the cross-section trichometer: a new device for … · the cross-section trichometer: a new device...
TRANSCRIPT

The Cross-Section Trichometer: A New Device for MeasuringHair Quantity, Hair Loss, and Hair Growth
BERNARD COHEN, MD�
BACKGROUND Office physicians are unable to measure hair quantity, hair loss, and hair growth in asimple and meaningful manner. One solution is to measure the cross-sectional area of a bundle of hairthat is growing within a premeasured cross-section of scalp.
OBJECTIVE The objective was to design a mechanical device that precisely measures the cross-sec-tional area of a bundle of hair and design a device that can precisely delineate an area of scalp. It wasassumed that density and diameter changes are evidenced by changes in the bundle cross-sectional areaand that growth and loss are the result of density and diameter changes. These assumptions wereconfirmed using various sized bundles of known diameter non-hair filaments.
MATERIALS AND METHODS Bundles of hair and surgical silk fibers were tested using a mechanicaldevice that compressed the bundle and measured its cross-sectional area. Balding patients were cat-egorized according to their observed severity of the loss. Bundles of their uncut hair from 4-cm2 scalpsites were measured and the values were compared to the patient’s category of hair loss severity.
RESULTS In patients with balding, there was a direct correlation between the bundle’s cross-sectionalarea and the observed severity of the loss. The cross-sectional area was expressed as square millimetersof hair per square centimeter of skin� 100 (mm2/cm2� 100) and named the trichometric index (TI). Usingsurgical silk fibers, there was a direct correlation between the bundle’s cross-sectional area and thenumber of filaments, the diameter of the filaments, and the dry weight of the filament bundle. Usingaggregates of cut human hair, there was a direct correlation between the cross-sectional area and the dryweight of the bundle.
CONCLUSION This prototype device shows promise as a diagnostic instrument for measuring changesin hair quantity (mass), hair diameter, and hair density, as evidenced by preliminary studies using silksutures, cut human hair, and patients with various degrees of balding. Formal clinical studies are need-ed. Although the device itself showed a high degree of precision, the accuracy and reproducibility of themeasurements can be compromised if the sampling method is not carefully performed using magni-fication. The device is intended for use on uncut hair that is more than 1 inch in length.
Dr. Cohen holds patents on the method and device described in this report and will receive royalties on thesales.
Hair loss affects 75% of men and 10% of
women, but office physicians are unable to
measure its parameters in a simple and meaningful
way. Precise instrumentation and methodologies
have been limited to research centers and industry
laboratories where clinical studies and drug evalua-
tions are performed. The office physician needs
a rapid, easy, and precise method for measuring a
patient’s clinical status.
Hair quantity is determined by measuring the hair’s
density (n/cm2) and diameter (mm). Hair loss and
hair growth result when there is a fluctuation in one
and/or the other. An ideal hair-measuring technology
should reflect the simultaneous influence of both
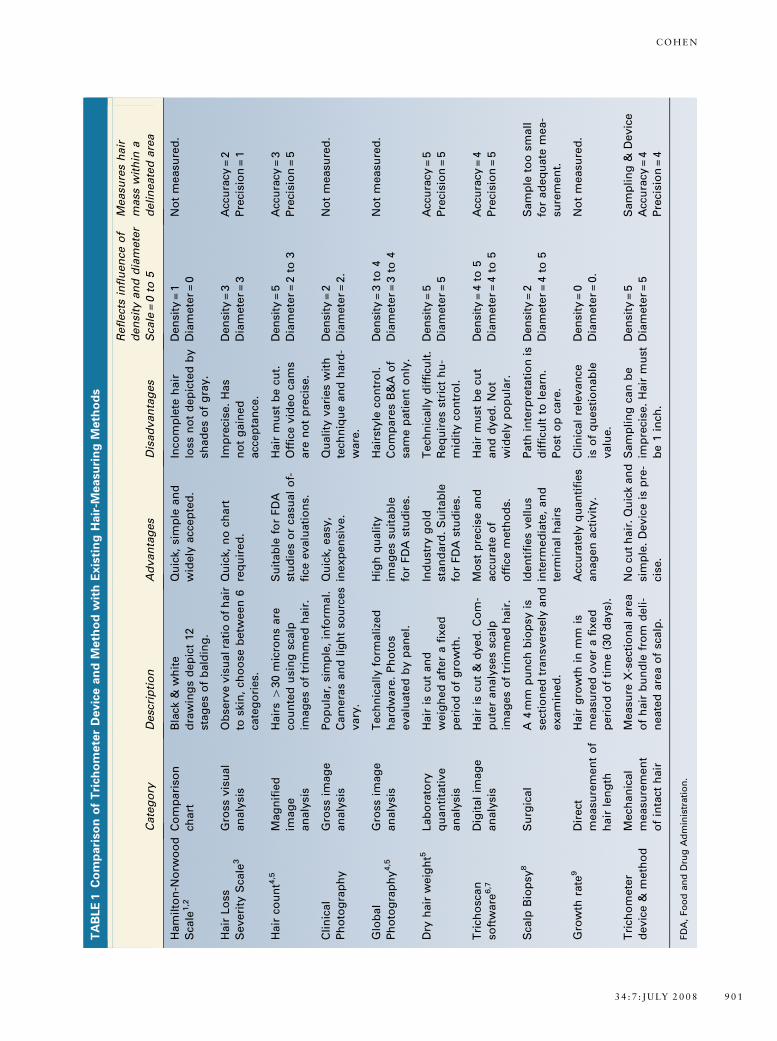
density and diameter. The present devices and
methods have advantages and limitations
(see Table 1).
In discussions of hair density and hair diameter, it is
helpful to draw the distinction between the termsF
shedding and thinning, since both result in hair loss.
In states of shedding, hairs with diameters of normal
size fall out. It is normal to shed about 50 to 100
& 2008 by the American Society for Dermatologic Surgery, Inc. � Published by Wiley Periodicals, Inc. �ISSN: 1076-0512 � Dermatol Surg 2008;34:900–911 � DOI: 10.1111/j.1524-4725.2008.34175.x
9 0 0
�Department of Dermatology and Cutaneous Surgery, University of Miami, Miller School of Medicine,Coral Gables, Florida
TA
BLE
1C
om
pari
so
no
fT
rich
om
ete
rD
evic
ean
dM
eth
od
wit
hE
xis
tin
gH
air
-Measu
rin
gM
eth
od
s
Cate
go
ryD
esc
rip
tio
nA
dvan
tag
es
Dis
ad
van
tag
es
Refl
ect
sin
flu
en
ceo
f
den
sity
an
dd
iam
ete
r
Sca
le=
0to
5
Measu
res
hair
mass
wit
hin
a
deli
neate
dare
a
Ham
ilto
n-N
orw
oo
d
Sca
le1,2
Co
mp
ari
son
chart
Bla
ck&
wh
ite
dra
win
gs
dep
ict
12
stag
es
of
bald
ing
.
