the einstein ext study 'xarelto' for the long-term prevention of recurrent venous...
TRANSCRIPT
The EINSTEIN EXT Study
'Xarelto' for the Long-Term Prevention of Recurrent Venous Thromboembolism
Persistent Threat of VTE Recurrence
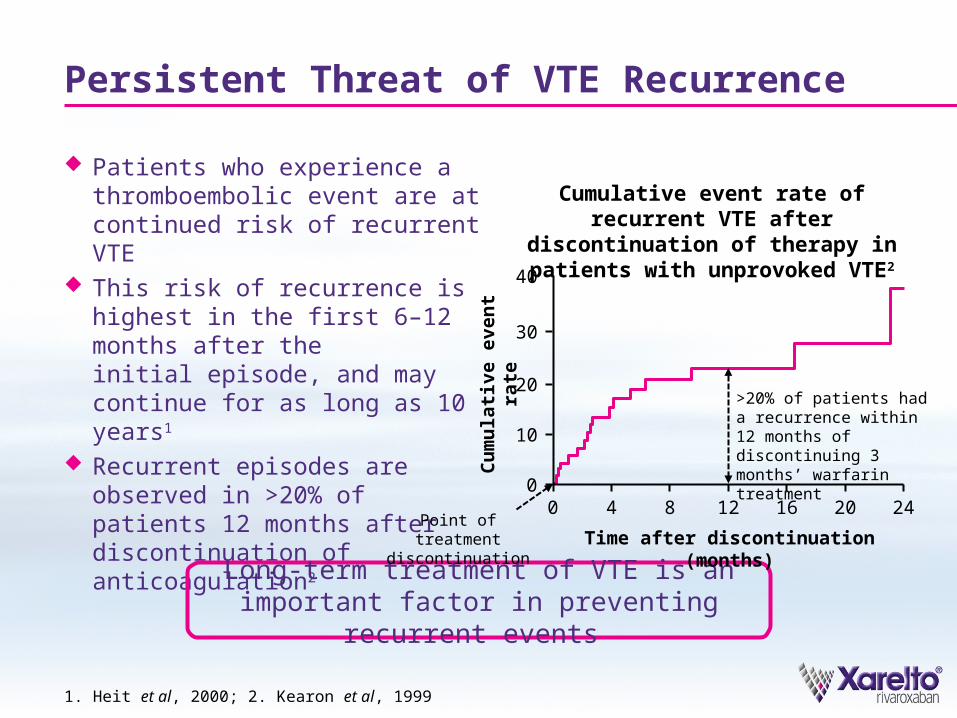
Patients who experience a thromboembolic event are at continued risk of recurrent VTE
This risk of recurrence is highest in the first 6–12 months after the initial episode, and may continue for as long as 10 years1
Recurrent episodes are observed in >20% of patients 12 months after discontinuation of anticoagulation2
Long-term treatment of VTE is an important factor in preventing recurrent events
1. Heit et al, 2000; 2. Kearon et al, 1999
Cumulative event rate of recurrent VTE after discontinuation of therapy in
patients with unprovoked VTE2
Cu
mu
lati
ve e
ven
t ra
te
40
Time after discontinuation (months)
30
20
10
00
4 8 12 16 20 24
