the direct anterior approach: here today, gone tomorrow—affirms
TRANSCRIPT

Author's Accepted Manuscript
The Direct Anterior Approach: Here Today, GoneTomorrow – Affirms
Brad L. Penenberg MD, Antonia Woehnl MD
PII: S1045-4527(14)00075-3DOI: http://dx.doi.org/10.1053/j.sart.2014.04.006Reference: YSART50595
To appear in:Semin Arthro
Cite this article as: Brad L. Penenberg MD, Antonia Woehnl MD, The Direct AnteriorApproach: Here Today, Gone Tomorrow – Affirms,Semin Arthro , http://dx.doi.org/10.1053/j.sart.2014.04.006
This is a PDF file of an unedited manuscript that has been accepted for publication. As aservice to our customers we are providing this early version of the manuscript. Themanuscript will undergo copyediting, typesetting, and review of the resulting galley proofbefore it is published in its final citable form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers that applyto the journal pertain.
www.elsevier.com/locate/enganabound

The Direct Anterior Approach: Here Today, Gone Tomorrow – Affirms
Brad L. Penenberg, MD, and Antonia Woehnl, MD
Brad L. Penenberg, MD
Director, Hip and Knee Section, Cedars-Sinai Medical Center, Los Angeles, CA
Antonia Woehnl, MD
Research Fellow, Cedars-Sinai Medical Center, Los Angeles, CA
Research from: Cedars-Sinai Medical Center, Los Angeles, CA
Dr. Penenberg has the following financial disclosures: Royalties: Microport Orthopedics;
Stock holder: Radlink Imaging
Address reprint requests to:Brad L. Penenberg, MD
Director, Hip and Knee Section, Cedars-Sinai Medical Center, Los Angeles, CA
120 South Spalding Drive, Suite 400
Beverly Hills, CA 90212, USA
Phone: 310.860.3470, Fax: 310.659.2724
Email: [email protected]
"I believe in everything until it's disproved. So I believe in fairies, the myths,
dragons … it all exists, even if it's in your mind."
John Lennon

There has been great enthusiasm for minimally invasive surgery (MIS) or accelerated
recovery total hip arthroplasty (THA) over the last decade. This has perhaps been driven
by economic imperatives as well as the decreasing average age of the THA patient and
the need to return to work.1 The first glimpse at what accelerated recovery might look
like was afforded by the two-incision approach to THA introduced in 2000.2,3 In spite of
the fact that dramatic improvement in immediate postoperative function could occur with
this approach, there was a difficult learning curve and a higher than acceptable
complication rate.2,4,5 It appears to have been all but abandoned. In the last 7 to 8 years
an approach to the hip that was first described in 1883 and then in 1917 by Smith-
Peterson, has received renewed interest.6-8
The initial appeal, of what is now referred to as the Direct Anterior approach
(DA), was the idea that, for the first time, a THA could be performed without cutting any
muscle or tendon. We were lead to believe preserving all of these structures was why
patients appeared to recover faster. Over the last year it has come to light that, in a very
high percentage of these cases, both tendon and capsular release are performed in order to
access the femoral canal safely.9,10 In spite of these additional releases, advocates
continue to see early return to function and feel that traditional hip precautions are not
necessary. There appears, however, to be an abundance of data that describes the
difficult learning curve prior to becoming proficient with this approach.11-15 The surgeon
new to this procedure can expect the occurrence of trochanteric fractures, wound
problems, and lateral femoral cutaneous nerve injury.11-13,16-18 19-24 It has even been
acknowledged that because of the location of the incision and the nature of the skin in