Qu
ick,
sim
ple
an
d
wid
ely
acc
ep
ted
.
Inco
mp
lete
hair
loss
no
td
ep
icte
db
y
shad
es
of
gra
y.
Den
sity
=1
Dia
mete
r=
0
No
tm
easu
red
.
Hair
Lo
ss
Severi
tyS
cale
3
Gro
ssvis
ual
an
aly
sis
Ob
serv
evis
ualra
tio
of
hair
tosk
in,
cho
ose
betw
een
6
cate
go
ries.
Qu
ick,
no
chart
req
uir
ed
.
Imp
reci
se.
Has
no
tg
ain
ed
acc
ep
tan
ce.
Den
sity
=3
Dia
mete
r=
3
Acc
ura
cy=
2
Pre
cisi
on
=1
Hair
cou
nt4
,5M
ag
nif
ied
imag
e
an
aly
sis
Hair
s4
30
mic
ron
sare
cou
nte
du
sin
gsc
alp
imag
es
of
trim
med
hair
.
Su
itab
lefo
rFD
A
stu
die
so
rca
sual
of-
fice
evalu
ati
on
s.
Hair
mu
stb
ecu
t.
Off
ice
vid
eo
cam
s
are
no
tp
reci
se.
Den
sity
=5
Dia
mete
r=
2to
3
Acc
ura
cy=
3
Pre
cisi
on
=5
Cli
nic
al
Ph
oto
gra
ph
y
Gro
ssim
ag
e
an
aly
sis
Po
pu
lar,
sim
ple
,in
form
al.
Cam
era
san
dli
gh
tso
urc
es
vary
.
Qu
ick,
easy
,
inexp
en
sive.
Qu
ali
tyvari
es
wit
h
tech
niq
ue
an
dh
ard
-
ware
.
Den
sity
=2
Dia
mete
r=
2.
No
tm
easu
red
.
Glo
bal
Ph
oto
gra
ph
y4,5
Gro
ssim
ag
e
an
aly
sis
Tech
nic
all
yfo
rmali
zed
hard
ware
.P
ho
tos
evalu
ate
db
yp
an
el.
Hig
hq
uali
ty
imag
es
suit
ab
le
for
FD
Ast
ud
ies.
Hair
style
con
tro
l.
Co
mp
are
sB
&A
of
sam
ep
ati
en
to
nly
.
Den
sity
=3
to4
Dia
mete
r=
3to
4
No
tm
easu
red
.
Dry
hair
weig
ht5
Lab
ora
tory
qu
an
tita
tive
an
aly
sis
Hair
iscu
tan
d
weig
hed
aft
er
afi
xed
peri
od
of
gro
wth
.
Ind
ust
ryg
old
stan
dard
.S
uit
ab
le
for
FD
Ast
ud
ies.
Tech
nic
all
yd
iffi
cult
.
Req
uir
es
stri
cth
u-
mid
ity
con
tro
l.
Den
sity
=5
Dia
mete
r=
5
Acc
ura
cy=
5
Pre
cisi
on
=5
Tri
cho
scan
soft
ware
6,7
Dig
ital
imag
e
an
aly
sis
Hair
iscu
t&
dyed
.C
om
-
pu
ter
an
aly
ses
scalp
imag
es
of
trim
med
hair
.
Mo
stp
reci
sean
d
acc
ura
teo
f
off
ice
meth
od
s.
Hair
mu
stb
ecu
t
an
dd
yed
.N
ot
wid
ely
po
pu
lar.
Den
sity
=4
to5
Dia
mete
r=
4to
5
Acc
ura
cy=
4
Pre
cisi
on
=5
Sca
lpB
iop
sy8
Su
rgic
al
A4
mm
pu
nch
bio
psy
is
sect
ion
ed
tran
svers
ely
an
d
exam
ined
.
Iden
tifi
es
vell
us
inte
rmed
iate
,an
d
term
inal
hair
s
Path
inte
rpre
tati
on
is
dif
ficu
ltto
learn
.
Po
sto
pca
re.
Den
sity
=2
Dia
mete
r=
4to
5
Sam
ple
too
small
for
ad
eq
uate
mea-
sure
men
t.
Gro
wth
rate
9D
irect
measu
rem
en
to
f
hair
len
gth
Hair
gro
wth
inm
mis
measu
red
over
afi
xed
peri
od
of
tim
e(3
0d
ays)
.
Acc
ura
tely
qu
an
tifi
es
an
ag
en
act
ivit
y.
Cli
nic
al
rele
van
ce
iso
fq
uest
ion
ab
le
valu
e.
Den
sity
=0
Dia
mete
r=
0.
No
tm
easu
red
.
Tri
cho
mete
r
devic
e&
meth
od
Mech
an
ical
measu
rem
en
t
of
inta
cth
air
Measu
reX
-sect
ion
al
are
a
of
hair
bu
nd
lefr
om
deli
-
neate
dare
ao
fsc
alp
.
No
cut
hair
.Q
uic
kan
d
sim
ple
.D
evic
eis
pre
-
cise
.
Sam
pli
ng
can
be
imp
reci
se.
Hair
mu
st
be
1in
ch.
Den
sity
=5
Dia
mete
r=
5
Sam
pli
ng
&D
evic
e
Acc
ura
cy=
4
Pre
cisi
on
=4
FD
A,
Fo
od
an
dD
rug
Ad
min
istr
ati
on
.
3 4 : 7 : J U LY 2 0 0 8 9 0 1
C O H E N

hairs per day, but in pathologic states of effluvium
and alopecia areata, shedding can be quite profound.
Underlying skin becomes more and more visible as
the shedding progresses. The hair density analysis or
hair count will accurately reflect this disorder.
Hair thinning is a disorder characterized by the
gradual miniaturization in the length and diameter
of individual scalp hairs. Underlying skin becomes
more and more visible as the hairs become smaller
and smaller. Thinning affects an estimated 75% of
men, and although it occurs in 10% of healthy
women, it might indicate an endocrine abnormality
in a small group of those affected. Unlike shedding,
thinning is not diffuse in its distribution over the
entire scalp, but almost always appears in a pattern
that spares the posterior and sides of the lower scalp,
creating a familiar horse-shaped fringe that persists
in spite of the most advanced cases. Thinning will
eventuate in lowered density as the affected hairs
vanish.
