be used when administering Enbrel to patients identified as carriers of hepatitis B virus and there have been reports of worsening hepatitis C in patients receiving Enbrel. Use with caution in patients with a history of hepatitis C. Whether treatment with Enbrel might influence the development and course of active and/or chronic infections is unknown. Concurrent administration of Enbrel and anakinra has been associated with increased risk of serious infections and neutropenia, and is therefore not recommended. In clinical studies, concurrent administration of abatacept and Enbrel resulted in increased incidences of serious adverse events, and is therefore not recommended. Use caution when considering combination therapy with DMARDs other than methotrexate. Reports of various malignancies have been received in the post-marketing period, therefore with current knowledge, a possible risk for the development of lymphomas, leukaemia or other haematopoietic or solid malignancies in patients treated with a TNF-antagonist cannot be excluded. Malignancies, some fatal, have been reported among children, adolescents and young adults (up to 22 years of age) treated with TNF-antagonists (initiation of therapy ≤ 18 years of age) in the postmarketing setting. Melanoma and non-melanoma skin cancer (NMSC) have been reported in patients treated with TNF-antagonists, including Enbrel. Post-marketing cases of Merkel cell carcinoma have been reported very infrequently in patients treated with Enbrel. Periodic skin examination is recommended for all patients, particularly those with risk factors for skin cancer. Enbrel has not been studied in combination with other systemic therapies or phototherapy for the treatment of psoriasis. Monitor closely if patient develops new infection during treatment. Discontinue treatment if serious infection or allergic reaction develops or if blood dyscrasias are confirmed. Caution should be used in patients who have moderate to severe alcoholic hepatitis and Enbrel should not be used in patients for the treatment of alcoholic hepatitis. Discontinue temporarily if significantly exposed to varicella virus. Live vaccines should not be given concurrently with Enbrel. Paediatric patients should have received all vaccines recommended in current immunization guidelines prior to starting Enbrel. Treatment with Enbrel may result in the formation of autoantibodies. Enbrel is not recommended for use in patients with Wegener’s granulomatosis. There have been reports of hypoglycaemia in Enbrel patients receiving medication for diabetes, necessitating a reduction in antidiabetic medication in some of these patients. There have been reports of Inflammatory Bowel Disease (IBD) and uveitis in JIA patients being treated with Enbrel. Caution should be exercised when treating the elderly and with particular attention to occurrence of infections. Pregnancy & Lactation: Enbrel is not recommended in pregnant or breastfeeding women. Undesirable Effects: Adults: The most commonly reported adverse reactions are injection site reactions, infections, allergic reactions, development of autoantibodies, itching, and fever. See SmPC for less commonly reported side effects. TNF-antagonists, such as Enbrel, affect the immune system and their use may affect the body’s defences against infection and cancer. Serious infections affect fewer than 1 in 100 patients treated with Enbrel. Reports have included fatal and life threatening infections and sepsis. Various malignancies have also been reported with use of Enbrel, including cancers of the breast, lung, skin and lymphatic system (lymphoma). Serious infections and other adverse events such as uncommon reports of: thrombocytopaenia, systemic vasculitis, uveitis and
scleritis, interstitial lung disease, rare reports of tuberculosis, opportunistic infections, anaemia, leucopaenia, neutropaenia, pancytopenia, seizures, worsening of heart failure, autoimmune hepatitis, Steven Johnson’s syndrome and very rare reports of : anaphylaxis, toxic epidermal necrolysis and aplastic anaemia have been reported. Reactivation of hepatitis B (a liver infection) has also been reported. Central and peripheral demyelinating events have been seen rarely and very rarely, respectively, with Enbrel use. There have been rare reports of lupus, lupus-related conditions, and vasculitis. Rate of new malignancies was similar to that expected for the population studied. Fatalities associated with serious infections, pancytopenia, aplastic anaemia and interstitial lung disease have also been reported. Paediatrics: Generally as for adults, except the following were more common: headaches, nausea, vomiting and abdominal pain. In addition the following were reported as severe events: varicella, appendicitis, gastroenteritis, depression/personality disorder, cutaneous ulcer, oesophagitis/gastritis, group A streptococcal septic shock, type I diabetes mellitus and soft tissue and post operative wound infection. There have been post-marketing reports of IBD and uveitis in JIA patients, including cases indicating a positive re-challenge. Legal Category: POM. Package Quantities: Enbrel Pre-filled Syringe: Each carton contains 4 pre-filled syringes containing either 25 mg or 50 mg of Enbrel and 4 alcohol swabs. Enbrel Pre-filled Pen (MYCLIC): Each carton contains 4 pre-filled pens containing 50 mg of Enbrel and 4 alcohol swabs. Enbrel Powder: Each carton contains 4 vials of Enbrel 25 mg powder, 4 pre-filled syringes of water for injections, 4 needles, 4 vial adaptors and 8 alcohol swabs. Enbrel Paediatric (10 mg): Each carton contains 4 vials of Enbrel 10 mg powder, 4 prefilled syringes of water for injections, 4 needles, 4 vial adaptors and 8 alcohol swabs.
European Marketing Authorisation Numbers: Enbrel Pre-filled Syringe 25 mg: EU/1/99/126/013 Enbrel Pre-filled Syringe 50 mg: EU/1/99/126/017 Enbrel Pre-filled Pen (MYCLIC) 50 mg: EU/1/99/126/020 Enbrel Powder 25 mg: EU/1/99/126/003 Enbrel Paediatric 10 mg: EU/1/99/126/022. S1B: Product subject to a prescription which may be renewed. European Marketing Authorisation Holder: Pfizer Limited, Ramsgate Road, Sandwich, Kent, CT13 9NJ, UK. For full prescribing information see the Summary of Product Characteristics. For further information on this medicine please contact: Pfizer Medical Information on 1800 363 633 or at [email protected]. For queries regarding product availability please contact: Pfizer Healthcare Ireland, Pfizer Building 9, Riverwalk, National Digital Park, Citywest Business Campus, Dublin 24 + 353 1 4676500. API Reference Number: EN 6_1. Date of Prescribing Information: December 2012.
References:1. Enbrel Summary of Product Characteristics August 2013. 2. Remicade Summary of Product Characteristics. 3. Humira Summary of Product Characteristics. 4. Orencia Summary of Product Characteristics. 5. Mabthera Summary of Product Characteristics. 6. Simponi Summary of Product Characteristics. 7. Singh J et al. CMAJ:2009 DOI;10.1503. 8. Hetland ML et al. Arthritis & Rheumatism. Vol 62, no 1, January 2010. 9. Data on File Pfizer Inc.10 Data on File Amgen
# Rheumatoid Arthritis, Psoriatic Arthritis, Juvenile Idiopathic Arthritis, Ankylosing Spondylitis and Psoriasis. For full prescribing information see the Summary of Product Characteristics.
ENB/2013/192/1Date of preparation: September 2013
A unique mechanism of action
• Enbrel is the only fully human soluble tumour necrosis factor (TNF) receptor 1,2,3,4,5,6
• It works differently than MAB’s 1
No neutralising antibodies 1
• Enbrel is not associated with the production of neutralising antibodies in humans
Enbrel has a short half life (<3 days) 1
• The half-life of anti-TNF agents should be taken into account if a treatment break is required
Efficacy
• Registry data and Cochrane Review data support efficacy & safety of Enbrel 7,8
The ENBREL way Indicated for RA, PsA, JIA, AS and PsO #
5873 Enbrel_Fast Facts A4 Advert_NIGP.indd 1 26/09/2013 18:08

8
News for IPNA br ANches couNtry wIderegional news
cAvAN/mONAGhAN
MARGARET GEOGHEGAN
Prior to the summer break the branch held two very interesting meetings.Our May meeting was sponsored by Abina O’Flynn from MSD.Pauline Kilpatrick Cardiac Rehabilitation Co-Coordinator from Cavan/Monaghan Hospital Group gave an
excellent presentation on the 2012 European guidelines on CVD prevention in clinical practice.At our June meeting members from the National Cancer Control programme gave us an update on cervical,
colorectal and retinopathy screening. The speakers were Carrie Powell, Carol McNamara & Teresa Shortt. we had a break for July & August to enjoy our lovely summer & what a summer it was.we had our AGM on Sept 11th. This meeting was sponsored by Paula McGoona from Meda. Ruth Morrow gave a
presentation on Allergic Rhinitis and Asthma.The minutes from the September NEC meeting were discussed. we took the opportunity to plan the branch
meetings for the year. we have some interesting topics and speakers and when these are confirmed they will be posted on IPNA website. Meetings will be held in the Errigal Hotel Cootehill and days of meeting will be staggered in an effort to facilitate members.
we urge all members to make a big effort to attend our meetings.we would like to take this opportunity to wish the North Dublin branch all the best with hosting the 2013 IPNA
conference. we are looking forward to sitting back this year and enjoying it.
NORTh dublIN
ORlA DONNEllY ANNE MARIE EllwOOD
The North Dublin Branch has spent the summer finalising the details for our upcoming hosting of the National Conference. It promises to be an educational and fun filled conference and we hope to see as many of you as possible there.
Our last educational meeting in May was an update on COPD guidelines given by Dr Dermot O’Callaghan, Respiratory Consultant from the Mater Hospital and sponsored by Astra Zeneca. Dr O’Callaghan gave a clear and concise talk which took the mystery out of COPD.
Our September meeting concluded our preparation for the Conference. Our November meeting following the Conference will be our AGM. we will be electing new officers at that meeting.
SOuTh dublIN
KAREN CANNING AND ANNE O’CONNOR
It was great to welcome so many of our branch members last week to our first meeting after the summer break held at Bewley’s Hotel, leopardstown.
John Barron, Boehrigner-Ingelheim, very kindly sponsored the night.Our guest speaker was Imelda Noone, Stroke CNS, St Vincent’s Hospital, who gave us a presentation on the
acute treatment of a patient following a stroke and whether they would be considered for warfarin or one of the newer anti-clotting agents.
She also touched briefly on the use of either in A. Fib.John followed with an interesting update on the current research on Pradaxa.Anne O’Connor (sec) welcomed our new members and congratulated Elaine Naughton on recently becoming
our first Nurse Prescriber. Anne also informed us of the topics and sponsors for most of the meetings until May 2014, which are listed on the IPNA website.
I updated those present on the minutes arising from the recent NEC meeting.we reminded those present that there were still places available to attend the upcoming National Conference,
being hosted by IPNA North Dublin branch and that it would be a great event and urged our members to attend.we would like to wish the North Dublin branch the best of luck with their first hosting of the conference and
we are thoroughly looking forward to what promises to be a great 2 days.

9
News for IPNA br ANches couNtry wIde regional news
wexfORd
DORA MullIGAN
Hello to everyone from the wexford branch, hope you all had a good summer and got your fair share of the sunshine. we finished in May with a very informative talk from the nurses in the Hope Cancer Support Centre Enniscorthy and a barbecue very kindly sponsored by Pam large from Boehringer. Our first meeting this month will be on wound Care.
wIcKlOw
MARY FINNEGAN
Hope everyone had a wonderful, stress free, happy, healthy summer! Not a bad few months weather wise this year, and the sun is still shining as I write this on 1st September! Hopefully we may have a few more weeks of good weather to look forward to. Hard to believe it is nearly ‘Flu vaccine’ season!
Since my last news item in the magazine we had 2 excellent meetings, one in April and 2nd in May.Our topic for the April meeting was The Practice Nurse›s Role in Managing Cardiovascular Risk Factors, which
was expertly given by Angela Chambers, who has been working as a Practice Nurse in general practice for over 10 years, providing care and education to hundreds of patients under the Heartwatch Programme, and through cardiovascular clinics which she runs in her own GP practice. She also gave us a brief talk and handouts on Common Interactions for patients on warfarin Therapy. These were excellent topics with lots of interest from those present. This meeting was very kindly sponsored by Ciaran O›Kelly from MSD.
In May our topic was Type2DM Patient Care in GP practice from a Practice Nurse›s Perspective. Once again this talk was given by a Practice Nurse, Karen Canning, who has been working in GP practice since 1999. Karen has been running a Diabetes Clinic in GP practice for many years, and has completed a Diploma in Clinical Primary Care, which continued on to a Masters on ‹Insulin Initiation in Primary Care for patients with Type 2 DM. Once again, an excellent talk received with great interest by those nurses present.
This meeting was kindly sponsored by David Kelly from Roche.we were particularly delighted to be able to avail of the expertise of two excellent Practice Nurses who are
experts in their own particular field, rather than having to look further afield, to one of our medical colleagues. There is such a wealth of knowledge, experience and expertise among our own peers, that it is wonderful to be able to avail of it for our ongoing educational updates.
Our next meeting is scheduled for Monday 23rd September at 8pm in the wilton Hotel In Bray.The topic for the meeting will be Chronic and Acute Pain Management Overview. Our guest speaker will be Dr
Hugh Gallagher, Consultant in Anaesthetic Medecine at SVuH and SCH. The meeting is kindly sponsored by Peter Daly from Mundipharma Pharmaceuticals.
we will have no meeting in October, as we hope to see everyone at the Annual Conference in Athlone on 10th and 11th! looks like an excellent weekend, and do hope as many of the Branch members as possible will be able to attend.
Our meeting in November will be held on 18th, and this will be the Branch AGM. Education topic TBA later.There will be no meeting in December. we resume again in January 2014Once again, can I thank all those who attended meetings on a regular basis last year, and look forward to
seeing you all again for this coming year. we need all your support to keep the Branch active and alive, and meetings are a great way to network with your peers, as well as keeping up with ongoing education, so do come along.....after all, it is only 6 meetings in the year!

10
clinical review
The management of hypertension AOIfe mORRIS, RGN, BSC HDIP CARDIOVASCulAR CARE, AlmA muRPhy, RGN, BSC HDIP CARDIOVASCulAR CARE, GAlwAY ClINIC, GAlwAY AND dR JOhN clARKe, CONSulTANT CARDIOlOGIST, EAGlE lODGE MEDICAl CENTRE, lIMERICK.
The following article charts the latest approaches to managing and treating this increasingly prevalent condition
The world Health Organisation (wHO) describes hypertension as “a condition in which blood vessels have persistently raised pressure”. If left untreated, hypertension can have detrimental effects on health and mortality, leading to preventable incidents such
as myocardial infarction, heart failure, stroke and kidney failure. There has been a surge in the prevalence of hypertension worldwide, climbing from six hundred million in 1980 to one billion in 2008 and if appropriate action is not taken, deaths due to cardiovascular disease are projected to rise, according to wHO.
definitionsDefining the cut-off point between normotensive and hypertensive has proven difficult (Mancia et al., 2013). Trials have demonstrated the beneficial reduction in cardiovascular risk when reducing systolic blood pressure (SBP) below 140mmHg (liu et al., 2005). However, trials to observe the benefit of aggressive SBP lowering below 130 mmHg were unable to find significant reduction in stroke or cardiovascular risk (ACCORD Study Group, 2010 and Yusuf, et al., 2008). In light of this and contrary to recent guidelines, the threshold for defining hypertension in a person with diabetes, cardiovascular disease or chronic kidney disease has been modified from 130/80 to 140/80 (Mancia et al., 2009). (Table 1).
Table 1. definition and classification of hypertension in adults, parameters (mmhg):
High normal 1 30–139 and/or 85–89
Grade 1 hypertension 140–159 and/or 90–99
Grade 2 hypertension 160–179 and/or 100–109
Grade 3 hypertension ≥180 and/or ≥110
(Mancia et al., 2013)
while ambulatory blood pressure monitoring (ABPM) and home blood pressure monitoring (HBPM) both provide a more reliable assessment of actual blood pressure and a more successful prediction of cardiovascular risk (Dolan et al., 2005 and Sega et al., 2005), guidelines still are based on office blood pressure being considered the current gold standard. This decision is based on considerations in relation to the cost and resources influencing best practice.
clinical managementHypertension in general is asymptomatic but may be associated with headaches, shortness of breath, dizziness, chest pain, palpitations and nosebleeds. A comprehensive clinical assessment, including family and medical history, with relevant recommended diagnostic tests is required to identify the presence of end organ damage and determine

