the islets of langerhans in rats with hypothalamic obesity
TRANSCRIPT
981
bring about a myogenic constriction of the arterioles,such as was observed by Folkow.2 This response wouldcause the blood-pressure to rise still further. As the
blood-pressure rises, the stimulus to a renal pressurereceptor distal to the clip will progressively declineand cardiac output will revert towards the normallevel. The situation known to exist in established hyper-tension would result, in which output appears to be
normal and peripheral resistance is raised.This hypothesis of renal hypertension has certain
implications:1. Chronic hypertension is a new equilibrium state in which
the hasmodynamic and other alterations of the developingphase are no longer present. When considering the patho-genesis of renal hypertension, it is important therefore to payattention to events in the developmental rather than theestablished phase.
2. Arterial vasoconstriction is maintained by a physiologicalprocess of myogenic autoregulation of tissue blood-flow, andnot by a circulating vasoconstrictor substance.
3. Substances thought to be concerned in the pathogenesisof hypertension should be examined for their possible effectson cardiac contractility, capacity vessel-tone, and extracellularfluid-volume-all of which are capable of influencing cardiacoutput.
SUMMARY
Rats in which experimental renal hypertension is
developing show a transient rise in cardiac output.There is usually marked bradycardia in the first few
days of developing hypertension.The relevance of these findings to a theory of the
pathogenesis of hypertension are discussed.We hould like to thank Prof. Clifford Wilson for his encourage-
ment and advice, and to acknowledge the invaluable assistance of Mr.Clifford Browning, senior electronics technician to the medical unit.
J. M. LEDINGHAMM.D. Lond., F.R.C.P.R. D. COHEN
M.B. Cantab., M.R.C.P.
Medical Unit,The London Hospital Medical College,
London, E.1
THE ISLETS OF LANGERHANS IN RATS
WITH HYPOTHALAMIC OBESITY
IN severe diabetes mellitus there is an absolute defi-
ciency of insulin 13 14 and atrophy of the islet-cells of thepancreas. 15 But in the early stages of the maturity-onsettype of diabetes in obese subjects, plasma-insulin may be raised in the fasting and thefed state, although the rise after glucosediminishes as glucose-tolerance deterior-ates. The primary defect in these cases
may be increased lipolysis causing insulinresistance. Ogilvie 16 showed that duringthe dynamic phase of developing obesityglucose-tolerance was good, but that itdeteriorated in the static phase; obese sub-jects generally had enlarged pancreaticislets." 7
Hypothalamic obesity in rats forms a
good experimental model to study the rela-tion of simple overnutrition to diabetes.In longstanding obesity of this type glucose-tolerance is impaired and spontaneous12. Folkow, B. B. Acta physiol. scand, 1952, 27, 99.13. Bornstein, J., Lawrence, R. D. Brit. med. J. 1951, ii,
1541.14. Hales, C. N., Randle, P. J. Lancet, 1963, i, 790.15. Best, C. H. in Experimental Diabetes (edited by J.
F. Delafresnaye and G. H. Smith). Oxford, 1954.16. Ogilvie, R. F. Quart. J. Med. 1935, 4, 345.17. Ogilvie, R. F. J. Path. Bact. 1933, 37, 473.
glycosuria sometimes develops,18 On the other hand,glucose-tolerance is raised in the dynamic phase, which lasts6-8 weeks, during which the animals are hyperphagic.19
Hales and Kennedy 20 found immediately after theintroduction of hypothalamic lesions in rats that plasma-glucose, non-esterified fatty acid, and insulin were un-altered. After 7 days of overeating the rats showedincreases in both non-esterified fatty acid and insulin; butafter 3 months, when obesity was fully developed and thefood intake was again normal, these changes were muchgreater and the raised insulin level persisted even afterfasting. It came as a surprise therefore to find the islet-cells of hypothalamic obese rats described as normal incontrast with various sorts of spontaneous " metabolic "obesity in which the islets were hyperplastic.21 22 A
preliminary re-examination of this finding has beenundertaken.