Thinning, in its earliest stages, cannot be visualized
and is difficult to diagnose and quantify. Simple
density counts comparing the permanent occi-
pital fringe to an area of balding are of limited
value because the balding area has a mixed popula-
tion of normal-sized and miniaturized hairs (see
Figure 1).
The anatomic fluctuations of density and diameter
result in hair loss and growth, but it should be noted
that the changes in hair diameter are considerably
more influential than changes in hair density. Coarse
hair has a diameter of about 80 mm, average hair
about 70mm, and fine hair about 60 mm. Surpris-
ingly, an 80-mm hair has almost twice the mass of a
60-mm hair because it has approximately double the
cross-sectional area (3.14� r2 = cross-sectional area).
If two individuals have the same number of hairs, all
the same length, the one with coarse hair has almost
twice as much hair mass as the one with fine hair.
A 10% change in hair density will result in a 10%
change in hair quantity. A 10% change in diameter
will result in a 20% change in hair quantity. Because
hair length varies with style, it is not considered in
the calculation of hair quantity.
Objectives
The broad objective was to develop a technology for
measuring the quantity of hair in a defined area of
scalp. If the density and diameter of hair determines
its quantity, and the cross-sectional area of an
aggregate of hair reflects the range of densities and
diameters within that aggregate, then the cross-
sectional area of the aggregate reflects the quantity
of hair within the aggregate. Based on this theory, a
technology was designed to measure the cross-
sectional area of all the hairs in an aggregate of hair
from a premeasured area of scalp. This value could
be used to quantify the hair that is present and then,
by comparison, quantify the amount of hair that has
been lost or gained.
To measure the collective cross-sections of hair in the
premeasured area, the ideal method/device must first
capture the hairs and compress the loose aggregate
into a rectangular bundle, before the measurement is
performed. The device should always compress the
bundle with the same exact load, regardless of the
Figure 1. In hair loss due to balding or thinning, the hairshave a wide range of diameters. When a hair count isperformed, any hair with a diameter larger than 30 mm iscounted as one hair.
D E R M AT O L O G I C S U R G E RY9 0 2
T H E C R O S S - S E C T I O N T R I C H O M E T E R

hair sample size. The compressive force should com-
pletely compact the bundle, but not with a force so
excessive to damage the captured hair. The load
should be incrementally applied with mechanical
precision rather than casual hand-applied force. A
precise scientific instrument should be included to
measure the cross-sectional area of the compressed
and fully compacted bundle. It is preferable that no
hair is cut and no physician supervision or oversight
be required. The device should be of small size, sen-
sibly priced, widely available, easy to use, and capable
of generating results in a short period of time.
The Resultant Device and the Method
for Testing
A device/method that fulfilled the above objectives
was created. It was tested using silk filaments and
human hair to determine if changes in the cross-
sectional area were correlated to changes in
the hair density (n/cm2) and/or diameter (mm)
(see Tables 2–4).
The device is a self-contained mechanical unit with a
rectangular anodized aluminum body that is held in
the right hand like a hypodermic syringe (see Figure
2). Extending from one end of the body is a hook-
shaped arm, and from the other end of the body, a
spring-loaded shaft with a retainer cap. The hook
and the cap are at opposite ends of one contiguous
shaft. An electronic sensing unit with LED display is
externally mounted on the side of the housing and
attached internally to the shaft. When the cap at the
end of the shaft is pressed with the thumb, the hook
arm extends out of the body at the opposite end, and
its travel distance is displayed on the LED screen in
hundredths of a millimeter. When the thumb is re-
leased, the hook retracts back toward the body.
To measure the cross-sectional area of a hair sample,
the arm is extended and hooked around a bundle of
hair that has been gathered from a 2� 2-cm area of
scalp (see Figures 3–5). When the thumb is lifted, the
bundle of hair is captured in a 1� 4-mm chamber
created on the ledge of the metal housing through
which the hook passes. The number and diameter of
hairs in the captured bundle determine the height of
the hair within the chamber. When initially captured,
the bundle is slightly compressed and not yet com-
pacted.
The mid portion of the long shaft has a threaded
portion that passes through a large threaded knob at
the base of the body. When the knob is turned
clockwise on the shaft, it compresses a heavy internal
spring. As a result, the spring delivers a precise load
to the upper and lower surface of the captured
rectangular bundle and compacts it.
TABLE 2. Correlation between Silk Strand Diame-
ter and the Bundle Cross-section
3-0 4-0 5-0 6-0
Bundle Cross-
section (mm2)
Strands per bundle
80 3.81
60 20 3.63
40 40 3.07
20 60 2.70
80 2.36
60 20 2.14
40 40 2.03
20 60 1.65
80 1.37
60 20 1.26
40 40 1.09
20 60 0.82
80 0.66
Eighty-strand bundles of mixed-size suture material were measured.
TABLE 3. Correlation between Silk Strand Density and the Bundle Cross-section
No. of Strands 20 40 60 80 100 120 140 160
Cross-Section (mm2) .36 .75 1.17 1.58 1.93 2.36 2.75 3.14
Cross-section divided by No. of strands .018 .019 .020 .020 .019 .020 .020 .020
Twenty-strand bundles of 5-0 suture material were measured.