11
clinical review
contributing risk factors (Madhur, 2013). A routine ECG provides information on cardiovascular disease and organ damage, as well as establishing the need for a 24-hour Holter monitor or echocardiogram if indicated by results (Mancia et al., 2013). Auscultating the heart, carotid arteries and renal arteries will verify the need for echocardiogram, carotid ultrasounds or renal vascular ultrasound in the presence of a murmur.
A urinalysis identifies the presence of microalbuminuria and assesses end organ renal damage and a fasting glucose to assess for diabetes. A renal profile provides a useful check for asymptomatic organ damage of the kidneys as well as establishing a baseline prior to commencing antihypertensive medications. A fasting lipid profile is advised, as the benefit of statins in people with high cardiovascular risk remains justified according to most recent guidelines (Mancia et al., 2013).
Other than urinalysis and measurement of urea and electrolytes, more extensive testing for identifiable causes is not generally indicated, unless blood pressure control is not achieved (Chobanian et al., 2003). Referral to specialist physicians is sometimes required as many people with hypertension will have more than one cardiovascular risk factor and baseline assessments may highlight the need for further investigations. McCormack and Cappuccio (2008) advise that measures should be taken prior to referring to a specialist such as ensuring adherence to medication – compliance being a major pitfall in control of hypertension – and lifestyle modification.
It is suggested that at primary care level, it is reasonable to see if satisfactory blood pressure control can be achieved with the use of two agents in combination before considering referral to a specialist unit. The standard combinations in use these days would include a calcium channel blocker as monotherapy moving to a combination of a calcium channel blocker and ACE inhibitor (ACE-I) as second line therapy. while beta-blockers are approved as first line agents, they would generally be reserved for patients with another indication such as angina pectoris, heart failure, atrial fibrillation or even anxiety.
Current European guidelines recommend screening for all patients for secondary sources of hypertension as a wise precaution but this may not be feasible in terms of resources (Mancia et al., 2013). Secondary hypertension accounts for 2-10 per cent of cases (Madhur, 2013). Possible causes of secondary hypertension include obesity, obstructive sleep apnoea, renal artery stenosis, nephritic syndrome, coarctation of the aorta, Conn’s Syndrome and drugs such as NSAIDs, steroids, combined contraceptive pill, ciclosporin, cocaine and alcohol (McCormack and Cappuccio, 2008).
medical therapyMedical therapy is recommended in grade 1 hypertension in people with organ damage, high cardiovascular risk factors, diabetes, cardiovascular disease, or chronic kidney disease. It is also recommended when blood pressure remains high, despite having modified one’s lifestyle for a reasonable period of time. Medical therapy can be commenced with grade 2 and 3 hypertension immediately with, or after a period of time of lifestyle changes (Mancia et al., 2013). In elderly hypertensive patients, drug therapy is recommended when systolic blood pressure is above 160mmHg and may be reduced to below 150mmHg, rather than 140mmHg, as studies have shown this to be effective. However, medication therapy may be considered in elderly patients when the SBP range is 140-159mmHg, provided the therapy is well tolerated (Mancia et al., 2013).
European Society of cardiology guidelines (2013) reinforce
the 2007 guidelines (Mancia et al., 2013) that concluded that diuretics, beta-blockers, calcium antagonists, angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers are all suitable for the initiation and maintenance of antihypertensive therapy as monotherapy or in some combinations.
An ACE-I prevents the conversion of angiotensin 1 to angiotensin 2 in the lungs during the renin-angiotensin cycle, decreasing peripheral vessel resistance causing vasodilation and preventing cardiac remodelling (lopez-Sendon et al., 2004). An ACE-I must not be given to patients with renal stenosis as this may cause a drop in renal perfusion and precipitate renal failure. Other contra indications include aortic stenosis, obstructive cardiomyopathy and hyperkalaemia (lopez-Sendon et al., 2004). Angiotensin 2 receptor blockers (ARBs) are indicated for patients who cannot tolerate an ACE-I, as they do not inhibit the breakdown of bradykinin in the lungs, therefore users will not be at risk of developing the associated cough. Contra indications are similar to an ACE-I. In addition, they may also increase hepatic enzyme levels (Chobanian et al., 2003).
Beta-blockers act as an anti-hypertensive, as well as producing an anti-arrhythmic and anti-ischaemic effect. Contraindications to beta-blocker initiation include asthma, symptomatic hypotension, bradycardia, severe heart failure, and heart block (lopez-Sendon et al., 2004).
For decades, thiazide diuretics have been recommended as first choice therapy and as a component in combination therapy in most cases (Chobanian et al., 2003). Contraindications include severe kidney dysfunction and hypernatraemia (Hermann, 2010). loop diuretics block reabsorption of sodium chloride and water in the kidneys. They may also cause severe kidney dysfunction and hypernatraemia (Mancia et al., 2013). Potassium-sparing diuretics work by acting on the distal tubule in the kidneys, independently of aldosterone. Potassium levels must be monitored for hyperkalaemia, especially when prescribed with an ACE-I or an ARB (Hermann, 2010).
Calcium antagonists can be divided into dihydropyridines (DHPs) and non-DHPs. DHPs may cause peripheral oedema, dizziness or headaches, while non-DHPs are contraindicated in patients with sick sinus syndrome, second and third-degree AV block (Basile, 2004).
lifestylelifestyle changes are essential in the prevention and treatment of hypertension and its associated risks. The most important
contraindications to beta-blocker initiation include asthma, symptomatic hypotension, bradycardia, severe heart failure, and heart block.

12
clinical review
behavioural risk factors are unhealthy diet, physical inactivity, tobacco use and harmful use of alcohol (wHO, 2013) as they contribute to the development of the metabolic risk factors of obesity, diabetes and raised blood lipid levels.
Mancia et al. (2013, p28) rank quitting smoking as “probably the single most effective lifestyle change measure for preventing cardiovascular disease”. Smoking cessation medications are recommended when necessary, yet these drugs are reported to be underused due to adverse effects, contraindications and cost (Mancia et al., 2013).
Necessary alterations to make the transition to a healthy lifestyle include a restricted salt intake to 5-6g per day, a moderate consumption of alcohol, a diet low in fat and high in vegetables, fruit and lean meat, maintaining an appropriate weight and partaking in regular exercise (Mancia, et al. 2013 and Dickinson, et al. 2006). Adopting this approach to modifiable risk factors has proved to be as successful as monotherapy in reducing blood pressure (Elmer, et al. 2006), however the difficulty lies in long-term compliance.
The rationale for therapy is to obtain an end result of lowering blood pressure within the appropriate parameters relevant to each individual. If optimal lifestyle and medical therapy do not reach desired results, invasive approaches may be an option to consider. Renal denervation and carotid baroreceptor stimulation show promising potential, however long-term comparison trials to establish persistent efficacy is required (Mancia et al., 2013).
follow upFollow up visits involve assessing the effectiveness of the prescribed antihypertensive therapy. This may involve a kidney function lab test to review potassium levels and renal function, depending on prescribed medication.
The role of the healthcare provider involves referring the individual to appropriate members of the multidisciplinary team in order to provide effective person-centred advice and care to assist them to continue to adhere to their antihypertensive therapy, e.g. smoking cessation, or dietitian. Ensuing visits offer an opportunity to educate, counsel and empower the person to become proactive in their own wellbeing (Madhur, 2013). Information and support for family members is also essential (Mclean and Timmins, 2007) as they can provide a supportive and encouraging role in modification risk factors. Aspirin may also be introduced during follow up reviews as it is recommended in people who have had a previous cardiovascular event, high cardiovascular risk or impaired renal function once blood pressure is controlled and its benefit outweighs potential harm (Mancia et al., 2013).
hypertension in general is asymptomatic but may be associated with headaches, shortness of breath, dizziness, chest pain, palpitations and nosebleeds.
References
The ACCORD Study Group. (2010)‘Effects of intensive blood-pressure control in type 2 diabetes mellitus’, New England Journal of Medicine, 362 (17), pp. 1575–1585.Basile, J. (2004) ‘The Role of Existing and Newer Calcium Channel Blockers in the Treatment of Hypertension’, The Journal of Clinical Hypertension,6 (11), pp. <http://onlinelibrary.wiley.com/doi/10.1111/jch.2004.6.issue-11/issuetoc> 621–629.Chobanian, A. V., Bakris, G. l., Black, H. R., Cushman, w. C.,Gren, l. A., Izzo, J. l., Jones, D. w., Materson, B. J., Oparil, S. and wright, J. T. (2003) ‘The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure’, Journal of the American Medical Association, 289:(19) 2560-2573. Dickinson, H. O., Mason, J. M., Nicolson, D. J., Campbell, F., Beyer, F. R., Cook, J. V., williams, B. andFord, G. A. (2006) ‘lifestyle interventions to reduce raised blood pressure: a systematic review of randomized controlled trials’, Journal of Hypertension, 24 (2), pp. 215–233.Dolan, E., Stanton, A., Thijs, l., Hinedi, K., Atkins, N., McClory, S., Den Hond, E., McCormack, P., Staessen, J. A. and O’Brien, E. (2005)‘Superiority of ambulatory over clinic blood pressure measurement in predicting mortality: the Dublin outcome study’, Hypertension, 46(1), pp. 156–161.Elmer, P.J., Obarzanek, E., Vollmer, w. M., Simons-Morton, D., Stevens, V. J., Young, D. R., lin, P. H., Champagne, C., Harsha, D. w., Svetkey, l. P., Ard. J., Brantley, P. J., Proschan, M. A., Erlinger, T. P. and Appel, l. J. (2006) ‘Effects of comprehensive lifestyle modification on diet, weight, physical fitness and blood pressure control: 18-month results of a randomized trial’, Annals of Internal Medicine, 144 (7), pp. 485–495.European Society of Hypertension-European Society of Cardiology (2003) ‘Guidelines for the management of arterial hypertension’, Journal of Hypertension, 21 (6), pp. 1011–1053.lopez-Sendon, J., Swedberg, K., McMurray, J., Tamargo, J., Maggioni, A. P., Dargie, H., Tendera, M., waagstein, F., Kjekshus, J., lecht, P. and Torp-Pederson,C. (2004) ‘Expert consensus document on B-adrenergic receptor blockers’, European Heart Journal, 25 (15), pp. 1341-1362.liu, l., Zhang, Y., liu, G., li, w., Zhang, X. and Zanchetti, A. (2005) ‘The Felodipine Event Reduction (FEVER) Study: a randomized long-term placebo-controlled trial in Chinese hypertensivePatients, Journal of Hypertension, 23 (12), pp. 2157–2172.Madhur, M. S. (2013) Hypertension Available at: http://emedicine.medscape.com/article/241381-overview(Accessed: 31 July 2013).Mancia, G.,Fagard, R., Narkiewicz, K., Josep Redon, J., Zanchetti, A., Bo¨hm, M., Christiaens, T., De Backer, G., Anna Dominiczak, A., Maurizio Galderisi, M., Diederick E. Grobbee, D.E.,T., Kirchhof, P., Kjeldsen, S. E., laurent, S., Athanasios J. Manolis, A. J., M. Nilsson, P., Ruilope, l. M., Schmieder, R,E., Sirnes, P. A., Peter Sleight, P., Margus Viigimaa, M., Bernardwaeber andZannad, (2013)‘European Society of Cardiology Guidelines for the management of arterial hypertension’,European Heart Journal, 34 (28), pp. 2159-2219.Mancia, G., laurent, S., Agabiti-Rosei, E., Ambrosioni, E., Burnier, M., Caulfield, M. J.,Cifkova, R., Clement, D., Coca, A., Dominiczak, A., Erdine, S., Fagard, R., Farsang, C.,Grassi, G., Haller, H., Heagerty, A., Kjeldsen, S. E., Kiowski, w., Mallion, J. M., Manolis, A.,Narkiewicz, K., Nilsson, P., Olsen, M. H., Rahn, K. H., Redon, J., Rodicio, J., Ruilope, l.,Schmieder, R. E., Struijker-Boudier, H. A., Van Zwieten, P. A., Viigimaa, M. and Zanchetti, A. (2009) ‘Reappraisal of European guidelines on hypertension management: a European Society of Hypertension Task Force document’,Journal of Hypertension, 27 (11), pp. 2121–2158.Mancia, G., De Backer, G., Dominiczak, A., Cifkova, R., Fagard, R., Germano, G., Grassi, G., Heagerty, A. M., Kjeldsen, S. E., laurent, S., Narkiewicz, K., Ruilope, l., Rynkiewicz, A., Schmieder, R. E., Boudier, H. A. and Zanchetti, A., (2007)‘Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of

Information about adverse event reporting can be found at www.imb.ie. Adverse events and inadvertent vaccination during pregnancy should also be reported to Sanofi Pasteur MSD by calling 00 44 1628 785291.
08/13 IR00150(1)
PNEUMOVAX® II solution for injection in a vial Pneumococcal Polysaccharide Vaccine Refer to Summary of Product Characteristics for full product information. Presentation: Pneumovax II is supplied as a single dose vial containing 0.5 millilitre of solution. Each dose contains 25 micrograms of each polysaccharide type derived from capsules of the 23 most prevalent pneumococci, dissolved in isotonic saline solution containing 0.25% phenol. Indications: For active immunisation against disease caused by the pneumococcal serotypes included in the vaccine. The vaccine is recommended for individuals 2 years of age or older in whom there is an increased risk of morbidity and mortality from pneumococcal disease. The specific at risk categories of persons to be immunised are to be determined on the basis of official recommendations. The vaccine is not effective for the prevention of acute otitis media, sinusitis and other common upper respiratory tract infections. Dosage and administration: One single dose of 0.5 millilitre is administered by intramuscular or subcutaneous injection. Special dosing: It is recommended that pneumococcal vaccine is given at least two weeks before elective splenectomy or the initiation of chemotherapy or other immunosuppressive treatment. Vaccination during chemotherapy or radiation therapy should be avoided, and the vaccine should not be administered any sooner than three months after completion of such therapy. Persons with asymptomatic or symptomatic HIV infection should be vaccinated as soon as possible after diagnosis is confirmed. Revaccination: Healthy adults and children should not be revaccinated routinely. Revaccination at intervals of less than three years is not recommended because of an increased risk of adverse reactions. Revaccination may be considered for adults at increased risk of serious pneumococcal infection who were given pneumococcal vaccine more than five years earlier or for those known to have rapid decline in pneumococcal antibody levels. Revaccination after 3 years may be considered for selected populations (e.g. asplenics) who are known to be at high risk of fatal pneumococcal infections and for children 10 years old or younger at high risk of pneumococcal infection. Contraindications: Hypersensitivity to any component of the vaccine. Warnings and precautions: As with any vaccine, adequate medical treatment, including epinephrine (adrenaline), and supervision should always be available in case of an acute anaphylactic reaction. It is not known whether the vaccine can cause foetal
harm or affect reproduction capacity when administered to a pregnant woman; the vaccine can be given to pregnant women only if clearly needed (potential benefit outweighs potential risk). It is not known whether this vaccine is excreted in human milk; caution should be exercised when thevaccine is administered to a nursing mother. Vaccination should be delayed in the presence of significant febrile illness or other active infection, except where delay involves greater risk.The vaccine should never be injected intravascularly. The vaccine should not be injected intradermally as injection by that route is associated with increased local reactions. If the vaccine is administered to patients who are immunosuppressed due to either an underlying condition or medical treatment (e.g. immunosuppressive therapy), the expected serum antibody response may not be obtained after a first or second dose, so such patients may not be as well protected against pneumococcal disease as immunocompetent individuals. Required prophylactic pneumococcal antibiotic therapy should not be stopped after vaccination. The vaccine may not be effective in preventing infection resulting from basilar skull fracture or from external communication with cerebrospinal fluid. As with any vaccine, vaccination with Pneumovax II may not result in complete protection in all recipients. Pneumovax II and Zostavax should not be given concurrently because concomitant use in a clinical trial resulted in reduced immunogenicity of Zostavax. Undesirable effects: Very common side effects: Fever and injection site reactions such as pain, soreness, erythema, warmth, swelling and induration. Other reported side effects that may potentially be serious include thrombocytopenia in patients with stabilised idiopathic thrombocytopenic purpura, haemolytic anaemia in patients who have had other haematologic disorders, leukocytosis, anaphylactoid reactions, serum sickness, angioneurotic oedema, Guillain-Barré Syndrome, radiculoneuropathy, febrile convulsions and injection site cellulitis. For a complete list of undesirable effects please refer to the Summary of Product Characteristics. Package quantities and basic NHS cost: Single pack containing one 0.5 millilitre single dose vial, basic NHS cost £8.32 (single). Marketing authorisation holder: Sanofi Pasteur MSD Limited, Mallards Reach, Bridge Avenue, Maidenhead, Berkshire SL6 1QP. Marketing authorisation number: PL 06745/0103 Legal category: POM Date of last review: August 2013
Are your patients at risk?
* See Immunisation Guidelines for Ireland www.immunisation.ie
Pneumococcal DiseaseVaccinate your at-risk patients and those 65 years and over against serious pneumococcal disease.
age 65+
chronic lung,liver, heart orrenal disease
weakenedimmunesystem
other at-risk groups*smoker
diabetesvis i t pneumo. ie
pneumovax A4 2013 v4.indd 1 27/09/2013 11:36