METHODS AND RESULTS
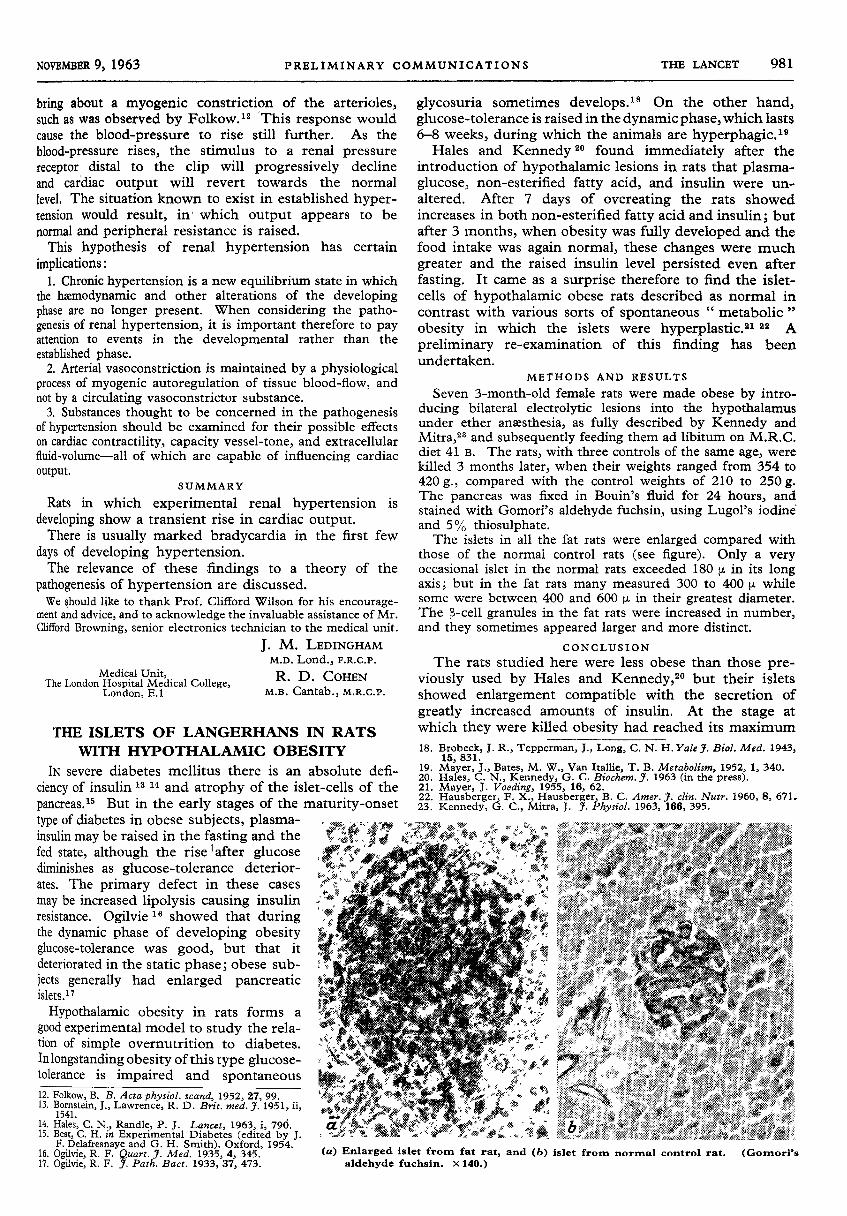
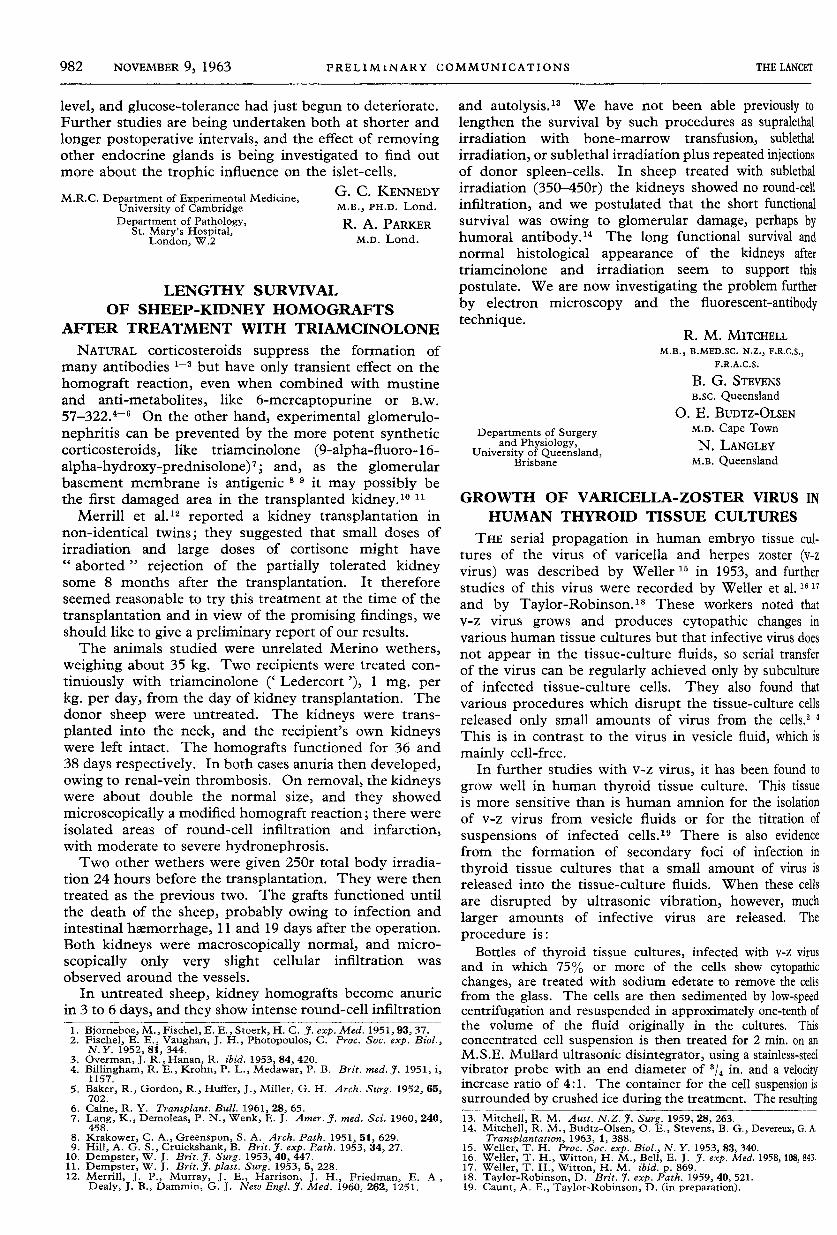
Seven 3-month-old female rats were made obese by intro-ducing bilateral electrolytic lesions into the hypothalamusunder ether anaesthesia, as fully described by Kennedy andMitral and subsequently feeding them ad libitum on M.R.C.diet 41 B. The rats, with three controls of the same age, werekilled 3 months later, when their weights ranged from 354 to420 g., compared with the control weights of 210 to 250 g.The pancreas was fixed in Bouin’s fluid for 24 hours, andstained with Gomori’s aldehyde fuchsin, using Lugol’s iodineand 5% thiosulphate.The islets in all the fat rats were enlarged compared with
those of the normal control rats (see figure). Only a veryoccasional islet in the normal rats exceeded 180 jj. in its longaxis; but in the fat rats many measured 300 to 400 (J. whilesome were between 400 and 600 !J. in their greatest diameter.The p-cell granules in the fat rats were increased in number,and they sometimes appeared larger and more distinct.
