the effect of medication management training on community mental health nurse's clinical skills
TRANSCRIPT

International Journal of Nursing Studies 40 (2003) 163–169
The effect of medication management training on communitymental health nurse’s clinical skills
Richard Gray*, Til Wykes, Kevin Gournay
Health Services Research Department, Institute of Psychiatry, De Crespigny Park, London SE5 8AF, UK
Received 20 May 2002; accepted 3 July 2002
Abstract
Background. There is evidence that compliance therapy improves treatment adherence and clinical outcomes in
patients with schizophrenia. Community Mental Health Nurses (CMHNs) are ideally placed to deliver compliance
therapy but require training to develop the necessary clinical skills.
Aim. To explore whether a brief medication management training package is effective in developing the compliance
therapy skills of CMHNs.
Method. The study had a within subjects repeated measures design. A representative sample of 52 CMHNs entered
the study. They performed a role-play task pre- and post-training that was videotaped and blind rated by an
independent rater using the Cognitive Therapy Scale (CTS). Knowledge was assessed pre- and post-training using a
knowledge about medication management questionnaire. Trainees also completed a satisfaction with training
questionnaire at the end of the course.
Results. Following training there was a statistically significant improvement in mean scores on the primary measure
of skills, the CTS (mean pre-training CTS-total score 13.88, mean post-training CTS-total score 31.12; po0:01). Therewas also a significant categorical improvement in the number of trainees who demonstrated satisfactory skills.
Knowledge about medication management was significantly improved and trainees reported that training was
acceptable and relevant to their clinical practice.
Conclusions. In this uncontrolled study training improved the medication management skills of CMHNs.
r 2002 Elsevier Science Ltd. All rights reserved.
Keywords: Medication management; Compliance therapy; Training; Clinical skills
1. Background
Antipsychotic medication is the mainstay in the
effective treatment of schizophrenia reducing symptoms
and, when used as maintenance treatment, preventing
relapse (Davis and Andriukaitis, 1986). However,
translation of this success into clinical practice is
attenuated by poor compliance (Weiden and Olfson,
1995), reasons for which include beliefs about treatment,
insight, and side effects (Buchanan, 1992). A recent
systematic review of interventions to improve adherence
to prescribed medication identified that compliance
therapy (Kemp et al., 1998, 1996) is an intervention
where there is evidence of efficacy in enhancing
adherence with antipsychotic medication (Haynes et al.,
2002). In the UK the National Service Framework for
mental health has recommended that mental health
practitioners use compliance therapy to address the
problem of non-compliance with antipsychotic medica-
tion (DoH, 1999).
Compliance therapy is an intervention based on
cognitive behavioural therapy and motivational inter-
viewing. The key principles of compliance therapy are
working collaboratively with patients, emphasising
personal choice and responsibility and addressing*Corresponding author. Tel.: +44-20-7848-0139.
E-mail address: [email protected] (R. Gray).
0020-7489/03/$ - see front matter r 2002 Elsevier Science Ltd. All rights reserved.
PII: S 0 0 2 0 - 7 4 8 9 ( 0 2 ) 0 0 0 4 5 - 7

patients concerns about treatment. Compliance therapy
is divided into three phases: reviewing the patients’
illness history, discussing common concerns about
treatment, and long term prevention and relapse (Kemp
et al., 1996). The intervention was evaluated in a rando-
mised controlled trial (Kemp et al., 1998, 1996).
Seventy-four psychotic inpatients were randomly as-
signed to receive either compliance therapy or non-
specific counselling. Patients received 4–6 sessions with a
research psychiatrist lasting, on average, 40min and
were assessed at baseline, post-treatment and 3, 6, 12,
and 18 month follow-up, using a battery of standardised
measures, including an observer rated measure of
compliance. Although an assessor blind to the treatment
condition performed the latter assessments the person
conducting the therapy undertook the initial interviews.
Treatment adherence was significantly better in the
compliance therapy group and was sustained through
follow-up. Unexpectedly, there was no significant
difference in psychopathology between the groups.
However, the improvements in compliance did result
in enhanced community tenure, with patients in the
compliance therapy group taking longer to relapse than
those who received non-specific counselling.