3 4 : 7 : J U LY 2 0 0 8 9 0 3
C O H E N
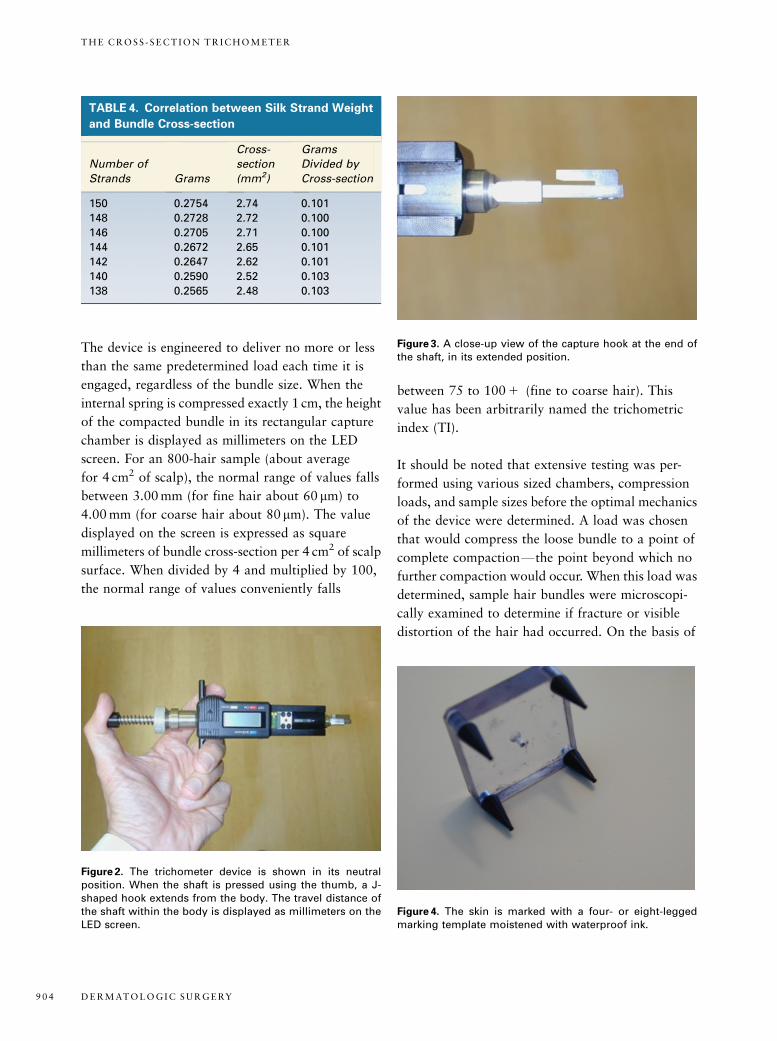
The device is engineered to deliver no more or less
than the same predetermined load each time it is
engaged, regardless of the bundle size. When the
internal spring is compressed exactly 1 cm, the height
of the compacted bundle in its rectangular capture
chamber is displayed as millimeters on the LED
screen. For an 800-hair sample (about average
for 4 cm2 of scalp), the normal range of values falls
between 3.00 mm (for fine hair about 60 mm) to
4.00 mm (for coarse hair about 80mm). The value
displayed on the screen is expressed as square
millimeters of bundle cross-section per 4 cm2 of scalp
surface. When divided by 4 and multiplied by 100,
the normal range of values conveniently falls
between 75 to 100 1 (fine to coarse hair). This
value has been arbitrarily named the trichometric
index (TI).
It should be noted that extensive testing was per-
formed using various sized chambers, compression
loads, and sample sizes before the optimal mechanics
of the device were determined. A load was chosen
that would compress the loose bundle to a point of
complete compactionFthe point beyond which no
further compaction would occur. When this load was
determined, sample hair bundles were microscopi-
cally examined to determine if fracture or visible
distortion of the hair had occurred. On the basis of
TABLE 4. Correlation between Silk Strand Weight
and Bundle Cross-section
Number of
Strands Grams
Cross-
section
(mm2)
Grams
Divided by
Cross-section
150 0.2754 2.74 0.101
148 0.2728 2.72 0.100
146 0.2705 2.71 0.100
144 0.2672 2.65 0.101
142 0.2647 2.62 0.101
140 0.2590 2.52 0.103
138 0.2565 2.48 0.103
Figure 2. The trichometer device is shown in its neutralposition. When the shaft is pressed using the thumb, a J-shaped hook extends from the body. The travel distance ofthe shaft within the body is displayed as millimeters on theLED screen.
Figure 3. A close-up view of the capture hook at the end ofthe shaft, in its extended position.
Figure 4. The skin is marked with a four- or eight-leggedmarking template moistened with waterproof ink.
D E R M AT O L O G I C S U R G E RY9 0 4
T H E C R O S S - S E C T I O N T R I C H O M E T E R
this, an optimal and safe standard compression load
was chosen. A working prototype was then designed
to deliver that same optimal load regardless of the
height (or the amount) of hair in the chamber. A self-
braking mechanism was added to prevent the oper-
ator from overtightening the threaded knob and
exceeding the optimal load. The spring material
and its design were further refined to insure that
the compression spring was in the center of its path
from fully opened to fully compressed, i.e., in the
mid range of its spring constant curve. This was done
to minimize the imprecision that metal springs
typically display at both ends of their compression
curves.
Results of Testing
The device was intended to indirectly measure den-
sity and diameter by directly measuring the cross-
sectional area of all the hairs in a premeasured area
of scalp skin. Four tests were performed. The first
was designed to determine if the device could detect
and measure small changes in surgical silk diameter
(mm). A second test was designed to determine if the
device could detect and measure small changes in the
bundle densities of hair and surgical silk (n/cm2).
A third test was designed to determine if there was a
correlation between the weight of the bundle and
its cross-sectional area. A fourth test sought to
establish a correlation between the observed hair loss
severity and the TI (mm2 hair per cm2 scalp� 100).
Diameter measurements were performed using
strands of 3-0, 4-0, 5-0, and 6-0 nonsterile braided
surgical silk (Havel’s Inc., Cincinnati, OH). Each
material was hand-measured using an electronic
micrometer (L.S. Starrett Co., Athol, MA), and
strand diameters were found to vary within 15 to
20mm along their length. The average diameters
were 3-0 = 150 mm, 4-0 = 100 mm, 5-0 = 75 mm, and
6-0 = 50 mm. Thirteen mixed-size bundles, composed
of 80 strands each, were prepared. The bundles were
incrementally reduced in size by mixing large caliber
strands with smaller caliber strands. Each bundle
was then measured using the device. When the re-
sults were plotted, the cross-sectional area of each
bundle was reduced in a sequence that mirrored the
incremental reduction of suture caliber (see Table 2).
Density measurements were performed using the
same braided silk suture material. Bundles of 5-0
silk, the diameter of which is approximately 75mm
(equivalent to the diameter of average-sized hair),
were prepared. Eight bundles, containing 20 fila-
ments each, were prepared. First the device was used
to measure the cross-sectional area of one bundle.
The device was then opened and a second bundle
was added. A second measurement was made, the
device was then reopened, and a third bundle was
added, etc. Bundles were incrementally placed in the
device until they totaled 160 fibers. The results are
posted in the chart below (see Table 3). The cross-
sectional area of the bundle was increased in a se-
quence that mirrored the incremental increase of
filaments added. The ratio of the number of fila-
ments to the cross-sectional diameter remained con-
stant.
