the clinical characteristics of unipolar vs. bipolar major depression in adhd youth
TRANSCRIPT
www.elsevier.com/locate/jad
Journal of Affective Disorde
Research report
The clinical characteristics of unipolar vs. bipolar major
depression in ADHD youthB
Janet Wozniak*, Thomas Spencer, Joseph Biederman, Anne Kwon,
Michael Monuteaux, Jeffrey Rettew, Kathryn Lail
Pediatric Psychopharmacology Research Unit, Massachusetts General Hospital, Harvard Medical School, Boston, MA, United States
Received 8 September 2003; accepted 19 May 2004
Abstract
Objective: To investigate the characteristics of unipolar vs. bipolar depression in youth using a sample of children referred for a
study on attention deficit hyperactivity disorder (ADHD).
Methods: We compared children with unipolar depression (N=109) to those with bipolar depression (N=43) using boys and girls
(N=280) referred for a study on ADHD. Comparisons were made in characteristics of depression, comorbidity and family
history. All diagnoses were made using the KSADS-E.
Results: In comparison to children with unipolar depression, children with bipolar depression were more likely to have met
criteria for depression due to both bsadQ and bmadQ mood states as stated in the KSADS-E, have severe depression with
suicidality, anhedonia and hopelessness. Children with bipolar depression were more likely to have comorbid conduct disorder,
severe oppositional defiant disorder, agoraphobia, obsessive compulsive disorder and alcohol abuse, compared to children with
unipolar depression. Bipolar depressed children had lower GAF scores and higher rates of hospitalization. Bipolar depression is
associated with higher levels of psychiatric disorders in first-degree relatives.
Conclusions: In youth, bipolar depression is distinct from unipolar depression in quality and severity of symptoms, comorbidity
and family history. This presentation can aid clinicians in identifying children and adolescents with bipolar disorder.
D 2004 Elsevier B.V. All rights reserved.
0165-0327/$ - see front matter D 2004 Elsevier B.V. All rights reserved.
doi:10.1016/j.jad.2004.05.013
B Supported by the Johnson and Johnson Pediatric Psycho-
pharmacology Research Center at Massachusetts General Hospital.
* Corresponding author. Massachusetts General Hospital ACC
725, Boston, MA 02114, United States. Tel.: +1 617 724 5600; fax:
+1 617 503 1060.
E-mail address: [email protected] (J. Wozniak).
1. Introduction
When a child or adolescent presents with a severe
disturbance of mood, both unipolar major depression
(MDD) and bipolar disorder should be considered in
the differential diagnosis. While mania and depression
can be distinguished from each other, differentiating
between unipolar and bipolar forms of depression
poses unique clinical and therapeutic challenges.
rs 82S (2004) S59–S69

J. Wozniak et al. / Journal of Affective Disorders 82S (2004) S59–S69S60
Although a few studies suggest that childhood onset
MDD is associated with the development of bipolar
disorder, questions remain as to which clinical
characteristics of MDD should alert clinicians to the
likelihood of a bipolar disorder clinical picture. As the
use of antidepressants may precipitate manic symp-
toms when used for bipolar depression, differentiating
unipolar from bipolar depression is of high clinical
relevance.
In a prospective longitudinal study of 60 hospi-
talized, depressed adolescents aged 13–16 years,
Strober et al. (1993) found that 20% switched to
bipolar disorder at 3–4-year follow-up and was
predicted by the rapid onset of depressive symptoms,
psychomotor retardation, mood-congruent psychotic
features, a family history of bipolar illness and a
history of pharmacologically induced hypomania.
Geller et al. (1994, 2001) followed-up 79 children
(80% prepubertal) with major depression and found
that 32% switched to mania by an average age of 11
years and 50% by the age of 21 years and the conduct
disorder symptom of bullying and family history were
predictors of switching. Luby and Mrakotsky (2003)
found early risk factors for switching to mania in a
group of depressed preschoolers. These authors
concluded that increased rates of restlessness in the
depressed preschoolers with a family history of
bipolar disorder may represent a precursor of bipolar
disorder. Taken together, these findings suggest that
juvenile MDD especially with a family history of
bipolar disorder is strongly associated with the
development of later mania.
The identification of characteristics of pediatric
depression that could predict the presence of manic
episodes is of high clinical importance. In a natural-
istic chart review by Biederman et al. (2000), these
authors found that prescribing an antidepressant to a
child with mania results in manic exacerbation, but in
addition prescribing an antidepressant to a child with
an earlier, distant history of mania also results in
manic exacerbation. Given concerns that the treat-
ments for depression may exacerbate bipolar disorder
in children with bipolar depression, early recognition
of bipolar depression can aid clinicians in the
management of such patients.
To this end, this study investigated whether
unipolar and bipolar depression in youth can be
distinguished from each other in terms of clinical
features and correlates. Based on the literature, we
hypothesized that bipolar depression as compared to
unipolar depression would be characterized by earlier
onset, family history of bipolar disorder and comor-
bidity, especially with conduct disorder. To our
knowledge, this effort represents the most compre-
hensive evaluation of this subject.
2. Methods
Study subjects were children and adolescents with
major depression, stratified by the presence or absence
of bipolar disorder. Controls without depression or
bipolar disorder were included in some analyses for
comparative purposes. All youth had been diagnosed
with ADHD and had been referred for a family
genetic study of ADHD, which is described in
previous publications (Biederman et al., 1992; Bieder-
man et al., 1996; Biederman et al., 1999; Faraone et
al., 1993; Faraone et al., 2000). These youth were all
index cases of ADHD (probands), and were com-
prised of Caucasian, non-Hispanic males (N=140) and
females (N=140) between the ages of 6 and 17 years.