>20% of patients had a recurrence within 12 months of discontinuing 3 months’ warfarin treatment
Point of treatment discontinuation
'Xarelto': Simple and Effective Single-Drug Approach for VTE Treatment
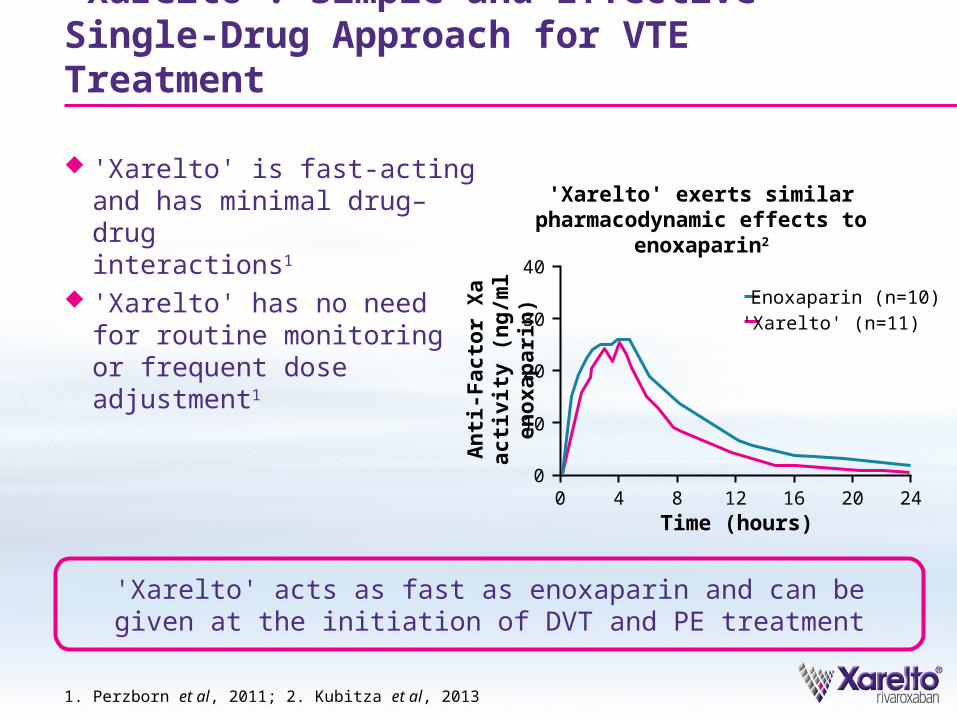
'Xarelto' is fast-acting and has minimal drug–druginteractions1
'Xarelto' has no need for routine monitoring or frequent dose adjustment1
1. Perzborn et al, 2011; 2. Kubitza et al, 2013
'Xarelto' acts as fast as enoxaparin and can be given at the initiation of DVT and PE treatment
'Xarelto' exerts similarpharmacodynamic effects to enoxaparin2
40
30
20
10
00
4 8 12 16 20 24A
nti
-Fac
tor
Xa
acti
vity
(n
g/m
l en
oxa
par
in)
Time (hours)
Enoxaparin (n=10)'Xarelto' (n=11)
The EINSTEIN EXT Study Design
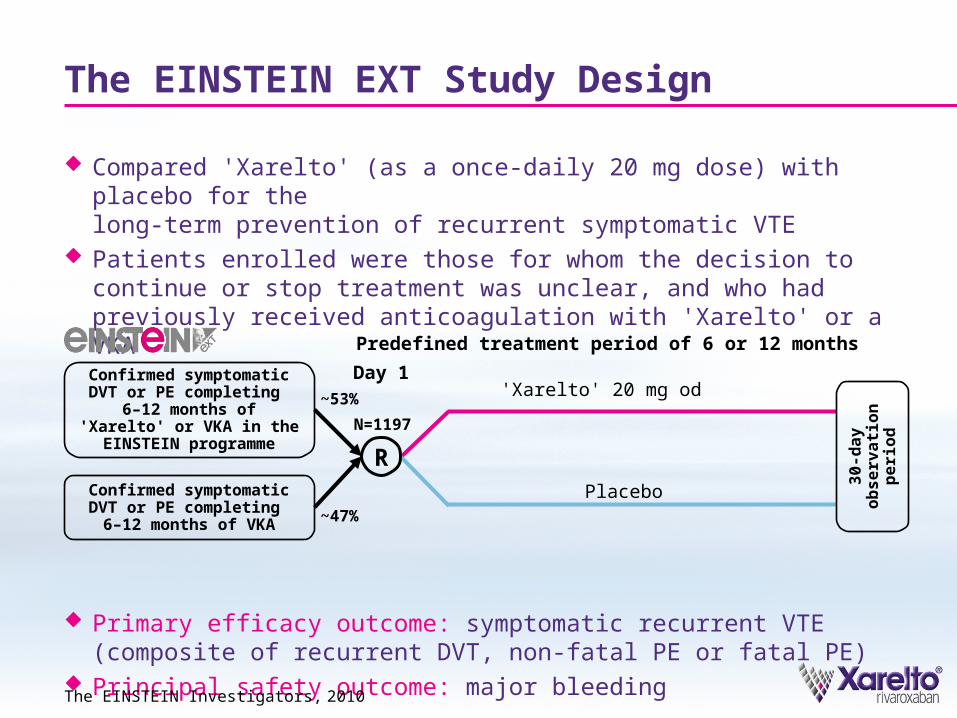
Compared 'Xarelto' (as a once-daily 20 mg dose) with placebo for the long-term prevention of recurrent symptomatic VTE