Weight measurements were performed using a
150-strand bundle of 5-0 surgical filaments to de-
termine if the weight and the cross-sectional area of
a bundle were directly correlated. The bundle was
weighed on an electronic analytic balance, and its
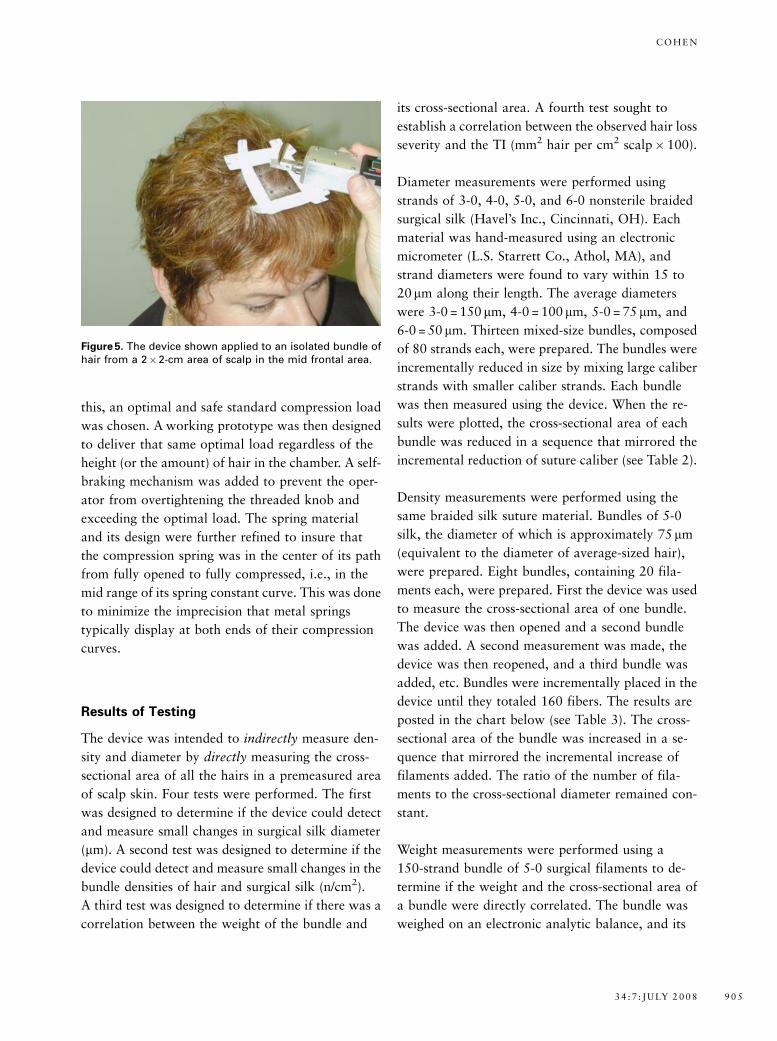
Figure 5. The device shown applied to an isolated bundle ofhair from a 2�2-cm area of scalp in the mid frontal area.
3 4 : 7 : J U LY 2 0 0 8 9 0 5
C O H E N

cross-sectional area was measured using the new
device. The measurements were performed in a lab-
oratory with no humidity control. Then two fila-
ments were cut from the bundle, the bundle was
reweighed, and its cross-section was remeasured.
This was repeated six times. The cross-sectional area
of the bundle was reduced in a sequence that mir-
rored the incremental reduction of bundle weight.
The ratio between the weight and the cross-section
remained constant (see Table 4).
Weight measurements were then performed using a
bundle of cut human hair to determine if the weight
and the cross-sectional area of a bundle were directly
proportional (see Table 5). The bundle contained an
aggregate of hairs (approximately 400) collected
from three different women, all of whom had un-
dergone hair coloring or permanents in the previous
3 months. The measurements were performed in a
laboratory with no humidity control. Hairs were
incrementally cut from the bundle, the bundle was
reweighed, and its cross-section was remeasured.
This was repeated eight times. The cross-sectional
area of the bundle was reduced in a sequence that
mirrored the incremental reduction of bundle
weight. The ratio between the weight and the cross-
section progressively increased over a period of
30 minutes. This was thought to be the result of
ambient moisture absorption during the time re-
quired to collect the data. With both silk filaments
and hair, the cross-sectional areas of the bundles
were reduced in a sequence that mirrored the incre-
mental reduction of bundle weight.
Twelve male patients, age 23 to 67 years with
balding, were examined without magnification. The
observed ratio of hair to skin in the vertex area of
each patient was estimated by an observer familiar
with the Hair Loss Severity Scale (HLSS) technique.
Each patient was placed into one of four categories:
minimal = much more hair than skin, mild = more
hair than skin, moderate = more skin than hair, and
severe = much more skin than hair (see Figure 6). The
hair within the 4� 4-cm center of the vertex area
was isolated and measured with the device and ex-
pressed as TIs (mm2 hair per cm2 skin� 100). The TI
and hair loss severity of each patient were charted to
determine if there was a correlation (see Table 6).
Collection of the Hair Sample
It was clear from the onset that the sampling method
would be quite influential in determining the sys-
tem’s total precision. A 2�2-cm square of hair-
TABLE 5. Correlation between Hair Weight and
Bundle Cross-section
Number of
Hairs Grams
Cross-
section
(mm2)
Grams
Divided by
Cross-section
X 0.5536 2.08 0.265
X minus 2 0.5528 2.04 0.271
X minus 4 0.5519 1.98 0.278
X minus 8 0.5511 1.95 0.284
X minus 10 0.5506 1.94 0.283
X minus 12 0.5494 1.92 0.286
X minus 14 0.5480 1.89 0.289
X minus 16 0.5467 1.87 0.292
X minus 20 0.5434 1.82 0.298
Hairs were cut from a bundle of approximately 600 hairs; the
bundle was reweighed, and its cross-section remeasured
Figure 6. The Hair Loss Severity Scale uses the visible ratioof hair to skin to quantify the hair within a localized area ofscalp.3 (A) minimal, (B) mild, (C) moderate, and (D) severe.
D E R M AT O L O G I C S U R G E RY9 0 6
T H E C R O S S - S E C T I O N T R I C H O M E T E R
bearing scalp skin was chosen because it could be
easily handled without magnification and repre-
sented a somewhat generous sample (see Figures 4
and 5). On average, this area contained about 800
hairs in patients with no loss. The sampling precision
was important since fewer than 3 hairs would, for
example, change the cross-sectional value of the
bundle from 3.30 mm2 to 3.31 mm2. The collection
method was not formally tested for reproducibility
because there were simply too many different combs,
tapes, clips, magnifying devices, marking pens, tem-
plates, stencils, bundling contraptions, etc., to be
evaluated. A standardized method for isolating the
hair sample from the 4-cm2 area (and immobilizing
the adjacent hair) has not been formalized at the
time of this publication. It should be pointed out
that the 4–cm2 site may be the shape of a triangle,
rectangle, or hexagon and is not limited to a
2� 2-cm square.
