the endothelial cell damage in acute glaucoma. on the corneal thickness response to intraocular...
TRANSCRIPT

A C T A O P H T H A L M O L O G I C A V O L . 5 8 1 9 8 0
Department of OphthalmoloQ (Head: N . Ehlers), Universitj of Aartiur, Denmark.
THE ENDOTHELIAL CELL DAMAGE IN ACUTE GLAUCOMA. ON THE CORNEAL THICKNESS RESPONSE
TO INTRAOCULAR PRESSURE
THOMAS OLSEN
In order to asses a possible damage to the corneal endothelium during pressure induced abnormal hydration of the cornea, 23 patients with a previous attack of unilateral acute glaucoma were photographed with the specular microscope. As compared to the healthy side, the endothelium of the affected side showed a mean decrease in cell density of 23.1 %, range -4.8 to 68% (P<O.OOl). In retrospect this cell loss was found to correlate significantly to the increase in corneal thickness measured during the acute attack on first day of admission. At present examination mean central corneal thickness was identical in the affected and unaffected eye. A large variation was, however, found in the intraocular pressure of the previously attacked eye. If the subject inter-eye difference in intraocular pressure was related to the inter-eye difference in corneal thickness a significant negative correlation appeared. It is concluded that the intraocular pressure has a dual effect on the corneal hydration: if the endothelium is intact, the intraocular pressure decreases corneal thickness, whereas an increase is seen only if the endothelium is acutely damaged.
Key wordi: cornea - endothelium - acute glaucoma - corneal thickness - intraocular pressure - specular microscope.
Abnormal hydration of the cornea may occur as epithelial and/or stromal oedema. The former is a well known clinical feature of increased intraocular pressure. In physical terms it has been explained to occur when the interstitial fluid pressure of the stroma becomes positive (Ytteborg & Dohlman 1965a) and may as such occur without stromal oedema.
The influence of the intraocular pressure on the total corneal hydration, of which
Received August 20, 1979.
A r u ophthal. 38. 2 257
17

Thomas Ol.sen
stromal hydration constitutes a large part, is however a confusing and controversial subject in ophthalmological literature. Does the intraocular pressure force fluid into the stroma or does it oppose the swelling tendency of the cornea?
The clinical index of total corneal hydration is the corneal thickness (see Mishima 1968). In clinical studies both increased (Ytteborg & Dohlman 1965a; De Cevallos et al. 1976) and decreased (Sbordone 1953; Olson & Kaufman 1978) corneal thickness have been observed with increased intraocular pressure. An increase in corneal thickness following a decrease in intraocular pressure has also been reported (Ehlers & Riise 1967; Ehlers 1970). In vitroexperiments have shown the ‘intraocular’ pressure to increase (Harris et al. 1956; Maurice & Hoefle 1973) and to decrease (Mayes & Hodson 1978) corneal hydration in experiments where the endothelium is claimed to be intact.
The above-mentioned studies have largely dealt with intraocular pressures around the physiological range and elevated pressures as they are encountered in open angle and secondary glaucomas. In severe cases of increased intraocular pressure, e.g. in acute glaucoma there is general agreement that, in addition to the epithelia1 oedema, a stromal oedema may develop (see Etienne 1969; Chandler & Grant 1965).
Since Leber’s time (1873) the corneal endothelium has been known to be a crucial factor for the water permeability of the cornea. A study on the state of the corneal endothelium during pressure-induced abnormal hydration of the cornea therefore seemed indicated.
Subjects and Methods
Twenty-three patients in the age range 50-84 years with a mean of 69 years participated in the study. They comprised all patients who had been admitted to the eye clinic for the past two years with one unilateral attack of acute glaucoma. Nineteen patients (15 women and 4 men) had suffered from acute angle closure glaucoma, while 4 patients (3 men and 1 woman) had acute haemorrhagic glaucoma. Patients with any other history of disease or trauma to either eye with the exception of senile lens opacities were excluded. On admission they all showed ‘corneal oedema’ with epithelial bullae as indicated in the case record. In some patients the actual corneal thickness had been measured on the first day of admission either by the doctor in charge or in some cases by the author. Following the acute attack all patients were trabeculectomized or iridectomized on the affected side. In the angle closure group, 12 patients were, a few months later, iridectomized on the other side, while the remainder of the patients were unoperated on the other eye at time of the present examination. Two patients were iridectomized on the other eye only three days prior to the examination. Tonometry and pachometry readings were discarded in these patients, while estimates on cell density were not. In the remainder the postoperative period for the control eye, if operated, was more than two months.