Referrals were obtained from two independent sour-
ces, psychiatrists and pediatricians. Psychiatrically
referred probands with ADHD were obtained through
consecutive referrals to the Pediatric Psychopharma-
cology Clinic at the Massachusetts General Hospital
(MGH), Boston. Pediatrically referred probands con-
sisted of pediatric patients from the Harvard Com-
munity Health Plan, a large health maintenance
organization (HMO).
Potential probands were excluded if they had been
adopted or if their nuclear family was unavailable for
study. We also excluded probands if they had major
sensorimotor handicaps (e.g., paralysis, deafness,
blindness), psychosis, autism or a Full-Scale IQ less
than 80. All of the probands with ADHD met
diagnostic criteria for current ADHD when clinically
referred. All subjects gave written informed consent
prior to enrollment in the study.
All diagnostic assessments were made using DSM-
III-R-based structured interviews. Psychiatric assess-
ments of probands and siblings were made with the
childhood version of the Schedule for Affective
Disorders and Schizophrenia, Epidemiologic version
(Kiddie-SADS-E) (Orvaschel and Puig-Antich, 1987).

J. Wozniak et al. / Journal of Affective Disorders 82S (2004) S59–S69 S61
Diagnoses were based on independent interviews with
the mothers and direct interviews of probands and
siblings, except for children younger than 12 years,
who were not directly interviewed. Psychiatric assess-
ments of parents and adult siblings were made using
the Structured Clinical Interview for DSM-III-R
(SCID) (Spitzer et al., 1990). For every diagnosis,
information was also gathered regarding the ages at
onset and offset of symptoms, number of episodes and
treatment history.
Interviews were conducted by raters with under-
graduate degrees in psychology who had been trained
to high levels of interrater reliability. We computed jcoefficients of agreement by having three experi-
enced, board-certified child and adult psychiatrists
diagnose subjects from audiotaped interviews made
by the assessment staff. Based on 175 interviews, all
disorders achieved j’s higher than 0.82. The mean jwas 0.90. We attained a j of 1.0 for ADHD and 0.91
for BPD. The reliability of maternal reports of these
disorders over a 1-year period was also high, with j’sfor ADHD and BPD being 0.95 and 0.71 (Faraone et
al., 1995).
All diagnoses were reviewed blindly by a diag-
nostic sign-off committee chaired by the service chief
(JB) who reviewed both the items endorsed during the
interview along with detailed notes taken by the
interviewer. Diagnoses of depression and mania
underwent extensive review. Diagnoses presented
for review were considered positive only if a con-
sensus was achieved that criteria were met to a degree
that would be considered clinically meaningful. By
bclinically meaningfulQ, we mean that the data
collected from the structured interview indicated that
the diagnosis should be a clinical concern due to the
nature of the symptoms, the associated impairment
and the coherence of the clinical picture. Because the
anxiety disorders compose many syndromes with a
wide range of severity, we also report results for two
or more anxiety disorders to index the presence of a
clinically meaningful anxiety syndrome. For children
older than 12 years, data from direct and indirect
interviews were combined by considering a diagnos-
tic criterion positive if it was endorsed in either
interview. Since the structured interviews generate
diagnostic information about both past and current
disturbances, the rates of illness reported herein are
lifetime prevalences.
Families were considered intact if there was no
divorce or separation in the proband’s family of origin.
Socioeconomic status was assessed with the Hollings-
head Four-Factor Index of Social Status (Hollings-
head, 1975), which uses parental education and
occupation to determine a family’s composite social
status. We also obtained information regarding cog-
nitive functioning using subtests from the Wechsler
Intelligence Scale for Children (WISC-R) (Wechsler,
1991). To evaluate school functioning, we assessed
three straightforward indices of school failure, based
on parent reports: placement in special classes, in-
school tutoring and repeated grades. Psychosocial
functioning was assessed using the DSM-III-R Global
Assessment of Functioning (GAF: 0=worst to
90=best). Scores for the Social Adjustment Inventory
(SAICA) (John et al., 1987) were obtained (where
higher scores indicate poorer functioning).
2.1. Statistical analysis
Comparisons were made between three groups (all
with ADHD): subjects with MDD only (unipolar
depression), subjects with MDD who fulfilled criteria
for mania (bipolar depression) and control subjects
without depression or bipolar disorder. Logistic or
ordinary least squares regression models were used to
predict clinical outcomes. Pairwise comparisons
between groups were also conducted if omnibus tests
were found to be significant. Omnibus analyses were
adjusted for SES and family intactness, while unipolar
vs. bipolar depression comparisons were adjusted for
gender and family intactness. Two-tailed tests were
used and statistical significance was set at the 0.05
level for omnibus statistics and 0.01 level for pairwise
comparisons.
3. Results
The three groups for comparison were ADHD boys
and girls meeting KSADS-E structured interview
criteria for MDD, but not for mania (unipolar depres-
sion group, N=109), meeting criteria for MDD plus
mania (bipolar depression, N=43), and ADHD boys
and girls without MDD or mania (control, N=128). In
the bipolar depressed group, 55% had a mixed
presentation and others had a biphasic presentation.