Patients enrolled were those for whom the decision to continue or stop treatment was unclear, and who had previously received anticoagulation with 'Xarelto' or a VKA
Primary efficacy outcome: symptomatic recurrent VTE (composite of recurrent DVT, non-fatal PE or fatal PE)
Principal safety outcome: major bleeding
The EINSTEIN Investigators, 2010
Confirmed symptomatic DVT or PE completing
6–12 months of 'Xarelto' or VKA in the
EINSTEIN programmeN=1197
Placebo
Predefined treatment period of 6 or 12 months
'Xarelto' 20 mg od
R
30
-da
y
ob
se
rva
tio
n
pe
rio
d
Confirmed symptomatic DVT or PE completing 6–12 months of VKA
~53%
~47%
Day 1
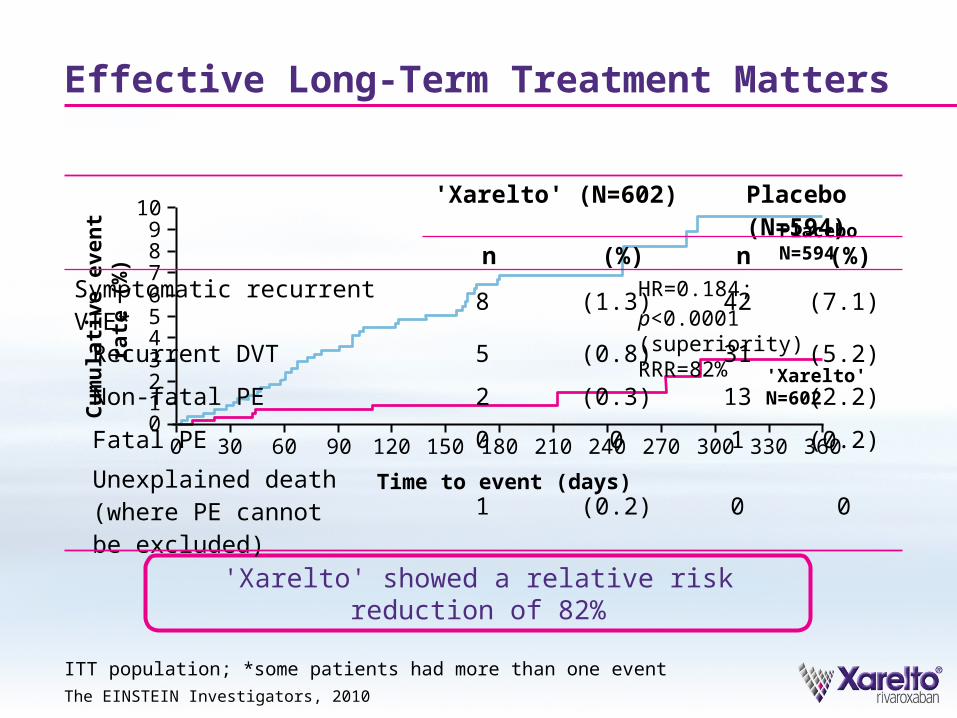
Effective Long-Term Treatment Matters
ITT population; *some patients had more than one event
The EINSTEIN Investigators, 2010
Time to event (days)
10
5
21C
um
ula
tive
eve
nt
rat
e (%
)
34
9
678
00 30 60 90 120 150 180 210 240 270 300 330 360
HR=0.184; p<0.0001 (superiority)RRR=82%
'Xarelto' N=602
PlaceboN=594