258
Corneal Endothelium in Acute Glaucoma
t 2 0
+10
0
-10
- 20 - 30 - 40
- 50 - 6 0
- 70
The shortest time period between onset of attack and present examination was one month; mean 13 months. One patient with haemorrhagic glaucoma was receiving antiglaucomatous treatment on the affected eye, while the rest of the patients either received the same medical treatment to both eyes (three patients) or were without medication at all.
The control group comprised 39 subjects in the age range 50-97 years (mean 72 years) with no history of eye disease or trauma other than senile lens opacities. Some of these subjects have been included in the normal series previously reported by Olsen (1979).
The central endothelium of both eyes of patients and normal subjects were photographed and central endothelial cell densities estimated as described earlier (Olsen 1979). From the control group a normal relative inter-eye variation in cell density was constructed by randomly choosing right or left eye as reference for the observed difference in cell counts. By doing this, the small systematical right-left difference observed in normal eyes (Olsen 1979) is neglected. In the acute glaucoma group the difference in cell counts observed between the affected and the unaffected eye was expressed as relative to the unaffected eye.
In order to ascertain a possible damage to the endothelium during glaucoma-operation, 7 other eyes were photographed before and after (range 3-5 months) a trabeculectomy or iridectomy in that eye.
Central corneal thickness was measured using a modified Haag-Streit pachometer (Ehlers & Sperling 1977). Intraocular pressure was measured using a Goldmann applanation tonometer attached to the slit lamp.
-
-
.....
-
-
-
-
-
-
-
normal acute % A subjects glaucoma
....... .$ .... . . .
I
t: . .. $
*:
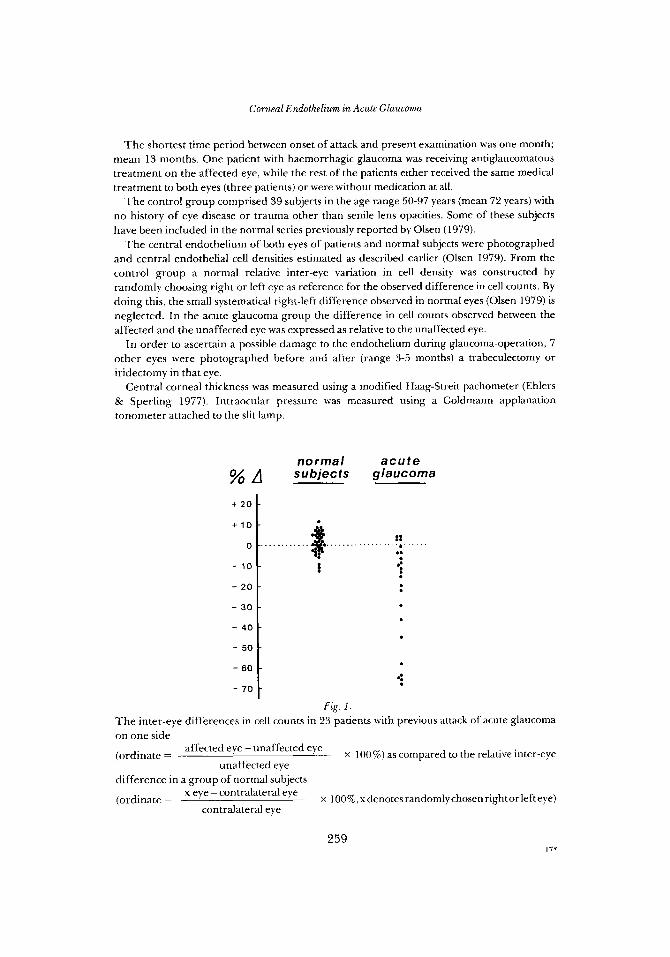
Fig. 1. The inter-eye differences in cell counts in 23 patients with previous attack of acute glaucoma on one side
(ordinate =
difference in a group of normal subjects
(ordinate =
affected eye - unaffected eye
unaffected eye x 100%) as compared to the relative inter-eye
x eye - contralateral eye
contralateral eye x loo%, xdenotes randomly chosen right or left eye)
259 I7*
Thomas 0l.tt-n
Patient No.