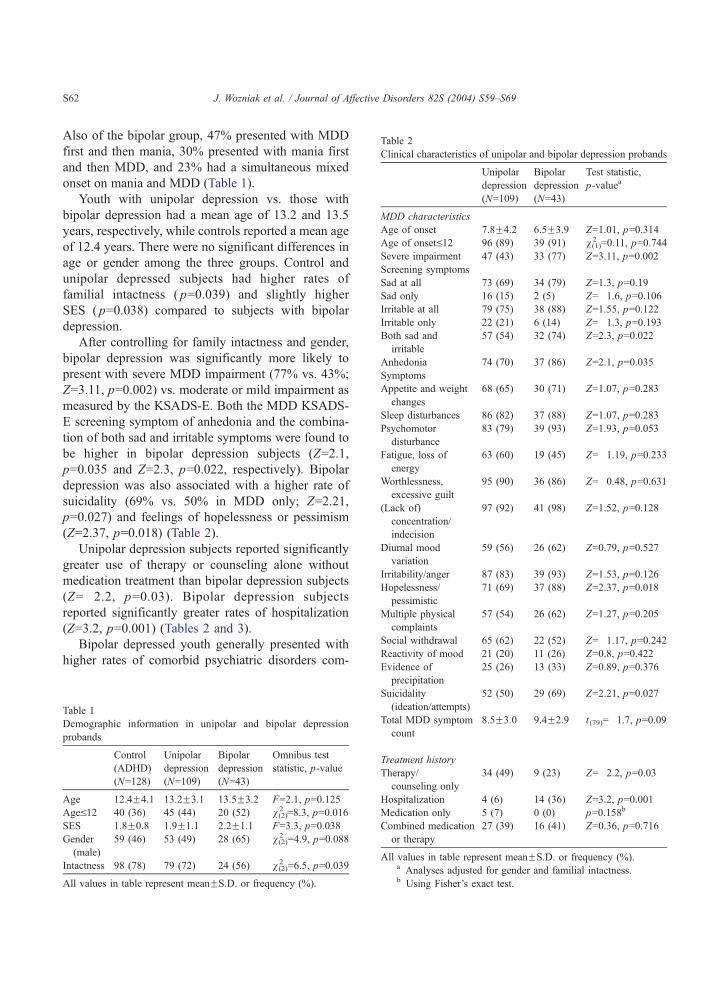
Table 2
Clinical characteristics of unipolar and bipolar depression probands
Unipolar
depression
(N=109)
Bipolar
depression
(N=43)
Test statistic,
p-valuea
MDD characteristics
Age of onset 7.8F4.2 6.5F3.9 Z=1.01, p=0.314
Age of onsetV12 96 (89) 39 (91) v(1)2 =0.11, p=0.744
Severe impairment 47 (43) 33 (77) Z=3.11, p=0.002
Screening symptoms
Sad at all 73 (69) 34 (79) Z=1.3, p=0.19
Sad only 16 (15) 2 (5) Z=�1.6, p=0.106
Irritable at all 79 (75) 38 (88) Z=1.55, p=0.122
Irritable only 22 (21) 6 (14) Z=�1.3, p=0.193
Both sad and
irritable
57 (54) 32 (74) Z=2.3, p=0.022
Anhedonia 74 (70) 37 (86) Z=2.1, p=0.035
Symptoms
Appetite and weight
changes
68 (65) 30 (71) Z=1.07, p=0.283
Sleep disturbances 86 (82) 37 (88) Z=1.07, p=0.283
Psychomotor
disturbance
83 (79) 39 (93) Z=1.93, p=0.053
Fatigue, loss of
energy
63 (60) 19 (45) Z=�1.19, p=0.233
Worthlessness,
excessive guilt
95 (90) 36 (86) Z=�0.48, p=0.631
(Lack of)
concentration/
indecision
97 (92) 41 (98) Z=1.52, p=0.128
Diurnal mood
variation
59 (56) 26 (62) Z=0.79, p=0.527
Irritability/anger 87 (83) 39 (93) Z=1.53, p=0.126
Hopelessness/
pessimistic
71 (69) 37 (88) Z=2.37, p=0.018
Multiple physical
complaints
57 (54) 26 (62) Z=1.27, p=0.205
Social withdrawal 65 (62) 22 (52) Z=�1.17, p=0.242
Reactivity of mood 21 (20) 11 (26) Z=0.8, p=0.422
Evidence of 25 (26) 13 (33) Z=0.89, p=0.376
J. Wozniak et al. / Journal of Affective Disorders 82S (2004) S59–S69S62
Also of the bipolar group, 47% presented with MDD
first and then mania, 30% presented with mania first
and then MDD, and 23% had a simultaneous mixed
onset on mania and MDD (Table 1).
Youth with unipolar depression vs. those with
bipolar depression had a mean age of 13.2 and 13.5
years, respectively, while controls reported a mean age
of 12.4 years. There were no significant differences in
age or gender among the three groups. Control and
unipolar depressed subjects had higher rates of
familial intactness ( p=0.039) and slightly higher
SES ( p=0.038) compared to subjects with bipolar
depression.
After controlling for family intactness and gender,
bipolar depression was significantly more likely to
present with severe MDD impairment (77% vs. 43%;
Z=3.11, p=0.002) vs. moderate or mild impairment as
measured by the KSADS-E. Both the MDD KSADS-
E screening symptom of anhedonia and the combina-
tion of both sad and irritable symptoms were found to
be higher in bipolar depression subjects (Z=2.1,
p=0.035 and Z=2.3, p=0.022, respectively). Bipolar
depression was also associated with a higher rate of
suicidality (69% vs. 50% in MDD only; Z=2.21,
p=0.027) and feelings of hopelessness or pessimism
(Z=2.37, p=0.018) (Table 2).
Unipolar depression subjects reported significantly
greater use of therapy or counseling alone without
medication treatment than bipolar depression subjects
(Z=�2.2, p=0.03). Bipolar depression subjects
reported significantly greater rates of hospitalization
(Z=3.2, p=0.001) (Tables 2 and 3).
Bipolar depressed youth generally presented with
higher rates of comorbid psychiatric disorders com-
precipitation
Suicidality
(ideation/attempts)
52 (50) 29 (69) Z=2.21, p=0.027
Total MDD symptom
count
8.5F3.0 9.4F2.9 t(79)=�1.7, p=0.09
Treatment history
Therapy/
counseling only
34 (49) 9 (23) Z=�2.2, p=0.03
Hospitalization 4 (6) 14 (36) Z=3.2, p=0.001
Medication only 5 (7) 0 (0) p=0.158b
Combined medication
or therapy
27 (39) 16 (41) Z=0.36, p=0.716
All values in table represent meanFS.D. or frequency (%).a Analyses adjusted for gender and familial intactness.b Using Fisher’s exact test.
