the effects of corneal surgery on corneal curvature : an experimental study on rabbits
TRANSCRIPT

T O P R O F E S S O R M A U N O V A N N A S O N T H E O C C A S I O N O F H I S 7 0 T H B I R T H D A Y
From the Department of Ophthalmology, University of Helsinki
(Head: Professor Mauno Vannas, M. D.)
THE EFFECTS OF CORNEAL SURGERY ON CORNEAL CURVATURE
An experimental study on rabbits
BY
ErkRi Tuovinen and Kaisu Viikari
The refractive power of the cornea is over two-thirds that of the eye as a whole. Thus corneal astigmatism is the most serious astigmatism caused by the refract- ing media. Its operative treatment has engaged the attention of many investi- gators, and the results achieved have varied considerably. Surgery of the cornea was employed by Sat0 in 1941 in his attempts to cure first keratoconus and later on astigmatism and myopia. In 1953, Yamamori reported encouraging results in rabbit experiments while Smejkal in 1958, using the same animals had rather poorly positive results. Although some workers (e. g. Fine 1958) mentioned that it is only rarely possible, even through scleral resection, to achieve a change in refraction of more than one or two diopters, Maitani re- ported in 1956 that he had effected considerable changes in the curvature of the cornea by this operation.
MATERIAL A N D METHOD
The purpose of the present work was to produce astigmatism operatively in rabbit cornea. Plastic surgery was performed on the cornea of 46 rabbit eyes by five different methods under Nembutal narcosis. The mean weight of these animals, which comprised the first part of the present material, was 2.8 kg. A feature common to four of these methods was the endeavour to curve the verti- cal meridian of the cornea, in other words to produce direct astigmatism. In the fifth method the intention was the reverse. Javal-Schiotz’s ophthalmometer was used to determine the degree of astigmatism. The readings were recorded according to its dioptric scale. The operative result was examined immediately in a part of the animals, in all of them at intervals of about one to four weeks.
445

The follow-up period was two months. Some cases (Nos. 14, 19, 27, 28, 34, 43 and 44) were followed for four to five months but without observing any note- worthy further change after the first two months.
A. Duplication of the cornea Duplication of the cornea was performed on the first group of 20 eyes. A
curved incision measuring one third of the circle of the cornea was made in the limbus and a flap was made taking in half of the thickness of the cornea (Fig. 1). The flap measured three mm in the middle. The base of this flap was pulled close to the margin of the limbus by means of two mattress sutures. The edge of the flap was fixed by three sutures to the surface of the sclera beneath the conjunctiva. The anterior chamber was not perforated except in one case. The deeper portion of the cornea remaining under the flap fell in a fold into the anterior chamber, from which the method derives its name. The results are shown in Table 1.
As the surgical intervention reduces the volume of the eyeball, it proved very difficult to close the flap since the sutures tended to shear. In one case (No. 15) an endeavour was made to reduce intraocular pressure by paracentesis on the opposite side of the cornea. Eight eyes were examined immediately after sur- gery and it was found that an average of ten diopters of direct astigmatism had been induced. It was still present in eight eyes, mean 7.5 diopters, one week later. No astigmatism at all remained in two eyes, and in five eyes it had changed into inverse astigmatism. The mean astigmatism was 3.5 diopters after a month in a total of nine eyes. Four eyes showed no astigmatism and in one eye it was inverse.
Fig. 1. Corneal duplication operation.
446

Table 1. The degree of astigmatism produced after the corneal duplication operation.
inv. = inverse astigmatism.
Eye No.
1
2
3
4
5
6
7
8
9
10
11
-
~ ~~~
Javal-Schiotz ophthalmometer reading in diopters
before operat.
-43 i" -43 i" -43 i" 41.5
L 4 2 . 5
-44
43.5
L 4 3 . 5
-45.5
-45
-43
-48.5
-47.5
mmediat after
operat.
no examin.
no examin.
no examin.
no examin.
no examin.
no examin.
no examin.
no examin.
no examin.
no examin.
no examin.
Javal-reading unclear
-42
-43.5
39
44
-30
-30
-44 i"
49
L 4 7
-46 i' -41.5 i" -40
-41.5
53
49
L 4 6
-45.5
-40.5
-48 i" 45
L 4 5
447
-41.5 i" 40.5
1 4 0
-42
-43 i" -45
46.5
L 4 5
-43
-52
44
L 4 4
Amount of
stigmat. in
liopters
1.5
1.5
1.5
0
4.5
1.5
1.0 inv.