In the UK mental health nurses provide much of the
care that patients receive. If the potential benefits to
patient’s and services of compliance therapy are to be
realised then mental health nurses will need to deliver
the intervention. A recent survey of 250 Community
Mental Health Nurses (CMHNs) working in the UK
reported that they feel that improving and maintaining
compliance with treatment is an important part of their
role but report that they require more training in the
area (Gray et al., 2001). Training may be an effective
way of developing CMHNs clinical skills to enable them
to deliver compliance therapy in routine clinical
practice.
It is tempting to assume that training will improve
clinical skills and move to undertake an expensive and
time consuming trial evaluating the impact of training
on clinical outcomes. Several studies have shown that
psychosocial intervention training can potentially
improve clinical outcomes (Lancashire et al., 1997;
Brooker et al., 1994). However, there has been surpris-
ingly little research examining the impact of psychoso-
cial intervention training on skills acquisition probably
because it is so difficult to do in a reliable and replicable
way. Brooker and Butterworth (1993) showed that at the
end of family work training nurses were able to
demonstrate competent clinical skills as measured using
the Cognitive Therapy Scale (CTS; Vallis et al., 1986).
However, no baseline scores are reported making it
difficult to attribute skill acquisition to training. There is
a need to explore, as a first step, if targeted training is an
effective way of developing CMHNs compliance therapy
skills. If skills are enhanced following training further
investigation into the impact of training on clinical
outcomes is warranted.
2. Methods
The aim of this study is to explore whether medication
management training is effective in improving the
clinical skills of CMHNs.
2.1. Community mental health nurses
Sixty CMHNs were recruited from two large mental
health care providers in London, England during 1998
and 1999. They were accepted into the study if they were
registered nurses and had at least 12 months post-
registration experience.
2.2. Study design
The study had a within subjects repeated measures
design. A 10-min standardised role-play task derived
from the method described by Scott et al. (1999),
focusing on a patient’s specific problem with antipsy-
chotic medication, was performed pre- and post-train-
ing. An experienced third party ‘actor’ role-played the
patient. These were videotaped and blind rated, in a
random order, by a trained cognitive therapist, who was
not involved in the study, using the CTS (Vallis et al.,
1986). A multiple-choice knowledge about medication
management test was administered pre- and post-
training and a satisfaction with training questionnaire
was completed at the end of course.
2.3. Training
A medication management course curriculum was
developed by an experienced multi-disciplinary group of
clinicians, academics and service users. The aim of
training was to provide CMHNs with the skills that they
needed to deliver compliance therapy. Medication
management training consisted of 10 days of teaching
delivered to small groups of 10 nurses on a day release
basis over 10 weeks (a total of 80 h contact time).
Training was funded by local mental health services. The
four key components of the training were assessment,
cognitive and compliance therapy skills, psychopharma-
cology, and clinical supervision. A multi-disciplinary
team, including a combination of academic, clinical staff
and service users provided teaching.
In the first component of the course, trainees were
taught to use a battery of valid and reliable assessment
tools to evaluate treatment with antipsychotic medica-
tion and derive a formulation of the patient’s problems
and/or concerns about their treatment. The formulation
was used to guide the selection of targeted compliance
R. Gray et al. / International Journal of Nursing Studies 40 (2003) 163–169164

therapy techniques. Measures were selected based on the
following criteria:
* validity and reliability,* availability,* ease of use, and* acceptability to patients and clinicians.
The main measures taught were the Hogan Drug
Attitude Inventory (DAI-30; Hogan et al., 1983) the
Insight Scale for Psychosis (IP; Birchwood et al., 1994)
and the Liverpool University Neuroleptic Side Effect
Rating Scale (LUNSERS; Day et al., 1995).
The second component of the course focused on
developing trainees’ skills in using compliance therapy
techniques to enhance adherence. To facilitate teaching,
discrete clinical interventions were described (for exam-
ple, reviewing the patients illness history, examining
beliefs about treatment and exploring ambivalence).
Video role-play was used to allow trainees to rehearse
each discrete intervention, critique their own practice
and receive balanced feedback from other members of
the group (Gask, 1999).