this area wound problems can persist beyond the learning curve.16 There have also been
admonitions to avoid larger patients and patients with lower offset hip.12,25-27 Industry
sources (Zimmer, DePuy, Stryker, Biomet, Microport Ortho) have claimed that in spite of
ongoing educational initiatives market penetration of the Direct Anterior approach has
remained level at about 20% of surgeons.
Emerging Alternative
Of interest to the remaining 80% of us (and probably many in that 20%) is the fact
that there appears to be a growing body of evidence in support of the fact that a highly
modified, or a Direct Posteriortm (DP) approach, can achieve all of the same goals as the
Direct Anterior approach, but without the risk. 28-33 The DP is essentially a sub-segment
of the traditional Moore, Gibson, or Kocher Langenbeck approach. Risk is mitigated by
the fact that, at any point in this procedure, it is possible to simply extend the dissection
and return to familiar landmarks (Figure 1b). The DPtm, an emerging alternative to the
DA, is typically performed in the familiar lateral decubitus position. The skin incision
travels obliquely a distance of approximately 3 to 6 inches from the posterior corner of
the greater trochanter (Figure 1a). The approach is essentially trans-gluteal. The
iliotibial band is not incised, but gluteus maximus fibers are gently teased apart. The
conjoined tendon is then identified by palpation and incised (as described for the DA).9
Obturator externus tendon and piriformis tendon are preserved in most cases and the
quadratus muscle is preserved in all cases (Figure 2).33
Mythology of the Direct Anterior Approach

The very visible nature of the DA, as it is marketed (by industry and surgeons)
and offered as a “new and unique technique” along with its imprecise comparisons to
“the posterior approach”, has resulted in a number of misconceptions (Figure 3).19 As
these promotional efforts continue, the superiority of the DA versus anything else,
especially anything “posterior” has come to be based on supposition and perhaps wishful
thinking, rather than data. The available database of peer-reviewed publications does not
support the fact that most of the attributes associated with the DA are unique to the
DA.28,30-32,34 In order to better understand where marketing and promotion leave off and
fact exists this paper presents the most notable misrepresentations of the Direct Anterior
approach.
Myth 1: The DA is the only alternative to result in accelerated recovery.
There is a growing body of data that demonstrates “accelerated recovery” with scaled
down or modified posterior approaches. The Direct Posterior approach, for example, has
resulted in an equally accelerated recovery with length of stay after THA of two days or
less and a mean time to cane of 5 days.28,30-34 When DA versus DP data are compared
there was no difference in early functional outcome.35,36
Myth 2: The DA is the only option permitting “no precautions” postoperatively.
As it turns out soft tissue preservation, capsular preservation and repair, and careful
attention to intraoperative range of motion testing have permitted the lifting of
postoperative precautions, even when a posterior approach is used. Studies with between
250 to 700 patients have been found to result in a dislocation rate of 0.0% to 0.4%
without the use of hip precautions after primary THA.28,30,37
Myth 3: The DA will be safe and precise after the “learning curve” of 50 cases.11-15

Advocates of the DA who publish this data on learning curves are usually surgeons with
a case volume of 200 hips per year or more. However, recent studies have found their
learning curve to include between 100 and 200 cases with complication rates of up to
16%.11-13,15,16,24 Wound healing complications for example were observed throughout one
series of 800 cases (4.6%).16 Figures 4 to 8 represent cases that were referred to the senior
author (BLP) within the past 12 months as complications from the Direct Anterior
approach. In each instance the surgeon told the patient that he had performed more than
100 DA cases (Figures 4 - 8).
Myth 4: The DA is indicated for all patients regardless of body habitus and type of
hip disease.12,25-27,38
Apparently, because of the difficulty achieving femoral access, it is recommended that
surgeons new to the technique avoid patients with large BMI and low offset.
Myth 5: The DA has a lower dislocation rate than “the” posterior approach.
Data pertaining to modern THA, with preservation and repair of the posterior capsule and
careful range of motion testing report dislocation rates identical to, or lower than, those
reported for the DA. It is important to realize that the high dislocation rates ascribed with
a broad stroke to the “posterior approach” appear in publications reporting on the
traditional posterior approach.13,16,18,27,28,37,39-43
Myth 6: It is essential to invest in costly capital equipment to achieve the results of
the DA.28,30-32,34
Numerous advocates of both approaches have described comparable results with and
without using a specialized table (fracture table, HANA table, etc)44,45