CONCLUSION
The rats studied here were less obese than those pre-viously used by Hales and Kennedy,2O but their isletsshowed enlargement compatible with the secretion of
greatly increased amounts of insulin. At the stage at
which they were killed obesity had reached its maximum18. Brobeck, J. R., Tepperman, J., Long, C. N. H. Yale J. Biol. Med. 1943,
15, 831.19. Mayer, J., Bates, M. W., Van Itallie, T. B. Metabolism, 1952, 1, 340.20. Hales, C. N., Kennedy, G. C. Biochem. J. 1963 (in the press).21. Mayer, J. Voeding, 1955, 16, 62.22. Hausberger, F. X., Hausberger, B. C. Amer. J. clin. Nutr. 1960, 8, 671.23. Kennedy, G. C., Mitra, J. J. Physiol. 1963, 166, 395.
(a) Enlarged islet from fat rat, and (b) islet from normal control rat. (Gomori’saldehyde fuchsin. x 140.)
982
level, and glucose-tolerance had just begun to deteriorate.Further studies are being undertaken both at shorter andlonger postoperative intervals, and the effect of removingother endocrine glands is being investigated to find outmore about the trophic influence on the islet-cells.
G. C. KENNEDYM.B., PH.D. Lond.
R. A. PARKERM.D. Lond.
M.R.C. Department of Experimental Medicine,University of CambridgeDepartment of Pathology,
St. Mary’s Hospital,London, W.2
LENGTHY SURVIVAL
OF SHEEP-KIDNEY HOMOGRAFTSAFTER TREATMENT WITH TRIAMCINOLONE
NATURAL corticosteroids suppress the formation of
many antibodies 1-3 but have only transient effect on thehomograft reaction, even when combined with mustineand anti-metabolites, like 6-mercaptopurine or B.w.
57-322.4-s On the other hand, experimental glomerulo-nephritis can be prevented by the more potent syntheticcorticosteroids, like triamcinolone (9-alpha-fluoro-16-alpha-hydroxy-prednisolone)7 ; and, as the glomerularbasement membrane is antigenic 11 9 it may possibly bethe first damaged area in the transplanted kidney.10 11
Merrill et al.12 reported a kidney transplantation innon-identical twins; they suggested that small doses ofirradiation and large doses of cortisone might have" aborted " rejection of the partially tolerated kidneysome 8 months after the transplantation. It thereforeseemed reasonable to try this treatment at the time of the
transplantation and in view of the promising findings, weshould like to give a preliminary report of our results.The animals studied were unrelated Merino wethers,
weighing about 35 kg. Two recipients were treated con-tinuously with triamcinolone (’Ledercort’), 1 mg. perkg. per day, from the day of kidney transplantation. Thedonor sheep were untreated. The kidneys were trans-planted into the neck, and the recipient’s own kidneyswere left intact. The homografts functioned for 36 and38 days respectively. In both cases anuria then developed,owing to renal-vein thrombosis. On removal, the kidneyswere about double the normal size, and they showedmicroscopically a modified homografI reaction; there wereisolated areas of round-cell infiltration and infarction,with moderate to severe hydronephrosis.Two other wethers were given 250r total body irradia-
tion 24 hours before the transplantation. They were thentreated as the previous two. The grafts functioned untilthe death of the sheep, probably owing to infection andintestinal hxmorrhage, 11 and 19 days after the operation.Both kidneys were macroscopically normal, and micro-scopically only very slight cellular infiltration was
observed around the vessels.In untreated sheep, kidney homografts become anuric
in 3 to 6 days, and they show intense round-cell infiltration1. Bjorneboe, M., Fischel, E. E., Stoerk, H. C. J. exp. Med. 1951, 93, 37.2. Fischel, E. E., Vaughan, J. H., Photopoulos, C. Proc. Soc. exp. Biol.,
N.Y. 1952, 81, 344.3. Overman, J. R., Hanan, R. ibid. 1953, 84, 420.4. Billingham, R. E., Krohn, P. L., Medawar, P. B. Brit. med. J. 1951, i,
1157.5. Baker, R., Gordon, R., Huffer, J., Miller, G. H. Arch. Surg. 1952, 65,
702.6. Calne, R. Y. Transplant. Bull. 1961, 28, 65.7. Lang, K., Demoleas, P. N., Wenk, E. J. Amer. J. med. Sci. 1960, 240,
458.8. Krakower, C. A., Greenspon, S. A. Arch. Path. 1951, 51, 629.9. Hill, A. G. S., Cruickshank, B. Brit. J. exp. Path. 1953, 34, 27.