Psychopharmacology formed the third component of
the course providing a comprehensive overview of drug
treatments in schizophrenia. The South London and
Maudsley NHS Trust Prescribing Guidelines (Taylor
et al., 2001) were used as a basis for teaching and to
provide trainees with evidential clinical practice guide-
lines. These were selected as they are the most widely
used and internationally recognised set of guidelines for
the treatment of mental health problems. Teaching,
using the guidelines as a template, focused on effective
treatment strategies, the management of antipsychotic
side effects, and the treatment of refractory illnesses.
Regular, weekly, clinical supervision formed a final
critical component of the course integrating skills learnt
in the classroom into clinical practice. Each trainee
presented a patient they were working with, concluding
the presentation by suggesting a supervision question for
discussion within the group. Following the discussion,
an action plan was agreed. Progress on the implementa-
tion of the action plan was monitored during the course.
2.4. Outcome measures
2.4.1. Primary outcome measure: cognitive therapy scale
(Vallis et al., 1986)
The CTS is extensively used internationally and is a
valid and reliable 10-item measure of clinicians’ general
and specific clinical skills. Each of the items—agenda
setting, feedback, understanding, interpersonal effec-
tiveness, collaboration, pacing and efficient use of time,
guided discovery, strategy for change, application of
specific compliance therapy techniques and an overall
clinician rating—were rated on a seven-point scale
ranging from poor (0) to excellent (6) producing a total
score of between 0 and 60. A satisfactory score for each
item is defined as 3, and for the total as 30. Each item
has four anchor points to facilitate rating.
2.4.2. Secondary outcomes measures
Two other measures were developed for this study
to assess the outcome of training. A knowledge about
medication management questionnaire (KAMMQ),
and a satisfaction with training questionnaire. It would
have been preferable to identify valid and reliable
measures from the literature but no appropriate
measures are available. The KAMMQ is a 16-item
multiple-choice questionnaire reflecting the medication
management course curriculum and recent develop-
ments in psychopharmacology, including the introduc-
tion of new drugs. Nurses are presented with 16
questions that relate to case vignettes with five possible
responses, of which only one is correct. The question-
naire produces a total score ranging from 0 to 16. The
questionnaire was designed to have content validity by
including questions on key aspects of medication
management taught within the course. To test this a
Consultant Psychiatrist and a Clinical Pharmacist
completed the questionnaire and were able to get
100% of the questions correct. Test re-test reliability
was established by correlating time one and time two
scores on the KAMMQ in a group of 10 mental health
nurses not associated with the project. A statistically
significant association was found (po0:05).The satisfaction with training questionnaire asked
nurses to rate how satisfied they had been with the
content of the course and the quality of the teaching.
They also rated how relevant the course was to their
clinical practice and if they were able to incorporate the
skills that they had learnt into their work with patients.
2.4.3. Nurse information
Nurses completed a brief questionnaire prior to
training detailing their age, gender, clinical and aca-
demic experience, grade and caseload. The trainer
throughout the course monitored attendance.
2.5. Statistical analysis
To identify within-group differences post-training the
t-test was used. Two-tailed tests were used as the most
conservative method of analysis even when the compar-
isons were supported by a specific hypothesis. The
McNmear test was used to test for changes in the
proportion of nurses achieving a satisfactory standard
on the CTS (items and total) following training.
Exploratory stepwise linear regression was used to
identify factors predictive of trainees’ knowledge and
skill following training (Kirkwood, 1998, p. 57–72).
R. Gray et al. / International Journal of Nursing Studies 40 (2003) 163–169 165
3. Results
3.1. Community mental health nurses
Fifty-two nurses entered the study and received
training: complete data are reported for 81% of the
sample. The demographic profile of the nurses who
entered the study was representative of mental nurses
currently working in the community in England and
Wales (Table 1; Brooker and White, 1997).
3.2. Withdrawals
All of the nurses who started training completed the
course. Average attendance was 8 out of 10 days (80%;
range 60–100%).