Myth 7: The DA is performed without cutting any tendons or the posterior joint
capsule.9,10
Over the last year, as authors beyond the technique developers have begun to report their
experience with the DA, it is becoming clear that modifications are being applied. To
access the femoral canal many surgeons advocating the DA have clearly indicated in
recent publications that tendon and capsule releases are frequently performed, affecting
the conjoined tendon in up to 71% and the piriformis tendon in 7%.9,46
Myth 8: A surgeon who does not perform the DA is a second-class citizen.
This of course is a subjective conclusion, but what else is a patient or a referring
physician supposed to believe if a fair and balanced story is not told (Figures 3 and 9).19 I
would suggest that it is appropriate for any surgeon interested in performing THA, to
become comfortable with the idea that he may have “chosen not to do that anterior
approach.” There is an abundance of data to support that choice and we should be
prepared to educate our patients regarding the true state of the art.
Conclusions
When we apply something new, the goal is to improve the outcome. Why choose
an option almost guaranteed to result in a life altering complication as it is being learned?
It is the only logical, if not the ethical choice, to favor an option that allows improvement
in surgical technique and outcome, but with the safety of knowing that the result can be
no worse than one’s baseline. Unlike the Direct Posterior approach, the Direct Anterior
approach does not offer a readily extensile option that permits the surgeon to return to

familiar territory and a “comfort zone” if a point of uncertainty occurs during the new
procedure.
It is clear that the DA can work but it presents a high-risk transition for most
surgeons. Once it becomes more widely understood that the advantages offered by the
Direct Anterior and Direct Posteriortm are equal, there is an excellent chance that the
Direct Anterior approach will be gone tomorrow.

References
1. US Department of Health and Human Services: Centers for Disease Control and
Prevention NCfHS: National Hospital Discharge Survey: 2010 table, procedures
by selected patient characteristics - number by procedure, category and
age. Available from:
http://www.cdc.gov/nchs/data/nhds/4procedures/2010pro4_numberprocedureage.
pdf, 2010
2. Pagnano MW, Trousdale RT, Meneghini RM, et al: Slower recovery after two-
incision than mini-posterior-incision total hip arthroplasty. Surgical technique. J
Bone Joint Surg Am 91 Suppl 2 Pt 1:50-73, 2009
3. Berger RA, Duwelius PJ: The two-incision minimally invasive total hip
arthroplasty: technique and results. Orthop Clin North Am 35:163-72, 2004
4. Pagnano MW, Leone J, Lewallen DG, et al: Two-incision THA had modest
outcomes and some substantial complications. Clin Orthop Relat Res 441:86-90,
2005
5. Bal BS, Haltom D, Aleto T, et al: Early complications of primary total hip
replacement performed with a two-incision minimally invasive technique.
Surgical technique. J Bone Joint Surg Am 88 Suppl 1 Pt 2:221-33, 2006
6. Hueter C: Fünfte Abtheilung, Neunundzwanzigstes Capitel, Die Verletzungen und
Krankheiten der Hüftgelenksgegend in: Grundriss der Chirurgie, Leipzig, Verlag
von F.C.W. Vogel, 1882, pp 870-945
7. Smith-Petersen MN: Approach to and exposure of the hip joint for mold
arthroplasty. J Bone Joint Surg Am 31A:40-6, 1949