Results
Cell count before After Operation
(cellsimm*)
On the average the cell count on the side with previous attack of acute glaucoma was 23.1% lower than the contralateral side with a large range in the inter-eye difference (Fig. 1). In the normal group the inter-eye difference was found to have a standard error of 5.7%. This means that 95% of the normal inter-eye differences was less than 11.4%, following the procedure of randomly chosing left or right eye as reference. In this way 13 of the patients could be said to have significantly lower endothelial cell density on the affected side. The counts themselves, however, did not show any definite grouping into normal and abnormal differences (Fig. 1) and taking the group as a whole the inter-eye differences were highly significantly different from zero. (A Wilcoxon test for paired differences showed P <0.001).
The subgroup of acute haemorrhagic glaucomas showed a mean decrease in cell density of 16.4% (range 4 to 46%). In either group the cell loss was not related to time after the attack.
Table I shows the cell counts obtained in 7 patients undergoing a standard glaucoma operation. Mean change in cell counts were found to be -1.3%. The standard error of independent cell counts obtained with the present technique has previously been shown to be 3.7% (Olsen 1979). Using this figure and assuming a normal distribution the 95% confidence limits for the observed mean value can be calculated to be -2.7 and +0.1%, respectively. Thus no significant cell loss occurred during the operation, and, if there was any, it was very small. This indicates the cell loss depicted in Fig. 1 not to be iatrogenic but to be a result of the attack.
In those instances where corneal thickness measurements were available on the
Table I . Estimated endothelial cell density in 7 patients before and 3-5 months after glaucoma
operation. Mean change in cell density is - 1.3%.
1 iridectom y 1430 1377 -3.7 2 trabeculectom y 2378 2485 +4.5 3 iridectomy 2825 277 1 -1.9 4 trabeculectom y 1627 1663 +2.2
6 trabeculectom y 2699 2646 +2.0 5 trabeculectom y 3003 2986 -0.6
7 trabeculectom y 3039 2807 -7.6
260

Comenl Endothelaurn in Aczitr GlaucomiL
CELL LOSS (%l
8 .
A C C T I I I I
0 0.1 0 .2 0.3 (mm)
Fig. 2. The increase in central corneal thickness (CCT) on the first day of admission related to the estimated cell loss on the affected eye. (Spearman’s rank correlation coefficient rs = 0.68,
P <0.05, n = 1 1 ) .
first day of admission, the increase in corneal thickness on the affected side as compared to contralateral side was found to be significantly correlated to the cell loss (Fig. 2). Attempts at correlating the cell loss to the visual acuity after the acute attack were unsuccessful.
At the present follow-up the corneal thicknesses on the affected side were not different from the unaffected side. Mean central corneal thickness (5 SD) was 0.515 k 0.021 and 0.516 f 0.026 mm, respectively. The corneal thickness showed no trend towards a gradual change versus time in the post-attack period studied. None showed epithelial oedema. Mean intraocular pressure (+ SD) was 18.2 & 8.8 (range 9-42) and 16.5 k 4.2 (range 12-26) mmHg on the affected an unaffected side, respectively. As can be seen the main difference existed in the much larger variation in the intraocular presures found in the eye with previous attack of acute glaucoma. If the inter-eye differences in intraocular pressure were plotted against the inter-eye differences in central corneal thickness, a significant negative correlation appeared (Fig. 3). Thus, in this situation where the patients served as their own controls the intraocular pressure was found to decrease the corneal thickness.