0
0
Notes
Postoperative corneal leucoma
Panophthalmitis after four weeks
Preoperative inverse astigmatis in the cornea
Preoperative inverse astigmatis in the cornea
Conjunctival flap

Eye No.
12
13
14
15
16
17
18
19
20
Table 1 (cont.).
Javal-Schiotz ophthalmometer reading
before operat.
47.5
L 4 7 . 5
-46
43
1 4 3
-46
-4 7
46.5
L 4 6 . 5
-4 7
45
L 4 5
-42
immediai after
operat.
no examin.
12-13 dii ast.
10-12 dil ast.
1 3 7
12 dir. ast.
10 dir. ast.
8 dir. ast.
9 dir. ast.
8-9 dir. ast.
in diopters
after one
week
-46.5
no examin.
-42
36
L 4 2
-46
vessels in the cornea
after four
weeks
-46
-4 6
no examin.
-44.5
after eight weeks
46
L 4 6
L 4 5
L 4 2
-4 r5 3
45.5
1 4 5
macula corneae
Amouni of
istigmai in
diopters
0
0
0
0.5
0.5
abscessus corn. cum peforatio
-46
-4 1.5
no :xamin.
-4 1.5
-45
-42.5
1.0 inv.
0
Notes
Conjunctival flap
conjunctival flap
conjunctival flap 4- tarsorrhaphy no change after five months
Conjunctival flap + tarsorrhaphy + extirpation of the nictitating mem- brane paracentesis within the opposite area of the cornea
conjunctival flap 4- tarsorrhaphy
conjunctival flap + tarsorrhaphy
Conjunctival flap + tarsorrhaphy
Extirpation of the nictitat. membrane + tarsorrhaphy: after 3.5 months direct astigmatism of two diopters
Extirpation of the nictitat. membrane + conjunctival flap + tarsorrhaphy
448
After two months, seven eyes showed direct astigmatism of 0.5-4.5 diopters. There was an equal number of eyes with no astigmatism, and two with inverse astigmatism. The authors attributed the decrease in the amount of inverse astig- matism to the healing of the corneal wound with a connective tissue scar which, on shrinking, pulled the cornea back to its former curvature. Disturbing corneal opacities developed in a couple of cases (Nos. 1 and 17), but in others there was practically no scar opacity (Fig. 2 is of eye No.20 nine weeks post- operatively).
B. Segment resection of the surface lamellae of the cornea Only a corneal flap like that described in method A was resected from four
eyes. In addition to this, in two eyes, such flaps were resected on the opposite sides of the cornea to weaken it so that intraocular pressure would stretch the cornea in this direction. Table 2 shows that only two eyes (Nos. 21 and 26) dis- played 1.5 and 3.5 diopters of the expected inverse astigmatism after a week, and this too had disappeared two months later.
C . Cautery of opposite pyramidal zones of the cornea In the next four eyes, thermocautery points were made with a needle one mm
in diameter in order to produce corneal astigmatism by means of constricting scars. Fairly deep points were burnt in each eye in two pyramidal zones (Fig. 3). Table 3 shows that immediate post-cautery astigmatism of three-six diopters was demonstrable; within a week, however, it was reduced in the greater part of the cases and in two months had disappeared. The same result was obtained
Fig. 2. Eye No. 20 nine weeks after the duplication operation on the cornea.
449

Table 2. The results of lamellar peripheral segment resection performed on the cornea
(the aim was inverse astigmatism).
50.5
L 5 0 . 5
49 48
L 5 2 . 5 1 4 7 . 5
L
-
Eye No.
25
26
21
22
23
24
51
1-5 1
50.5
L 5 0 . 5
Javal-Schiiitz ophthalmometer reading in diopters
before operat.
48.5
1 4 8 . 5
49
1-49
1-49
1-49
49
49
after one
week
47.5
1-49
48.5
1 4 7 . 5
1 4 7 . 5
47.5
47
1-47
after four
weeks
47
1-48
L 4 7
46
L 4 6
46.5
L 4 6 . 5
after eight weeks
r5 -45.5
L 4 5
15
L 4 5
1-46
46
imount of
stigmat. in
liopters
0
0
0
0
Notes
~
Perforation of anterior conjunctival flap no change after five mths.