14
clinical review
Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC)’,Journal of Hypertension, 25(6), pp. 1105–1187.McCormack T. and Cappuccio, F. P. (2008) ‘10 steps before you refer for hypertension’, British Journal of Cardiology, 15(5), pp. 254-257.Mclean S. and Timmins F. (2007) ‘An Exploration of the Information Needs of Spouse/Partner following Acute Myocardial Infarction using Focus Group Methodology’, Nursing in Critical Care,12 (3), pp. 141 – 150.Moser, M. (1983) ‘A decade of progress in the management of hypertension’,Hypertension, 5 (6), pp. 808-813.Sega, R., Facchetti, R., Bombelli, M., Cesana, G., Corrao, G., Grassi, G., and Mancia, G. (2005)‘Prognosticvalue of ambulatory and home blood pressures compared with office bloodpressure in the general population: follow-up results from the Pressioni ArterioseMonitorate e loro Associazioni (PAMElA) study,Circulation, 111 (14), pp. 1777–1783.Yusuf, S., Diener, H. C., Sacco, R. l., Cotton, D., Ounpuu, S., lawton, w. A., Palesch, Y., Martin, R. H., Albers, G. w., Bath, P., Bornstein, N., Chan, B. P., Chen, S. T., Cunha, l., Dahlof, B., De Keyser, J., Donnan, G. A., Estol, C., Gorelick, P., Gu, V., Hermansson, K., Hilbrich, l., Kaste, M., lu, C., Machnig, T., Pais, P., Roberts, R., Skvortsova, V., Teal, P., Toni, D., VanderMaelen, C., Voigt, T.,weber, M. and
Yoon, B. w.(2008) ‘Telmisartan to prevent recurrentstroke and cardiovascular events’,New England Journal of Medicine,359 (12), pp. 1225–1237.V.A. Cooperative study group (1967) ‘Effects of Treatment on Morbidity in Hypertension Results in Patients with Diastolic Blood Pressures Averaging 115 Through 129 mm Hg’, Journal of the American Medical Association,202(11), pp. 1028-1034.world Health Organisation (2013) A global brief on hypertension: silent killer, global public health crisis. Available at: http://www.who.int/cardiovascular_diseases/publications/global_brief_hypertension/en/ (Accessed: 31 July 2013)world Health Organisation (2011) Global status report onnoncommunicable diseases 2010: Description of the global burden of NCDs, their risk factors and determinants. Available at: http://www.who.int/nmh/publications/ncd_report2010/en/ (Accessed: 31 July 2013)world Health Organisation. (2007) Prevention of Cardiovascular disease: Guidelines for assessment and management of cardiovascular risk. Available at: www.who.int/cardiovascular_diseases/guidelines/prevention_of_cardiovascular_disease/en/ <http://www.who.int/cardiovascular_diseases/guidelines/prevention_of_cardiovascular_disease/en/> (Accessed: 31 July 2013).
Practice nurse requireddublin 6w
Practice Nurse required for Dublin 6w Medical Centre from October 2013. Part-time 25 hours moving to full time and permanent for the right candidate. The position is open to one candidate or two job sharing. Experience in cervical cytology, childhood immunisation and phlebotomy required.
Please email c.v. to: [email protected]
Practice nurse requiredcork city
Part-time position available for an experienced Practice Nurse in a relatively new, (6 years in operation) very pleasant mixed practice just north of Cork city. The practice has computerized and has exceptional secretarial support. we are also involved with local community health initiatives.
The hours are: Mon, wed, Thurs mornings 9:30-12:00 and Tuesday evenings, 4:30 to 7:00. If necessary, there could be some leeway in these hours.
Rate of pay is negotiable.
Please send cv and references to [email protected]
Practice nurse requireddublin south west
Experienced Practice Nurse required, for busy family practice, based in south west Dublin. Full-time position. Main duties include childhood vaccinations, cervical smears, ear irrigation, wound care, phlebotomy, chronic disease management and cryotherapy. Experience in midwifery a distinct advantage. Position offers an excellent remuneration package.
Please email cv to [email protected] or call 087 2050379 after 6pm.
Practice nurse requiredTallaght, d24
Practice Nurse required for full time position for busy surgery in Tallaght, Dublin 24. Fully computerised dynamic 4 doctors 3 nurses practice.
cv and references to [email protected] or telephone Pauline on 01-4513589
To advertise here contact Graham: [email protected] or louis: [email protected] Tel: 01 4410024
Practice Nurse Recruitment

15
clinical review
Review of GINA asthma guidelines in stable adult asthmaRuTh mORROw
Asthma affects over 470,000 people in Ireland. 7.1% of Irish adults have asthma (www.asthmasociety.ie accessed 6th August 2013). In 2013, one person continues to die from asthma in Ireland every week despite advances in knowledge of the mechanisms
of asthma and pharmacology. Asthma is a condition that can be treated effectively and most patients can obtain good control through optimal use of their medication and appropriate management plans. Optimally controlled asthma includes:• little or no use of reliever inhaler• no night-time or daytime symptoms• productive physically active lives• near normal lung function• avoidance of serious attacks
(GINA, 2012)
This article seeks to review the recently updated asthma guidelines for general practice: Asthma Control in General Practice Adapted from the GINA Global Strategy for Asthma Management & Prevention (2012). The focus of this article is on stable adult asthma.
Signs and symptoms The symptoms of asthma include wheezing, coughing,
shortness of breath and chest tightness following exposure to allergens. These symptoms are variable and usually troublesome at night or early morning. Patients may present with one, two, three or all four symptoms. Some patients may also present with colds that “go to the chest” or take more than 10 days to clear.
diagnosisThe diagnosis of asthma is made by the patient’s symptoms and medical history with the measurement of lung function using spirometry (GINA, 2012).
If the patient has a history of any of the following then
asthma should be suspected:• cough which is worse at night• recurrent wheeze• recurrent difficulty breathing• recurrent chest tightness
Symptoms are variable and may occur or worsen in a season-able pattern. The patient may also have eczema and hayfever. A positive family history of asthma or other atopic conditions may also be present. The patient may describe their symptoms becoming worse when exposed to certain trigger factors. These may include animal dander, aerosol chemicals, changes in temperature, dust mite, exercise, pollen, respiratory infec-tions (viral), smoke and emotion. The list of possible trigger factors can be lengthy and it may take the patient some time before they can identify their trigger factors.
Spirometry is the preferred method for measuring airflow obstruction with reversibility to establish a diagnosis of asthma. An increase in FEV1 of 12% or 200mls fifteen minutes after inhaling a bronchodilator demonstrated airflow limitation con-sistent with asthma (GINA, 2012). However, not all patients with asthma will have reversibility and repeated tests are advised.
Peak flow measurements can be used if the patient is unable to perform spirometry and are very useful as a monitoring and educational tool for patients. An improvement of 60l/min or greater than 20% post bronchodilator or a greater than 20% in diurnal variation (with twice daily readings, more than 10%) suggests a diagnosis of asthma (GINA, 2012).
Measure of allergic status (IgE, RAST, skin allergy tests) can be useful in identifying risk factors. The presence of allergies, ec-zema and allergic rhinitis increase the probability of a diagnosis of asthma.
Challenges to the diagnosis of asthma include:• Cough variant asthma – some patients have chronic cough
which occurs at night. Evidence of lung function variability

16
clinical review
treatment steps and patients may move up or down the steps de-pending on symptoms and the amount of reliever therapy being used (see Table 2). Inhaled glucocorticosteroids are the corner-stone of asthma treatment and are the most effective controller medications available (see Table 3). However, there are additional medications such as leukotriene receptor antagonists which can be added on, and are very useful in patients who have an allergy component to their asthma. These medications are also licensed for use in allergic rhinitis, a condition which a significant number of people with asthma also have. Newly diagnosed patients who are not yet on medication should be commenced on Step 2 or Step 3 depending on severity of symptoms (GINA, 2012). Patients who do not reach an acceptable level of control at Step 4 can be considered to have difficult to treat asthma and should be referred to a respiratory specialist for management.
and airway hyper-responsiveness are important to determine the presence or absence of asthma.
• Exercise induced bronchoconstriction – for some patients, physical activity may be the only trigger for asthma. An 8 minute running challenge can confirm an asthma diagnosis.
• Asthma in the elderly can be difficult to determine as there are several complicating factors such as poor perception of symptoms, reduced expectations of mobility and activity and the possibility of other conditions such as COPD, heart failure, lung cancer, and TB to mention but a few.
• Occupational asthma requires a defined history of occupa-tional exposure to sensitizing agents, an absence of asthma symptoms prior to employment and a documented relation-ship between symptoms and the workplace. The patient should be asked to maintain a peak flow diary while at work and while away from work to help determine the diagnosis. The opinion of an occupational respiratory physician should be sought.
classification of asthma by level of controlTable 1 illustrates levels of asthma control and the future risk of exacerbations, instability, decline in lung function and side ef-fects. All patients should be assessed and their level of control established. In general, good clinical control of asthma leads to reduced risk of exacerbations (GINA, 2012). There are a number of well validated tools available which can assist the practice nurse in assessing asthma control such as the asthma Control Test (www.asthmacontrol.com)
management of asthmaAll patients should be assessed to establish their treatment regi-men and that they are on the appropriate control for their level. This may mean either increasing or decreasing their treatment. However, before any changes are made to the patient’s regimen, inhaler technique and concordance with medication should be established (GINA, 2012). Each patient is assigned to one of five
A. ASSeSSmeNT Of cuRReNT clINIcAl cONTROl (PRefeRAbly OveR 4 weeKS)
chARAcTeRISTIc cONTROlled(All of the following)
PARTly cONTROlled(Any measure present)
uNcONTROlled
daytime symptoms None (twice or less/week) More than twice /week
Three or more features of partly controlled asthma*†
limitation of activities None Any
Nocturnal symptoms/awakening None Any
Need for reliever/rescue treatment
None (twice or less/week) More than twice /week
lung function (Pef or fev1)‡ Normal <80% predicted or personal best (if known)
One in any week†
exacerbations None One or more per year*
B. ASSeSSmeNT Of fuTuRe RISK (RISK Of exAceRbATIONS, INSTAbIlITy, RAPId declINe IN luNG fuNcTION, SIde effecTS)
Features that are associated with increased risk of adverse events in the future include:Poor clinical control, frequent exacerbations in the past year*, ever admission to critical care for asthma, low FEV1, exposure to cigarette smoke, high dose medications.
* Any exacerbation should prompt review of maintenance treatment to ensure that it is adequate† By definition, an exacerbation in any week makes that an uncontrolled asthma week‡ without administration of bronchodilator, lung function is not a reliable test for children 5 years and younger
Complete control of asthma is commonly attained with treatment, the aim of which should be to achieve and maintain control for prolonged periods with due regard to safety of treatment, potential for adverse effects, and cost.The Asthma Control Test (ACT) is a useful tool for patients to check their level of control at home. For further information see www.asthmacontroltest.com and www.asthmasociety.ie.
Table 1: Assessing the level of asthma control (GINA, 2012)
Patients should be offered self-management plans with instructions on how to adjust their medications in response to worsening symptoms and/or worsening PefR.

fl utiform® (FLUTICASONE PROPIONATE AND FORMOTEROL FUMARATE) PRESSURISED INHALATION SUSPENSION. Prescribing Information Ireland. Please read the Summary of Product Characteristics before prescribing.Presentation: Pressurised inhalation suspension, in a pressurised metered dose inhaler (pMDI), containing fl uticasone propionate and formoterol fumarate dihydrate at strengths of 50 µg/5 µg, 125 µg/5 µg or 250 µg/10 µg per actuation. Indications: Regular treatment of asthma where the use of a combination product (inhaled corticosteroid and long-acting ß2-agonist) is appropriate: For patients not adequately controlled with inhaled corticosteroids and ‘as required’ inhaled short-acting ß2-agonist (SABA), or for patients already adequately controlled on both an inhaled corticosteroid and a long-acting ß2-agonist (LABA). fl utiform 50 µg/5 µg and 125 µg/5 µg per actuation are indicated for use in adults and adolescents 12 years and above. fl utiform 250 µg/10 µg per actuation is only indicated for use in adults. Dosage and administration: For inhalation use. The patient should be shown how to use the inhaler correctly by a physician or other healthcare professional. Patients should be given the strength of fl utiform containing the appropriate fl uticasone propionate dose for their disease severity (note that fl utiform 50 µg/5 µg per actuation is not appropriate in patients with severe asthma). The appropriate strength should be taken as two inhalations, twice-daily (normally in the morning and evening) and used every day, even when asymptomatic. fl utiform should not be used in children under 12 years. Prescribers should be aware that in asthmatics, fl uticasone propionate is as effective as some other inhaled steroids when administered at approximately half the total daily microgram dose. Total daily dose can be increased if asthma remains poorly controlled by administering a higher strength inhaler. Appropriate doses of the ß2-agonist and inhaled corticosteroid (ICS) in separate inhalers, or the ICS alone, should be prescribed if a patient requires doses outside the recommended dose regimens. Patients should be assessed regularly and once asthma is controlled, treatment should be reviewed and stepped down to the lowest effective dose, or an ICS alone. It is extremely important to regularly review patients as their treatment is stepped down. ICSs alone are fi rst line treatment for most patients. fl utiform is not intended for initial treatment of mild asthma. For patients with severe asthma the ICS therapy should be established before prescribing a fi xed-dose combination product. Patients on fl utiform must not use an additional LABA. An inhaled SABA should be taken for immediate relief of asthma symptoms arising between doses. The AeroChamber Plus® spacer device is recommended in patients who fi nd it diffi cult to use inhalers; re-titration should always follow the introduction of a spacer device. Patients should be advised to contact their prescriber when the fl utiform dose indicator is getting near zero.Contra-indications: Hypersensitivity to any of the active substances or excipients. Precautions and warnings: fl utiform should not be used for the fi rst treatment of asthma, to treat acute asthma symptoms or for prophylaxis of exercise-induced asthma. It should not be initiated during an exacerbation, during signifi cantly worsening or acutely deteriorating asthma, and should not be stopped abruptly. Patients should use their fl utiform maintenance treatment as prescribed, even when asymptomatic. If a patient experiences serious asthma-related adverse events or exacerbations, they should continue treatment but also seek medical advice. Patients should be reviewed as soon as possible if there is any indication of deteriorating asthma control. In the case of sudden and progressive deterioration, which is potentially life-threatening, an urgent medical assessment should be carried out. Use with caution in patients with: pulmonary tuberculosis; quiescent tuberculosis; fungal, viral or other infections of the airway; thyrotoxicosis; pheochromocytoma; diabetes mellitus (consider additional blood sugar controls); uncorrected hypokalaemia; predisposition to low levels of serum potassium; impaired adrenal function (monitor HPA axis function regularly) ; hypertrophic obstructive cardiomyopathy; idiopathic subvalvular aortic stenosis; severe hypertension; aneurysm or other severe cardiovascular disorders. There is risk of potentially serious hypokalaemia with high doses of ß2-agonists or concomitant treatment with ß2-agonists and drugs that can induce or potentiate a hypokalaemic effect. Particular caution is recommended in unstable or acute severe asthma and other conditions when the likelihood for hypokalemia adverse effects is increased. Monitoring of serum potassium levels is recommended during these circumstances. Formoterol may induce prolongation of the QTc interval. Caution must be observed when treating patients with existing prolongation of QTc interval. fl utiform should be discontinued immediately if there is evidence of paradoxical bronchospasm. Systemic effects with an ICS may occur, particularly at high doses for prolonged periods or when combined with potent CYP3A4 inhibitors, but are less likely than with oral corticosteroids. Use of a spacer device may also cause an increased systemic exposure. Increased exposure can be expected in patients with severe hepatic impairment. Prolonged
treatment with high doses of corticosteroids may result in adrenal suppression and acute adrenal crisis, particularly in adolescents and children or potentially as a result of trauma, surgery, infection or rapid dose reduction. Patients should be advised that fl utiform contains a small amount of ethanol; however this negligible amount does not pose a risk to patients. fl utiform is not recommended in children under 12 years of age. Interactions: Caution is advised in long-term co-administration with strong CYP3A4 inhibitors (e.g. ritonavir, atazanavir, clarithromycin, indinavir, itraconazole, nelfi navir, saquinavir, ketoconazole and telithromycin); co-administration should be avoided if possible. Ritonavir in particular should be avoided, unless the benefi ts outweigh the risks of systemic side-effects. Caution is advised with use of non-potassium sparing diuretics (e.g. loop or thiazide), xanthine derivatives, glucocorticosteroids, L-Dopa, L-thyroxine, oxytocin, alcohol or other adrenergic drugs. There is an increased risk of arrhythmias in patients receiving concomitant anaesthesia with halogenated hydrocarbons. Hypokalaemia may increase the risk of arrhythmias in patients being treated with digitalis glycosides. Concomitant use of ß-adrenergic drugs can have a potentially additive effect. Extreme caution should be taken when using formoterol fumarate with drugs known to prolong the QTc interval, such as tricyclic antidepressants or MAOIs (and for two weeks following their discontinuation), as well as antipsychotics (including phenothiazines), quinidine, disopyramide, procainamide and antihistamines. Concomitant use of an MAOI or a similar agent, such as furazolidone or procarbazine, may precipitate hypertensive reactions. ß-blockers and formoterol fumarate may inhibit the effect of each other. ß-blockers may produce severe bronchospasm in asthma patients, and they should not normally be treated with ß-blockers including those that are used as eye drops to treat glaucoma. Under certain circumstances, e.g. as prophylaxis after myocardial infarction, cardioselective ß blockers could be considered with caution Pregnancy and lactation: fl utiform is not recommended during pregnancy. It should only be considered if benefi ts to the mother outweigh risks to the foetus. It is not known whether fl uticasone propionate or formoterol are excreted in breast milk; a risk to the breast feeding infant cannot be excluded. A decision should be made on whether to discontinue breastfeeding or discontinue/abstain from fl utiform. Side-effects: Potentially serious side-effects: hyperglycaemia; depression; aggression; behavioural changes (predominantly in children); paradoxical bronchospasm; agitation; vertigo; palpitations; ventricular extrasystoles; angina pectoris; tachycardia; hypertension; dyspnoea; peripheral oedema; Cushings Syndrome; adrenal suppression; growth retardation; cataract and glaucoma; hypersensitivity reactions and QTc interval prolongation. Please consult the SPC for details of non-serious side-effects and those reported for the individual molecules. Legal category: POM Package quantities: One inhaler containing 120 actuations 50 µg/5 µg, 125 µg/5 µg, 250 µg/10 µg Marketing Authorisation numbers: PA 1688/13/1-3 Marketing Authorisation holder: Mundipharma Pharmaceuticals Limited, Millbank House, Arkle Road, Sandyford, Dublin 18, Ireland. Member of the Mundipharma Pharmaceutical Group. For medical information enquiries, please contact [email protected] of preparation: January 2013
Reference:1. fl utiform Summary of Product Characteristics
® FLUTIFORM is a registered trademark of Jagotec AG, and is used under licence.® AEROCHAMBER and AEROCHAMBER PLUS are registered trade marks of Trudell Medical International. © 2012 Mundipharma Pharmaceuticals Limited.
Adverse events should be reported. Reporting forms and information can be found at http://www.imb.ie/EN/Safety--Quality/Online-Forms/Human- Medicine-Adverse-Drug-Reaction.aspx Adverse events should also be reported to Mundipharma Pharmaceuticals Limited on 01 206 3800/1800 991830 (outside offi ce hours).
IRE/FL-12042
A P O W E R F U L P A R T N E R S H I P
NEW
fluticasone propionate/formoterolfl utiform is indicated for the regular treatment of asthma in adults and adolescents (12 years and over),where use of a combination product (inhaled corticosteroid [ICS] and long-acting ß2-agonist [LABA]) is appropriate. fl utiform 250/10µg indicated in adults only.
Rapid onset* andlong lasting effi cacy**
COMBINATION
Modern aerosol device with a patient-facing dose counter1
INNOVATION
Modern aerosol device with a patient-facing dose counter
INNOVATION
* Open label study, signifi cant increase in FEV1 5 mins after dosing (p=o.oo1) (Aalbers et al: Onset of Bronchodilationwith fl uticasone/formoterol combination versus fl uticasone/salmeterol in an open-label, randomised study; Adv Ther 2012)** 6-12 month open label study, signifi cant improvement in spirometric secondary endpoints vs baseline (Mansur et al,Long Term Safety and Effi cacy of fl uticasone/formoterol combination therapy in Asthma; JAMP -Vol 25, No0, 2012 p1-10)
NEW
50/5 µg 125/5 µg 250/10 µg
The NEW asthma maintenance treatment