'Xarelto' showed a relative risk reduction of 82%
'Xarelto' (N=602) Placebo (N=594)n (%) n (%)
Symptomatic recurrent VTE* 8 (1.3) 42 (7.1)
Recurrent DVT 5 (0.8) 31 (5.2)
Non-fatal PE 2 (0.3) 13 (2.2)
Fatal PE 0 0 1 (0.2)
Unexplained death (where PE cannot be excluded)
1 (0.2) 0 0
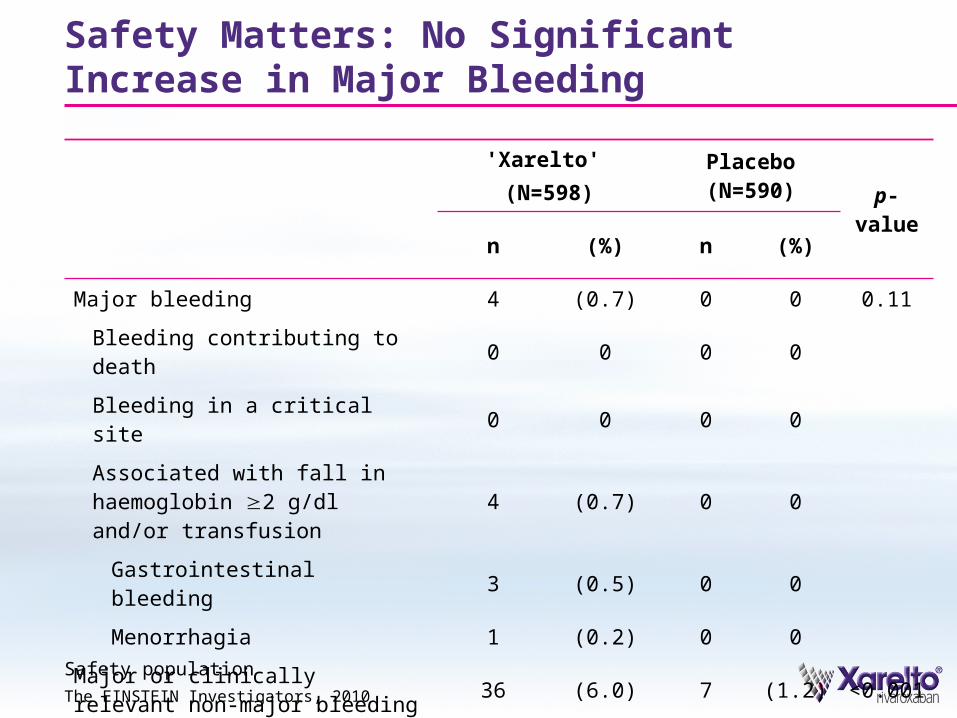
'Xarelto' (N=598)
Placebo (N=590) p-value
n (%) n (%)
Major bleeding 4 (0.7) 0 0 0.11
Bleeding contributing to death 0 0 0 0
Bleeding in a critical site 0 0 0 0
Associated with fall in haemoglobin 2 g/dl and/or transfusion 4 (0.7) 0 0
Gastrointestinal bleeding 3 (0.5) 0 0
Menorrhagia 1 (0.2) 0 0
Major or clinically relevant non-major bleeding 36 (6.0) 7 (1.2) <0.001
Clinically relevant non-major bleeding 32 (5.4) 7 (1.2)
Safety Matters: No Significant Increase in Major Bleeding
Safety population
The EINSTEIN Investigators, 2010
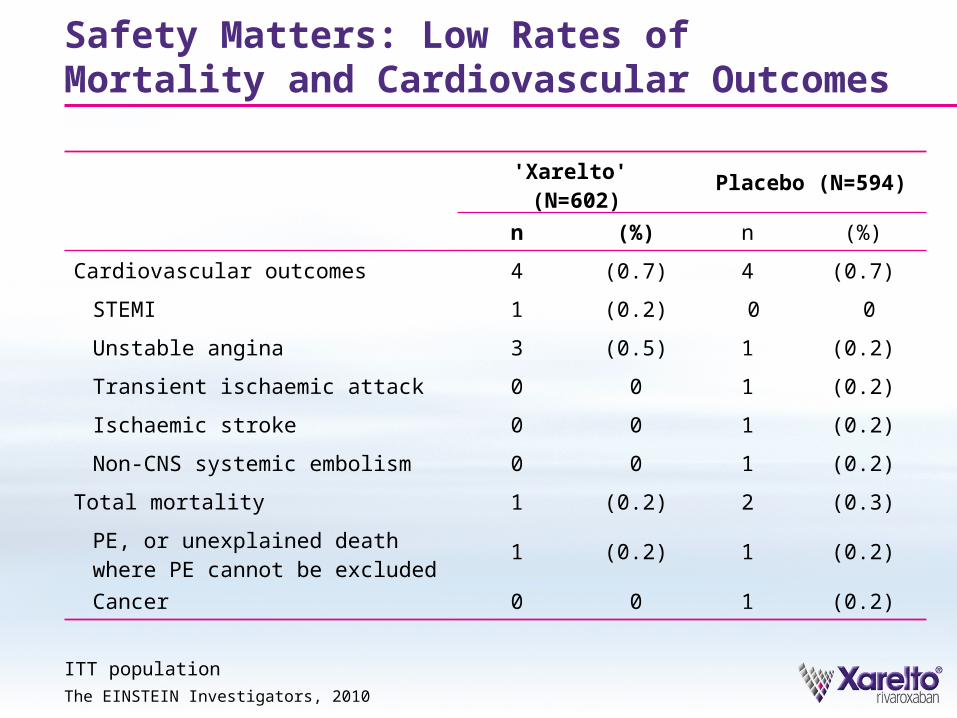
ITT population
'Xarelto' (N=602) Placebo (N=594)