Table 1
Demographic information in unipolar and bipolar depression
probands
Control
(ADHD)
(N=128)
Unipolar
depression
(N=109)
Bipolar
depression
(N=43)
Omnibus test
statistic, p-value
Age 12.4F4.1 13.2F3.1 13.5F3.2 F=2.1, p=0.125
AgeV12 40 (36) 45 (44) 20 (52) v(2)2 =8.3, p=0.016
SES 1.8F0.8 1.9F1.1 2.2F1.1 F=3.3, p=0.038
Gender
(male)
59 (46) 53 (49) 28 (65) v(2)2 =4.9, p=0.088
Intactness 98 (78) 79 (72) 24 (56) v(2)2 =6.5, p=0.039
All values in table represent meanFS.D. or frequency (%).
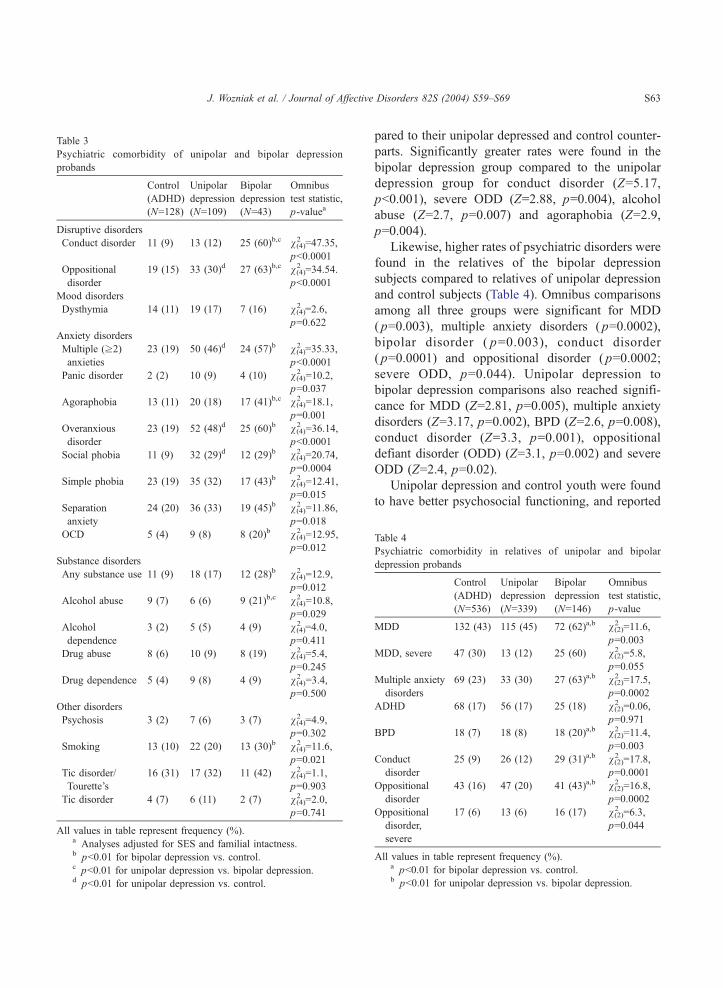
Table 3
Psychiatric comorbidity of unipolar and bipolar depression
probands
Control
(ADHD)
(N=128)
Unipolar
depression
(N=109)
Bipolar
depression
(N=43)
Omnibus
test statistic,
p-valuea
Disruptive disorders
Conduct disorder 11 (9) 13 (12) 25 (60)b,c v(4)2 =47.35,
pb0.0001
Oppositional
disorder
19 (15) 33 (30)d 27 (63)b,c v(4)2 =34.54.
pb0.0001
Mood disorders
Dysthymia 14 (11) 19 (17) 7 (16) v(4)2 =2.6,
p=0.622
Anxiety disorders
Multiple (z2)
anxieties
23 (19) 50 (46)d 24 (57)b v(4)2 =35.33,
pb0.0001
Panic disorder 2 (2) 10 (9) 4 (10) v(4)2 =10.2,
p=0.037
Agoraphobia 13 (11) 20 (18) 17 (41)b,c v(4)2 =18.1,
p=0.001
Overanxious
disorder
23 (19) 52 (48)d 25 (60)b v(4)2 =36.14,
pb0.0001
Social phobia 11 (9) 32 (29)d 12 (29)b v(4)2 =20.74,
p=0.0004
Simple phobia 23 (19) 35 (32) 17 (43)b v(4)2 =12.41,
p=0.015
Separation
anxiety
24 (20) 36 (33) 19 (45)b v(4)2 =11.86,
p=0.018
OCD 5 (4) 9 (8) 8 (20)b v(4)2 =12.95,
p=0.012
Substance disorders
Any substance use 11 (9) 18 (17) 12 (28)b v(4)2 =12.9,
p=0.012
Alcohol abuse 9 (7) 6 (6) 9 (21)b,c v(4)2 =10.8,
p=0.029
Alcohol
dependence
3 (2) 5 (5) 4 (9) v(4)2 =4.0,
p=0.411
Drug abuse 8 (6) 10 (9) 8 (19) v(4)2 =5.4,
p=0.245
Drug dependence 5 (4) 9 (8) 4 (9) v(4)2 =3.4,
p=0.500
Other disorders
Psychosis 3 (2) 7 (6) 3 (7) v(4)2 =4.9,
p=0.302
Smoking 13 (10) 22 (20) 13 (30)b v(4)2 =11.6,
p=0.021
Tic disorder/
Tourette’s
16 (31) 17 (32) 11 (42) v(4)2 =1.1,
p=0.903
Tic disorder 4 (7) 6 (11) 2 (7) v(4)2 =2.0,
p=0.741
All values in table represent frequency (%).a Analyses adjusted for SES and familial intactness.b pb0.01 for bipolar depression vs. control.c pb0.01 for unipolar depression vs. bipolar depression.d pb0.01 for unipolar depression vs. control.