3.3. Primary training outcomes
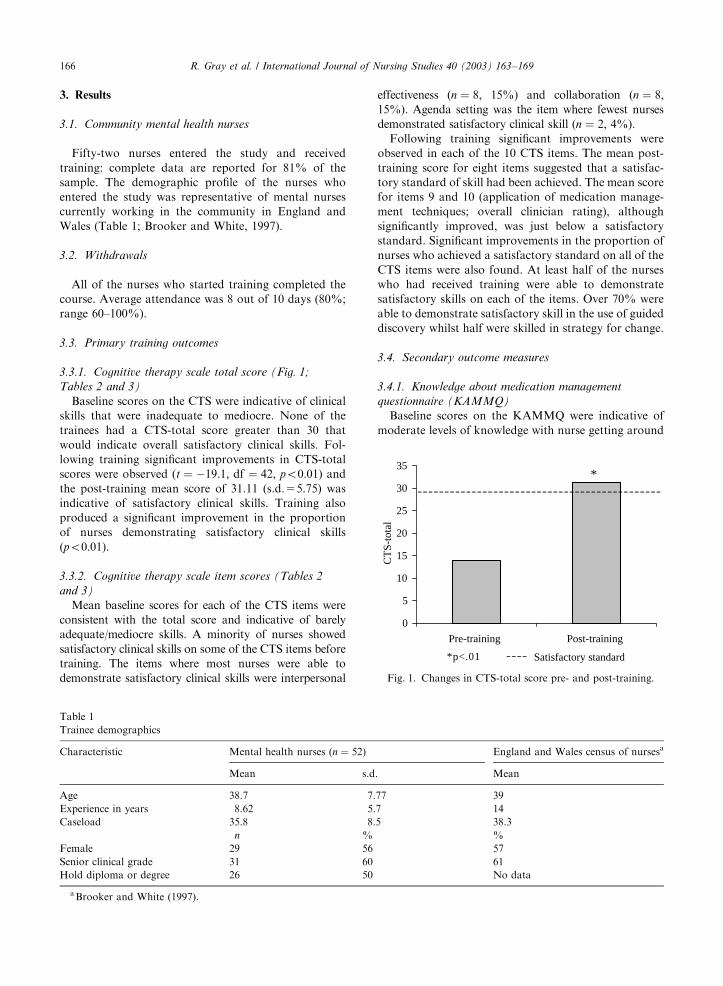
3.3.1. Cognitive therapy scale total score (Fig. 1;
Tables 2 and 3)
Baseline scores on the CTS were indicative of clinical
skills that were inadequate to mediocre. None of the
trainees had a CTS-total score greater than 30 that
would indicate overall satisfactory clinical skills. Fol-
lowing training significant improvements in CTS-total
scores were observed (t ¼ �19:1; df ¼ 42; po0:01) andthe post-training mean score of 31.11 (s.d.=5.75) was
indicative of satisfactory clinical skills. Training also
produced a significant improvement in the proportion
of nurses demonstrating satisfactory clinical skills
(po0:01).
3.3.2. Cognitive therapy scale item scores (Tables 2
and 3)
Mean baseline scores for each of the CTS items were
consistent with the total score and indicative of barely
adequate/mediocre skills. A minority of nurses showed
satisfactory clinical skills on some of the CTS items before
training. The items where most nurses were able to
demonstrate satisfactory clinical skills were interpersonal
effectiveness (n ¼ 8; 15%) and collaboration (n ¼ 8;15%). Agenda setting was the item where fewest nurses
demonstrated satisfactory clinical skill (n ¼ 2; 4%).
Following training significant improvements were
observed in each of the 10 CTS items. The mean post-
training score for eight items suggested that a satisfac-
tory standard of skill had been achieved. The mean score
for items 9 and 10 (application of medication manage-
ment techniques; overall clinician rating), although
significantly improved, was just below a satisfactory
standard. Significant improvements in the proportion of
nurses who achieved a satisfactory standard on all of the
CTS items were also found. At least half of the nurses
who had received training were able to demonstrate
satisfactory skills on each of the items. Over 70% were
able to demonstrate satisfactory skill in the use of guided
discovery whilst half were skilled in strategy for change.
3.4. Secondary outcome measures
3.4.1. Knowledge about medication management
questionnaire (KAMMQ)
Baseline scores on the KAMMQ were indicative of
moderate levels of knowledge with nurse getting around
Table 1
Trainee demographics
Characteristic Mental health nurses (n ¼ 52) England and Wales census of nursesa
Mean s.d. Mean
Age 38.7 7.77 39
Experience in years 8.62 5.7 14
Caseload 35.8 8.5 38.3
n % %
Female 29 56 57
Senior clinical grade 31 60 61
Hold diploma or degree 26 50 No data
aBrooker and White (1997).
