the immunofluorescent detection of leptospira interrogans serogroup icterohaemorrhagiae serovar...
TRANSCRIPT

Letters in Applied Microbiology 1987,4,25-27 AIT/006
The immunofluorescent detection of Leptospira interrogans serogroup Icterohaemorrhagiae serovar icterohaemorrhagiae infections in human tissues
J.V. HOOKEY, SHEENA A. WAITKINS & M. PALMER WHOJFAO Collaborating Centre for Research and Reference on Leptospirosis, PHLS Leptospira Reference Unit, County Hospital, Hereford HR12ER, U K
Received 30 October 1986 and accepted 31 October 1986
HOOKEY, J.V., WAITKINS, S .A. & PALMER, M. 1987. The immunofluorescent detection of Leptospira interrogans serogroup Icterohaemorrhagiae serovar icterohaemorrhagiae infections in human tissues. Letters in Applied Microbiology 4, 25-27.
The identification of Leptospira interrogans serogroup Icterohaemorrhagiae serovar icterohaemorrhagiae infections in post-mortem tissues by direct fluorescence microscopy is demonstrated by the use of a serogroup-specific fluorescein iso- thiocyanate label.
Leptospirosis is an acute, febrile zoonotic disease distributed world-wide (Faine 1982). The clinical syndrome of Weil’s disease varies in severity from the subclinical to hepato-renal failure when associated with the Ictero- haemorrhagiae serogroup (Turner 1967, 1968).
The laboratory diagnosis of leptospirosis in man relies on the isolation of leptospires from body fluids and tissues or the demonstration of an increase in specific serum antibody levels (Galton et al. 1962; Turner 1968; Terpstra et al. 1985; Waitkins 1985). Antibodies may take up to 21 d to develop and their rise may be inter- fered with by the use of antibiotics. Therefore, serodiagnosis based upon antibody detection cannot be relied upon when a patient dies soon after the clinical date of onset.
No more successful is the isolation of lepto- spires from body fluids and tissues since lepto- spiraemia and leptospiruria are transitory (Turner 1968). The use of broad spectrum anti- biotics and correct isolation media (Palmer et al. 1984) are factors that determine the rate of isolation. Furthermore, the detection of leptospires by dark-field microscopy is limited, requiring the presence of viable motile bacteria that may be confused by the presence
of proteinaceous filaments or pseudo-leptospires (Rahman & Macis 1979).
Conversely, immunofluorescence has proved to be of value in the rapid detection of lepto- spiral infections in animal tissues (Ellis et al. 1982; Giles et al. 1983) and also in human muscle tissue (Sheldon 1953).
In this paper we report on two fatal cases of leptospiral infections in humans and demon- strate the detection of the infecting serogroup, Leptospira interrogans Icterohaemorrhagiae, in post-mortem tissues by serogroup-specific immunofluorescent methods.
Materials and Methods
PATIENT C A S E HISTORIES
Patient A died 10 d after the clinical date of onset. Initial serological results, based upon the microscopic agglutination test (MAT), the com- plement fixation test and the enzyme-linked- immunosorbent assay (ELISA) were negative. However, a serum sample taken after 8 d gave a positive ELISA-IgM result and a weak positive MAT result, though no predominant infecting serogroup could be established (see Table 1). No
26 J. I/. Hookey et al. Tahle 1
Serological test Patient A Patient B Microscopic agglutination test Icterohaemorrhagiae SO* Icterohaemorrhagiae 1280*
Sejroe 40 Autumnalis 160 Autumnalis 0 Sejroe 40 Canicola 0 Canicola 0
Complement fixation test so* 640* ELISA IgG 0 0 ELISA IeM hdo* Ado*
* Reciprocal end-point titre.
leptospires were isolated from blood or post- mortem tissues.
Patient B died 12 d after the clinical date of onset. No leptospires were isolated from either blood or post-mortem tissues. Serological results indicated leptospirosis and the infecting serogroup appeared to be Icterohaemorrhagiae (see Table 1).
A fluorescent antibody technique was applied to the post-mortem tissues from both patients.
P R O D U C T I O N O F IgG I M M U N O G L O B U L I N S
Hyperimmune rabbit sera directed against L. interrogans serogroup Icterohaemorrhagiae serovar icterohaemorrhagiae, serogroup Canic- ola serovar canicola and serogroup Sejroe serovar hardjo were raised following the method discussed by Faine (1982).