8. Rachbauer F, Kain MS, Leunig M: The history of the anterior approach to the hip.
Orthop Clin North Am 40:311-20, 2009
9. Rodriguez JA, Walters BL, Cooper HJ: SE 32 - Applied Anatomy. AAOS
Chicago, 2013 (Poster)
10. Ito Y, Matsushita I, Watanabe H, et al: Anatomic mapping of short external
rotators shows the limit of their preservation during total hip arthroplasty. Clin
Orthop Relat Res 470:1690-5, 2012
11. Spaans AJ, van den Hout JA, Bolder SB: High complication rate in the early
experience of minimally invasive total hip arthroplasty by the direct anterior
approach. Acta Orthop 83:342-6, 2012
12. Hallert O, Li Y, Brismar H, et al: The direct anterior approach: initial experience
of a minimally invasive technique for total hip arthroplasty. J Orthop Surg Res
7:17, 2012
13. Woolson ST, Pouliot MA, Huddleston JI: Primary total hip arthroplasty using an
anterior approach and a fracture table: short-term results from a community
hospital. J Arthroplasty 24:999-1005, 2009
14. Goytia RN, Jones LC, Hungerford MW: Learning curve for the anterior approach
total hip arthroplasty. J Surg Orthop Adv 21:78-83, 2012
15. Masonis J, Thompson C, Odum S: Safe and accurate: learning the direct anterior
total hip arthroplasty. Orthopedics 31, 2008
16. Jewett BA , Collis DK: High complication rate with anterior total hip
arthroplasties on a fracture table. Clin Orthop Relat Res 469:503-7, 2011

17. Bal BS, Lowe JA, E Gietler A, et al: Heterotopic ossification after 2-incision total
hip arthroplasty. J Arthroplasty 25:538-40, 2010
18. Bal SB: Bal versus Sculco over Anterior THA: Orthopedics This Week, 2013.
19. Martin CT, Pugely AJ, Gao Y, et al: A Comparison of Hospital Length of Stay
and Short-term Morbidity Between the Anterior and the Posterior Approaches to
Total Hip Arthroplasty. J Arthroplasty 28:849-54, 2013
20. Leunig M, Faas M, von Knoch F, et al: Skin Crease 'Bikini' Incision for Anterior
Approach Total Hip Arthroplasty: Surgical Technique and Preliminary Results.
Clin Orthop Relat Res, 2013.
21. Bhargava T, Goytia RN, Jones LC, et al: Lateral femoral cutaneous nerve
impairment after direct anterior approach for total hip arthroplasty. Orthopedics
33:472, 2010
22. Goulding K, Beaulé PE, Kim PR, et al: Incidence of lateral femoral cutaneous
nerve neuropraxia after anterior approach hip arthroplasty. Clin Orthop Relat Res
468:2397-404, 2010
23. Myers SR, Leahy M: Anterior Approach Total Hip Arthroplasty: The Heuter
Interval. Seminars in Arthroplasty 19:201-204, 2008
24. Yi C, Agudelo JF, Dayton MR, et al: Early complications of anterior supine
intermuscular total hip arthroplasty. Orthopedics 36:e276-81, 2013
25. Restrepo C, Parvizi J, Pour AE, et al: Prospective randomized study of two
surgical approaches for total hip arthroplasty. J Arthroplasty 25:671-9.e1, 2010

26. Seng BE, Berend KR, Ajluni AF, et al: Anterior-supine minimally invasive total
hip arthroplasty: defining the learning curve. Orthop Clin North Am 40:343-50,
2009
27. Sariali E, Leonard P, Mamoudy P: Dislocation after total hip arthroplasty using
Hueter anterior approach. J Arthroplasty. 23:266-72, 2008
28. Penenberg BL, Bolling WS, Riley M: Percutaneously assisted total hip
arthroplasty (PATH): a preliminary report. J Bone Joint Surg Am 90 Suppl 4:209-
20, 2008
29. Brody JE: Less-Invasive Hip Surgery Makes Inroads, The New York Times,
February 9, 2010
30. Chow J, Penenberg B, Murphy S: Modified micro-superior percutaneously-
assisted total hip: early experiences & case reports. Curr Rev Musculoskelet Med
4:146-50, 2011
31. Roger DJ, Hill D: Minimally invasive total hip arthroplasty using a
transpiriformis approach: a preliminary report. Clin Orthop Relat Res 470:2227-
34, 2012
32. Daluga DJ: Accuracy of the acetabular index using the percutaneous assisted total
hip technique. Am J Orthop (Belle Mead NJ) 41:74-8, 2012
33. Penenberg B: Total Hip Arthroplasty: The Direct Posterior Approach, Advances
in Orthopaedics, Cedars-Sinai Medical Center, Los Angeles, CA, Winter 2014
34. Murphy SB, Ecker TM, Tannast M: THA performed using conventional and
navigated tissue-preserving techniques. Clin Orthop Relat Res 453:160-7, 2006