J. Wozniak et al. / Journal of Affective Disorders 82S (2004) S59–S69 S63
pared to their unipolar depressed and control counter-
parts. Significantly greater rates were found in the
bipolar depression group compared to the unipolar
depression group for conduct disorder (Z=5.17,
pb0.001), severe ODD (Z=2.88, p=0.004), alcohol
abuse (Z=2.7, p=0.007) and agoraphobia (Z=2.9,
p=0.004).
Likewise, higher rates of psychiatric disorders were
found in the relatives of the bipolar depression
subjects compared to relatives of unipolar depression
and control subjects (Table 4). Omnibus comparisons
among all three groups were significant for MDD
( p=0.003), multiple anxiety disorders ( p=0.0002),
bipolar disorder ( p=0.003), conduct disorder
( p=0.0001) and oppositional disorder ( p=0.0002;
severe ODD, p=0.044). Unipolar depression to
bipolar depression comparisons also reached signifi-
cance for MDD (Z=2.81, p=0.005), multiple anxiety
disorders (Z=3.17, p=0.002), BPD (Z=2.6, p=0.008),
conduct disorder (Z=3.3, p=0.001), oppositional
defiant disorder (ODD) (Z=3.1, p=0.002) and severe
ODD (Z=2.4, p=0.02).
Unipolar depression and control youth were found
to have better psychosocial functioning, and reported
Table 4
Psychiatric comorbidity in relatives of unipolar and bipolar
depression probands
Control
(ADHD)
(N=536)
Unipolar
depression
(N=339)
Bipolar
depression
(N=146)
Omnibus
test statistic,
p-value
MDD 132 (43) 115 (45) 72 (62)a,b v(2)2 =11.6,
p=0.003
MDD, severe 47 (30) 13 (12) 25 (60) v(2)2 =5.8,
p=0.055
Multiple anxiety
disorders
69 (23) 33 (30) 27 (63)a,b v(2)2 =17.5,
p=0.0002
ADHD 68 (17) 56 (17) 25 (18) v(2)2 =0.06,
p=0.971
BPD 18 (7) 18 (8) 18 (20)a,b v(2)2 =11.4,
p=0.003
Conduct
disorder
25 (9) 26 (12) 29 (31)a,b v(2)2 =17.8,
p=0.0001
Oppositional
disorder
43 (16) 47 (20) 41 (43)a,b v(2)2 =16.8,
p=0.0002
Oppositional
disorder,
severe
17 (6) 13 (6) 16 (17) v(2)2 =6.3,
p=0.044
All values in table represent frequency (%).a pb0.01 for bipolar depression vs. control.b pb0.01 for unipolar depression vs. bipolar depression.
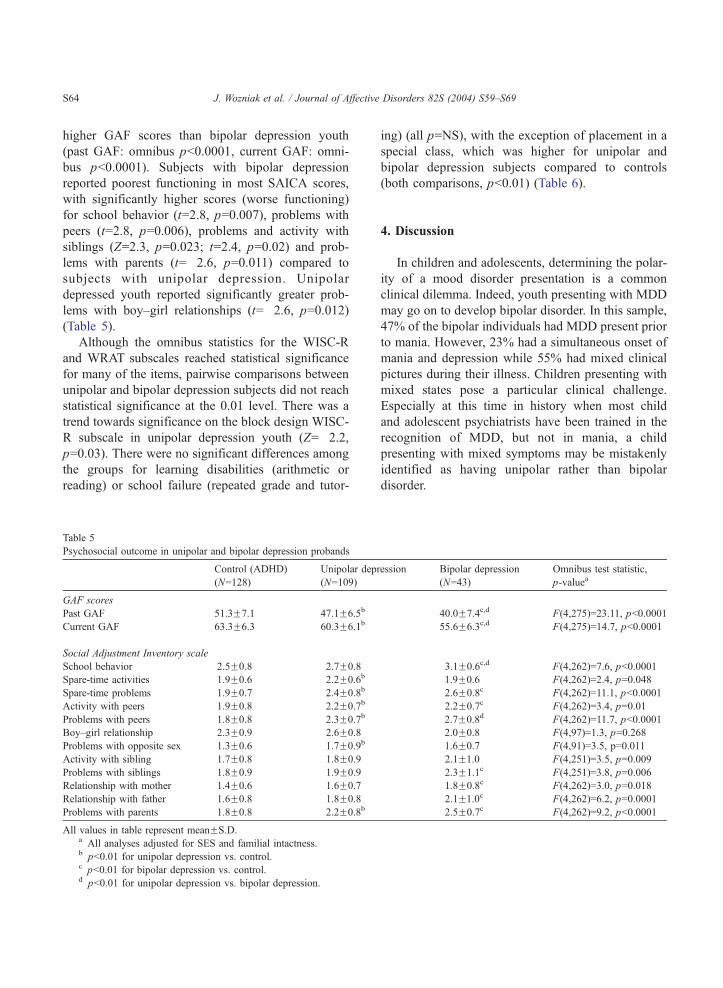
J. Wozniak et al. / Journal of Affective Disorders 82S (2004) S59–S69S64
higher GAF scores than bipolar depression youth
(past GAF: omnibus pb0.0001, current GAF: omni-
bus pb0.0001). Subjects with bipolar depression
reported poorest functioning in most SAICA scores,
with significantly higher scores (worse functioning)
for school behavior (t=2.8, p=0.007), problems with
peers (t=2.8, p=0.006), problems and activity with
siblings (Z=2.3, p=0.023; t=2.4, p=0.02) and prob-
lems with parents (t=�2.6, p=0.011) compared to
subjects with unipolar depression. Unipolar
depressed youth reported significantly greater prob-
lems with boy–girl relationships (t=�2.6, p=0.012)
(Table 5).