The IgG immunoglobulins were pFepared from each serum using a DEAE ‘AffGel Blue’ dedicated chromatographic support according to the conditions specified by the manufacturers (Bio-Rad Laboratories, Watford, UK).
C O N J U G A T I O N OF FLUORESCEIN I S O T H I O C Y A N A T E TO IgG IMMUNOGLOBULINS
Each preparation was conjugated to fluorescein isothiocyanate (FITC, isomer I; Sigma Chemi- cal Co., Poole, UK) by the method of The & Feltkamp (1970).
The fluorochrome-protein ratio was calcu- lated (Hudson & Hay 1980) and the end-point titre determined by direct immunofluorescent titration against acetone fixed smears of homologous antigen.
PREPARATIONS A N D IMMUNOFLUORESCENT S T A I N I N G OF H U M A N TISSUES
Post-mortem kidney and liver tissues from both patients were homogenized in bovine serum albumin diluent (bovine serum albumin fraction V, 5% w/v, Sigma Chemical Co.; phosphate buffered saline, pH 7.2, Oxoid, Basingstoke, UK) by pressure through the barrel of a syringe. The homogenates were smeared onto ethanol- cleaned glass slides, allowed to dry at room temperature and fixed in acetone for 10 min. The conjugate, diluted in bovine serum albumin diluent, was added to fixed smears and incu- bated in a moist chamber for 60 min at 30°C. The preparations were then washed twice in bovine serum albumin diluent for 10 min, lightly blotted and mounted in Citifluor (Citifluor Ltd, The City University, London, UK). Prep- arations were examined by incident light fluo- rescence microscopy (Leitz Instruments Ltd, Luton, UK). A positive diagnosis was made only where fluorescing organihs with typical leptospiral morphology were observed.
Results
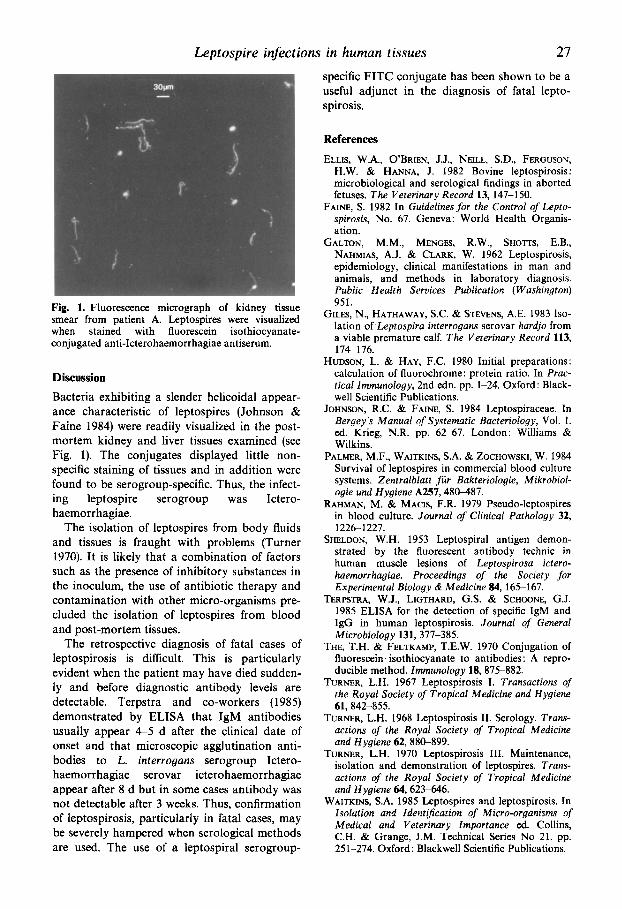
The serological results from patients A and B are given in Table 1. The fluorochrome-protein ratios of the conjugates were 1.5 (serogroup Icterohaemorrhagiae), 1.5 (serogroup Canicola) and 1.7 (serogroup Sejroe) and the end-point titre for each fluorescent label was 1 : 100. Post- mortem tissues from both patients exhibited strong fluorescence with FITC-conjugated anti- body to serogroup Icterohaemorrhagiae (see Fig. 1) while there was no reaction with FITC- conjugated antibodies to the serogroups Canic- ola or Sejroe.
Leptospire infections in human tissues 27
specific FITC conjugate has been shown to be a useful adjunct in the diagnosis of fatal lepto- spirosis.
Fig. 1. Fluorescence micrograph of kidney tissue smear from patient A. Leptospires were visualized when stained with fluorescein isothiocyanate- conjugated anti-Icterohaemorrhagiae antiserum.
