the interface between microbiologist and clinician - bsim · pdf filethe interface between...
TRANSCRIPT
1
The interface between microbiologist and clinician
A. Naessens
The interface
A surface which forms the boundary between
two phases or systems
The laboratory The clinician

2
The role of the physician
Physical examination
Differential diagnosis
Request adequate laboratory test to
confirm/exclude the diagnosis
Start adequate treatment
Role of the microbiological laboratory
The provision of accurate clinically significant data for the diagnosis and treatment of infections
The production of laboratory data is a culmination of sequential processes including preanalytic, analytic, and postanalytic laboratory activities and begins with the clinician’s request for a specific test in an individual patient

3
Interfaces
Physician Lab Physician
Request sample Sample processing
Generating result Interprete
result
Treat
Interfaces
Physician Lab Physician
Request sample Sample processing
Generating result Interpret
result
Exchange the information as rapidly as possible
As accurate as possible
As clearly as possible

4
Interfaces
Physician Lab Physician
Request sample Sample processing
Generating result Interpret
result
Treat
Sample request
Clinician’s responsability
Adequate sample for the
condition
Adequate transport
medium
Adequate labeling
Lab’s responsability
Instructions to sampling
and transportation
Easy acces
Up to date
Electronic version

5

6

7

8
Patient sampling
Clinician’s responsability
Adequate sample for the
condition
Adequate transport
medium
Adequate labeling

9
Adequate sample identification
Information
Add info only when it is important
Abces: cerebral/abdominal/prostetic joint
Blood culture: suspicion of brucella
Do not give info if the sample is clear cut
Urine, throat
Consise
Do not mention clinically unimportant items (fever, pain)
Info for specific search for certain MO
CMV
Interfaces
Physician Lab Physician
Request sample Sample processing
Generating result Interpret
result
Treat

10
Generate result
As soon as possible
Organization of the laboratory
Day 0 Sample processing in the lab.
Gram stain
Overnight incubation.
Day 1 Inspection of the culture for
bacterial growth.
If positive: presumptive
identification. Further work
out
If negative: further incubation
Day 2 Identification + reading
suceptibility
Imrove speed? What can be done

11
Imrove speed of detecting micro-organisms
Molecular techniques
Molecular techniques
PCR:
Advantages:
“quick” result
Ideal for difficult to grow micro-organisms
Disadvantages
Cost
Technical more demanding
Contamination problems (false pos results)
Request for specific pathogens
Explosion of requests

12
Dynamcis of rapid increase of pcr requests
1. PCR for pathogen became available
2. Diagnostic tool is used in wel circumscribed clinical entities on well defined samples
3. Diagnostic tool is used in less well defined entities in samples not well validated
4. A positive result is found!
5. An abstract of this case is presented at an international congress
6. ….
Need for a good interface
Dynamcis of rapid increase of pcr requests
1. All classical test results remaine negative in a
critically ill patient
2. Question from clinicician to the lab
We want to have tested this patient with all the
PCR’ tests that are available
Need for a good interface

13
Interface
1 Restricted use of PCR on clinically relevant
samples (information in an easy to acces
laboratory guide)
2 Possibility to offer rapid testing in selected
cases
Interfaces
Physician Lab Physician
Request sample Sample processing
Generating result Interpret
result
Treat

14
Result transmission
Rapid
Alert transmission
Blood cultures
TBC
Use the communication best suited for the situation
Limit the alert results to those which really matter
Alert results are dependent on the speciality
Interfaces
Physician Lab Physician
Request sample Sample processing
Generating result Interpret
result
Treat

15
Interfaces
Physician Lab Physician
Request sample Sample processing
Generating result Interprete
result
Start empirical
treatment
Change
Treatment
Starting empirical treatment
Based on experience; determined from
experimental data
Starting therapy based on
The microorganisms most often isolated in the
respective infections
The antimicrobial sensitivity of the micro-organism