18
clinical review
Ongoing monitoring is essential to maintain control and establish the lowest dose of medication for optimal control. If asthma is not controlled, treatment should be stepped up. If partly controlled, consider stepping up. If asthma is controlled for at least 3 months, consider stepping down treatment. The goal of treatment is to be on the least amount of medication to maintain optimal control.
Patients should be offered self-management plans with instructions on how to adjust their medications in response to worsening symptoms and/or worsening PEFR. An example of a self-management plan is available on www.asthmasociety.ie
Non-pharmacological management of asthma includes management of trigger factors, smoking cessation, management of obesity and annual influenza vaccination. Identification and management of allergic rhinitis, sinusitis and nasal polyposis is required as the presence of these conditions may exacerbate asthma. Also, the management of gastro-oesophageal reflux can exacerbate asthma and symptoms may improve when reflux is corrected. Hormones can also play a
significant role in asthma control. Some patients will experience worsening of their asthma symptoms pre-menstrually or during menstruation. During pregnancy, asthma control may improve, disimprove or stay the same as pre-pregnancy.
Inhaled glucocorticosteroids in asthmaInhaled glucocorticosteroids are the cornerstone of asthma treatment. Table 3 outlines the treatment options available to patients.
All patients with asthma should be monitored and assessed at frequent intervals. Table 4 illustrates the management approach based on control.
conclusionThis article has reviewed the updated Asthma Control in General Practice Adapted from the GINA Global Strategy for Asthma Management & Prevention (2012). The diagnosis and management of stable asthma in adults has been discussed from a primary care perspective.
Step 1: As-needed reliever medication
As-needed reliever medication only is reserved for:•Untreatedpatientswithoccasionaldaytimesymptomsofcough/wheeze/dyspnoea occurring twice or less/week, lasting only a few hours•Patientswhoareasymptomaticbetweenepisodes,withnormalFEV1•PatientswithnonocturnalwakeningFor the majority of patients a rapid-acting inhaled β2-agonist is the rec-
ommended reliever treatment (evidence A). An inhaled anticholinergic, short-acting oral β2-agonist, or short-acting theophylline may be consid-ered as alternatives, but they have a slower onset of action and a higher risk of side effects (evidence A). when symptoms are more frequent, and/or worsen periodically, patients require regular controller medica-tion (Step 2 or higher) in addition to as-needed reliever medication.
Step 2: As-needed reliever medication plus a single controller
Step 2 is the initial treatment for most treatment-naïve patients with persistent asthma symptoms. All newly diagnosed patients should be reviewed within 2–4 weeks after treatment initiation.
A low-dose inhaled glucocorticosteroid (ICS) is recommended as the initial controller treatment for asthma patients of all ages (Evidence A). Alternative controller medications include leukotriene modifiers (Evi-dence A) appropriate for patients unable/unwilling to use ICS, or who experience intolerable side effects such as persistent hoarseness from
ICS. Sustained-release theophylline has only weak anti-inflammatory and controller efficacy (Evidence B), is commonly associated with side effects and is not recommended for routine use as initial or first-line controllers in Step 2. Cromones have comparatively low efficacy, though a favourable safety profile (Evidence A).
Step 3: As-needed reliever medication plus one or two controllers
The recommended option for children older than 6, adolescents and adults is to combine a low dose of ICS with an inhaled long-acting β2-agonist, either in a combination inhaler or as separate components (evidence A). Due to the additive effect of this combination, the low dose of ICS is usually sufficient, and need only be increased if control is not achieved within 3–4 months with this regimen (evidence A). If a combination inhaler containing formoterol and budesonide is se-lected, it may be used for both rescue and maintenance. This approach has been shown to result in reductions in exacerbations and improve-
ments in asthma control in adults at relatively low doses of treatment (evidence A).Another option, for both adults and children, is to increase to a medium-dose ICS (evidence A). For patients of all ages use of a spacer device is recommended to improve delivery to the airways, and reduce systemic absorption (evidence A).Another option at Step 3 is to combine low-dose ICS with leukotriene modifiers (evidence A) or alternatively the use of slow-release theophyl-line at low dose may be considered (evidence B).
Step 4: As-needed reliever medication plus two or more controllers
The selection of treatment at Step 4 depends on prior selections at Steps 2 and 3. The order in which additional medications should be added is based upon evidence of their relative efficacy in clinical trials. where possible, patients not controlled on Step 3 should be referred to a health professional with expertise in the management of asthma for investigation of alternative diagnoses and/or causes of difficult to-treat asthma.The preferred treatment at Step 4 is to combine a medium – or high dose ICS with a long acting inhaled β2-agonist. However, in most patients, the increase from a medium – to a high-dose ICS provides relatively little additional benefit (evidence A). The high dose is recom-mended only on a trial basis for 3 to 6 months when control cannot
be achieved with a medium-dose ICS combined with a longacting β2-agonist and/or a third controller (e.g. leukotriene modifiers or sustained release theophylline evidence B).At medium and high doses, twice-daily dosing is necessary for most but not all ICS (evidence A). with budesonide, efficacy may be improved with more frequent dosing (four times daily evidence B).Patients who do not reach an acceptable level of control at Step 4 can be considered to have difficult-to-treat asthma. These patients may have an element of poor glucocorticosteroid responsiveness and may require higher doses of ICS. There is no evidence to support continuing these high doses of ICS beyond 6 months. It is uncommon that patients are completely resistant to glucocorticosteroids.
Step 5: As-needed reliever medication plus additional controller options
Addition of oral glucocorticosteroids to other controller medications may be effective (evidence D) but is associated with severe side effects (evidence A) and should only be considered if the patient’s asthma re-mains severely uncontrolled on Step 4 medications with daily limitation of activities and frequent exacerbations. Patients should be counselled
about potential side effects. Addition of anti IgE treatment has been shown to improve control of severe allergic asthma when control has not been achieved on combinations of other controllers including high doses of inhaled or oral glucocorticosteroids (evidence A).
Table 2: Treatment steps (GINA, 2012)
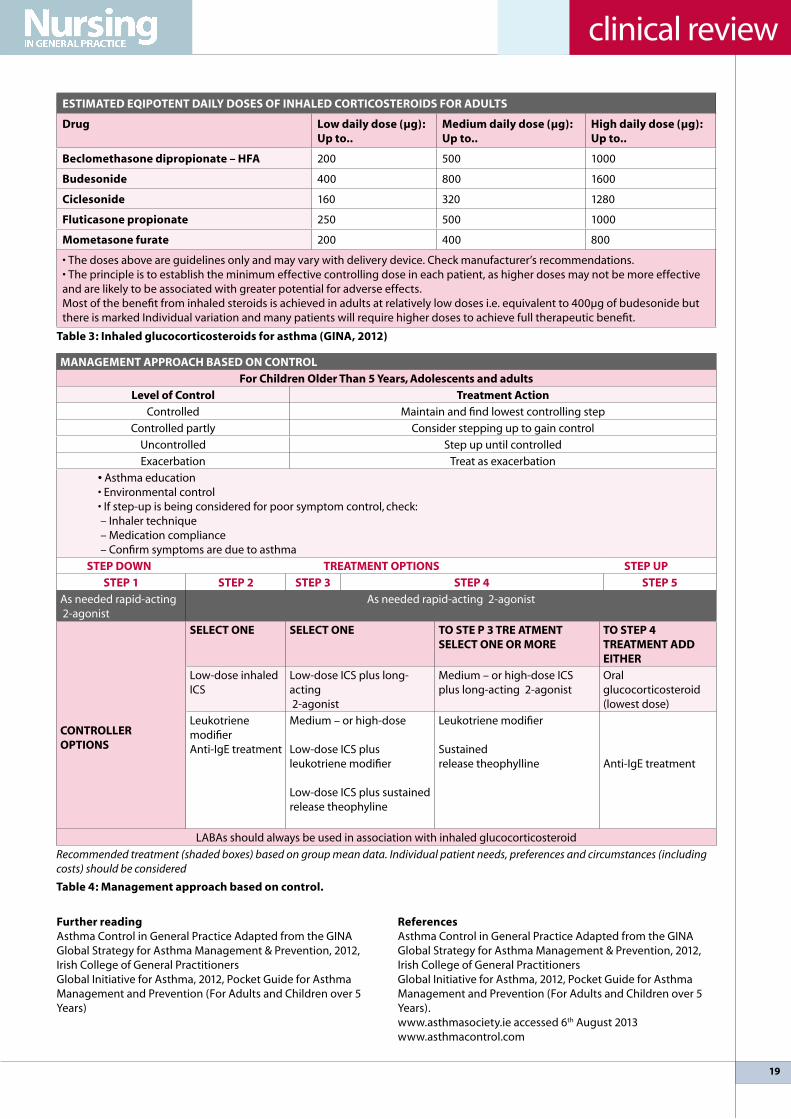
19
clinical review
eSTImATed eqIPOTeNT dAIly dOSeS Of INhAled cORTIcOSTeROIdS fOR AdulTS
drug low daily dose (µg): up to..
medium daily dose (µg): up to..
high daily dose (µg): up to..
beclomethasone dipropionate – hfA 200 500 1000
budesonide 400 800 1600
ciclesonide 160 320 1280
fluticasone propionate 250 500 1000
mometasone furate 200 400 800
•Thedosesaboveareguidelinesonlyandmayvarywithdeliverydevice.Checkmanufacturer’srecommendations.•Theprincipleistoestablishtheminimumeffectivecontrollingdoseineachpatient,ashigherdosesmaynotbemoreeffectiveand are likely to be associated with greater potential for adverse effects.Most of the benefit from inhaled steroids is achieved in adults at relatively low doses i.e. equivalent to 400µg of budesonide but there is marked Individual variation and many patients will require higher doses to achieve full therapeutic benefit.
Table 3: Inhaled glucocorticosteroids for asthma (GINA, 2012)
further readingAsthma Control in General Practice Adapted from the GINA Global Strategy for Asthma Management & Prevention, 2012, Irish College of General PractitionersGlobal Initiative for Asthma, 2012, Pocket Guide for Asthma Management and Prevention (For Adults and Children over 5 Years)
mANAGemeNT APPROAch bASed ON cONTROl
for children Older Than 5 years, Adolescents and adults
level of control Treatment Action
Controlled Maintain and find lowest controlling step
Controlled partly Consider stepping up to gain control
uncontrolled Step up until controlled
Exacerbation Treat as exacerbation
• Asthma education•Environmentalcontrol•Ifstep-upisbeingconsideredforpoorsymptomcontrol,check: – Inhaler technique – Medication compliance – Confirm symptoms are due to asthma
STeP dOwN TReATmeNT OPTIONS STeP uP
STeP 1 STeP 2 STeP 3 STeP 4 STeP 5
As needed rapid-actingβ2-agonist
As needed rapid-acting β2-agonist
cONTROlleR OPTIONS
SelecT ONe SelecT ONe TO STe P 3 TRe ATmeNT SelecT ONe OR mORe
TO STeP 4 TReATmeNT Add eITheR
low-dose inhaled ICS
low-dose ICS plus long-actingβ2-agonist
Medium – or high-dose ICSplus long-acting β2-agonist
Oral glucocorticosteroid(lowest dose)
leukotriene modifierAnti-IgE treatment
Medium – or high-dose
low-dose ICS plusleukotriene modifier
low-dose ICS plus sustainedrelease theophyline
leukotriene modifier
Sustainedrelease theophylline Anti-IgE treatment
lABAs should always be used in association with inhaled glucocorticosteroid
Recommended treatment (shaded boxes) based on group mean data. Individual patient needs, preferences and circumstances (including costs) should be considered
Table 4: management approach based on control.
ReferencesAsthma Control in General Practice Adapted from the GINA Global Strategy for Asthma Management & Prevention, 2012, Irish College of General PractitionersGlobal Initiative for Asthma, 2012, Pocket Guide for Asthma Management and Prevention (For Adults and Children over 5 Years).www.asthmasociety.ie accessed 6th August 2013www.asthmacontrol.com