0
5
10
15
20
25
30
35
Pre-training Post-training
CT
S-to
tal
*
*p<.01 Satisfactory standard
Fig. 1. Changes in CTS-total score pre- and post-training.
R. Gray et al. / International Journal of Nursing Studies 40 (2003) 163–169166

half of the questions correct (mean=9.05, s.d.=2.15).
Following training significant improvements in
knowledge were observed (mean=12.43, s.d.=2.34,
t ¼ �11:04; df ¼ 38; po0:01) with nurses getting around
75% of questions correct.
3.4.2. Ratings of nurse satisfaction with training
All trainees (n ¼ 47; 100%) reported that they were
either very satisfied or satisfied with the content of the
course and the quality of the teaching. They also
reported that they were able to apply the skills they
had learnt to the patients on their caseload.
3.4.3. Safety and aceptability of training
Safety was examined by looking at the number of
trainees whose clinical skills had deteriorated at the
post-training assessment. The acceptability of training
was determined by examining the number of trainees
who dropped out of training. Clinical skills did not
deteriorate in any of the participants and none of the
CMHNs withdrew from training. There were no other
unexpected effects of training.
3.5. Prediction of change
Exploratory stepwise linear regression was used to
identify factors predictive of trainees’ knowledge and
skill following training. Post-training scores on the CTS
and the KAMMQ were the dependent variables. Base-
line scores were entered first and then the following
variables were entered on the second level using stepwise
procedures: Trainees’ caseload size, experience, clinical
Table 2
CTS total and item scores pre- and post-training
CTS item Pre-training (n ¼ 52) Post-training (n ¼ 43) p
Mean s.d. Mean s.d.
Agenda setting 0.93 0.95 2.95 0.96 o0.01
Feedback 1.40 1.1 3.25 0.99 o0.01
Understanding 1.22 0.85 3.36 1.03 o0.01
Interpersonal effectiveness 1.62 0.89 3.14 1.17 o0.01
Collaboration 1.60 0.96 3.02 1.37 o0.01
Pacing and efficient using of time 1.31 0.95 3.20 0.97 o0.01
Guided discovery 1.36 0.83 3.39 1.15 o0.01
Strategy for change 1.40 0.94 3.14 1.17 o0.01
Application of medication management techniques 1.44 0.81 2.84 1.03 o0.01
Clinician rating 1.58 0.83 2.77 0.89 o0.01
Total score 13.88a 4.27 31.12a 5.75 o0.01
aSatisfactory total score defined as X30.
Table 3
Proportion of mental health nurses whose skills were rated as satisfactory on the CTS pre- and post-training
CTS item Pre-training (n ¼ 52) Post-training (n ¼ 43)a p
n % n %
Agenda setting 2 4 31 60 o0.01
Feedback 7 13 33 64 o0.01
Understanding 2 4 33 63 o0.01
Interpersonal effectiveness 8 15 31 60 o0.01
Collaboration 8 15 27 52 o0.01
Pacing and efficient using of time 4 8 34 65 o0.01
Guided discovery 2 4 37 71 o0.01
Strategy for change 6 12 26 50 o0.01
Application of medication management techniques 3 6 27 52 o0.01
Clinician rating 5 10 30 58 o0.01
Total score 0 0 24 46 o0.01
aAs the most conservative method of handling missing values it was assumed that nurses who dropped out of the study did not have
satisfactory clinical skills.
R. Gray et al. / International Journal of Nursing Studies 40 (2003) 163–169 167

grade, highest academic qualification and attendance
(Kirkwood, 1998, pp. 57–72).
A model that included trainees’ highest academic
qualification, grade and attendance was predictive of
CTS scores post-training. Baseline scores alone ac-
counted for 67% of the variance in CTS scores
(R2 ¼ 0:67; F ¼ 109:34; po0:001). Highest academic
qualification, grade and attendance accounted for an
additional 29% of the variance (R2 ¼ 0:98 (adjusted
R2 ¼ 0:96), F ¼ 71:18; po0:001).Baseline scores on the KAMMQ were predicative of
trainees’ knowledge post-training (R2 ¼ 0:91; F ¼ 109:3;po0:001). No other significant predictors emerged.