16
Based on (inter)national recommendations
International guidelines
National guidelines
Need for national
epidemiology
Starting empirical treatment
How can the laboratory help in selecting the
empirical treatment?
17
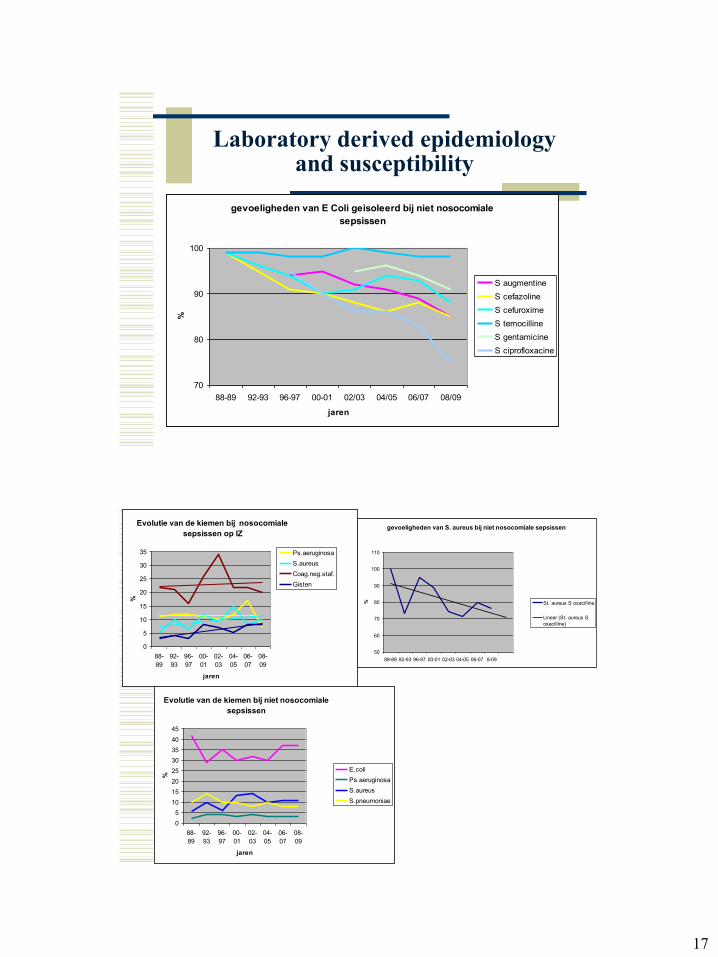
Laboratory derived epidemiology and susceptibility
yearly epidemiological review of the isolated
microorganisms
Follow up of the susceptibility of the isolated
micro organisms
gevoeligheden van E Coli geisoleerd bij niet nosocomiale
sepsissen
70
80
90
100
88-89 92-93 96-97 00-01 02/03 04/05 06/07 08/09
jaren
%
S augmentine
S cefazoline
S cefuroxime
S temocilline
S gentamicine
S ciprofloxacine
Evolutie van de kiemen bij niet nosocomiale
sepsissen
0
5
10
15
20
25
30
35
40
45
88-
89
92-
93
96-
97
00-
01
02-
03
04-
05
06-
07
08-
09
jaren
%
E.coli
Ps.aeruginosa
S.aureus
S.pneumoniae
gevoeligheden van S. aureus bij niet nosocomiale sepsissen
50
60
70
80
90
100
110
88-89 92-93 96-97 00-01 02-03 04-05 06-07 8-09
% St. aureus S oxacilline
Linear (St. aureus S
oxacilline)
Evolutie van de kiemen bij nosocomiale
sepsissen op IZ
0
5
10
15
20
25
30
35
88-
89
92-
93
96-
97
00-
01
02-
03
04-
05
06-
07
08-
09
jaren
%
Ps.aeruginosa
S.aureus
Coag.neg.staf.
Gisten
18
Lab and clinician: the interfaces
The lab is helping the clinician
The lab need not perform blindly all request
from the clinician
Find a good balance
Realize and aknowledge the work
The better the lab and the clinician are working
together the better the patient will be cared for