n (%) n (%)
Cardiovascular outcomes 4 (0.7) 4 (0.7)
STEMI 1 (0.2) 0 0
Unstable angina 3 (0.5) 1 (0.2)
Transient ischaemic attack 0 0 1 (0.2)
Ischaemic stroke 0 0 1 (0.2)
Non-CNS systemic embolism 0 0 1 (0.2)
Total mortality 1 (0.2) 2 (0.3)
PE, or unexplained death where PE cannot be excluded 1 (0.2) 1 (0.2)
Cancer 0 0 1 (0.2)
Safety Matters: Low Rates of Mortality and Cardiovascular Outcomes
The EINSTEIN Investigators, 2010
'Xarelto' (N=602), %
Placebo (N=594), % HR (95% CI) p-value
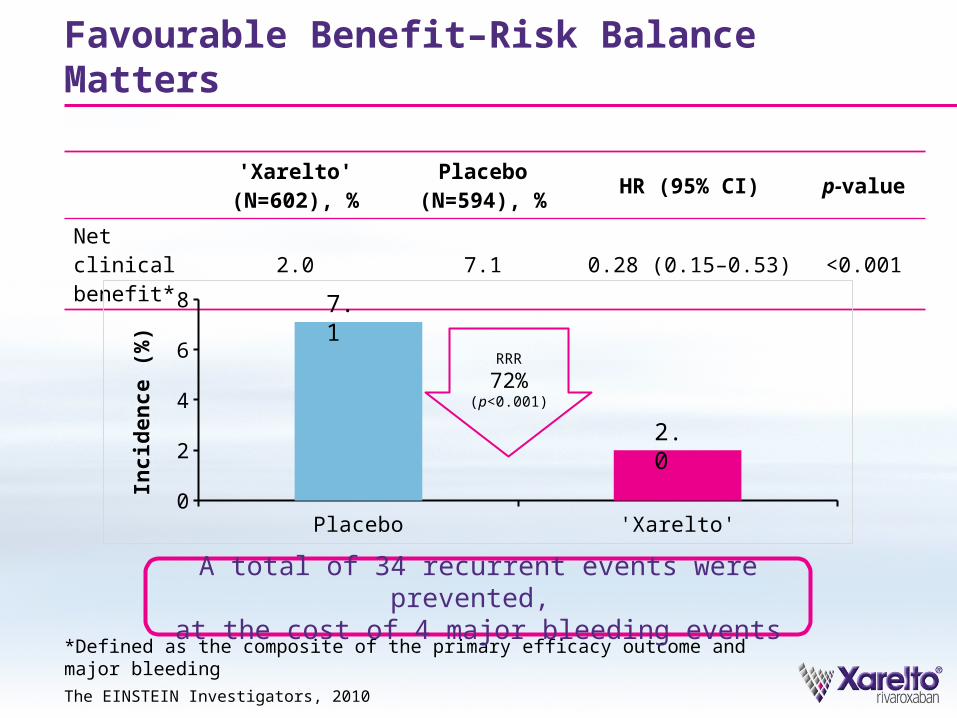
Net clinical benefit* 2.0 7.1 0.28 (0.15–0.53) <0.001
Favourable Benefit–Risk Balance Matters
The EINSTEIN Investigators, 2010
*Defined as the composite of the primary efficacy outcome and major bleeding
A total of 34 recurrent events were prevented, at the cost of 4 major bleeding events
RRR
72%(p<0.001)
Placebo 'Xarelto'0
2
4
6
8
Inc
ide
nc
e (
%)
7.1
2.0
'Xarelto': Simple Sustained Protection from Hospital to Home