Although the omnibus statistics for the WISC-R
and WRAT subscales reached statistical significance
for many of the items, pairwise comparisons between
unipolar and bipolar depression subjects did not reach
statistical significance at the 0.01 level. There was a
trend towards significance on the block design WISC-
R subscale in unipolar depression youth (Z=�2.2,
p=0.03). There were no significant differences among
the groups for learning disabilities (arithmetic or
reading) or school failure (repeated grade and tutor-
Table 5
Psychosocial outcome in unipolar and bipolar depression probands
Control (ADHD)
(N=128)
Unipolar dep
(N=109)
GAF scores
Past GAF 51.3F7.1 47.1F6.5b
Current GAF 63.3F6.3 60.3F6.1b
Social Adjustment Inventory scale
School behavior 2.5F0.8 2.7F0.8
Spare-time activities 1.9F0.6 2.2F0.6b
Spare-time problems 1.9F0.7 2.4F0.8b
Activity with peers 1.9F0.8 2.2F0.7b
Problems with peers 1.8F0.8 2.3F0.7b
Boy–girl relationship 2.3F0.9 2.6F0.8
Problems with opposite sex 1.3F0.6 1.7F0.9b
Activity with sibling 1.7F0.8 1.8F0.9
Problems with siblings 1.8F0.9 1.9F0.9
Relationship with mother 1.4F0.6 1.6F0.7
Relationship with father 1.6F0.8 1.8F0.8
Problems with parents 1.8F0.8 2.2F0.8b
All values in table represent meanFS.D.a All analyses adjusted for SES and familial intactness.b pb0.01 for unipolar depression vs. control.c pb0.01 for bipolar depression vs. control.d pb0.01 for unipolar depression vs. bipolar depression.
ing) (all p=NS), with the exception of placement in a
special class, which was higher for unipolar and
bipolar depression subjects compared to controls
(both comparisons, pb0.01) (Table 6).
4. Discussion
In children and adolescents, determining the polar-
ity of a mood disorder presentation is a common
clinical dilemma. Indeed, youth presenting with MDD
may go on to develop bipolar disorder. In this sample,
47% of the bipolar individuals had MDD present prior
to mania. However, 23% had a simultaneous onset of
mania and depression while 55% had mixed clinical
pictures during their illness. Children presenting with
mixed states pose a particular clinical challenge.
Especially at this time in history when most child
and adolescent psychiatrists have been trained in the
recognition of MDD, but not in mania, a child
presenting with mixed symptoms may be mistakenly
identified as having unipolar rather than bipolar
disorder.
ression Bipolar depression
(N=43)
Omnibus test statistic,
p-valuea
40.0F7.4c,d F(4,275)=23.11, pb0.0001
55.6F6.3c,d F(4,275)=14.7, pb0.0001
3.1F0.6c,d F(4,262)=7.6, pb0.0001
1.9F0.6 F(4,262)=2.4, p=0.048
2.6F0.8c F(4,262)=11.1, pb0.0001
2.2F0.7c F(4,262)=3.4, p=0.01
2.7F0.8d F(4,262)=11.7, pb0.0001
2.0F0.8 F(4,97)=1.3, p=0.268
1.6F0.7 F(4,91)=3.5, p=0.011
2.1F1.0 F(4,251)=3.5, p=0.009
2.3F1.1c F(4,251)=3.8, p=0.006
1.8F0.8c F(4,262)=3.0, p=0.018
2.1F1.0c F(4,262)=6.2, p=0.0001
2.5F0.7c F(4,262)=9.2, pb0.0001
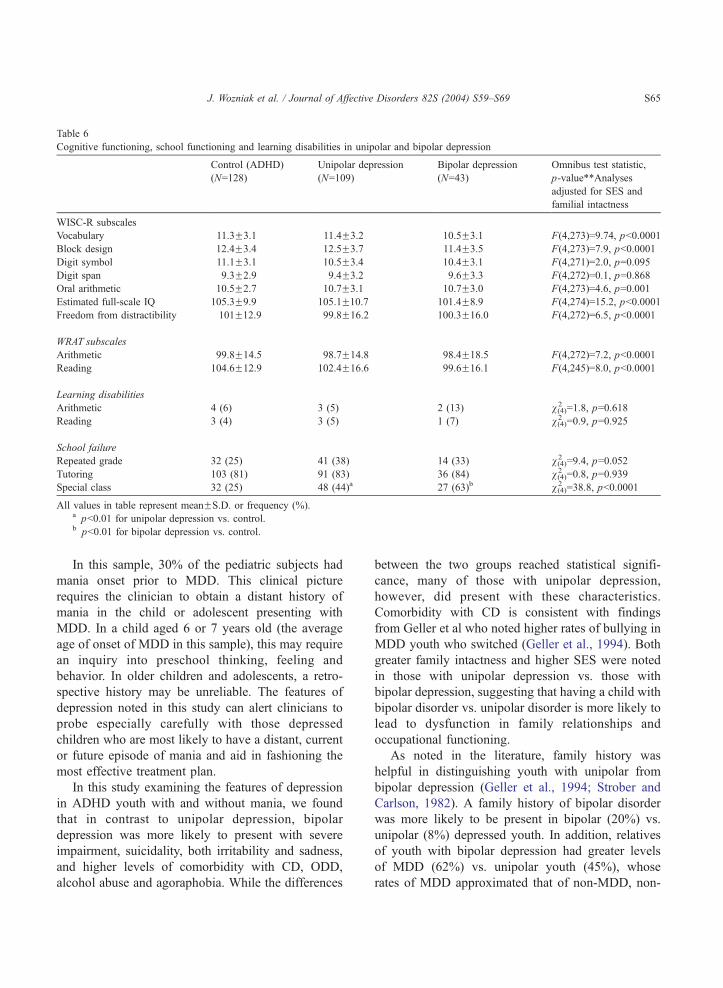
Table 6
Cognitive functioning, school functioning and learning disabilities in unipolar and bipolar depression
Control (ADHD)
(N=128)
Unipolar depression
(N=109)
Bipolar depression
(N=43)
Omnibus test statistic,
p-value**Analyses
adjusted for SES and
familial intactness
WISC-R subscales
Vocabulary 11.3F3.1 11.4F3.2 10.5F3.1 F(4,273)=9.74, pb0.0001
Block design 12.4F3.4 12.5F3.7 11.4F3.5 F(4,273)=7.9, pb0.0001
Digit symbol 11.1F3.1 10.5F3.4 10.4F3.1 F(4,271)=2.0, p=0.095
Digit span 9.3F2.9 9.4F3.2 9.6F3.3 F(4,272)=0.1, p=0.868
Oral arithmetic 10.5F2.7 10.7F3.1 10.7F3.0 F(4,273)=4.6, p=0.001
Estimated full-scale IQ 105.3F9.9 105.1F10.7 101.4F8.9 F(4,274)=15.2, pb0.0001
Freedom from distractibility 101F12.9 99.8F16.2 100.3F16.0 F(4,272)=6.5, pb0.0001
WRAT subscales
Arithmetic 99.8F14.5 98.7F14.8 98.4F18.5 F(4,272)=7.2, pb0.0001
Reading 104.6F12.9 102.4F16.6 99.6F16.1 F(4,245)=8.0, pb0.0001
Learning disabilities
Arithmetic 4 (6) 3 (5) 2 (13) v(4)2 =1.8, p=0.618
Reading 3 (4) 3 (5) 1 (7) v(4)2 =0.9, p=0.925
School failure
Repeated grade 32 (25) 41 (38) 14 (33) v(4)2 =9.4, p=0.052
Tutoring 103 (81) 91 (83) 36 (84) v(4)2 =0.8, p=0.939
Special class 32 (25) 48 (44)a 27 (63)b v(4)2 =38.8, pb0.0001
All values in table represent meanFS.D. or frequency (%).a pb0.01 for unipolar depression vs. control.b pb0.01 for bipolar depression vs. control.
J. Wozniak et al. / Journal of Affective Disorders 82S (2004) S59–S69 S65
In this sample, 30% of the pediatric subjects had
mania onset prior to MDD. This clinical picture