4. Discussion
The aim of this study was to explore whether
medication management training was effective in im-
proving the clinical skills of CMHNs.
4.1. Were community mental health nurses
representative?
In this study the demographic characteristics of
participants were comparable with those in the recent
census of CMHNs (Brooker and White, 1997). This
suggests that they were representative of those currently
practicing in the UK.
4.2. Was training effective?
This study demonstrates that medication management
training for nurses improves clinical skills and knowl-
edge. The primary outcome measures showed statisti-
cally significant improvements in clinical skills post-
training. Significant improvements were also observed in
nurse’s knowledge about medication management.
Overall all nurses who attended training were satisfied
with the content of the course and reported that it was
relevant to their clinical practice.
The finding that, following training, clinical skills
have improved to a satisfactory standard is consistent
with Brooker and Butterworth (1993) and may suggest
that medication management training equips nurses with
the clinical skills and knowledge that are needed to
deliver compliance therapy in clinical practice safely and
effectively. However, this is an uncontrolled study and it
is not possible to rule out the possibility that clinical
skills may have developed over time independently
of training. It is also not possible to exclude that
training had non-specific effects that were not related to
the content of the course. That is to say attention
(exposure to a teaching environment) improves clinical
skills (the Hawthorne effect). It is also unclear from this
study whether the impact of training on skills is durable
over time. However, the findings of this study do suggest
that further exploration into the effects of medication
management training on nurse’s skills, practice and on
clinical outcomes is warranted.
4.3. Was training safe and acceptable?
Medication management training was acceptable to
nurses and did not result in unexpected findings with
regard to safety. Training involved the use of videotaped
role-play exercises that involve critical examination of
clinical skills. It is possible that this may have been
unacceptable to nurses. However, this did not seem to be
the case as satisfaction was high and there were no
withdrawals from training.
4.4. Predictors of response
A regression model found that clinical grade, level of
academic preparation and attendance was predictive of
skill but not knowledge acquisition. This may suggest
that senior, and more qualified, nurses are more
receptive to training and learning new skills. The model
also suggests that there is a dose dependent effect of
training. That is to say that the more exposure to
training the more skills develop.
4.5. Pre-training skills and knowledge
In a representative sample of CMHNs, pre-training
scores on the CTS were indicative of clinical skills that
were barely adequate. This finding is consistent with the
survey of reported practice by Gray et al. (2001) that
showed that CMHNs acknowledged that they needed
more training in interventions to improve adherence in
patients with schizophrenia. These findings suggest that
patients are being deprived of therapeutic approaches
that will benefit their mental symptoms and may reduce
unnecessary side effects they are experiencing from their
medication.
4.6. Methodological considerations
Clinical skills were measured by asking nurses to
undertake a 10-min role-play task that was videotaped
and then blind rated. This method is a proxy of the skills
used in actual clinical practice. However, it is possible
that improvements seen post-training could be attrib-
uted to a reduction in nurses’ anxiety about being
videotaped or rehearsal of how to perform during the
role-play. Brooker and Butterworth (1993) used an
alternative method: they asked participants to audiotape
sessions with patients that were subsequently submitted
for analysis. However, nurses are able to select which
session they submit for rating and there is the potential
for tapes not to be submitted. The method of measuring
R. Gray et al. / International Journal of Nursing Studies 40 (2003) 163–169168

clinical skills in this study represents a novel, practical
way of examining the impact of training on clinical
skills.
5. Conclusions and recommendations
Compliance therapy can improve clinical outcomes in
patients with schizophrenia by maximising the clinical
potential of antipsychotic medicines to treat psychotic
symptoms and prevent relapse. The British National
Service Framework for Mental Health (DoH, 1999) has
recommended that Compliance Therapy should be
incorporated into the routine clinical practice of
psychiatric professionals. This study aimed to demon-
strate that training was effective in developing CMHNs
medication management clinical skills and knowledge
enabling them to potentially deliver compliance therapy
safely and effectively in routine clinical practice.