35. Nakata K, Nishikawa M, Yamamoto K, et al: A clinical comparative study of the
direct anterior with mini-posterior approach: two consecutive series. J
Arthroplasty 24:698-704, 2009
36. Maffiuletti NA, Impellizzeri FM, Widler K, et al: Spatiotemporal parameters of
gait after total hip replacement: anterior versus posterior approach. Orthop Clin
North Am 40:407-15, 2009
37. Eslampour A, Erens G, Bradbury TL, et al: P020 - Are Hip Precautions Necessary
after Posterior Approach to Total Hip Arthroplasty? AAOS Chicago, 2013
(Poster)
38. Oinuma K, Eingartner C, Saito Y, et al: Total hip arthroplasty by a minimally
invasive, direct anterior approach. Oper Orthop Traumatol 19: 10-26, 2007
39. Matta JM, Shahrdar C, Ferguson T: Single-incision anterior approach for total hip
arthroplasty on an orthopaedic table. Clin Orthop Relat Res 441:115-24, 2005
40. Browne JA, Pagnano MW: Surgical technique: a simple soft-tissue-only repair of
the capsule and external rotators in posterior-approach THA. Clin Orthop Relat
Res 470:511-5, 2012
41. Gulati A, Dwyer AJ, Shardlow DL: The impact of posterior approach for total hip
arthroplasty on early complications. Acta Orthop Belg 74:200-5, 2008
42. Weeden SH, Paprosky WG, Bowling JW: The early dislocation rate in primary
total hip arthroplasty following the posterior approach with posterior soft-tissue
repair. J Arthroplasty 18:709-13, 2003

43. White RE, Forness TJ, Allman JK, et al: Effect of posterior capsular repair on
early dislocation in primary total hip replacement. Clin Orthop Relat Res 163-7,
2001
44. Kennon RE, Keggi JM, Wetmore RS, et al: Total hip arthroplasty through a
minimally invasive anterior surgical approach. J Bone Joint Surg Am 85-A Suppl
4:39-48, 2003
45. Berend KR, Lombardi AV, Seng BE, et al: Enhanced early outcomes with the
anterior supine intermuscular approach in primary total hip arthroplasty. J Bone
Joint Surg Am 91 Suppl 6:107-20, 2009
46. Meneghini RM, Pagnano MW, Trousdale RT, et al: Muscle damage during MIS
total hip arthroplasty: Smith-Petersen versus posterior approach. Clin Orthop
Relat Res 453:293-8, 2006