20
clinical review
Role of the PN in the National cancer control ProgrammehIlARy muRPhy, NuRSE SPECIAlIST, NATIONAl CANCER CONTROl PROGRAMME
The National Cancer Control Programme aims to minimise the burden of cancer in Ireland through a ‘whole population, integrated cohesive approach that involves prevention, screening, diagnosis, treatment and support’. Nurses working in primary care are
ideally placed to help their practice population reduce their risk of cancer through lifestyle changes; improve their uptake of appropriate screening programmes; increase awareness of concerning symptoms and facilitate rapid review and referral within the practice; and support those diagnosed with cancer through their journey. The NCCP cancer education programme for nurses working in primary care supports nurses with the tools to take on this critical role in cancer control.
Introduction Cancer is a common illness, with over 32,500 people in Ireland diagnosed with cancer annually.1 Given our ageing population, we are facing an enormous challenge, with the number of new cancers in Ireland expected to double over the next 20 years.
In 2007, the National Cancer Control Programme (NCCP) was established to implement the recommendations of the National Cancer Strategy.2 The Strategy defined cancer control as a ‘whole population, integrated cohesive approach that involves prevention, screening, diagnosis, treatment and support.’
Restructuring of cancer services involved the designation of eight cancer centres in which complex diagnostic and treatment developments would be concentrated, to ensure best outcomes for patients. However, the strategy also recognised the need to build capacity within primary and community care, so that health professionals in the community sector can play a greater part in cancer control.
Nurses in primary care are ideally placed to help their
practice population to reduce their risk of cancer through lifestyle changes; improve their uptake of appropriate screening programmes; increase awareness of concerning symptoms and facilitate rapid review and referral within the practice; and support those diagnosed with cancer through their journey.
cancer preventionwe now know that more than half of all cancers could be prevented through lifestyle changes – as smoking contributes to 30% of cancers, diet and lack of physical activity to 35% and alcohol to approximately 5%.
The NCCP has developed information materials for the public (available at www.cancercontrol.hse.ie) on lifestyle changes that can reduce cancer risk. Making such changes is not always easy however and is dependent on more than provision of information. People also require support and motivation, to feel empowered to make such changes. Evidence supports the ability of nurses in primary care to intervene and effect such positive change.
The NCCP training programme for nurses in primary care (outlined in more detail below) aims to provide nurses with strategies to employ, in bringing about healthier lifestyles in their practice population. For example, the techniques used in motivational interviewing3 centre on motivational processes within the individual themselves to facilitate change.
Specifically in relation to smoking cessation skills, online learning is available for community health care professionals, with the support of the Irish Practice Nurses Association, at www.promotingsmokingcessation.ie . The NCCP is now also working on specific pharmacotherapy guidelines, to assist heath care professionals in the treatment of tobacco dependence.
21
clinical review
cancer ScreeningIreland has a number of quality-assured, free, government-funded screening programmes in place. The National Cancer Screening Service (NCSS) has responsibility for three established cancer screening programmes and a non-cancer screening programme for diabetic retinopathy. All programmes are free to those eligible and have been designed to make them as accessible and user-friendly as possible.
The primary care community play a key role in supporting screening programmes. Research indicates that the biggest influence on a person to participate in a screening programme is encouragement from their GP. • BreastCheck – The National Breast Screening Programme
offers women aged 50 to 64 (over 430,000 women) a free mammogram every two years and screening began in February 2000. As of 30 November 2011, 5,071 cancers from the 826,210 mammograms provided to 368,851 women were identified. www.breastcheck.ie or Freephone 1800 45 45 55
• CervicalCheck – The National Cervical Screening Programme offers free smear tests to women aged 25 to 60 (over 1.3 million women). During 2011 alone pre-cancerous abnormalities were detected in 8,091 women and cervical cancer was identified in 104 women. www.cervicalcheck.ie or Freephone 1800 45 45 55
• BowelScreen – The National Bowel Screening Programme is a recently commenced programme for the early detection of bowel cancer in men and women aged 55-74 (over 1 million people). The programme is initially aimed at people aged 60 to 69 years and may take up to three years for the first round, after which each round should be completed in two
Nurses in primary care are ideally placed to help their practice population to reduce their risk of cancer…increase awareness of concerning symptoms,… facilitate rapid review and referral within the practice; and support those diagnosed with cancer through their journey.
designated cancer centres
A Strategy for cancer control in Ireland 2006ap
The New bowelscreen Programme
having your Prostate checked: A Guide for men

22
clinical review
years. Bowel screening is a simple home test that looks for tiny amounts of blood in the bowel motion which are not visible to the eye. The home test does not confirm if there is bowel cancer but it identifies people who require further investigation. www.bowelscreen.ie or Freephone 1800 45 45 55
PSA testingProstate cancer concerns and requests for PSA testing are common issues in primary care. The prostate cancer referral guideline (referred to further below) outlines the steps in investigation of a man with symptoms suggestive of prostate cancer. It is important to note that there is currently no evidence to support a national population-based prostate cancer screening programme, as the potential risks outweigh the potential benefits.4 An asymptomatic man who wishes to have his prostate checked should be fully informed of the advantages and disadvantages, and understand that an accurate assessment requires both PSA testing and a digital rectal examination of the prostate. The NCCP has produced a booklet to support this discussion with men – ‘A guide for men. Having your prostate checked – what you should know’.
Referral for suspected cancerGP referral guidelines have been developed to assist in the recognition and investigation of suspicious symptoms for the commoner cancers, i.e. lung, breast, prostate and malignant melanoma skin cancer. National referral forms for these four
cancers are also available. Rapid access clinics for urgent lung and prostate referrals are located in all eight designated cancer centres. Breast referrals can be sent to any of the cancer centres, plus the satellite unit in letterkenny. Referrals for possible melanomas should be sent to the local consultant dermatologist or plastic surgeon.
The NCCP Electronic Cancer Referral Project commenced in 2008 and is now live nationwide for breast, prostate and lung cancer referrals in all eight cancer centres. Once the GP sends an electronic cancer referral via Healthlink (www.healthlink.ie), an immediate acknowledgment is given. In addition the cancer team sends a response to the GP with the date of the patient’s appointment, within five working days. There is now direct referral to the cancer service via the four ICGP accredited GP practice management software systems (Complete GP, Helix Practice, Manager, Health One, Socrates). The number of electronic cancer referrals is increasing each year, and currently 30% of all breast, prostate and lung cancer referrals are sent electronically nationwide.
Some symptoms may cause great concern, even if not associated with cancer. An example of this is cyclical breast pain, which is very common but not an alarm symptom for breast cancer, especially in the under 35s. The NCCP has produced a breast pain booklet and diary, to assist primary care health care professionals in the assessment and management of a woman with a normal clinical breast examination, who is suffering from cyclical breast pain. This can also be downloaded as a free App for iphones or smart phones.
diagnosis, treatment and survivalNCCP expert tumour groups have been brought together for the common cancers, to draw up national guidelines as to the diagnosis and treatment. Cancer treatment is still primarily hospital based but certain supportive measures can be carried out safely in the community, such as care of central venous access devices. The community oncology nurse education programme is an initiative to give public health nurses the skills to provide such care in the patient’s own home, with the support of the local treating medical oncology unit. The pilot programme has been favourably evaluated. Public health nurses undertaking the enhanced programme will now receive university accreditation.
It is a great achievement that long-term survival from cancer has increased so much in Ireland over the past decade. Survival at five years has increased from 42% in 1994-1999 to 60% in 2005-2009 in men and from 52% to 62% in women. Survival for some cancers–testis, prostate and thyroid–is now over 90% at five years.1 Increasingly, cancer survivors can be expected to lead healthy and fulfilling lives after their treatment. It is important that they, and the health care professionals they
The NccP training programme for nurses in primary care aims to provide nurses with strategies to employ, in bringing about healthier lifestyles in their practice population.
A Strategy and educational framework for Nurses caring for People with cancer in Ireland
National Prostate cancer GP Referral Guidelines
National lung cancer GP Referral Guidelines

23
clinical review
come in contact with, appreciate the ways in which they can maximise their health – whether this is general lifestyle measures, undergoing regular surveillance, or understanding how to cope with side effects of their treatment or with anxiety or distress after a cancer diagnosis. The NCCP is currently developing survivorship care plans, to support patients and health care professionals with this.
cancer education for nurses working in primary careThe national strategy and educational framework for nurses caring for people with cancer in Ireland5 was developed in part-nership with the Office of the Nursing and Midwifery Division (OMNSD). It describes the competencies required by nurses to care for patients with cancer in both generalist and specialist healthcare settings. All cancer education programmes for nurses sit within this strategy.
Since 2011 the NCCP has provided a two day cancer educa-tion programme for nurses who work in the primary and com-munity care, covering the following four modules:• Cancer prevention and principles of motivational interview-
ing techniques • Cancer screening: BreastCheck, CervicalCheck and BowelS-
creen (the new colorectal cancer screening programme) • Clinical presentation of the common cancers, referral path-
ways and holistic treatment • Psychosocial, support and communication aspects for the
person living with cancerThe programme aims to enhance nurses’ knowledge and
skills to enable them play a key role in cancer control in the primary care setting. It is approved by Nursing and Midwifery Board of Ireland and accredited for 13 Continuing Education units (CEu). It is delivered in designated cancer centres, with video links to other hospitals and regional Centre of Nurse Midwifery Education (CNME), and to date over 600 nurses have participated. There are also plans to develop e-learning modules in the future, to help overcome barriers to participation in the current training programme.
On completion of the course, the nurse in primary care should be able to:• Have an enhanced awareness of the impact of modifiable
lifestyle cancer risk factors e.g. smoking, alcohol, nutrition, obesity, physical activity and uV radiation exposure and how to apply suitable evidence-based prevention interventions
• Critically discuss motivational interviewing techniques in the context of encouraging people to adopt a healthy lifestyle
• Discuss the implementation of evidence based strategies in primary care to promote optimal uptake of cancer screening
breast Pain: A Guide for womenbreast Pain App
• Recognise symptoms suspicious of cancer• Critically discuss the referral pathway for patients from
primary care to the specialist cancer services for the common cancers e.g. breast, prostate, lung and skin
• Discuss the role of the multi-disciplinary team (MDT) in the assessment, diagnosis and treatment of cancer
• Discuss the different treatment modalities for common cancers
• Recognise and discuss the psychological aspects of a cancer diagnosis; living with cancer as a chronic condition; the role of the nurse in providing patient support in conjunction with the multidisciplinary primary care team. Those interested in attending the course should contact their
Regional Centre of Nurse Midwifery Education, their Profes-sional Development Coordinator for Practice Nursing or email [email protected].
Additional informationThe NCCP website www.cancercontrol.hse.ie contains further information on the programme and has downloadable copies of referral guidelines, patient information leaflets etc. For hard copies of any materials, please phone 01 8287100 or email [email protected]
For further information on the National Cancer Screening Service, check the website www.cancerscreening.ie
Online smoking cessation training is available at www.promotingsmokingcessation.ie
Information on electronic referral is available on the NCCP website. To register with healthlink, go to www.healthlink.ie
References1. National Cancer Registry. Cancer in Ireland 2013: Annual
report of the National Cancer Registry. Cork: National Cancer Registry Ireland; 2013
2. Department of Health and Children. A Strategy for Cancer Control in Ireland. Dublin: Stationary Office; 2006
3. Miller wR, Rollnick S. what’s new since MI-2?. In: International Conference on Motivational Interviewing; 2010 June 6; Stockholm, Sweden. Available from: http://www.motivationalinterview.org/quick_links/about_mi.html
4. Moyer VA, uS Preventive Services Task Force. Screening for prostate cancer: u.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;157(2):120-134.
5. Hanan T, laffoy, M, wynne, M. A strategy and educational framework for nurses caring for people with cancer in Ireland. Dublin: NCCP/ONMSD; 2012

Old Issues –New Ideas The 18th Annual National conference
11th-12th October, Radisson Blu, Athlone
conference Timetablefriday 11th October12.00 –14.00 Registration, Tea/Coffee, Exhibitions14.00 –14.15 Opening address14.15 –15.00 dr.catherine conlon, HSE Crisis
Pregnancy Programme-Astudy of migrant women’s sexual and reproductive health
15.00–15.45 Philip James, CNS, Adolescence Substance Abuse, Y.O.D.A. Tallaght.
15.45 –16.15 deirdre carmody, Drug liaison midwife CoombeHospital
16.15 –16.30 Questions and Answers16:30 –18:00 Exhibition19.00 –20.30 Gala Dinner20.30–21:30 Key Note: mary Scott’s Good Sexual
history21:30 Awards –including Practice Nurse of the
Year Award22:00 Entertainment
Saturday 12th October08:30–09:30 Exhibition09.30–09:45 Opening address09.45 –10.30 Prof. donal O’Shea, Obesity and the
Immune System, St Vincent’s Hospital.10.30 –11.15 dr Jay Sharma, Hypertension,
Midlands Hospital Portlaoise.11.15 –11.30 Questions and Answers11.30 –12.30 Coffee and Exhibition12.30 –13.15 dr Patrick Ormond, Dermatology,St
James Hospital13:15–13:30 Questions and Answers13:30 Presentation of Valerie Mangan Award13.45–14:30 lunch14:30 AGM
The Annual Irish Practice Nurse Association conference is the only National conference dedicated to nurses working in General Practice in Ireland. Attendance is open to all 700 members of the association as well as associate members.
The 2013 conference hosted by the members of North Dublin branch will be held at the centrally-located RadissonBluHotel in Athlone(www.radissonblu.ie/hotel-athlone)
Network with the Primary care frontline
with the continued expansion of primary care in Ireland, practice nurses are having a greater input into practice purchasing decisions than ever before. Join us for the 18th annual conference and exhibition. Attendance is a great way to gain accredited education whilst networking with fellow nurses.
Practice Nurses–Ready to learn
The IPNA conference continues to move with the times. The agenda is topical and the educational opportunities it provides are invaluable. we know you are keentocontinually improve the quality of care you offer your patients,so we have designed an event that gives you real information that will remain useful long after the event is over.
engaging conference – The conference programme has been designed to provide innovative insight and an overview of the latest developments within an enjoyable and mutually educational environment.
exhibition – Our exhibition provides an informal environment to talk to companies to learn about the latest products, services and equipment that are relevant to you.

25
training
understanding and supporting couple relationships dR mAeve huRley, GENERAl PRACTITIONER AND lEAD, BRIEF ENCOuNTERS
This is a report on the delivery of a new format of Brief Encounters training; using an e-learning component supported by a one day workshop.
The overall aim of the programme is to enable practitioners to offer preventive interventions in troubled relationships as part of routine care of couples and their families” (Brief Encounters 2013). This is especially relevant in our country’s present
recession with many families being affected by unemployment and austerity as they struggle to maintain their families as best they can.
Ag Eisteacht is the charity that runs the Brief Encounters training here in Ireland. Ag Eisteacht has a license agree-ment with One Plus One, a uK based charity with over 30 years research in the area of relationships.
The pilot was run by Rhonda Forsythe, Professional Develop-ment Co-Ordinator for Practice Nurses, who advertised and re-cruited for the course and who herself had previously attended the 3 day Brief Encounters training.
The advertisement read: OnePlusOne’s Dept. of Education funded relationship support programme has been delivered to 3000 practitioners in the uK and you can be part of the first group in Ireland…
The programme consists of an award winning blended e-learning online module which takes approximately 2 hours
to complete including reading material, followed by a one day facilitated skills workshop.
The online module provides you with the latest knowledge about what makes relationships work and why it is important to keep in mind the adult relationship when working with your patients. Incorporated in this module are a series of evidence based relationship insights to help understand what is really going on.
The module then introduces the Brief Encounters model which is explored further at the facilitated workshop. The e-learning module prepares you for the workshop and needs to be completed prior to attending.
The Skills workshop is designed to build on the learning from the module. It is a skills laboratory where you can see how to integrate the Brief Encounters model alongside the knowledge and relationship insights from the module into your work setting. using case examples, group work and skills practice, you will be able to see how to support your patients to explore and understand their experience, about what might help them work through their difficulties. This workshop, facilitated by two experienced trainers, will provide an opportunity to reflect on working with your patients and also how to use the skills and relationship theory in peer support and supervision.
“

26
training
course set up The workshop was held in Swords on May 7th 2013. A total of 13 participants completed the e-learning and workshop components. Nurses attended from different disciplines: Practice Nursing, Public Health Nursing, and Mental Health Nursing along with two Ag Eisteacht trainers and one intern who had previous listening skills training. The workshop was delivered by Maeve Hurley and leon ledwidge, Training Officer, workforce Development, Children and Family Services HSE Dublin NE. The Programme was awarded Category 1 Approval from the Nursing Midwifery Board of Ireland (NMBI) and carries an award of 6 ECus.
feedback: online module The e-learning was considered informative and helpful by participants. However, for the majority of those participants it took much longer to complete than the 2 hours recommended. Many advised that it required at least 3 hours to complete, along with additional time required for reading. Some individuals had problems accessing specific elements of the programme and for some it was their first experience of e-learning.
In general, participants found the online modules very informative and positively evaluated them. It gives the practitioner adequate evidence based theory to support the workshop component. One consideration going forward might be to look at having shorter modules; this may increase the number of modules for completion over a longer period of time within a specific time limit.
feedback: workshopThe workshop component of the programme was very well received. The trainers were very highly evaluated by the majority of those participating. 92% stated that the trainers were well prepared, delivered the workshop well, created a good learning environment and encouraged participation of attendees.
One participant stated that the course far exceeded her expectations and how it will assist in improving her practice. It was considered that having the theory from the e-learning prior to the workshop was very helpful. Participants also stated that the programme would enable them to have more impact in their every day work. “I will have more confidence in my self-worth to engage clients if I suspect they are experiencing difficulties.”
Some participants suggested that it gave them a platform to build on managing their time at work; more effectively and efficiently. “I expect time-management to improve immensely as well as being more effective in my contacts”. Participants also suggested that the programme improved their listening skills. “The course far exceeded my expectations. I have learnt to step back and be a better listener and feel better equipped with the knowledge”. Many would have liked to have had additional time at the workshop and suggested this would have been helpful and beneficial.
Participants also commented that the training would be very helpful when dealing with multidisciplinary teams. All present enjoyed the programme, and found it relevant both for practice and everyday life. Many remarked that there was a good skills mix and learning environment, with a positive sharing of experiences among colleagues present.
In conclusionThe programme overall was a great success and all those who attended would recommend it. Going forward, the programme will benefit from more structure based around the Irish health system. Issues in relation to accessing the programme and estimated time to complete the e-learning programme will need to be addressed. Brief Encounters training not only benefits the patient/client but also benefits the health care professionals (HCPs) as it empowers them. The HCP learns how to use his/her listening skills and use their time more efficiently and effectively. Participants also suggested that a two day programme would be of benefit and could include Supervision/Support and Self Care. This highlights the need for better understanding, more education and courses addressing these specific areas.
Acknowledgements I would like to acknowledge Rhonda Forsythe (RGN RM BNS MSC Professional Development Co-ordinator Dublin NE) who provided commentary on this pilot initiative. Also the HSE’s support particularly Paul Fitzgibbon for releasing leon to facilitate this day. One Plus One provided the online access for this project at no cost and Rhonda organised the venue and refreshments.
It was a true collaborative effort and was further enhanced by the enthusiastic group of committed HCPs who attended and engaged making it an enriching experience for us all.
If you would like to enhance you or your teams’ effectiveness when supporting families at times of stress or those experiencing relationship difficulties, we are available to organise blended learning or 3 day courses throughout the country. For more information see www.ageisteacht.com or phone Maeve 086-1708092
The Skills workshop is designed to build on the learning from the module. It is a skills laboratory where you can see how to integrate the brief encounters model alongside the knowledge and relationship insights from the module into your work setting.