10. Dempster, W. J. Brit. J. Surg. 1953, 40, 447.11. Dempster, W. J. Brit. J. plast. Surg. 1953, 5, 228.12. Merrill, J. P., Murray, J. E., Harrison, J. H., Friedman, E. A,
Dealy, J. B., Dammin, G. J. New Engl. J. Med. 1960, 262, 1251.
and autolysis.13 We have not been able previously tolengthen the survival by such procedures as supralethalirradiation with bone-marrow transfusion, sublethal
irradiation, or sublethal irradiation plus repeated injectionsof donor spleen-cells. In sheep treated with sublethalirradiation (350-450r) the kidneys showed no round-cellinfiltration, and we postulated that the short functionalsurvival was owing to glomerular damage, perhaps byhumoral antibody,14 The long functional survival andnormal histological appearance of the kidneys aftertriamcinolone and irradiation seem to support this
postulate. We are now investigating the problem furtherby electron microscopy and the fluorescent-antibodytechnique.
R. M. MITCHELLM.B., B.MED.SC. N.Z., F.R.C.S.,
F.R.A.C.S.
B. G. STEVENSB.SC. Queensland
O. E. BUDTZ-OLSENM.D. Cape Town
N. LANGLEYM.B. Queensland
Departments of Surgeryand Physiology,
University of Queensland,Brisbane
GROWTH OF VARICELLA-ZOSTER VIRUS INHUMAN THYROID TISSUE CULTURES
THE serial propagation in human embryo tissue cul-tures of the virus of varicella and herpes zoster (v-zvirus) was described by Weller 15 in 1953, and furtherstudies of this virus were recorded by Weller et al. 1617and by Taylor-Robinson. 18 These workers noted thatv-z virus grows and produces cytopathic changes invarious human tissue cultures but that infective virus doesnot appear in the tissue-culture fluids, so serial transferof the virus can be regularly achieved only by subcultureof infected tissue-culture cells. They also found thatvarious procedures which disrupt the tissue-culture cellsreleased only small amounts of virus from the cells." ’ 1
This is in contrast to the virus in vesicle fluid, which ismainly cell-free.
In further studies with v-z virus, it has been found to
grow well in human thyroid tissue culture. This tissueis more sensitive than is human amnion for the isolationof v-z virus from vesicle fluids or for the titration of
suspensions of infected cells.19 There is also evidencefrom the formation of secondary foci of infection in
thyroid tissue cultures that a small amount of virus isreleased into the tissue-culture fluids. When these cellsare disrupted by ultrasonic vibration, however, muchlarger amounts of infective virus are released. The
procedure is:Bottles of thyroid tissue cultures, infected with v-z virus
and in which 75% or more of the cells show cytopathicchanges, are treated with sodium edetate to remove the cellsfrom the glass. The cells are then sedimented by low-speedcentrifugation and resuspended in approximately one-tenth ofthe volume of the fluid originally in the cultures. Thisconcentrated cell suspension is then treated for 2 min. on anM.S.E. Mullard ultrasonic disintegrator, using a stainless-steelvibrator probe with an end diameter of 3/4 in. and a velocityincrease ratio of 4:1. The container for the cell suspension issurrounded by crushed ice during the treatment. The resulting13. Mitchell, R. M. Aust. N.Z.J. Surg. 1959, 28, 263.14. Mitchell, R. M., Budtz-Olsen, O. E., Stevens, B. G., Devereux, G. A.
Transplantation, 1963, 1, 388.15. Weller, T. H. Proc. Soc. exp. Biol., N. Y. 1953, 83, 340.16. Weller, T. H., Witton, H. M., Bell, E. J. J. exp. Med. 1958, 108, 843.17. Weller, T. H., Witton, H. M. ibid. p. 869.18. Taylor-Robinson, D. Brit. J. exp. Path. 1959, 40, 521.19. Caunt, A. E., Taylor-Robinson, D. (in preparation).