Several other issues needed to be addressed. Should
the hair be wet or dry? It was easier to gather a
sample with precise margins on the 2�2-cm square
if the hair was wet. Wet hair measurements were
performed in a salon setting where each client almost
always presented to the operator immediately fol-
lowing a shampoo. Almost all the samples gathered
in the physician’s office were performed on dry hair.
In both situations, a fine-toothed comb, 2.5�
magnifying loupes, and a sharp wooden toothpick
were used. The easiest method of demarcating the
2� 2-cm area was marking dots with a four-legged
or eight-legged template moistened on a pad of wa-
terproof ink. Stencils with four and eight holes were
also used to place the dots on the scalp skin surface.
When wet hair was combed away from the 2� 2-cm
square of scalp, it remained immobilized and firmly
in place. When the sampling was performed on dry
hair, the peripheral hair required immobilization
with hair clips or gummed tape. Several methods of
demarcating the area, without placing any ink marks
on the skin, have since been developed and will be
the subject of a future report.
The second sampling issue to be addressed was re-
turning to precisely the same site for a subsequent
measurement. Typically, when industry standard hair
counts and hair weight measurements are performed,
dots are tattooed on the scalp to identify the previous
test site. Tattoos were performed on several patients,
although our goal was to design a method that
would not require a permanent tattoo. Initially we
used a quick and easy method of simply extending a
nonstretchable 4-mm tape from the junction of the
upper lip and nose columella, on to and over the tip
of the nose, then up the forehead and along the
midline of the scalp along which the hair was cleanly
parted. An ink dot was simultaneously placed on the
tape and the scalp. The tape was removed and the
distance between the two points on the tape was
measured with a ruler attached to a tabletop. How-
ever, vertical movement of nose tip caused a 5- to 7-
mm variation in the anterior to posterior dot
placement.
The movement from side to side was considered less
critical when returning to the exact same site because
the gradation of hair loss in a balding individual is
much greater along the sagittal axis than the coronal
axis. Several methods and devices that enable a re-
turn to precisely the same area, without skin mark-
ing, have since been developed and will be the
subject of a future report.
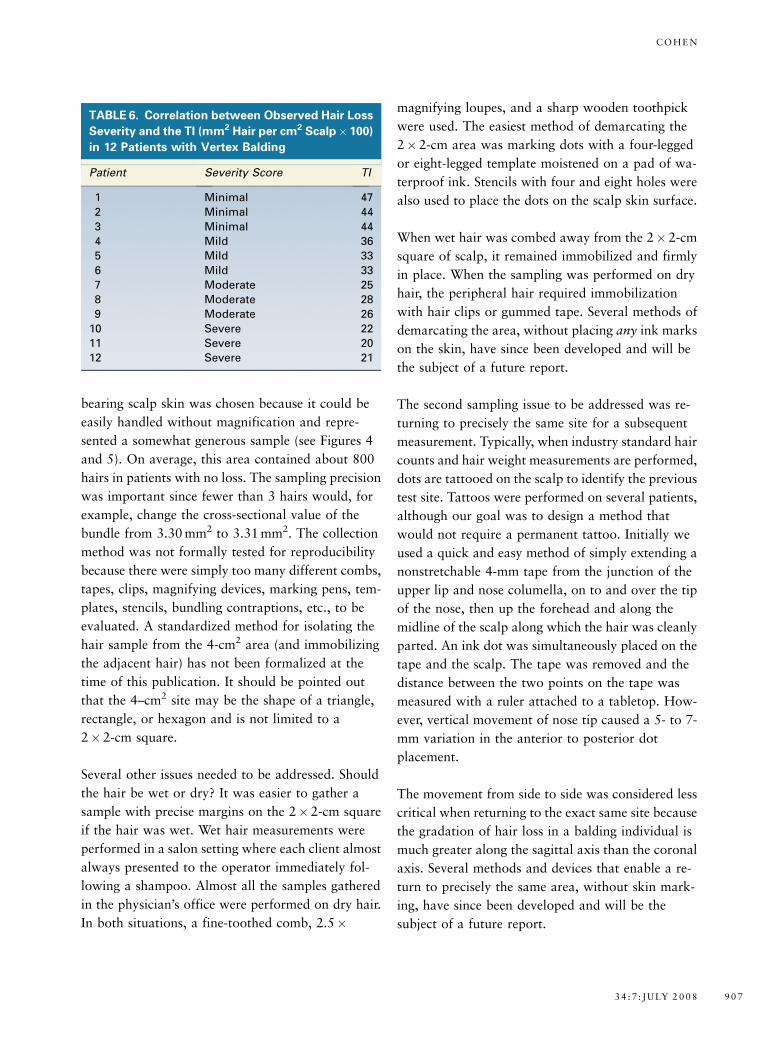
TABLE 6. Correlation between Observed Hair Loss
Severity and the TI (mm2 Hair per cm2 Scalp� 100)
in 12 Patients with Vertex Balding
Patient Severity Score TI
1 Minimal 47
2 Minimal 44
3 Minimal 44
4 Mild 36
5 Mild 33
6 Mild 33
7 Moderate 25
8 Moderate 28
9 Moderate 26
10 Severe 22
11 Severe 20
12 Severe 21
3 4 : 7 : J U LY 2 0 0 8 9 0 7
C O H E N

It is important to note that the sampled hair must be
a minimum of 1 inch (2.5 cm) in length at time of
testing. If not, the distance between the scalp surface,
the hook/anvil will be too small; and the hair might
be painfully tugged when the device is fully engaged.
Furthermore, if one anticipates newly emerging
hairs, be aware that the new hairs might not be of
sufficient length for capture. If the hair is too short,
the testing should be postponed until it has grown to
adequate length. If a clinical trial is being performed,
one should consider the time frame for anticipated
emergence of new hairs and their rate of growth.
Dates for retesting should be appropriately planned.
At first we assumed that the quantity of hair in
normal individuals was evenly distributed over the
entire scalp. We also assumed that in women with
telogen effluvium, diffuse hair loss, or sheddingF
the loss was evenly distributed over the entire surface
of the scalp. During the pilot studies, it was clear
that neither of these assumptions were correct.