Conjunctival flap after five months:
45.5
Conjunctival flap
Conjunctival flap
Two lamellar peripheral segment resections made on the opposite sides of each cornea:
47
-47 I 47
0
1 L 4 7 1 *
Conjunctival flap
Conjunctival flap
Fig. 3. Thermocautery points of opposite pyramidal zones of the cornea.
after electrocautery by Bock (1940) according to whom the radius is restored in a few days and changes lasting longer than two months are exceptional when a needle with a diameter of one mm is used.
450
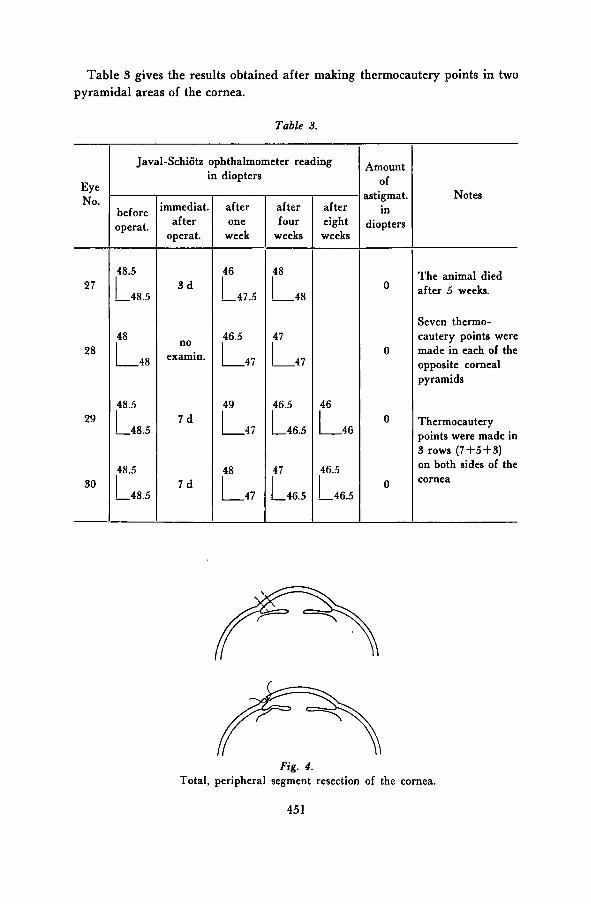
Table 3 gives the results obtained af te r making thermocautery points in two pyramidal areas of the cornea.
Table 3.
Eye No.
27
28
29
30
Javal-Schiotz ophthalmometer reading in diopters
before operat.
-48.5 r '" L 4 8
-48.5
-48.5
mmediat after
operat.
3 d
no examin.
7 d
7 d
after one
week
-47.5 r r 4 7
L 4 7
-47 r
after four
weeks
-48 i" -4 7
46.5
L 4 6 . 5
-46.5
after eight weeks
L 4 6
r:6.5
4mount of
.stigmat. in
iiopters
Notes
The animal died after 5 weeks.
Seven thermo- cautery points were made in each of the opposite corneal pyramids
Thermocautery points were made in 3 rows (7+5+3) on both sides of the cornea
Fig. 4. Total, peripheral segment resection of the cornea.
45 1

Table 4. The degree of astigmatism produced after total resection of the peripheral segment of
the cornea. inv. = inverse astigmatism.
Eye No.
3 1
32
33
34
35
36
37
38
39
40
Javal-Schjotz ophthalmometer reading in diopters
before operat.
43
L I P . !
1 4 3
L 4 3
L 4 3 . 5
43
42
L 4 2
43
43.5
42.5
-42.5
44
-44
44
-4.1
16
-48
42
-42
immedial after
operat.
no examin.
no examin.
no examin.
no examin.
no examin.
no examin.
no examin.
no examin.
no examin.
no examin.
after one
week
-45
-46
-43
L 4 3
-45 i""
L 4 7
42
1 4 6 . 5
42
L 4 6 . 5
L 4 1
-39
after four
weeks
-44 r5 42.5
1 4 6 . 5
41.5
L 4 2 . 5
L 4 3
L 4 6
41.5
-45.5
42
-4 7
43
-45
49
-43
11
-43
after eight weeks
42.5
L 4 4
L 4 7
i k 4 2
-45 I"
40
L 4 1 . 5
40
1 4 4
40
1-46
42
L 4 5
I"' -44.5
42.5
-42
Amounf of
astigmaf in
diopters
2 inv.