261

Thomas Olsen
t 1 0 -
0 -
-10 -
- 20 -
-30-
A IOP ( m m Hgl .
a . . . . . . . . t o . . . .
.
Discussion
Leber ( 1873) was the first to demonstrate the importance of the corneal endothelium in preserving corneal hydration. In a number of thoroughly conducted experiments he always ended up with the same conclusion: a posterior hydrostatic pressure could only force fluid through the cornea if its posterior limiting membrane was altered either deliberately, or as the result of post mortem changes or accidental trauma. The duration of his experiments was however rather short, as they were mainly directed towards an understanding of the physiological role of the endo- thelium.
The proliferative power of the adult human corneal endothelium is generally thought to be very limited (Kaufman et al. 1966; Stocker 1971), and specular microscopic studies of the adult human endothelium have consistently shown a decrease, and never an increase in the cell density in response to injury (Bourne & Kaufman 1976; Forstot et al. 1977; Rao et al. 1978). After cataract extraction there is a problem of an accurate measurement of the cell loss due to the non-uniformly distribution of the cell density on the cornea (Rao et al. 1978). In acute glaucoma it seems unlikely that there is any such uneven distribution of the damage to the endothelium. The decrease in the cell density observed in the present study is
262

Corneal Endothelium in Acute Glaucoma
therefore strongly indicative of the irreversible cell loss having occurred during the acute attack of glaucoma. The results of Svedberg (1975) suggest that the pressure itself may destroy the endothelial layer, but it may be suggested that additional factors such as speed of onset, ischemia and anaerobic metabolism due to impaired flow of aqueous may also contribute to the endothelial damage.
The endothelial damage had important consequences on the corneal hydration as shown in Fig. 2. It was not tried to correlate the duration of the attack and the actual ocular tension to the cell loss due to difficulty in precise determinations of these variables. It may be suggested, however, that the cellular destruction was ‘the final common path’ of these variables to increase the corneal hydration.
Irvine (1956) noted an association between a low number of endothelial cells and the tendency of the cornea to become oedematous at increased intraocular pressure. He concluded, however, the low cell density as such to be the cause of the abnormal hydration. The results of the present study indicate that it is the active break-down of cells that matters. It is remarkable, that even if more than 50% of the cells had been destroyed it did not seem to have a permanent effect on corneal hydration. Mean corneal thickness of the previously attacked eye was found not to differ from the unaffected eye. The latter result is in accordance with other authors (Lowe 1969; De Cevalloset al. 1976).
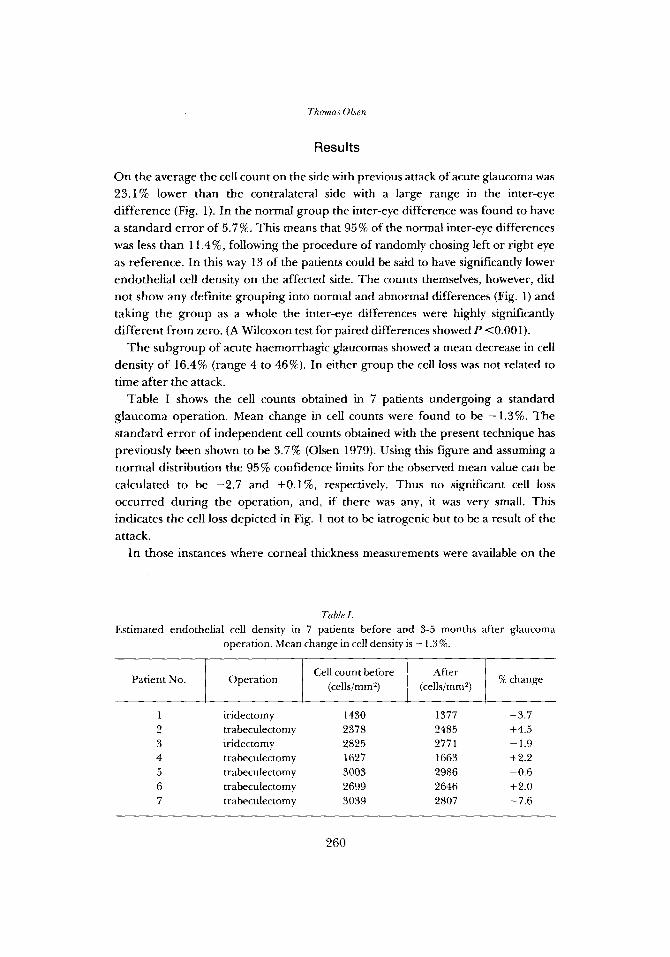
At the present follow-up examination, the patients turned out to have a large variation in the intraocular pressure in the previously attacked eye. Using the patients contralateral eye as control, the intraocular pressure was shown to be inversely correlated to the corneal thickness (Fig. 3) . In interpreting these results it is important to remember that the patients at this time had an intact endothelium as documented by the intact endothelial reflex (Fig. 4). During the acute attack with increased corneal thickness it has never in hands of the author been possible to obtain a normal endothelial reflex (Fig. 5 ) .