EINSTEIN EXT confirmed the benefits of the simple, single-drug approach with 'Xarelto' for long-term treatment of DVT/PE
No significant increase in major bleeding events or vascular events
Significant reductions in recurrent VTE compared with placebo – an 82% relative risk reduction
An acceptable benefit–risk balance for patients receiving long-term treatment in whom there is no clear decision whether to
continue or stop anticoagulation

Pack Shot
BACK-UP SLIDES
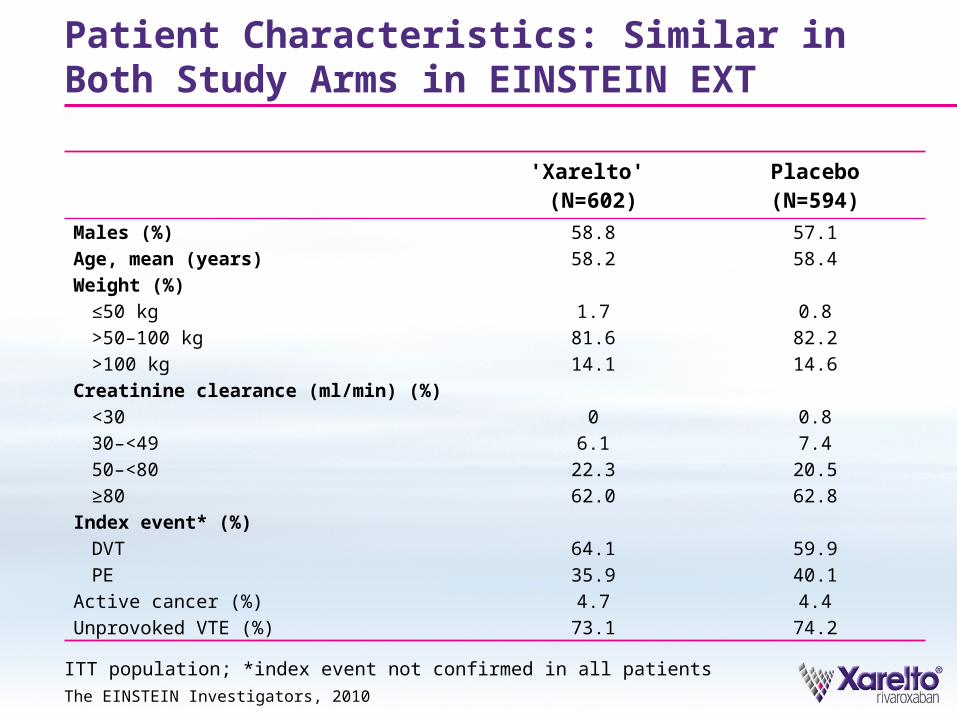
'Xarelto' (N=602)
Placebo(N=594)
Males (%) 58.8 57.1
Age, mean (years) 58.2 58.4
Weight (%)
≤50 kg 1.7 0.8
>50–100 kg 81.6 82.2
>100 kg 14.1 14.6
Creatinine clearance (ml/min) (%)
<30 0 0.8
30–<49 6.1 7.4
50–<80 22.3 20.5
≥80 62.0 62.8
Index event* (%)
DVT 64.1 59.9
PE 35.9 40.1
Active cancer (%) 4.7 4.4
Unprovoked VTE (%) 73.1 74.2
Patient Characteristics: Similar in Both Study Arms in EINSTEIN EXT
The EINSTEIN Investigators, 2010