5 inv.
1.5 inv.
1 .o
4 inv.
4 inv.
6 inv.
3 inv.
9.5
0.5
Notes
vascularised scar p in the cornea
fiite, thick scar up I the cornea. he pupil drawn ?wards
he wound opened 'ter a week. fter four 41 onths
L4 6
-44.5 onths
reoperatively verse astigmatism ro diopters id hypotonic .taract eye
452

Table 4 (cont.).
before operat.
-
Eye No. immediat. after
after one operat. week
41
42
8 dir. ast.
12 dir. ast.
Javal-Schiotz ophthalmometer reading in diopters
no examin.
no examin.
-44 i' 42
L 4 2
after four
weeks
-46 r 45.5
L 4 1 . 5
after eight weeks
42.5
L 4 4 . 5
r 1 2 . 5
Amount of
istigmat. in
diopters
2 inv.
4
Notes
Extirpation of the nictitating mem- brane + conjunc- tival flap
Extirpation of the nictitating mem- brane + conjunct. flap + tarsorrhaphy. A broad scar remains in the upper part
D. Total peripheral segment reseclion of the cornea Total resection of the peripheral segment of the cornea was performed on a
total of 12 eyes. (Fig. 4). A perforating incision for one third of the circle was made with a cataract knife in the limbus and a two mm wide semilunar piece was resected from the edge with scissors. The margins of the wound thus formed were drawn together by three to five sutures. The results are shown in Table 4.
The difficulty in this method was to prevent prolapse of the base of the iris. When closing the wound the iris was held out of the way with a spatula. The primary outcome was examined in two cases only and it revealed astigmatism of eight and 11 diopters. The astigmatism was reversed within a week, averag- ing four diopters inverse. After two months, inverse astigmatism averaging 4.5 diopters was established in eight eyes and direct astigmatism of the same degree in four eyes. The high incidence of inverse astigmatism within a week of the operation was due to the primary opening of the wound and its secondary closure with connective tissue. Fig. 5, a photograph of eye No. 42 taken nine weeks postoperatively, shows the lower margin of the cicatricial area and the intact centre of the cornea.
E. Segment resection of the deep layers of the cornea Lamellar segment resection of the deep layers of the cornea was another
operation performed. It was made on four eyes (Fig. 6). A two to three mm
453 Acta Ophthalmol. Vol. 59, 111 ? I
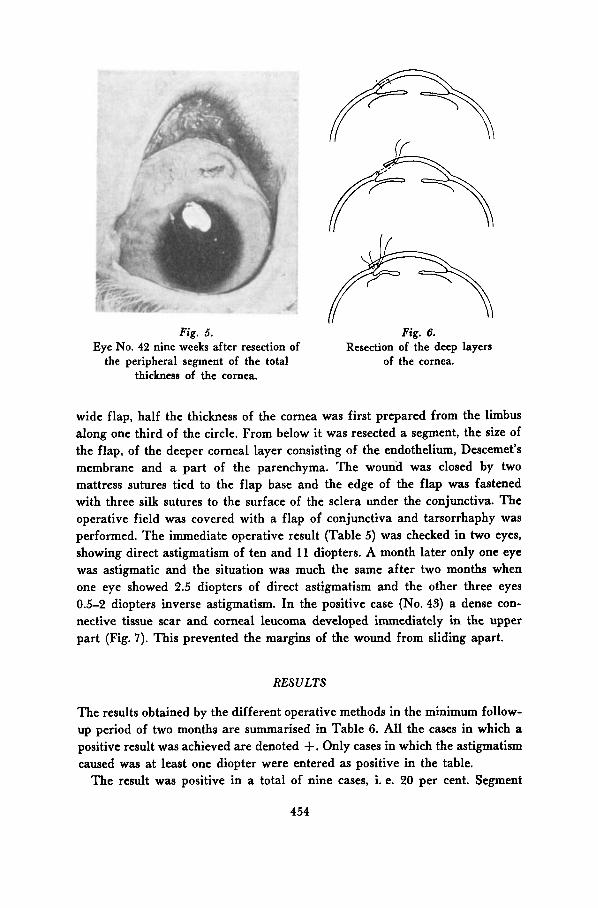
Fig. 5. Fig. 6. Eye No. 42 nine weeks after resection of
the peripheral segment of the total thickness of the cornea.