The results of the present study therefore indicate that the intraocular pressure increases corneal thickness if the endothelial layer i s damaged but decreases the corneal thickness if the endothelial layer is preserved. The hypothesis that the state of the endothelium may switch the thickness response of the cornea in either direction has been suspected by some authors (Mishima 1968; Ehlers 1970) but not documented.
In animal experiments Ytteborg & Dohlman (1965) suggested that the increased intraocular pressure might have damaged the endothelium for the increased thickness to occur. The clinical data reported by these authors (Ytteborg & Dohlman 1965a) are however inconclusive on that point, since many of their patients must have had secondary glaucoma where damage to the endothelium via other routes (operation, inflammation) cannot be ruled out (Olson & Kaufman 1978).
263
PYZ

Corneal En.dotheEiu.m in. Acute Glaucoma
T h e fact that the cornea with intact endothelium thins in response to elevated intraocular pressure raises some theoretical questions as to the function of the endothelium in this situation. If the endothelium was highly impermeable to water it would be understandable that an increased pressure gradient across the cornea would make it thin. The endothelium has however failed to demonstrate such an impermability to water in the rabbit (Mishima & Hedbys 1967) and in the human (Stanley 1972). The fact that the cornea does riot swell in vivo has therefore called for the existence of an active endothelial pump which constantly pumps fluid out of the stroma into the aqueous (Mishima 1968; Maurice 1969, 1972; Hodson & Miller 1976). O n basis of this model, a very leaky endothelium and a large pumping activity, the hydration of the cornea would be expected to increase if the pressure gradient across the endothelium was raised.
In view of the present findings and other reports showing an inverse relationship between IOP and corneal thickness at presumed intact endothelium (Ehlers & Riise 1967; Ehlers 1970; Olson & Kaufman 1978), it seems that if the pump-leak concept for the function of the endothelium is to be maintained it would require the pump to be activated or the leakage to be lowered in response to an increased intraocular pressure as long as the pressure does not damage the endothelium.
Acknowledgments
This study was supported by the Danish Medical Research Council and the Danish Committee for Prevention of Blindness. The technical assistance of Mrs. Anette Poulsen is gratefully acknowledged.
References
Bourne W. M. & Kaufman H . E. (1976) Cataract extraction and the corneal endothelium.
Chandler P. A. & Grant W. M. (1965) Lectures on glaucoma. Philadelphia, p. 166. Lea &
De Cevallos E., Dohlman C. H. & Reinhart W. J. (1976) Corneal thickness in glaucoma. Ann.
Ehlers N . (1970) On corneal thickness and intraocular pressure 11. Actu ophthar! (Kbh.) 48,
Ehlers N. & Riise D. (1967) On corneal thickness and intraocular pressure. Acta ophthal. (Kbh.)
Ehlers N . & Sperling S. (1977) A technical improvement of the Haag-Streit pachometer. Actn
Etienne R. (1969) Les glaucoma. Lyon, p. 353.