ITT population; *index event not confirmed in all patients
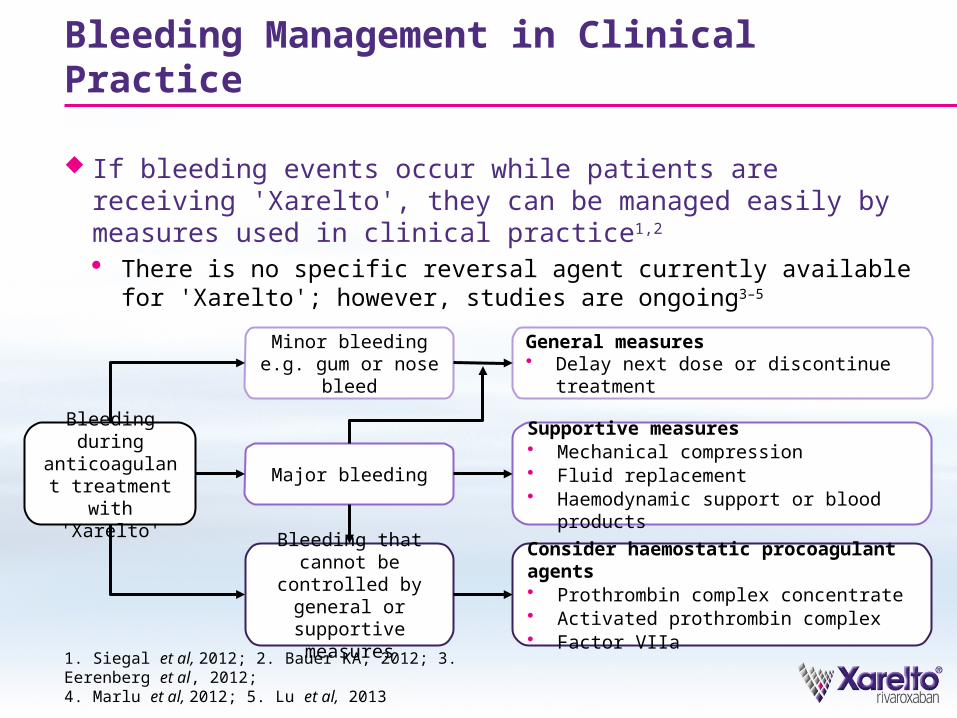
Bleeding Management in Clinical Practice
If bleeding events occur while patients are receiving 'Xarelto', they can be managed easily by measures used in clinical practice1,2
· There is no specific reversal agent currently available for 'Xarelto'; however, studies are ongoing3–5
1. Siegal et al, 2012; 2. Bauer KA, 2012; 3. Eerenberg et al, 2012; 4. Marlu et al, 2012; 5. Lu et al, 2013
Bleeding during anticoagulant treatment with
'Xarelto'
Minor bleeding e.g. gum or nose bleed
Major bleeding
Bleeding that cannot be controlled by
general or supportive measures
General measures Delay next dose or discontinue treatment
Supportive measures Mechanical compression Fluid replacement Haemodynamic support or blood products
Consider haemostatic procoagulant agents Prothrombin complex concentrate Activated prothrombin complex Factor VIIa