The Direct Anterior Approach: Here Today, Gone Tomorrow – Affirms
Brad L. Penenberg, MD, and Antonia Woehnl, MD
In recent years there has been a wave of enthusiasm for the DA. Its appeal centers around
the possibility of performing a THA “without cutting muscle or tendon.” This allegedly
provides the benefit of accelerated recovery, reduced dislocation rate, and absence of
postoperative precautions. However, literature shows that the price to the patient can be
unacceptably high. This paper provides some perspective on this risk and presents a safe
alternative (DPtm), which can achieve similar clinical results. The readily extensile DP
gives the surgeon new to the technique an opportunity to minimize risk associated with
the learning curve.
Key Words: total hip arthroplasty, direct anterior approach, direct posterior approach
The Direct Anterior Approach: Here Today, Gone Tomorrow – Affirms
Brad L. Penenberg, MD, Antonia Woehnl, MD
CAPTIONS
Figure 1 – Skin Incision for Direct Posterior
Figure 1a – The incision for the Direct Posteriortm approach (yellow, ITB intact) begins at
a point approximately 1 cm distal to the posterior corner of the greater trochanter. It is
directed posteriorly, 45˚ to the long axis of the patient. It typically spans a distance of
approximately 10 cm.
Figure 1b – For the beginner, carrying the DPtm incision more distally immediately
provides access to a more familiar landscape. The surgeon new to this approach has the
opportunity to stay in his or her comfort zone at all times. It is possible to scale down as
comfort and patient safety dictate.
ITB – iliotibial band, GMax – gluteus maximus, CT – conjoined tendon, P – piriformis,
sg – superior gemellus, oi – obturator internus, ig – inferior gemellus, OE – obturator
externus, QF – quadratus femoris
Figure 2 – Preferred Tendon Release
In the preferred version of the Direct Posteriortm approach, after incising the gluteus
maximus fascia, the fibers of the muscle are carefully teased apart. At a point
approximately 1 cm distal to the tip of the greater trochanter, the conjoined tendon can

almost always be palpated. Overlying fat is removed using electrocautery and suction.
The tendon can then be visualized as it courses beneath the posterior edge of the greater
trochanter. This is distinct from the piriformis, which inserts at the tip of the greater
trochanter. The CT is released beneath the edge of the trochanter as close to its insertion
as possible. In most instances, all remaining external hip rotators and the ITB can be
spared.33
ITB – iliotibial band, GMax – gluteus maximus, GMed – gluteus medius, GMin – gluteus
minimus, CT – conjoined tendon, P – piriformis, sg – superior gemellus, oi – obturator
internus, ig – inferior gemellus, OE – obturator externus, QF – quadratus femoris, gt –
greater trochanter, lt – lesser trochanter, c - capsule
Figure 3 – Newspaper Articles Making Inaccurate Comparisons
This New York Times article (March 18, 2013) leaves the reader with the impression that
the anterior approach is uniquely capable of “helping patients recover more quickly,”
return to cycling, lifting weights, etc, and “feel like I never had surgery.” It incorrectly
states that the dislocation rate is lower than with “the posterior” approach.
Figure 4a and 4b – Fluoroscopic Images with DA
This 44 year-old woman underwent bilateral DA. Figure 4a shows the limited
intraoperative view when using fluoroscopy during the DA. Figure 4b shows the
postoperative anteroposterior pelvic radiograph indicating a cup inclination of minus two
degrees on the right and of 68 degrees on the left side.

Figure 5 – Intraoperative Peritrochanteric Fracture during DA
This 58 year-old woman presented to the senior author 11 months following an attempted
THA via the DAA. The operating surgeon told the patient he had performed more than
300 such procedures. She suffered an intraoperative peritrochanteric fracture. She
required repositioning in order for the surgeon to switch to an extensile posterolateral
approach in attempt to fix the fracture and salvage a “routine” primary THA. She
remained wheelchair bound for 8 months as the femoral component slowly subsided and
it became clear she needed revision surgery.
Figure 6a and 6b – Intraoperative Trochanteric Fracture and Femoral Neuropathy
with Brooker III+ HO
This 62 year-old male, cardiologist and former cyclist, underwent a DA by a surgeon who,
according to the patient had “a lot of experience with this approach.” He presented to the
senior author at 10 months postoperatively with extensive heterotopic ossification and
flexion to 40 degrees. He suffered an intraoperative trochanteric fracture described by
the operating surgeon as inaccessible for fixation. He also suffered a femoral neuropathy
that he was told was responsible for the weakness that lead to a fall the day after surgery.
He was told that it was this fall that lead to his re-operation 3 days postoperatively
because of femoral subsidence.
Figure 7 – Wound Healed by Secondary Intention after DA
Thin skin in this area can lead to wound problems.16 This wound was left to heal by
secondary intention. It closed 18 days after surgery.