requires the clinician to obtain a distant history of
mania in the child or adolescent presenting with
MDD. In a child aged 6 or 7 years old (the average
age of onset of MDD in this sample), this may require
an inquiry into preschool thinking, feeling and
behavior. In older children and adolescents, a retro-
spective history may be unreliable. The features of
depression noted in this study can alert clinicians to
probe especially carefully with those depressed
children who are most likely to have a distant, current
or future episode of mania and aid in fashioning the
most effective treatment plan.
In this study examining the features of depression
in ADHD youth with and without mania, we found
that in contrast to unipolar depression, bipolar
depression was more likely to present with severe
impairment, suicidality, both irritability and sadness,
and higher levels of comorbidity with CD, ODD,
alcohol abuse and agoraphobia. While the differences
between the two groups reached statistical signifi-
cance, many of those with unipolar depression,
however, did present with these characteristics.
Comorbidity with CD is consistent with findings
from Geller et al who noted higher rates of bullying in
MDD youth who switched (Geller et al., 1994). Both
greater family intactness and higher SES were noted
in those with unipolar depression vs. those with
bipolar depression, suggesting that having a child with
bipolar disorder vs. unipolar disorder is more likely to
lead to dysfunction in family relationships and
occupational functioning.
As noted in the literature, family history was
helpful in distinguishing youth with unipolar from
bipolar depression (Geller et al., 1994; Strober and
Carlson, 1982). A family history of bipolar disorder
was more likely to be present in bipolar (20%) vs.
unipolar (8%) depressed youth. In addition, relatives
of youth with bipolar depression had greater levels
of MDD (62%) vs. unipolar youth (45%), whose
rates of MDD approximated that of non-MDD, non-

J. Wozniak et al. / Journal of Affective Disorders 82S (2004) S59–S69S66
BPD ADHD youth (43%). Relatives of youth with
bipolar depression also had higher rates of other
disorders when compared to relatives of youth with
unipolar depression including multiple anxiety dis-
orders (63% vs. 30%), CD (31% vs. 12%) and ODD
(43% vs. 20%). While work by Strober (1992) and
Strober et al. (1988) indicates that early onset bipolar
disorder carries with it a greater genetic loading for
bipolar disorder, little is written on the loading for
other disorders. Our study, consistent with an
emerging literature addressing the family genetics
of conditions which frequently present comorbidly
with pediatric bipolar disorder (Wozniak et al., 2001,
2002), not only finds high levels of bipolar disorder
in family members, but high levels of other
conditions as well when compared to relatives of
probands with unipolar depression. This finding
supports the concept of heterogeneity of bipolar
disorder with the pediatric onset form presenting
with distinct features, including a strong family
history of various psychiatric disorders.
In comparison to youth with unipolar depression,
youth with bipolar depression were more likely to
endorse both the sad and irritable screens (as opposed
to one or the other) on the KSADS structured
interview and require both medication treatment and
counseling (rather than counseling alone, which was
seen among more unipolar youth). Based on GAF
scores, hospitalization, KSADS severity rating and the
presence of suicidality, bipolar depression in youth
appears to present with much greater morbidity than
unipolar depression. This may not be surprising, as
manic states bring with them greater levels of
impulsivity and aggression, which could be directed
against the self as well as outward. However, the only
study to examine severity done with an adult
population, Mitchell et al. (2001) found no difference
in severity between unipolar and bipolar depression
based on Hamilton Rating Scale Score for Depression.
This may in part be due to the fact that the severity
outcome measure was limited to the Hamilton score
only and also that the sample included a large number
of subjects who were already hospitalized (and thus
more severely affected), whereas this sample is
entirely an outpatient sample. This may also indicate
that findings in adults regarding differences in
unipolar vs. bipolar depression cannot be extrapolated
to youth.