27
technology
Practice Nurses’ quality of lifeHow is your work/life balance these days?Did you just snort in total exasperation?!
lISA NOlAN
Nursing journals, research, blogs and all those on the front line of healthcare are increasingly referring to the fact that nurses and other healthcare profession-als are at breaking point. HCPs burned out, working harder than ever, doing longer hours but earning
less, seeing exasperated patients who have been waiting for longer than usual, often not having enough time to provide nursing care as thoroughly as they’d like.
Recent statistics from Scotland show that Practice Nurse con-sultations now account for 30% of all consultations in general practice there.1 There are 16 million consultations every year in general practices in Ireland.2 If the Scottish statistics were ap-plied here, then Practice Nurses in Ireland could be carrying out 4,800,000 consultations per year. First of all – wow. Secondly – yikes! No wonder a Google search of Nurse Burnout yields millions of results.

28
technology
of leisure time in maintaining a good quality of life. Engaging in leisure time activities, such as spending time with one’s fam-ily and friends, and being engaged in physical activities, can prevent burnout.”3
Even more seriously, “Sleep deprivation can impair job performance and increase risk for worker errors and injuries. Errors made by fatigued healthcare workers also can endanger patients.”4
So, for your sake and for those who depend on you, take a few minutes now to plan some changes (however small) to make a difference; to help you rearrange your life, refocus your priorities, ensure you allocate enough time for the good things in life or whatever you need to ensure the perfect balance for you.
Take action now!There is a vast array of websites and online resources offering time management tools. Most offer very useful tips, but this one can be done right now, as you are reading this, without having to log on to the internet. And it will only take 5 minutes!1. Get a pen and paper and actually write down what you do
every day. Everything. This includes sleeping, eating, exercis-ing, showering, commuting, work, housework, etc.
2. Sort this list in order of importance. 3. Allocate a specific amount of time for the essentials.4. Don’t forget that leisure time is essential! You would mark
a dental appointment in your calendar. Mark time in your diary to have a walk, catch up with an old friend, or to sit in an armchair with a book. I’m a big fan of the ‘free’ stuff, like spending 15 minutes lying outside on the grass beside your kids to spot shapes in the clouds. Doesn’t cost a cent, means so much to them and goes a small way towards protecting your mental health. Set aside the time for these and don’t stand yourself up or back out of your arrangement with yourself!
5. Allow some time every day and week for the unexpected, because life is life and emergencies happen.
6. Ruthlessly, (and I mean RuTHlESSlY!) identify the pointless things that steal your time and aren’t productive. Delegate these if you can afford to.
7. Relegate if you can’t.
Remember, life is short and graveyards are full of ‘indispensi-ble’ people. Now is the moment to stop and take a breath.
References1. General Practice – GP workforce and practice population
statistics to 2012, Information Services Division Scotland. www.idsscotland.org (direct link is on IPNA website, Re-search page)
2. Primary Care: A New Direction, Department of Health & Children http://www.dohc.ie/publications/fulltext/primary_care_new_direction/part_two.html
3. work satisfaction, quality of life, and leisure time of neonatology fellows and senior neonatologists in Is-rael, Israel Journal of Health Policy Research 2012, 1:50 doi:10.1186/2045-4015-1-50
4. Running on Empty: Fatigue and Healthcare Professionals. Medscape, Aug 02, 2012.
The well-documented increase in general practice workloads over the past 5 years means that Practice Nurses, just like their colleagues in secondary care, are now working at full speed throughout the day. Most Practice Nurses, by the nature of the experience required to do their job, have families. So we can as-sume you are all racing home from surgeries to multi-task there as well. Juggling work and family commitments was difficult enough during the Celtic Tiger era, but reduced incomes mean that now we are also trying to do more tasks ourselves to make ends meet; cooking every night of the week to avoid the cost of a takeaway; cutting the grass ourselves instead of paying the lo-cal lawnmower-owning budding entrepreneurs to do it. I’m sure you could add lots to this list yourself.
while constantly lauded as an essential skill for most jobs, multi-tasking constantly all day every day, at work and at home, is only effective if it’s productive. If you feel that you are meeting yourself coming back, that you are becoming chronically sleep deprived, have stopped exercising, have to scramble around the ironing pile looking for clean clothes or are opting for conveni-ence food most days of the week – it’s time to stop and think.
Adequate sleep, eating well, exercising and enjoying life with family are ABSOluTElY ESSENTIAl to life. These are the things that provide the physical, mental and emotional nourishment we need to work and be productive, but they are often the things we tend to cut back on when work and other responsi-bilities take over. when we do this for too long, work becomes harder or less productive and, worse still, our health and wellbe-ing deteriorates – so cutting back on sleep and leisure time achieves absolutely nothing.
Practice Nurses take every opportunity to promote healthy living to their patients, but tend to neglect themselves. As nurs-es are trained to seek out evidence, below are some research findings that might help remind you to take your own advice!
A recent study of neonatologists stated that the researchers’ findings “are similar to physicians’ feelings that their work pre-vents their having leisure time and emphasizes the importance
Sleep deprivation can impair job performance and increase risk for worker errors and injuries. errors made by fatigued healthcare workers also can endanger patients.

Access your digital copy today!
www.mindo.ie
Did you know as a nurse you can also access our award winning medical newspaper
online at

30
meeting report
The four types of asthma patientInternational experts have said that there needs to be a cohesive primary care team approach to the management of asthma patients.
Speaking at the launch of the results from the pan-European REAlISE (Recognising Asthma and link to Symptoms and Experience) survey recently, Prof David Price, Professor of General Practice at the university of Aberdeen, said “the whole team is fundamentally
important”.“Andrew wilson in the uK recently did a survey of at-risk
registers and that was very interesting because it showed that if you could identify the high-risk patients and make the whole primary care team aware of it, they were actually able to show a reduction in hospitalisation.”
Prof Price made the comments in relation to the survey results which revealed that 45 per cent of asthma patients in Europe remain uncontrolled.
controlThe GINA guidelines define asthma as being uncontrolled if at least three of the following features are present:• Daytime symptoms more than twice per week• limitation of activities• Nocturnal symptoms• Need for reliever medication at least twice per week• lung function <80% predicted
Partial control is defined as the presence of any of the above features.
Prof Price said the data demonstrates that we have not achieved all we should be achieving in relation to asthma control and that many patients remain at significant risk of acute exacerbations.
The survey found that among the uncontrolled group, 40 per cent had been treated in a hospital emergency department (ED) in the previous year due to their asthma. Almost two-thirds had been prescribed at least one course of oral steroids in the same period.
Among patients whose disease was partially controlled, 13 per cent had attended an ED with an asthma attack in the previous year and 31 per cent had been prescribed at least one course of oral steroids. Almost two-thirds experienced symptoms on one or two days in the previous week.
Even in the controlled group – which represented just one in five patients – 7 per cent had attended an ED in the previous year and 24 per cent had been prescribed a course of oral steroids. More than a third had experienced symptoms on one or two days in the previous week.
Furthermore, a third of all participants felt their asthma stopped them living life to the full and a fifth said the disease affected their sex life. Approximately 43 per cent said they tended to ignore symptoms so that they could feel normal and fit in with friends and peers. More than half worried about the impact their condition would have on their future health.
“So even patients who consider themselves well still experience restrictions on their day to day lives, relationships, emotional wellbeing and the way they manage their condition,” Prof Price pointed out. “In spite of us having great guidelines, great treatments, a third of them say asthma stops them living life to the full.”
Prof Price recommended exploring symptoms and control with patients to determine the root cause and improve disease management.
“There are two elements to flare-ups. we know that patients who are uncontrolled are at high risk of flare-ups. That may be because people are not taking their treatment or it may be that they have difficult to treat asthma. we do see in all our databases that there actually are patients who are adhering well – the striving patients. They are even over-striving in some cases. we actually have some work that shows that these patients who are over 100 per cent adherent are often still likely to be the ones who are in trouble. So there is a group of people struggling to gain control,” he said.
“There is another group who may not be taking their asthma seriously enough and actually are potentially at risk because they think they are under control but actually they are not.”
“Then there’s a final group that is much more difficult which is those who may be symptom free but triggers still upset them. For some people viral infections in particular, maybe allergen exposure for others, can trigger people off.”
“There has always been an assumption in medicine that the person who is telling you that they are uncontrolled, that they are struggling, that they are just not taking their medication... but actually it may be that we need to recognise that not everything is working for them,” Prof Price said. “Maybe we are giving them the wrong inhaler type. Maybe we haven’t addressed their co-morbidites. Maybe we haven’t actually recognised that they have more severe disease or maybe we have gotten the diagnosis wrong. That is important to consider.”
“It’s about recognising our patients who are striving and struggling and to actually work with them in that rather than just thinking they are non-compliant and thinking they are difficult patients, and to remember that everyone is at risk. Even patients who are symptom free are still at risk for acute attacks and we should never forget that,” he said.
behaviourFor the first time, the study also showed that asthma sufferers fall into four clearly defined behavioural groups with characteristic attitudes to their disease and these attitudes can have a significant impact on the success of treatment.
The Mundipharma-sponsored survey of 8,000 asthma patients throughout western Europe aimed to evaluate the level of symptom and the role of patient attitudes and behaviours in disease management. Participants in the online survey were required to have received at least two prescriptions for asthma in the previous two years.
A cluster analysis of the REAlISE data identified four clear patient groups and revealed that a patient’s attitude to their disease has a significant impact on symptom control.
Presenting the results at a recent seminar, Prof Thys van de Model, Professor of General Practice at the university Medical Centre in Groningen in the Netherlands, said that stratifying patients according to behaviours may assist healthcare

31
meeting report
professionals (HCPs) in improving the disappointing levels of symptom control in asthma at present.
The four patient groups identified by the study comprised the over-confident type, the concordant patient, the adrift patient and the striving patient.
The over-confident group were most likely to feel very confident about managing their condition and were least likely to be concerned about their asthma, Prof van de Molen reported. However, he said, asthma symptoms were controlled in just 20 per cent of these patients. In terms of demographics, 71 per cent of patients in this group were female and 61 per cent were less than 35 years of age. The vast majority of the group were not comfortable being labelled as ‘sick’.
The concordant patient, he said, tended to be relatively compliant and confident in managing their asthma, seeking assistance where necessary. An overwhelming 91 per cent followed their doctor’s advice and 52 per cent reported taking their preventer inhaler every day. However 28 per cent of these patients remained uncontrolled.
The adrift group made up 25 per cent of the 8,000 patients who took part in the survey. This was the only group where the proportion of male patients was larger than the proportion of female patients. Approximately 59 per cent of adrift patients were male and 61 per cent were under the age of 35 years. More than two-thirds remained uncontrolled and 64 per cent were concerned about the impact their asthma would have on their future health.
These patients said their asthma does cause them problems and they would like to control it better but they did not follow their doctor’s advice and were non-compliant with treatment, and sought out advice elsewhere, such as the internet, Prof van de Molen explained.
The final group identified was the striving patient. “These patients want to manage their asthma but don’t feel confident doing so. They consider their asthma to be serious and so follow their doctor’s advice and take their medication every day but worry about the impact on their future health. They want to control their asthma and try to follow the doctor’s advice but in some ways that advice does not help as 70 per cent are uncontrolled. It could be that this group have difficult to manage asthma,” the professor said.
More than 70 per cent of these patients were female and 55 per cent were over 35 years of age. Approximately 59 per cent said their asthma stopped them living life to the full and 62 per cent were anxious about not knowing when the next attack would occur.
“These are the patients that should maybe be seen more often in the practice and should be followed up with questionnaires or maybe seen every three months,” he advised.
“understanding patient attitudes and helping HCPs in Europe to understand [how patient attitudes affect treatment success] might help improve asthma management,” according to Prof van de Molen. “A better understanding of patients’ needs and beliefs, and better communication between patients and HCPs, could help reduce exacerbations and improve disease control for people with asthma.”
“HCPs need to work together with their patients to develop joint management plans and maybe the idea that there are different types of patients might influence these plans and might influence the goals that we want to set with our patients,” he added.
conclusionCommenting on the data, Ms Monica Fletcher, primary care nurse, Chair of the European lung Foundation and Chief Executive of Education for Health in the uK said: “Although current treatments are efficacious and have been shown to improve asthma control in clinical trials, real world asthma control remains sub-optimal.”
“Personally I find it shocking, as a HCP, that we are still in this position after all these years, with good treatments and guidelines,” she said.
She pointed out that in western Europe at least one person dies of asthma every hour. The condition is estimated to affect 30 million people in western Europe alone and is associated with annual total costs in the region of €17.7 billion.
“what we are reinforcing from this survey is that asthma is still a big problem. we’ve got 30 million people living with asthma. It’s costing a lot of money and still, I think, we haven’t made the in-roads, despite not just a range of treatments, but also a plethora of different devices now available. we know what to do and we’ve got good guidelines. we know far more about the underlying disease than we’ve ever known before and yet we still have this disconnect,” Ms Fletcher said.
“I’m hoping that by exploring the issues that [the survey has raised] we might find some solutions or at least tools for the many, particularly primary care HCPs out there, managing asthma on a day to day basis.”
“It’s about recognising our patients who are striving and struggling and to actually work with them rather than just thinking they are non-compliant and thinking they are difficult patients.”

32
product news
Focus on: RHEuMAToLoGY
A randomized, double-blind, phase III trial in moderate osteoarthritis knee pain comparing topical ketoprofen gel with ketoprofen-free gel
matthias Rother and Philip G.
conaghan
This randomized, double-blind, phase III study evaluated the efficacy and safety of ketoprofen in an ultradeformable vesicle gel compared with ketoprofen-free gel in osteoarthritis (OA) knee pain.
Patients with American College of Rheumatology-defined OA of the knee and moderate pain were randomized to receive 100 mg ketoprofen in 4.4 g transfersome gel (IDEA-033) or 4.4 g ketoprofen-free vehicle (TDT 064) topically, twice daily, for 12 weeks. The primary endpoint was mean change in western Ontario and McMaster universities Osteoarthritis Index (wOMAC) pain subscale score from baseline to week 12.
Patients (n = 555) were randomized and treated. Mean baseline wOMAC pain scores were 5.2 (SD 1.0) for IDEA-033 and 5.3 (SD 1.0) for TDT 064. Mean change in wOMAC pain scores from baseline to week 12 was 38.6% for IDEA-033 and 44.6% for TDT 064 (Mann-whitney estimator 0.4505; p = 0.022). Both groups reported progressive decreases in pain and improvements in function and stiffness. Mean baseline wOMAC function scores decreased from 5.4 to 3.4 with IDEA-033 and 3.1 with TDT 064 at week 12. The proportion of patients achieving ≥ 50% decrease in wOMAC pain score from baseline at week 12 was 41.2% (95% CI 0.35–0.47) with IDEA-033 and 50.5% (95% CI 0.45–0.57) with TDT 064. Mild skin and subcutaneous tissue disorders were the most frequently reported treatment-related adverse events (AE).
The authors concluded that IDEA-033 was inferior to drug-free gel (TDT 064) in relieving moderate OA knee pain and improving joint function.
A multicentre, randomized, placebo – and active-controlled trial comparing the efficacy and safety of topical ketoprofen in Transfersome gel (IDEA-033) with ketoprofen-free vehicle (TDT 064) and oral celecoxib for knee pain associated with osteoarthritis
Philip G. conaghan, John
dickson, wolfgang bolten, Gregor
cevc, and matthias Rothery
The purpose of this trial was to assess the efficacy and safety of 12-week treatment with ketoprofen in ultradeformable phospholipid vesicles in patients with OA knee pain and to compare the efficacy with that of ketoprofen – free vehicle and celecoxib.
A multicentre, double-blind controlled study in which patients with knee OA and moderate pain were randomized to one of the six arms: topical ketoprofen 50 or 100mg in ultradeformable vesicles (IDEA-033), 2.2 or 4.4 g ketoprofen-free vehicle (TDT 064), oral celecoxib 100 mg or matching oral placebo, all bd. The primary outcome was change from baseline in the wOMAC pain subscale at week 12.
A total of 1395 patients received treatment. Baseline mean wOMAC pain scores ranged from 4.7 to 4.8 across groups. The mean reduction in wOMAC pain score at week 12 was – 1.9 (β40.8%) forketoprofen 50mg, – 1.9 (-40.9%) for ketoprofen 100mg, – 1.9 (-39.8%) for 2.2g TDT064, – 1.8 (-37.8%) for 4.4g TDT 064, – 1.9 (-40.4%) for celecoxib and – 1.4 (-29.3%) for oral placebo. IDEA-033 was not statistically superior to TDT064. All topical treatments were statistically superior to oral placebo and non-inferior to celecoxib. The most frequent types of treatment-related adverse events reported were gastrointestinal for oral (15.9% for celecoxib) and dermal for topical applications (12.2% for ketoprofen 100 mg).
Conclusion. IDEA-033 was not superior to ketoprofen-free vehicle, but both formulations were superior to oral placebo and non-inferior to celecoxib in reducing OA knee pain.