Figure 8a and 8b Trochanteric Fracture and Inadequate Fixation
This 89 year-old severely osteopenic female suffered a trochanteric fracture during the
course of her THA via a DA approach. Incision was extended and ORIF was attempted.
She was referred to the senior author because of severe limp and limited ambulation 1
year postoperatively.
Figure 9 – Misleading Publication Title Comparing DA to “The” Posterior
Approaches19
Articles such as this fail to differentiate that all “posterior approaches” are not the same.
This creates confusion unless the reader takes the time to read carefully thru this article
and realize this is a comparison to the “traditional posterior approach.” There is no
acknowledgement that modifications of this approach might be comparable to DA.

Fig 1A

Fig 1B
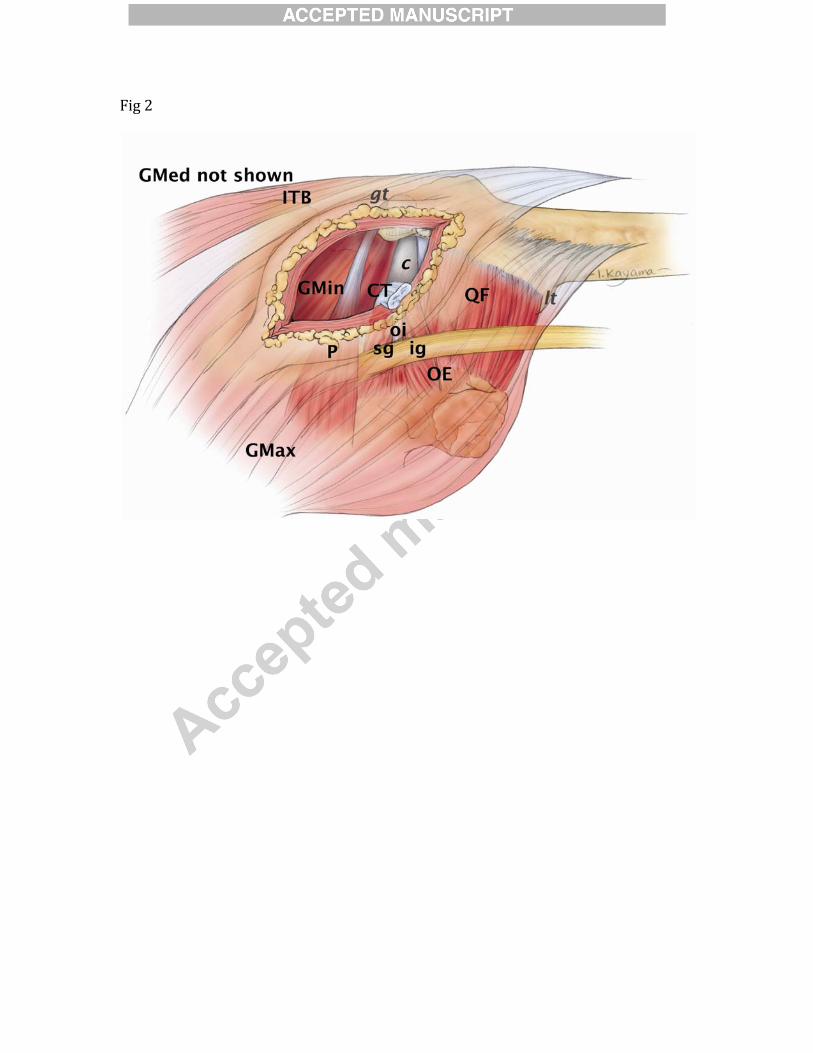
Fig 2

Fig 3

Fig 4A

Fig 4B

Fig 5

Fig 6
6A

Fig 6
6B

Fig 7
7

Fig 8
8A

Fig 8
8B

Fig 9