A significant number of patients with no complaints
of hair loss had values higher on the top of the head
than in the occipital region. The same unexpected
distribution pattern was seen in women with com-
plaints of excessive shedding. Further search of the
literature revealed that the hair density changes
dramatically with age and that density is in fact
unequally distributed over the scalp, often highest on
the top of the head.10,11 These observations are sig-
nificant if one compares the occipital and midscalp
values when attempting to distinguish between
diffuse and pattern loss in women with complaints of
hair loss.
Conclusions and Discussion
The method/device described in this report is a me-
chanical refinement of the author’s previous pub-
lished HLSS.3 When using the HLSS, the observer is
asked to determine the ratio of grossly visible hair to
grossly visible skin. A series of photographs give
examples of the categories to be chosen. The
trichometer device/method described in this report
likewise compares the ratio of hair to skin, but uses
direct mechanical measurement of the hair and skin
cross-sections instead of imprecise visual determi-
nation. The HLSS method was used to determine the
correlation between hair loss severity and bundle
cross-sectional area (see Table 6 and Figure 6).
The notion of using an instrument to measure the
cross-sectional ratio of hair to skin, for the purpose
of measuring the quantity of hair, has been previ-
ously described. To the best of our knowledge, it was
first described in a 1936 patent by Nessler,12 who
designed a rudimentary device with a rectangular
slot for capturing hair and then hand-compressed the
hair with a blunt, guillotine-like anvil. The height of
the hair in the slot was measured using ruler-like
markings engraved on the side of the brass hand-held
device. The Nessler device appears to have never
gained popularity and no references could be found
in the medical literature.
In 2001, Arnold13 formally presented a method for
measuring the quantity of hair in a premeasured area
of scalp. Although the work was not published, Ar-
nold deserves full credit for introducing the concept
of measuring hair quantity using hair/skin cross-
sectional ratio to the hair science community. Ar-
nold’s work served as the inspiration for the method/
device described in this report.
Arnold isolated the hair from a premeasured area of
scalp, but he chose to measure the hair bundle using
a thread wrapped snugly around the bundle’s pe-
riphery. An ink mark was made on the circumfe-
rentially applied loop of thread at the point where
the strand crossed over itself. The thread was then
removed and stretched out, and the distance between
the two marks was measured. Arnold had measured
the circumference of the bundle and called this value
the hair mass index. Neidel and Bretschneider14 have
described and published the details of Arnold’s hair
mass measurement technique.
Nessler and Arnold did not standardize the load
applied to the bundle or control its application with
a mechanical apparatus. Because the bundle of hair
D E R M AT O L O G I C S U R G E RY9 0 8
T H E C R O S S - S E C T I O N T R I C H O M E T E R

is soft and quite compressible, the variability of their
load and their method of application introduced
significant imprecision. Nessler’s ruler and Arnold’s
measuring thread technique were significantly im-
precise as well. The methods of Nessler, Arnold,
Hamilton-Norwood, Ludwig, and Cohen (HLSS) are
all imprecise and not suitable for scientific studies,
and although hair weight measurement, global pho-
tography, and hair counts are precise, and suitable
for scientific studies, they too have the following
limitations as mentioned in Table 1.
Global photography requires special equipment and
hairstyle conformity. It is designed to compare the
relative difference between the before and after ap-
pearance of a single patient. It does not generate a
single quantitative value for a localized area of the
scalp. Hair counts on the other hand do generate a
single quantitative value but the value does not re-
flect the wide variation of diameters seen in condi-
tions of thinning, i.e., androgenetic alopecia. Hair
weight measurement, the gold standard, is simply
too difficult and time-consuming to perform as an
office procedure, and hair weight, hair counts, and
Trichoscan all require that hair be cut. The tricho-
meter technology overcomes many of these limita-
tions and generates a value that simultaneously
reflects the influence of density and diameter alone.
Preliminary study results, using both silk fibers and
hair, were the same. The incremental changes in the
filament number, filament diameter, and bundle
weight were reflected as equal and proportionate in-
cremental changes in the bundle cross-sectional area.
It was concluded that the device could be used as a
reliable substitute for every instrument and method
that is presently used to measure the parameters of
hair loss and growth, including the dry hair weight
measurementFthe industry gold standard.
Although the device itself showed a high degree of
precision, it should be emphasized that the accuracy
and reproducibility of the measurements can be
compromised if the sampling method is not carefully
performed using magnification. Returning to the
same area for retesting without using a tattoo com-
promises the measurements as well. Both of these
issues will be the subject of a subsequent report.
The general availability of a simple hair-measuring
technology introduces a number of possibilities (see
Table 7). Any clinical condition characterized by
shedding and/or thinning could be informally quan-
tified and tracked. A patient’s hair growth response
to minoxidil, finasteride, and iron supplement could
be easily measured. The efficacy of popular modal-
ities like low-intensity laser, biotin, and saw pal-
metto could be informally determined by practicing
physicians. Unsubstantiated anecdotes could be
challenged, and hair growth scams revealed.
Hundreds of common drugs, prescription and over
the counter, are known to cause hair loss. These
include retinoids, anticoagulants, cholesterol-lower-
ing agents, anticonvulsants, antidepressants, gastric
TABLE 7. Possible Applications of the Trich-
ometer Technology
1. Quantify hair mass in a localized area of
thinning and/or shedding
2. Quantify the efficacy of proven and unproven
hair growth products and devices
3. Quantify the medical treatment response in
thyroid disease, iron deficiency, etc.
4. Quantify the results of hair transplantation
surgery
5. Quantify the donor hair available for hair
transplantation surgery15
6. Detect the reversal and recovery from post
partum effluvium
7. Detect balding before it is visible
8. Determine a new drug’s potential for causing
hair loss
9. Determine the incidence of hair loss caused by
FDA-approved drugs
10. Provide a simple 1–100 scoring system for hair
loss
11. Provide a new measuring modality for hair
science research
12. Enable the office physician to track and mea-
sure a patient’s clinical status
13. Improve and simplify communication between
hair professionals
FDA, Food and Drug Administration.
3 4 : 7 : J U LY 2 0 0 8 9 0 9
C O H E N

acidity suppressants, cardiac arrhythmia and anti-
hypertensive agents, anti-inflammatory agents, hor-
mones, and weight reduction drugs . . . plus the
entire category of antineoplastic agents. Patients
taking these drugs could be evaluated to determine
the incidence and magnitude of their hair loss. New
drugs could be screened, before FDA approval, to
determine if they have the potential side effect of
causing hair loss.