Resection of the deep layers of the cornea.
wide flap, half the thickness of the cornea was first prepared from the limbus along one third of the circle. From below it was resected a segment, the size of the flap, of the deeper corneal layer consisting of the endothelium, Descemet’s membrane and a part of the parenchyma. The wound was closed by two mattress sutures tied to the flap base and the edge of the flap was fastened with three silk sutures to the surface of the sclera under the conjunctiva. The operative field was covered with a flap of conjunctiva and tarsorrhaphy was performed. The immediate operative result (Table 5) was checked in two eyes, showing direct astigmatism of ten and 11 diopters. A month later only one eye was astigmatic and the situation was much the same after two months when one eye showed 2.5 diopters of direct astigmatism and the other three eyes 0.5-2 diopters inverse astigmatism. In the positive case (No. 43) a dense con- nective tissue scar and corneal leucoma developed immediately in the upper part (Fig. 7). This prevented the margins of the wound from sliding apart.
RESULTS
The results obtained by the different operative methods in the minimum follow- up period of two months are summarised in Table 6. All the cases in which a positive result was achieved are denoted +. Only cases in which the astigmatism caused was at least one diopter were entered as positive in the table.
The result was positive in a total of nine cases, i. e. 20 per cent. Segment
454

Table 5 . The degree of astigmatism produced after deep (Descemet's membrane + I/z of the parenchyma) lamellar segment resection of the cornea. inv. = inverse astigmatism.
after one
week
Eye No. after
four weeks
43
44
45
46
L 5 0
43
Javal-Schiotz ophthalmometer reading in diopters
L 4 3
45
before operat.
L 5 . 5
r5 -46.5
46
-46 I
45
1-45 2xamin. no
mmediat after
operat.
11 dir. ast.
no examin.
no examin.
10 dir. ast. L 4 6
after eight weeks
iT43 L3
i"" -45.5
46
L46.5
Amount of
.stigmat. in
iiopters
2.5
2 inv.
0.5 inv.
2 inv.
Notes
Penicillin 100,000 I. u. Corneal leucoma in the upper part After four months direct astigmatism four diopters
No astigmatism left after nix months
Extirpation of the nictitating membrane
Extirpation of the nictitating membrane
Fig. 7. Eye No. 43 four months after lamellar segment resection (deep lamellae).
455
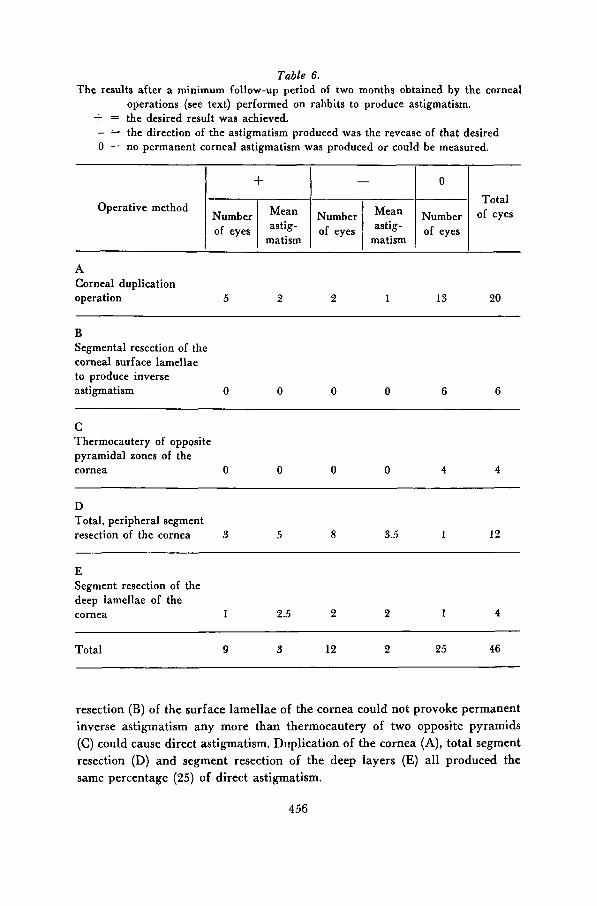
Table 6. The results after a minimum follow-up period of two months obtained by the corneal
operations (see text) performed on rabbits to produce astigmatism. + = the desired result was achieved. - - - the direction of the astigmatism produced was the revease of that desired 0 = no permanent corneal astigmatism was produced or could be measured.