Old Issues –New Ideas The 18th Annual National conference
11th-12th October, Radisson Blu, Athlone
conference Timetablefriday 11th October12.00 –14.00 Registration, Tea/Coffee, Exhibitions14.00 –14.15 Opening address14.15 –15.00 dr.catherine conlon, HSE Crisis
Pregnancy Programme-Astudy of migrant women’s sexual and reproductive health
15.00–15.45 Philip James, CNS, Adolescence Substance Abuse, Y.O.D.A. Tallaght.
15.45 –16.15 deirdre carmody, Drug liaison midwife CoombeHospital
16.15 –16.30 Questions and Answers16:30 –18:00 Exhibition19.00 –20.30 Gala Dinner20.30–21:30 Key Note: mary Scott’s Good Sexual
history21:30 Awards –including Practice Nurse of the
Year Award22:00 Entertainment
Saturday 12th October08:30–09:30 Exhibition09.30–09:45 Opening address09.45 –10.30 Prof. donal O’Shea, Obesity and the
Immune System, St Vincent’s Hospital.10.30 –11.15 dr Jay Sharma, Hypertension,
Midlands Hospital Portlaoise.11.15 –11.30 Questions and Answers11.30 –12.30 Coffee and Exhibition12.30 –13.15 dr Patrick Ormond, Dermatology,St
James Hospital13:15–13:30 Questions and Answers13:30 Presentation of Valerie Mangan Award13.45–14:30 lunch14:30 AGM
The Annual Irish Practice Nurse Association conference is the only National conference dedicated to nurses working in General Practice in Ireland. Attendance is open to all 700 members of the association as well as associate members.
The 2013 conference hosted by the members of North Dublin branch will be held at the centrally-located RadissonBluHotel in Athlone(www.radissonblu.ie/hotel-athlone)
Network with the Primary care frontline
with the continued expansion of primary care in Ireland, practice nurses are having a greater input into practice purchasing decisions than ever before. Join us for the 18th annual conference and exhibition. Attendance is a great way to gain accredited education whilst networking with fellow nurses.
Practice Nurses–Ready to learn
The IPNA conference continues to move with the times. The agenda is topical and the educational opportunities it provides are invaluable. we know you are keentocontinually improve the quality of care you offer your patients,so we have designed an event that gives you real information that will remain useful long after the event is over.
engaging conference – The conference programme has been designed to provide innovative insight and an overview of the latest developments within an enjoyable and mutually educational environment.
exhibition – Our exhibition provides an informal environment to talk to companies to learn about the latest products, services and equipment that are relevant to you.

34
product news
TIOSPIR trial reinforces Respimat efficacy profile in COPD
The TIOSPIR (Tiotropium Safety and Performance in Respimat) trial with over 17,000 COPD patients, one of the largest international COPD trials ever conducted, has confirmed the comparable safety and efficacy profile of the two available Spiriva formulations – Spiriva Respimat 5µg and Spiriva HandiHaler 18µg.
The highly anticipated results from the three-year trial were published in the New England Journal of Medicine on 8 September. TIOSPIR was designed to provide evidence of the relative safety and efficacy profile of Spiriva Respimat 5µg or an investigational dose of Respimat 2.5µg compared with Spiriva HandiHaler 18µg. TIOSPIR was specifically designed to be of an adequate size and duration to enable analysis of all-cause mortality and time to first COPD exacerbation in a large COPD patient population, with broad inclusion criteria, that closely reflects the real-world COPD patient population.
Commenting on the results, trial investigator Prof Antonio Anzueto, Professor of Pulmonary/Critical Care Medicine, university of Texas Health Science Center at San Antonio, Texas said: “TIOSPIR is a landmark clinical trial providing a robust data set that reinforces the safety and efficacy of tiotropium delivered by either HandiHaler or Respimat. Importantly,
this large and rigorous clinical trial provides evidence that tiotropium is safe in a broad population of COPD patients, including those with a history of cardiac disease. The critical message from this large-scale trial is that physicians can be confident that they can prescribe this proven maintenance therapy across the severity spectrum of COPD patients.”
The trial demonstrated comparable results for time to first COPD exacerbation for both formulations of Spiriva. In particu-lar, the median time to COPD exacerbation was more than two years for both formulations. For Spiriva Respimat 5µg this was 756 days compared to 719 days for Spiriva HandiHaler 18µg.
COPD exacerbations have a significant impact on patients’ lives and reducing their frequency and severity are principal goals of COPD treatment. The TIOSPIR results demonstrate that Respimat and HandiHaler showed comparable results for time to first COPD exacerbation, exacerbation frequency as well as rate of COPD exacerbations associated with hospitalisation. TIOSPIR builds upon the established efficacy profile of Spiriva HandiHaler 18µg as demonstrated in several trials, including the four-year uPlIFT trial, as well as a large-scale trial, POET-COPD, that was specifically powered to investigate COPD exacerbations.
New treatment for ADHD in children and adolescents – Tyvense
Shire Pharmaceuticals Ireland ltd recently announced that its single-daily dose long-acting prodrug stimulant, Tyvense, has been authorised by Irish Medicines Board, for the treatment of ADHD in children aged 6 years and over when response to previous methylphenidate treatment is considered clinically inadequate.
Tyvense is the first stimulant prodrug to be launched in Europe for the treatment of ADHD. It provides a long duration of effect to help patients achieve control of their ADHD symp-toms. The prodrug is ingested in an inactive form and subse-quently activated within the body, meaning that the active part of Tyvense is gradually released over time.
ADHD is a complex condition and every patient has specific needs. while there is no cure for ADHD, treatment gener-ally includes educational approaches, behavioural or other psychotherapies, and medication (depending on patient age and ADHD severity), or a combination of all of these. European guidelines recommend the use of ADHD medications that reduce the need for children to take medication through the course of the school day.
The most commonly prescribed medications for ADHD are stimulants. In Europe, the most frequently prescribed stimulant is methylphenidate. However, not all patients show a clinically adequate response to this treatment.
Speaking at the launch of this important new treatment, Dr Eithne Foley (Child & Adolescent Psychiatrist with the HSE) said: “Every child with ADHD is different and will vary in his
or her response to the available treatments, which include behavioural and psychological interventions, educational strategies and pharmacological treatments.
This new stimulant treatment is a very welcome development and means that we have an additional pharmacological treatment option for those patients who have not responded to a first line medication. This new medication will give an additional pharmacological treatment option as part of a comprehensive treatment package for ADHD.”
Attention Deficit Hyperactivity Disorder (ADHD) is one of the most common psychiatric disorders in children and adoles-cents, and is recognized by the world Health Organisation (wHO). Globally, ADHD affects around 5%of children and ado-lescents. Based on this prevalence rate, one can estimate that 5 million young people in the Eu experience ADHD.
Commenting on the launch of Tyvense, Brian Martin, General Manager, Shire Pharmaceuticals Ireland ltd said, “we are delighted that Tyvense is now licensed for use in children and adolescents with ADHD in Ireland. Shire is committed to improving the understanding and treatment of ADHD and to ensuring that patients diagnosed with ADHD continue to benefit from these advances.”
Treatments such as Tyvense are believed to work by enhancing the availability of two neurotransmitters (chemical messengers in the brain) noradrenaline and dopamine, helping to correct a presumed chemical imbalance and reduce symptoms such as inattention, impulsivity and hyperactivity.

35
product news
Positive reimbursement recommendation for Eliquis (apixaban) for the prevention of stroke and systemic embolism in adults with non-valvular atrial fibrillation
BMS and Pfizer Healthcare Ireland have welcomed the results of the Health Technology Assessment (HTA) conducted by the National Centre for Pharmacoeconomics (NCPE) which has found that Eliquis (apixaban) to be cost effective in the prevention of stroke and systemic embolism in people with non-valvular atrial fibrillation (NVAF). In finding apixaban cost-effective, the NCPE has recommended that it is reimbursed.1
Commenting on the decision Mr Graham Morris, Business unit Director, CV /Metabolics BMS uK & Ireland said “we welcome the findings of the NCPE report as it is important that Irish patients continue to get access to advanced and innovative medicines.”
No head-to-head data is available for apixaban compared with the other novel oral anticoagulants (NOACs). The efficacy of apixaban, in the VKA-suitable populations, was compared to dabigatran etexilate and rivaroxaban indirectly using a network meta-analysis. The report states that apixaban showed a statistically significant reduction in myocardial infarction compared to dabigatran 150mg and 110mg and had a statistically significant lower incident of all bleeding outcomes compared to rivaroxaban. In addition, apixaban had a statistically significant lower incidence of major bleeding, other major bleeding, gastro-intestinal bleeding, and ‘any bleeding’ compared with Dabigatran 150 mg. There were no statistically significant differences between the three drugs for the primary efficacy outcome (stroke and systemic embolism) and for the other efficacy outcomes.
One of the most serious medical concerns for individuals
with atrial fibrillation is the increased risk of stroke, which is five times higher in people with atrial fibrillation than those without this arrhythmia. It is estimated that AF is responsible for up to a quarter of all strokes, often resulting in greater mortality, longer hospital stay and increased disability.
Mr Richard Stakelum, PCBu lead Pfizer Healthcare Ireland said: “we welcome this positive HTA which shows apixaban to be cost effective. It is a very significant outcome especially given the costs associated with warfarin monitoring were not included in the assessment.”
In April 2013 Bristol-Myers Squibb Pharmaceuticals and Pfizer Healthcare Ireland submitted an economic evaluation on the cost effectiveness of apixaban (Eliquis®) for the prevention of stroke and systemic embolism in people with non-valvular atrial fibrillation (NVAF). The evaluation is presented from the perspective of the Health Services Executive. The base case analysis pertains to the General Medical Services (GMS) population. Cost effectiveness on the Drug Payment Scheme (DPS) was investigated in a scenario basis.
The cost effectiveness of apixaban was assessed using a comprehensive Markov model. The model predicts that the incremental cost effectiveness ratios (ICERs) of apixaban vs. warfarin (the standard of care in VKA suitable patients) will be €11,087/QAlY and €16,533/QAlY in the GMS and the DPS populations respectively.i The model also predicts that the drug is cost effective compared to dabigatran and rivaroxaban in the VKA suitable population and to aspirin in the VKA unsuitable population.
Xtandi authorised in the EU for advanced prostate cancerThe European Commission (EC) has now granted the marketing authorisation for Xtandi (enzalutamide) capsules for the treatment of adult men with metastatic castration-resistant prostate cancer whose disease has progressed on or after docetaxel therapy.1 Xtandi had previously received a positive opinion by the European Medicines Agency (EMA) and a positive Committee for Medicinal Products for Human use (CHMP) opinion on 25th April 2013.
Enzalutamide is a novel, once-daily, oral androgen receptor signalling inhibitor.1 It inhibits multiple steps in the androgen receptor (AR) signalling pathway, which has been shown to decrease cancer cell growth and induce cancer cell death (apoptosis).3 The Eu authorisation is based on results from the phase III AFFIRM study. The phase III AFFIRM trial was a randomised, double-blind, placebo-controlled, multinational trial evaluating enzalutamide (160 mg/day) versus placebo in 1,199 men with progressive metastatic castration-resistant
prostate cancer who were previously treated with docetaxel-based chemotherapy.
AFFIRM confirmed that enzalutamide demonstrated a statisti-cally significant improvement (p<0.0001) in overall survival compared to placebo, with a median survival of 18.4 months in the enzalutamide group versus 13.6 months in the placebo group, an advantage of 4.8 months [hazard ratio (HR) = 0.631]. The study also concluded that enzalutamide was generally well tolerated by patients and met all secondary endpoints.2
Professor John Mc Caffrey, Mater Misericordiae university Hospital comments:
“Enzalutamide is an important development in prostate cancer therapeutics providing a critically important, orally available and well tolerated new option to the armamentarium of active drugs in advanced prostate cancer. Enzalutamide has a significant impact on quality of life and survival from this disease, this is good news for Irish patients and their families”
36
product news
Picato by LEO Pharma will help tackle pre-cancer sun damage
A new treatment for the potentially dangerous skin condition actinic keratosis (AK), which dramatically reduces topical treatment time for patients, is now available in Ireland.
Picato (ingenol mebutate) gel, manufactured by dermatology company lEO Pharma, is licensed for the cutaneous treatment of non-hyperkeratotic, non-hypertrophic AK in adults. AK is a type of skin damage caused by long-term sun or uV exposure that has the potential to progress to the non-melanoma skin cancer, squamous cell carcinoma (SCC).
Current topical, patient-applied therapies that have treatment durations from three up to 12 weeks – treatment periods which research shows can lead to patient adherence levels as low as 37 per cent. Picato effectively manages AK with a once-daily treatment, which is applied over two or three days and demonstrates high patient adherence in clinical trials of more than 98 per cent.
AK often appears as red, rough, sandpapery patches of skin on areas that are more exposed to sun such as the face, head, arms and legs. It can occur as a single lesion or multiple lesions, affecting an entire area (known as the ‘field’). where there are multiple lesions, it is important to treat the entire field.
An extensive phase III clinical trial programme has demon-strated that three days of treatment application with Picato 150mcg/g on the face or scalp led to an 83 per cent median
reduction in the number of AK lesions compared to baseline, when measured at day 577. Following two days of treatment application on the trunk or extremities with Picato 500mcg/g, there was a 75 per cent median reduction in the number of AK lesions compared to baseline, when measured at day 577.
Dr william O’Connor, Consultant Dermatologist, Bon Secours Hospital, Cork commenting on the launch of the new product, said: “The launch of Picato gel in Ireland is a positive step forward for patients with AK. As it is not always possible to predict which AK will advance to non-melanoma skin cancer, early detection and treatment is very important.”
“In addition, the short treatment duration of Picato gel is very attractive for patients who currently have to use topical treatments for up to three months. The comparable efficacy of Picato gel should also lead to higher compliance rates, similar to those seen in the clinical trials in which more than 98 per cent of patients completed their treatment course.”
Dr Johnny loughnane, a GP with a special interest in dermatology said: “In Ireland the majority of people have fair skin and, as a consequence, AK, a pre-malignant form of skin lesion, is particularly common. Most cases can be effectively diagnosed and treated in primary care. Picato offers the GP an effective treatment that can be completed in either two or three days.”
Drug-free osteoarthritis pain gel hailed by leading rheumatologistsA breakthrough new drug-free pain relief gel for Irish arthritis sufferers has been hailed by leading health professionals.
Key clinical data supporting Flexiseq has just been published in The Journal of Rheumatology in the uK.
The journal is the latest high profile publication to back the gel which selling 15,000 tubes a week.
The gel has already won the German Pharmacy Industry Award for Innovation this year.
The publication reports that Flexiseq (TDT 064) was very effective in managing the pain associated with osteoarthritis (OA) and was again found to have a much stronger safety profile than other treatments.
Dr Matthias Rother, lead author of the publication, said: “This is an important study which further confirms the safety and efficacy of Flexiseq for treatment of the chronic pain and stiffness that troubles so many patients with OA.
“The effect size seen here for Flexiseq is comparable to the effect sizes seen in a comparative study using the same design which demonstrated that Flexiseq has equivalent efficacy to the widely-used oral NSAID, celecoxib. That study was published in Rheumatology earlier this year. These two studies are among several which consistently demonstrate the benefits of this drug-free gel.’
The findings offer hope to 450,000 Irish OA patients,
particularly those who are at risk from the common gastrointestinal and cardiovascular side effects associated with NSAIDs, such as celecoxib and diclofenac.
Prof Philip Conaghan, co-author of the paper, said: “Osteoarthritis is a widespread and chronic disease that causes pain and loss of function which adversely affects patients’ lives. A great many patients suffer from OA and this number is growing. Many of these patients should not take or cannot tolerate current oral analgesics because of side effects. There is a desperate need for new effective and safe analgesics for OA and this study provides further insight into the efficacy of this treatment that has demonstrated excellent safety and tolerability.”
Prof Conaghan, who was a key speaker at the recent Irish Society of Rheumatology (ISR) autumn meeting: “The launch of Flexiseq in Ireland provides an opportunity for patients to have access to a new approach for managing their OA symptoms and we look forward to knowing more about this treatment”.
The study also grabbed the attention of Arthritis Research uK, which noted: “There are fewer and fewer safe, available, pain-relieving options for people with osteoarthritis. If this product can relieve their long-term pain without side effects, then that is good news for the millions of people who suffer with this debilitating condition.”