Marritt observed that a man must lose 50% of his
hair mass before the loss can be seen with the naked
eye.16 This was confirmed in Table 6. The TI’s of
men with minimal hair loss were about 50% lower
than the TI’s of men with no loss at all. (Normal
range for TI is 75 to 100 plus.) Logically, the
trichometer might be used to identify men in very
early stages of balding, when diameter reduction
silently precedes visible loss. By measuring and
comparing the frontal and occipital regions of men
with normal-appearing hair, a loss as small as 5 or
10% could be detected y perhaps 10 or 15 years
before balding was actually visible. The speed of
progression and response to treatment could be
easily monitored.
References
1. Hamilton JB. Patterned loss of hair in men; types and incidence.
Ann NY Acad Sci 1951;53:708–28.
2. Norwood OT. Male pattern baldness: classification and incidence.
South Med J 1975;68:1359–65.
3. Cohen BH. Hair loss profile, index, and severity scale. In: Haber
R, Stough D, editors. Hair Transplantation. Philadelphia: Elsevier;
2006. p. 12.
4. Canfield D. Photographic documentation of hair growth in
androgenetic alopecia. Dermatol Clin 1996;14:713–21.
5. Price VH, Menefee E, Strauss PC. Changes in hair weight and
hair count in men with androgenetic alopecia, after application
of 5% and 2% topical minoxidil, placebo, or no treatment.
J Am Acad Dermatol 1999;11:41.
6. Van Neste D, Dumrotier M, De Coster W. Phototrichogram
analysis: technical aspects and problems in relation with
automated quantitative evaluation of hair growth by computer-
assisted image analysis. In: Van Neste D, Lachapelle JM, Antoine
JL, editors. Trends in human hair growth and alopecia research.
Dordrecht: Kluwer (Amsterdam); 1989. p. 155–65.
7. Hoffman R. TrichoScan: combining epiluminescence microscopy
with digital image analysis for the measurement of hair growth.
Eur J Dermatol 2001;11:362–8.
8. Headington J. Transverse microscopic anatomy of the human
scalp: a basis for a morphometric approach to disorders of the hair
follicle. Arch Dermatol 1984;120:449–56.
9. Barth JH, Rushton DH. Measurement of hair growth. In: Serud J,
Jemec G, editors. Non-invasive methods and the skin. Ann Arbor:
CRP Press; 1995. p. 543–8.
10. Olsen EA, Canfield D. Age-related changes in scalp hair density.
Tokyo: European Hair Research Society; 2001.
11. Van Neste D. Female patients complaining about hair loss:
documentation of defective scalp hair dynamics with contrast-
enhanced phototrichogram. Skin Res Technol 2006;5:83–8.
12. Nessler C. Means for ascertaining the hair production of a
subject. US Patent 1,962,518, United States Patent Office, June
12, 1934.
13. Arnold J. Hair mass index, 4th Annual Congress European
Society of Hair Restoration Surgery. Barcelona, 2001.
14. Neidel FG, Bretschneider P. Measuring hair mass. In: Unger W,
Shapiro R, editors. Hair Transplantation. New York: Marcel
Dekker; 2004. p. 876.
15. Parsley W. Donor site measurement. In: Haber R, Stough D,
editors. Hair Transplantation. Philadelphia: Elsevier; 2006.
p. 101.
16. Marritt E. The death of the density debate. Dermatol Surg
1999;5:654–60.
Address correspondence and reprint requests to: BernardCohen, MD, 4425 Ponce de Leon Boulevard, Suite 230,Coral Gables, FL 33145, or e-mail: [email protected]
COMMENTARY
The current standards for measuring hair loss and hair growth are laden with problems and inefficiencies.
The ongoing search for a simple and accurate method of measuring hair quantity has finally found respite
in a novel device recently christened the cross-section trichometer. This device, developed by Dr. Bernie
Cohen, is featured in this issue of Dermatologic Surgery. As Dr. Cohen has quoted many times, ‘‘Medicine
is a language of numbers. Simple numbers are used to make a diagnosis like hypertension, diabetes, fever,
D E R M AT O L O G I C S U R G E RY9 1 0
T H E C R O S S - S E C T I O N T R I C H O M E T E R

and obesity. In fact, it’s the manipulation of these numbers that determines the manner by which we treat
these disorders. In simple terms, if it can’t be measured, it can’t be managed.’’
The challenge when evaluating all hair growth drugs is obtaining consistent methodology for measure-
ment. In the past, global photography has been utilized to document the overall change in the appearance
of hair from a baseline setting. Using serial global photographs, subjects were classified into distinct
categories, i.e., (1) greatly decreased in appearance, (2) slight decrease in appearance, (3) no change in
appearance, (4) slight increase in appearance, (5) moderate increase in appearance, and (6) great increase
in appearance. Unfortunately, the results are influenced by the F-stop settings on the camera.
Additionally, the lighting, film quality, grooming practices, and length of hair must be kept identical to the
original baseline photography or an erroneous change of appearance results. Keeping all of the above
factors constant is daunting and often not feasible. Global photography is a very crude and often in-
accurate method of assessing hair quantity in terms of both loss and growth. Global photography cannot
properly reflect changes in hair counts. To assess changes in hair counts, microphotographic techniques
are utilized. These techniques involve computer overlay in comparison to baseline photographs. The
addition of or loss of hairs is determined by a numerical value generated by the computer when comparing
photographs. This seems to be a more precise method, but fails to account for the changes in hair shaft
diameter, which often show the visible results.
Since the positive effect of minoxidil and 5a-reductase inhibitors (finasteride and dutasteride) use is in part
due to changes in hair shaft; the hair counts may be minimally affected. In other words, a positive effect
may be observed in a study patient by global photography with no change over baseline in actual hair
count. It is obvious from the above that our current methods are inadequate in providing a precise change
in hair mass. Dr. Cohen’s device offers a solution. When it is applied to a bundle of hair, any change in
density and diameter will be evident and measured numerically.
The article presented herein by Dr. Cohen is well written and deserves the attention of those involved in
hair research, clinical evaluations of hair disorders, and practicing hair transplant surgeons. It is not
unreasonable to project that at some point in the future residents in dermatology will utilize a device such
as the cross-section trichometer to routinely evaluate the success or failure of hair loss treatments in their
clinical patients. Practitioners look forward to this device being available to use on their patients. It will be
important for clinicians to produce the same, reproducible accurate results as presented in this article.
Dr. Cohen is to be applauded for both his success in bringing this to the field and his contributions in
advancing hair research.
DOW STOUGH, MD
Hot Springs, AR
3 4 : 7 : J U LY 2 0 0 8 9 1 1
C O H E N