+ Operative method Number Mean
of eyes astig- matism
Total
of eyes matism ,
-
Number Mean
of eyes astig-
A Corneal duplication operation 5 2 2 1 13 20
B Segmental resection of the corneal surface lamellae to produce inverse astigmatism 0 0 0 0 6 6
C Thermocautery of opposite pyramidal zones of the cornea 0 0 0 0 4 4
D Total, peripheral segment resection of the cornea 3 5 8 3.5 1 12
E Segment resection of the deep lamellae of the cornea 1 2.5 2 2 1 4
Total 9 3 12 2 25 46
resection (B) of the surface lamellae of the cornea could not provoke permanent inverse astigmatism a n y more than thermocautery of two opposite pyramids (C) could cause direct astigmatism. Duplication of the cornea (A), total segment resection (D) a n d segment resection of the deep layers (E) all produced the same percentage (25) of direct astigmatism.
456
The operative field was covered with a conjunctival flap in 18 cases. Palpe- bra1 suturing was performed in eight eyes and the nictitating membrane was removed from seven eyes. These measures did not affect the final result in any way.
The sutures were removed a t the earliest a week postoperatively. The suture material was 0000-00000 silk and thin catgut in some of the cases and colla- genous fibres of rat tail in the other cases (Vannas et Larmi 1959). A drawback of silk was the ease with which it tended to cut through the tissue during constant tension. In the majority of the cases catgut caused irritation, swelling and an opacity in the cornea. although only transiently. The least irritating material was biological rat tail suture, although there was no significant dif- ference in the results obtained.
The eyes tolerated the operations fairly well. Only two fatal postoperative infections occurred (Nos. 2 and 18) although Irgamid ointment (Geigy) applied locally at the end of the operation was the only drug therapy given - except for two rabbits which received penicillin injections.
DISCUSSION
A common feature of all the operative methods except group B was that they reduced the volume of the eyeball. In this respect there is a great resemblance to scleral resection. Changes in refraction produced by the various modifications of scleral resection, especially in myopic persons, have been reported by Holth (191 1) and since then by e. g. Gronholm in 1922, Salgado in 1956 and Vannas in 1958.
The inverse astigmatisms of the present material were produced chiefly by tha methods (D and E) in which the anterior chamber of the eye was per- forated. This was because diastase tended to develop within a few days of surgery, the sutures stretching or shearing and the wound healing subsequently with a connective tissue scar. In about half of the cases the cornea reassumed its preoperative regular curvature.
Additional tests were performed to find out whether, in addition to the elasticity of the tissues, intraocular pressure or other factors played a role in this.
Posterior sclerotomies were performed on 13 eyes under retrobulbar anesthe- sia (1.5 ml of two per cent novocain) which made the eyeballs hypotonic. Lamellar corneal duplication (A, Fig. 1) was made in nine of these eyes in the manner described above, however, so that surfaces of the corneal flap and the opposing scleral areas were coagulated in order to prevent sliding, observing the same principle as was reported by Vannas in 1958 in connection with scleral duplication. Total resection of the peripheral segment (D) was made
457

from 4 eyes. All the rabbits were given Diamox because of the reducing effect of this inhibitor of carbonic acid anhydrase on intraocular pressure in rabbit (e. g. Gloster and Perkins, 1955). The pressure was followed by Schiotz’s tono- meter. Although it remained normal or subnormal (10-25 mm Hg) throughout the observation period of nearly a month, the astigmatism, which was initially 12 diopters on an average, and the number of positive cases were reduced to less than half.
In volumetric studies of animals in 1949 Scheie and Jerome noted that the eyeball stretched to its former volume e. g. after scleral resection. The same conclusion was reached in 1956 by Everett from microscopical studies of dogs. As the effect of intraocular pressure as a factor impairing the results was con- sidered to be eliminated, the present authors’ attention was attracted by the role of the vitreous, mentioned also by Everett. The maximum operative result was achieved by total resection of the peripheral segment of the cornea (D) in eye No. 39; it had direct astigmatism of 9.5 diopters two months later. This eye had been used several months earlier for transplantation of the vitreous. It had shown preoperatively an inverse astigmatism of two diopters and a traumatic, posteriorly displaced cataract. No inflammatory symptoms were noted. The phthisic nature of the eye was illustrated by the fact that the radius of curvature of the fully clear cornea was 0.8 mm shorter than that of the other, healthy eye of the same rabbit (No. 40) in which the same operation produced only 0.5 diopters of astigmatism. The degenerated, possibly fluid vitreous of such an eye cannot offer equal resistance to changes in the volume of the eyeball as the gelatinous vitreous of normal consistency in all the other, healthy eyes of our material. This might explain the great variations reported (e. g. Salgado) in the effects of scleral shortening operations on the refractive power of the eyes even when they are performed by the same surgeon and using the same method. A better result may perhaps be expected in cases of degenera- tion of the vitreous and myopias of higher degree (detachment of vitreous) than in eyes with vitreous of normal consistency.