Discussion Bacteria exhibiting a slender helicoidal appear- ance characteristic of leptospires (Johnson & Faine 1984) were readily visualized in the post- mortem kidney and liver tissues examined (see Fig. 1). The conjugates displayed little non- specific staining of tissues and in addition were found to be serogroup-specific. Thus, the infect- ing leptospire serogroup was Ictero- haemorrhagiae.
The isolation of leptospires from body fluids and tissues is fraught with problems (Turner 1970). It is likely that a combination of factors such as the presence of inhibitory substances in the inoculum, the use of antibiotic therapy and contamination with other micro-organisms pre- cluded the isolation of leptospires from blood and post-mortem tissues.
The retrospective diagnosis of fatal cases of leptospirosis is difficult. This is particularly evident when the patient may have died sudden- ly and before diagnostic antibody levels are detectable. Terpstra and co-workers (1985) demonstrated by ELISA that IgM antibodies usually appear 4-5 d after the clinical date of onset and that microscopic agglutination anti- bodies to L. interrogans serogroup Ictero- haemorrhagiae serovar icterohaemorrhagiae appear after 8 d but in some cases antibody was not detectable after 3 weeks. Thus, confirmation of leptospirosis, particularly in fatal cases, may be severely hampered when serological methods are used. The use of a leptospiral serogroup-
References
ELLIS, W.A., O’BRIEN, J.J., NEILL, S.D., FERGUSON, H.W. & HANNA, J. 1982 Bovine leptospirosis: microbiological and serological findings in aborted fetuses. The Veterinary Record 13, 147-150.
FAINE, S. 1982 In Guidelines for the Control of Lepto- spirosis, No. 67. Geneva: World Health Organis- ation.
GALTON, M.M., MENGES, R.W., SHOTTS, E.B., NAHMIAS, A.J. & CLARK, W. 1962 Leptospirosis, epidemiology, clinical manifestations in man and animals, and methods in laboratory diagnosis. Public Health Seruices Publication (Washington) 951.
GILES, N., HATHAWAY, S.C. & STEVENS, A.E. 1983 Iso- lation of Leptospira interrogans serovar hardjo from a viable premature calf. The Veterinary Record 113, 1 7 6 1 76.
HUDSON, L. & HAY, F.C. 1980 Initial preparations: calculation of fluorochrome: protein ratio. In Prac- tical Immunology, 2nd edn. pp. 1-24. Oxford : Black- well Scientific Publications.
JOHNSON, R.C. & FAINE, S. 1984 Leptospiraceae. In Bergey’s Manual of Systematic Bacteriology, Vol. 1. ed. Krieg, N.R. pp. 62-67. London: Williams & Wilkins.
PALMER, M.F., WAITKINS, S.A. & ZOCHOWSKI, W. 1984 Survival of leptospires in commercial blood culture systems. Zentralblatt fur Bakteriologie, Mikrobiol- ogie und Hygiene A257,48&487.
RAHMAN, M. & MACIS, F.R. 1979 Pseudo-leptospires in blood culture. Journal of Clinical Pathology 32, 1226-1227.
SHELDON, W.H. 1953 Leptospiral antigen demon- strated by the fluorescent antibody technic in human muscle lesions of Leptospirosa ictero- haemorrhagiae. Proceedings of the Society for Experimental Biology & Medicine 84, 165-167.
TERPSTRA, W.J., LIGTHARD, G.S. & SCHOONE, G.J. 1985 ELISA for the detection of specific IgM and IgG in human leptospirosis. Journal of General Microbiology 131, 377-385.
THE, T.H. & FELTKAMP, T.E.W. 1970 Conjugation of fluorescein isothiocyanate to antibodies : A repro- ducible method. Immunology 18, 875-882.
TURNER, L.H. 1967 Leptospirosis I. Transactions of the Royal Society of Tropical Medicine and Hygiene
TURNER, L.H. 1968 Leptospirosis 11. Serology. Trans- actions of the Royal Society of Tropical Medicine and Hygiene 62,88G899.
TURNER, L.H. 1970 Leptospirosis 111. Maintenance, isolation and demonstration of leptospires. Trans- actions of the Royal Society of Tropical Medicine and Hygiene 64,623-646.
WAITKINS, S.A. 1985 Leptospires and leptospirosis. In Isolation and IdentijScation of Micro-organisms of Medical and Veterinary Importance ed. Collins, C.H. & Grange, J.M. Technical Series No 21. pp. 251-274. Oxford: Blackwell Scientific Publications.
61,842-855.