37
crossword
Name:
Address:
Email:
Congratulations to the winner of last month’s crossword, Peggy O’Halloran, c/o Dr Hackett, 71 Church Street, listowel, Co Kerry.
Please send your answers to the Editor, Nursing in General Practice, GreenCross Publishing, 7 leeson Street, Dublin 4. Closing date for entries: 31 October 2013.winner will receive v50. Please note: the winners’ cheques will be sent out within 45 days.
Caltrate is a trademark. PA 172/38/1. Full prescribing information available from Pfizer Consumer Healthcare ltd., 9 Riverwalk, National Digital Park, Citywest Business Campus, Dublin 24 or from www.medicines.ie
1 2 3 4 5
6 7
8
9 10
11 12 13
14
15 16
17
18 19 21
22 23
20
AcROSS6 All in on oily wool extract (7)7 Dance between Heaven and Hell? (5)9 One gets a sound return from it! (4)10 Crop slut posing for statue-maker (8)11 Military display of skin-art? (6)13 Meat, we hear, to encounter (4)15 Hee-Haw Town in wicklow? (4)16 Don’t accept this rubbish! (6)18 Connecting or popping the question? (8)21 A kind of ache for everyone (4)22 Stiff Egyptian mother? (5)23 They are down in the mouth due to slots in
disarray (7) dOwN1 Play it, strike it or marry! (5)2 Muddle or cry on a type of hearty artery (8)3 Don’t hit her! (4)4 Thpeak like thith with thith? (4)5 Bond me a different stomach! (7)8 Amputate or isolate (3,3)12 large root vegetable, Pi perhaps? (6)13 Her job is to rub people up the right way! (8)14 Mica urn surprisingly found under 17 Down (7)17 Claps stupidly on one’s head (5)19 Mary manouvered soldiers (4)20 Olga wiggled for the prison (4)
AcROSS: 6 Kildare, 7 Aorta, 9 lean, 10 Spectrum, 11 Bikini, 13 Cock, 15 Thus, 16 Tom cat, 18 Immunity, 21 Iron, 22 Psalm, 23 Antenna. dOwN: 1 Dimes, 2 Adenoids, 3 Iris, 4 Hoot, 5 Staunch, 8 Medium, 12 In trim, 13 Clarinet, 14 Chemist, 17 Mount, 19 ugly, 20 Yank

Herceptin SC
Less waiting time More free time
All the benefits of Herceptin, now in a faster format1-4
p07/09/13
ABRIDGED PRESCRIBING INFORMATION (Early & Metastatic Breast Cancer Indication Only) (For full prescribing information, refer to the Summary of Product Characteristics [SmPC] HERCEPTIN¨ (trastuzumab) 600mg/5ml solution for injection Indications: Metastatic Breast Cancer (mBC): Treatment of patients with HER2 positive mBC: (i) as monotherapy following at least 2 chemotherapy regimens for mBC. Prior chemotherapy to include at least an anthracycline and a taxane, unless unsuitable for treatments. Hormone receptor positive patients must also have failed hormonal therapy, unless unsuitable for treatments. (ii) in combination with paclitaxel for patients who have not received chemotherapy for mBC and where anthracyclines not suitable. (iii) in combination with docetaxel for patients who have not received chemotherapy for mBC. (iv) in combination with an aromatase inhibitor for the treatment of postmenopausal patients with hormone-receptor positive mBC, not previously treated with Herceptin. Early Breast Cancer (eBC): Treatment of patients with HER2 positive eBC (i) following surgery, chemotherapy (neoadjuvant or adjuvant) and radiotherapy (if applicable) (ii) following adjuvant chemotherapy with doxorubicin and cyclophosphamide, in combination with paclitaxel or docetaxel. (iii) in combination with adjuvant chemotherapy consisting of docetaxel and carboplatin. (iv) in combination with neoadjuvant chemotherapy followed by adjuvant Herceptin therapy for locally advanced (including inflammatory) disease or tumours >2cm diameter. Herceptin should only be used in mBC or eBC patients whose tumours have either HER2 overexpression or HER2 gene amplification as determined by an accurate and validated assay. Dosage and Administration: HER2 testing mandatory prior to Herceptin therapy. Only physicians experienced in cytotoxic chemotherapy should initiate Herceptin: The injection should be administered by a healthcare professional only. Herceptin subcutaneous (SC) formulation is not intended for intravenous (IV) administration and should be administered via a SC injection only. Check product labels to ensure correct formulation administered. Limited information available on switching from one formulation to another. Not recommended in patients <18 years of age. Dedicated PK studies in older people and those with renal or hepatic impairment have not been carried out. Refer to SmPC for dose reduction and missed doses. Treat mBC patients until disease progression. Treat eBC patients for 1 year or until disease progression; whichever occurs first. Recommended dose is 600mg/5ml irrespective of the patient’s body weight. No loading dose is required. This dose should be administered subcutaneously over 2-5 minutes every three weeks, refer to SmPC. Patients should be observed for six hours after the first injection and for two hours after subsequent injections for signs or symptoms of administration-related reactions. Refer to SmPC for chemotherapy combination dosing. Contraindications: Hypersensitivity to trastuzumab, murine proteins, hyaluronidase or any excipients. Severe dyspnoea at rest due to complications of advanced malignancy or requiring supplementary oxygen therapy. Warnings and Precautions: HER2 testing in a specialised laboratory mandatory to ensure adequate validation of test. No trial data available on re-treatment of patients with previous exposure to Herceptin in the adjuvant setting. Heart failure observed in patients receiving monotherapy or in combination with paclitaxel or docetaxel, particularly following anthracycline-containing regimens: may be moderate to severe, has been fatal. All candidates for treatment (especially those with prior anthracycline and cyclophosamide exposure) should undergo baseline cardiac assessment including history and physical examination, ECG, echocardiogram, and/or MUGA scan or magnetic resonance imaging. A careful risk-benefit assessment should be made. In all patients cardiac assessments should be repeated every 3 months during treatment and every 6 months following discontinuation until 24 months from the last dose. Anthracycline therapy should be avoided for up to 27 weeks after last dose of Herceptin. Formal cardiological assessment should be considered in patients with cardiovascular concerns following baseline screening. For patients who develop cardiac dysfunction monitoring should take place every 6-8 weeks. Consider discontinuing treatment in patients with asymptomatic decreased LVEF function if no clinical benefit seen. Caution in treating patients with symptomatic heart failure, history of hypertension, Coronary artery disease, and in eBC patients with LVEF of 55% or less. If LVEF drops 10 ejection fraction points from baseline and to below 50% treatment should be suspended, repeat LVEF assessment within 3 weeks. If LVEF does not improve or further declines, consider discontinuation, refer to SmPC. All such patients should be reviewed by cardiologist and followed up. If symptomatic cardiac failure develops during therapy, treat with standard medications.. Most patients in the pivotal trials who experienced heart failure improved with standard medication, refer to SmPC. mBC: Herceptin and Anthracyclines should not be given concurrently in the metastatic breast cancer setting. Increased risk of cardiotoxicity in patients who previously received anthracycline therapy. eBC: For eBC patients, cardiac assessment, as performed at baseline, should be repeated every 3 months
during treatment and every 6 months following discontinuation of treatment for duration of 24 months from the last dose. Further monitoring is recommended for patients receiving anthracycline containing chemotherapy and should occur yearly up to 5 years from the last dose or longer if a continuous decrease of LVEF is observed. In eBC, no data on patients with existing or a history of documented CHF (New York Heart Association Class greater than or equal II), history of MI, LVEF of <55%, other cardiomyopathy, hemodynamic effective pericardial effusion, cardiac arrhythmia requiring medical treatment, angina pectoris requiring medical treatment, clinically significant cardiac valvular disease, poorly controlled hypertension. Therefore treatment not recommended. Herceptin and anthracyclines should not be given concurrently in the adjuvant treatment setting. In eBC adjuvant patients, the incidence of symptomatic and asymptomatic cardiac events increased when Herceptin (IV formulation) was administered after anthracycline-containing chemotherapy compared to administration with a non-anthracycline regimen of docetaxel and carboplatin and was more marked when Herceptin was administered concurrently with taxanes than when administered sequentially to taxanes. Most symptomatic cardiac events occurred within the first 18 months, regardless of the regimen used, refer to SmPC for further details.. In patients eligible for neoadjuvant-adjuvant treatment, low dose anthracycline regimens (maximum cumulative doses: doxorubicin 180 mg/m2 or epirubicin 360 mg/m2) can be administered concurrently with chemotherapy na•ve Herceptin patients. If patients have been treated concurrently with low dose anthracyclines and Herceptin in the neoadjuvant setting, no additional cytotoxic chemotherapy should be given after surgery. Experience of concurrent administration of anthracycline regimens is low, refer to SmPC for details. Neoadjuvant-adjuvant treatment is not recommended for patients older than 65 years of age refer to SmPC. Administration-related reactions (ARRs) are known to occur with Herceptin SC formulation. Pre-medication may reduce risk, refer to SmPC. Serious ARRs were not reported in the clinical trial however ARRs have been associated with the IV formulation. ARRs can be treated with an analgesic/antipyretic, or antihistamine. In rare cases, ARRs have resulted in fatal outcome. Patients experiencing dyspnoea at rest due to complications of advanced malignancy and co-morbidities may be at increased risk of fatal ARR and pulmonary events, therefore these patients should not be treated with Herceptin. Refer to SmPC for delayed (including fatal) ARR and pulmonary events. Severe pulmonary events have been reported with use of the IV formulation, occasionally fatal. Cases of interstitial lung disease reported: risk factors include prior or concomitant therapy with other anti-neoplastic therapies known to be associated with it such as taxanes, gemcitabine, vinorelbine and radiation therapy. Exercise caution for pneumonitis, especially in patients treated concomitantly with taxanes. Drug Interactions: No formal drug interaction studies have been performed. Effect of Herceptin on the pharmacokinetics of other antineoplastic agents: Pharmacokinetic data (PK) from studies BO15935 and M77004 in women with HER2 positive MBC suggest that exposure to paclitaxel and doxorubicin is not altered by Herceptin IV loading or maintenance dose, refer to SmPC. However Herceptin may elevate the overall exposure of one doxorubicin metabolite (7-deoxy-13 dihydro-doxorubicinone, D7D). The bioactivity of D7D and the clinical impact of the elevation of this metabolite is unclear. Study JP16003 in HER2 positive Japanese MBC patients suggest administration of Herceptin has no effect on the single dose PK of docetaxel. Study JP19959, a substudy of BO18255 performed in male and female Japanese patients with advanced gastric cancer studied the PK of capecitabine and cisplatin administered with or without Herceptin. Exposure to the bioactive metabolite 5 –FU of capecitabine was not affected by the concurrent use of cisplatin plus Herceptin. However, higher concentrations and a longer half-life of capecitabine were demonstrated when combined with Herceptin. The PK of cisplatin was not affected by concurrent use of capecitabine or by concurrent use of capecitabine plus Herceptin, refer to SmPC. Effect of antineoplastic agents on Herceptin pharmacokinetics: Study JPI6003 in Japanese HER2 positive MBC patients found no evidence of a PK effect on Herceptin with concurrent administration of docetaxel. Comparison of PK results from phase II & III clinical trials in HER2 positive MBC patients indicate that individual and mean Herceptin trough serum concentrations varied within and across studies however no clear effect of the concomitant administration of paclitaxel on the pharmacokinetics of Herceptin, refer to SmPC for further details. The administration of anastrozole did not appear to influence the pharmacokinetics of trastuzumab. Fertility, Pregnancy and Lactation: Avoid during pregnancy unless potential benefit for mother outweighs risk to foetus. Do not breast-feed during and for 7 months after last treatment. Cases of foetal renal growth and and/or function impairment in association with oligohydramnios (some associated with fatal pulmonary hypoplasia of the foetus) reported in pregnant women in the post-marketing setting. Use effective contraception during and for at least 7 months
after treatment has concluded. Advise women who become pregnant of potential foetal harm and manage with a multidisciplinary team. Side Effects and Adverse Reactions: Most serious and/or common adverse reactions (reported for IV and SC formulations) are cardiac dysfunction, ARRs, haematotoxicity (especially neutropenia), infections and pulmonary events. The safety profile of Herceptin SC formulation from the pivotal trial in eBC was overall similar to the known safety profile of the IV formulation. Adverse events reported more frequently for the SC formulation: serious adverse events which included post-operative wounds infections, ARRs, hypertension. The following adverse reactions have been reported with Herceptin IV monotherapy or in combination with chemotherapy in trials and in the post marketing setting: Very Common (≥1/10): febrile neutropenia, anaemia, neutropenia, leukopenia, hypertension, hypotension, dyspepsia, constipation, alopecia, mucosal inflammation, infusion related reactions, tremor, dizziness, headache, increased/decreased BP, irregular heart beat, palpitation, cardiac flutter, decreased ejection fraction, wheezing, dyspnoea (14%), diarrhoea, vomiting, nausea, lip swelling, hot flush, conjunctivitis, increased lacrimation, abdominal pain, erythema, rash, facial swelling, arthralgia, muscle tightness, myalgia, asthenia, chest pain, chills, fatigue, cough, epistaxis, rhinorrhoea, influenza-like symptoms, IRR, pain and pyrexia. Common (≥1/100 - <1/10): pneumonia (<1%), neutropenic sepsis, cystitis, herpes zoster, infection, influenza, nasopharyngitis, sinusitis, skin infection, rhinitis, upper respiratory tract infection, urinary tract infection, erysipelas, cellulitis, thrombocytopenia, , hypersensitivity, weight decreased/weight loss, anorexia, anxiety, depression, insomnia, abnormal thinking, peripheral neuropathy, paraesthesia, hypertonia, somnolence, dysgeusia, ataxia, dry eye, congestive cardiac failure (2%), supraventricular tachyarrhythmia, cardiomyopathy, hypotension, vasodilation, asthma, lung disorder, pharyngitis, pancreatitis, dyspepsia, haemorrhoids, constipation, dry mouth, hepatitis, liver tenderness, hepatocellular injury, acne, , dry skin, ecchymosis, hyperhydrosis, maculopapular rash, nail disorder, pruritus, dermatitis, arthritis, back pain, bone pain, muscle spasms, neck pain, renal disorder, breast inflammation/mastitis, peripheral oedema, malaise, , oedema and contusion. Serious or potentially serious: Severe infections, heart failure (New York Association [NYHA] class II-IV, hypertension, immunogenicity, pneumonitis, acute pulmonary oedema, renal failure and febrile neutropenia. Refer to SmPC for full listings of adverse events. Legal Category: Limited to sale and supply on prescription only. Presentation and Marketing Authorisation Number: EU/1/00/145/002 Pack of one 6mL vial containing 5mL of solution Marketing Authorisation Holder: Roche Registration Limited, 6 Falcon Way, Shire Park, Welwyn Garden City, AL7 1TW, United Kingdom. Herceptin is a registered trade mark. Full prescribing information is available from Roche Products (Ireland) Limited, 3004 Lake Drive, Citywest, Naas Road, Dublin 24. Telephone: (01) 4690700. Fax: (01) 4690791. Date of Preparation: 09th September 2013.
References: 1. Ismael G, et al. Lancet Oncol. 2012; 13(9):869–878. 2. Jackisch C, et al. Oral presentation at the 8th European Breast Cancer Conference, Vienna,Austria 2012 (Abstract 1BA). 3. Pivot X, et al. Poster presentation at the 37th ESMO, Vienna, Austria 2012 (Poster 272P). 4. Herceptin (trastuzumab) combined IV and SC (vial) SmPC, August 2013. 5. Jackisch C, et al. Poster presentation at the 37th ESMO, Vienna, Austria 2012 (Poster 271P). 6. Pivot X, et al. Poster presentation at the 13th St Gallen Breast Cancer Conference, St Gallen, Switzerland 2013 (Poster 207).
Administer the standard of care in just 2 - 5 minutes compared to between 30 minutes to two hours with Herceptin IV1-4 Proven comparable efficacy and safety to I.V. Herceptin1, 2, 5 Simple, ready to use formulation, frees up clinic resources6
5549 Herceptin SC_press ad 395X273_AW.indd 1 18/09/2013 12:37