SUMMARY
In order to produce corneal astigmatism, plastic corneal operations were per- formed on 46 rabbit eyes as follows: (A) corneal duplication on 20 eyes; (B) segment resection of the corneal surface lamellae on six eyes to produce inverse astigmatism; (C) thermocautery of two opposite pyramids of the cornea on four eyes; (D) total, peripheral segment resection of the cornea on 12 eyes, and (E) peripheral segment resection of the deep lamellae (Descemet’s membrane + 1/s of the parenchyma) of the cornea on four eyes.
The cases examined immediately after the operation had a mean astigmatism
458
of nine diopters. Taking one diopter as the minimum degree to be termed astigmatism, nine eyes showed after the follow-up period of two months an average astigmatism of three diopters of the desired direction and 12 eyes an average inverse astigmatism of two diopters. The primary astigmatism had disappeared in the remaining 25 eyes (54 per cent). No permanent astigmatism at all was caused in groups B and C. It was produced in the desired direction in a fourth of the eyes of the other groups. With the exception of group B, the operative methods used reduced the volume of the eyeball. With the methods (D and E) involving perforation of the cornea the incidence of inverse astigma- tism was considerably higher than with the other methods, but no other com- plications occurred. Postoperative leucomas did not extend to the optic area.
To eliminate a possible elevation of the intraocular pressure, posterior sclerotomies were also performed on 12 eyes. In nine of these cases it was followed immediately by duplication of the cornea (A) and in four by total peripheral segment resection of the cornea (D). The pressure was followed by a Schiotz tonometer. Although the pressure kept within normal limits (10-25 mm Hg), the number of positive cases and the immediate postoperative mean astigmatism of 12 diopters were reduced to less than half within one month. Maximum astigmatism after two months, 9.5 diopters, was produced in a pre- viously traumatised, slightly phthisic cataract eye. It is suggested that besides the elasticity of the tissues of the wall of the bulbus oculi, the nature of the vitreous might also be of significance for the achievement of a permanent result in operations changing the shape and reducing the volume of the eyeball.
REFERENCES
1. Bock, J.: Deutsche Ophth. Gesell. 1940: 53: 278. 2. Everett, W. G.: Am. J. Ophth. 1956: 42: part 11: 95. 3. Fine, M.: Tr. Pacific Coast Oto-Ophth. SOC. 1958 p. 292. 4. Gloster, J. and Perkins, E. S.: Brit. J. Ophth. 1955: 39: 647. 5. Gronholm, V.: Archiv f. Ophth. 1922: 107: 489. 6. Holth, S.: Bericht d. Ophthalm. Gesellsch. in Heidelberg 1911 s. 293-315. 7. Maitani, M.: Acta SOC. Ophth. Jap. 1956: 60: 1168. Ref. AMA. Arch. Ophth. 1959:
8. Salgado. G . E.: Ann. d'Ocul. 1956: 189: 217. 9. Sato, T.: Am. J. Ophth. 1950: 33: 943.
10. Sato, T.: Klin. Mbl. f. Augenheilk. 1941: 107: 234. 11. Sato, T.: Am. J. Ophth. 1953: 36: 464. 12. Scheie, H . G . and Jerome, B.: Am. J. Ophth. 1949: 32: 60, part 11. 13. Smejkal. V.: Ophthalmologica 1958: 3: 135: 211. 14. Vannas, M.: Acta Ophth. 1958: 36: 432. 15. Vannas, S. and Larmi, T.: Acta Ophth. 1959: 37: 371. 16. Yamamori, A.: Acta SOC. Ophth. Jap. 1953: 57: 1332.Ref. Ophth. Lit. 1953: 7: 2139.
61: 325.
459