Following training there were statistically significant
improvements in mean scores on the CTS and just under
half of the trainees demonstrated satisfactory clinical
skills. Knowledge improved significantly and there was
evidence that training was acceptable to nurses and did
not produce any unexpected outcomes. Whether these
improvements are translated into improved clinical
practice may warrant further examination.
Acknowledgements
This project was funded by the South London and
Maudsley NHS Trust and the Institute of Psychiatry,
Kings College, London. There are no conflicts of
interest.
References
Birchwood, M., Smith, V., Drury, V., et al., 1994. A self-
report insight scale for psychosis: reliability, validity and
sensitivity to change. Acta Psychiatrica Scandinivica 89,
62–67.
Brooker, A., Butterworth, C., 1993. Training in psycho-
social intervention: the impact of the role of community
psychiatric nurses. Journal of Advanced Nursing 18,
583–590.
Brooker, C., Fallon, I., Butterworth, A., et al., 1994. The
outcome of training community psychiatric nurses to deliver
psychosocial intervention. British Journal of Psychiatry 165,
222–230.
Brooker, C., White, E., 1997. The fourth quinquennial national
community mental health nursing census of England and
Wales. University of Manchester, Manchester.
Buchanan, A., 1992. A two-year prospective study of treatment
compliance in patients with schizophrenia. Psychological
medicine 22, 787–797.
Day, J.C., Wood, G., Dewey, M., Bentall, R.P., 1995. A self-
rating scale for measuring neuroleptic side-effects. Valida-
tion in a group of schizophrenic patients. British Journal of
Psychiatry 166, 650–653.
Davis, J.M., Andriukaitis, S., 1986. The natural course of
schizophrenia and effective maintenance drug treatment.
Journal of Clinical Psychopharmacology 6, 2S–10S.
Department of Health, 1999. The National Service Framework
for Mental Health. The Stationary Office, London.
Gask, L., 1999. Acquisition of clinical skills. Advances in
Psychiatric Treatment 5 (4), 31–316.
Gray, R., Wykes, T., Parr, A.-M., Harls, E., Goumay, K., 2001.
The use of outcome measures to evaluate the efficacy and
tolerability of antipsychotic medication: a comparison of
thorn graduate and CPN practice. Journal of Psychiatric
and Mental Health Nursing 8, 191–196.
Haynes, R.B., Montague, P., Oliver, T., et al., 2002. Interven-
tions for helping patients follow prescription for medica-
tions (Cochrane Review). In: The Cochrane Library, Issue
5, Update Software, Oxford.
Hogan, T.P., Awad, A.G., Eastwood, R., 1983. A self-report
scale predictive of drug compliance in schizophrenic:
reliability and discriminative validity. Psychological Medi-
cine 13, 177–183.
Kemp, R., Hayward, P., Applewhaite, G., Eventt, B., David,
A., 1996. Compliance therapy in psychotic patients:
randomised controlled trial. British Medical Journal 312,
702, 345–349.
Kemp, R., Kirov, G., Everitt, P., et al., 1998. Randomised
controlled trial of compliance therapy 18-month follow-up.
British Journal of Psychiatry 172, 413–419.
Kirkwood, B., 1998. Essentials of Medical Statistics. Blackwell
Science, Oxford.
Lancashire, S., Haddock, G., Tarrier, N., et al., 1997. The
impact of training community psychiatric nurses to use
psychosocial interventions with people who have severe
mental health problems. Psychiatric Services 48, 39–41.
Scott, J., Jennings, T., Standard, S., et al., 1999. The impact of
training in problem-based interviewing on the detection and
management of psychological problems presenting in
primary care. British Journal of General Practice 49 (443),
441–445.
Taylor, D., McConnell, D., McConnell, H., et al., 2001. The
Bethlem and Maudsley NHS Trust Prescribing Guidelines,,
6th Edition. Martin Dunitz, London.
Vallis, T.M., Shaw, B.F., Dobson, K.S., 1986. The cognitive
therapy scale: psychometric properties. Journal of Consult-
ing and Clinical Psychology 54 (3), 381–385.
Weiden, P.J., Olfson, M., 1995. Cost of relapse in schizo-
phrenia. Schizophrenia Bulletin 21, 419–429.
R. Gray et al. / International Journal of Nursing Studies 40 (2003) 163–169 169