Amer. J . Ophtiial. 82, 44-47.
Febiger.
Ophthal. 8, 177 - 182.
1107- 11 12.
45, 809-813.
ophthal. (Kbh.) 55, 333-336.
265

Thomas Olsen
Forstot S. L., Blackwell W. L., Jaffe N. S. & Kaufman H. E. (1977) The effect of intraocular lens implantation on the corneal endothelium. Trans. Amer. Acad. Ophthat. Otolaryng. 83, I95 -203.
Harris J. E., Gersitz L. & Gruber L. (1956) The hydration of the cornea 11. the effect of the
Hodson S. & Miller F. (1976) The bicarbonate ion pump which regulates the hydration of
Irvine A. R. (1956) The role of the endothelium in bullous keratopathy. Arch. Ophthul.
Kaufman H. E., Capella J. A. & Robbins J. E. (1966) The human corneal endothelium. Amer.
Leber T. (1873) Studien Uber den Flussigkeitswechel im Auge. Albert v . Graefe’s Arch. f.
Lowe R. F. (1969) Central corneal thickness, ocular correlations in normal eyes and those with
Maurice D. M. (1969) The cornea and sclera. In: The Eye, Davson H. (ed), vol. 1, pp.
Maurice D. M. (1972) The location of the fluid pump in the cornea. J . Phusiol. 221,43-54. Maurice D. M. & Hoefle F. B. cited in Kaye G. I., Sibley R. C. & Hoefle F. B. (1973) Recent
studies on the nature and function of the corneal endothelial barrier. Exp. Eye Res. 15, 585-613.
Mayes K. R. & Hodson S. (1978) Some effects of hydrostatic pressure on corneal hydration
Mishima S. (1968) Corneal thickness. Sum. Ophthal. 13,57-96. Mishima S. & Hedebys B. 0. (1967) The permeability of the corneal epithelium and
Olsen T. (1979) Non-contact specular microscopy of human corneal endothelium. Acta
Olson R. J. & Kaufman H. E. (1978) Intraocular pressure and corneal thickness after
Rao N. G., Shaw E. L., Arthur E. & Aquavella J. V. (1978) Morphological appearance of the
Sbordone G. (1953) Richerche sullo spessore della cornea in occhi glaucomatosi. Rms. Ottal.
Stanley J. A. (1972) Water permeability of the human cornea. Arch. Ophthal. (Chicago) 87,
Stoker F. W. (1971) The endothelium of the cornea and its clinical implications. ed. 2. Charles
Svedberg B. (1975) Effect of artificial intraocular pressure elevation on the corneal endo-
Ytteborg J. & Dohlman C. H. (1965) Corneal oedema and intraocular pressure I. Animal
Ytteborg J. & Dohlman C . H. (1965a) Corneal oedema and intraocular pressure 11. Clinical
intraocular pressure. Amer. J . Ophthal. 42, 325-329.
rabbit cornea. J . Physiol. 263, 563-577.
(Chicago) 56, 338-351.
J . Ophthal. 61 , 835-841.
Ophthal. 19, 87- 185.
primary angle closure glaucoma. Brit.J. Ophthal. 53 , 824-826.
489-600. Academic Press, London & N. Y .
during specular microscopy. Exp. Eye RPS. 26, 141 - 145.
endothelium to water. Exp. Eye Res. 6, 10-32.
ophthal. (Kbh.) 57, 986-998.
penetrating keratoplasty. Amer. J . Ophthal. 86, 97- 100.
healing corneal endothelium. Arch. Ophthal. (Chicago) 96,2027-2030.
22,262-268.
568-573.
C. Thomas. Springfield Ill.
thelium in the vervet monkey. Acta ophthal. (Kbh.) 53,839-855.
experiments. Arch. Ophthal. (Chicago) 7 4 , 375-381.
results. Arch. Ophthal. (Chicago) 74, 477-484.
Author’s addres.r :
Thomas Olsen, Department of Ophthalmology, Arhus Kommunehospital, DK-8000 Aarhus C, Denmark.
266