This study finds a higher rate of suicidality
(ideation and attempts) among youth with bipolar
depression than among youth with unipolar depres-
sion. This is consistent with findings from Brent et al.
(1988) who found that suicide victims (N=27)
compared to those with ideation or suicide attempt
(N=56) were more likely to suffer from bipolar
disorder with a trend toward higher comorbidity with
ADHD, a condition which combines mood instability
with high degrees of impulsivity. The finding of
higher levels of suicidality in those with bipolar
disorder is important from a clinical, scientific and
public health perspective. From a clinical perspective,
when evaluating children and adolescents for suicide
risk and the attendant need for precautions or
hospitalization, including questions regarding symp-
toms of mania may be important. From a public health
perspective, this finding could lead to more efficient
screening of children and adolescents at risk. From a
scientific standpoint, when evaluating the genetics of
suicide a possible link to bipolar disorder should be
explored.
While our study focused on a pediatric popula-
tion, Mitchell et al. (2001) compared clinical features
of depression in 39 matched pairs of inpatients and
outpatients adults meeting DSM IV criteria for
unipolar and bipolar depression. In this study, the
bipolar patients were more likely to have psycho-
motor-retarded melancholic features and atypical
depressive features (mood reactivity, reversed sleep
and appetite disturbances, psychomotor disturbance)
as well as previous episodes of psychotic depres-
sion. In contrast, our study of children and adolescents
did not find the atypical features of depression to
be useful in distinguishing unipolar from bipolar
depression.
One reason these findings may not extrapolate to
the pediatric population is the observation that child-
hood depression in general may be more likely to be
characterized by atypicality as compared to adult
depression, thus rendering this feature less useful in
distinguishing between unipolar and bipolar depres-
sion in youth. Consistent with this idea, in their study
of the characteristics of depressed youth who
switched, Geller et al. (1994) note that atypical
features of depression were not predictive of switch-
ing. While some studies of adults which compare
unipolar and bipolar depression have found lower age

J. Wozniak et al. / Journal of Affective Disorders 82S (2004) S59–S69 S67
at onset, more comorbidity and more atypical features
associated with bipolar depression, other studies find
few differences. (Goodwin and Jamison, 1990) Con-
flicting findings have been reported regarding the
presence or absence of psychomotor retardation and
agitation, suicidal behavior and chronic course
(Benazzi et al., 1999a,b, 2003; Kuhs and Reschke,
1992). In a study comparing psychotic bipolar and
unipolar depression, no differences in any of these
variables was found (Benazzi, 1999).
The findings from this study and others may be
useful to clinicians in the important clinical decision of
whether to use an antidepressant or a mood stabilizer
with an antidepressant in a child or adolescent
presenting with severe mood disturbance suggestive
of depression. Recent data suggesting that the anti-
depressant paroxetine should not be used in individuals
under the age of 18 due to increased suicidality only
highlights the importance of this issue (Waechter,
2003). Studies of adults with bipolar disorder have
begun to extensively examine the issue of the use of
antidepressants in bipolar individuals. Such studies
indicate that adult bipolar disorder is more likely to be
characterized by the depressive than the manic phase of
the illness (Altshuler et al., 2003a,b, 2002; Post et al.,
1977, 2001, 2003). Furthermore, these studies indicate
that the extended use of an antidepressant can treat the
depressive phase of the illness without exacerbating
mania in many individuals (Altshuler et al., 2003b).
The field awaits further studies which address whether
depression in youth with bipolar disorder can be
effectively treated without exacerbating mania.
In summary, although a few studies suggest that
childhood onset MDD is associated with the develop-
ment of bipolar disorder, questions remain as to which
clinical characteristics of depression should alert
clinicians to the likelihood of bipolar disorder. A
limitation of this study is that it is a cross-sectional
examination of the features of MDD in individuals
who have and have not already developed mania.
Therefore, it may assist in determining whether an
individual with MDD is unipolar or bipolar, but
whether the features described offer any predictive
value regarding switching is less certain. Because this
is an ADHD sample, differences in rates of ADHD
could not be examined between the groups with
unipolar and bipolar depression. However, as early
onset bipolar disorder is characterized by high rates of
comorbid ADHD, any bipolar sample is likely to have
high rates of ADHD. The universal presence of ADHD
in both the unipolar and bipolar groups may have
dampened our ability to detect differences in cognitive
and school functioning. As psychosis was an exclu-
sionary criteria in the original sample of ADHD
children, the reported rates of psychosis are lower
than would be anticipated. This exclusionary charac-
teristic of the sample also renders it impossible to test
the hypothesis that bipolar depression is more likely
than unipolar depression to be accompanied by mood-
congruent psychotic features (Strober et al., 1993).
Future work would benefit from examining unipolar
and bipolar depression in an unselected sample. As the
sample is young, not all individuals have passed
through the age of risk for developing bipolar disorder
and some portion of the unipolar group may actually
be bpre-bipolarQ.In addition, for this study, we have set the
statistical significance level at p=0.01, consistent with
a Bonferroni correction for pairwise comparisons. As
many statistical comparisons were made overall, the
possibility that our findings are due to chance alone
are increased. However, as this study is hypothesis
generating and represents the only such comparison of
its kind between unipolar and bipolar depression in
youth, we felt the findings are of clinical and research
interest nonetheless.
The symptoms found to differentiate bipolar from
unipolar depression, while statistically significant,
were often not greater than 20% between the two
groups (e.g. anhedonia was present in 86% of the
bipolar depressed group vs. 70% of the unipolar
depressed group). In addition, the differentiating
symptoms were often present in at least 50% of the
unipolar depressed group. Thus, from a clinical
standpoint, these symptoms and characteristics
should be viewed as aids in distinguishing these
groups and not as specific and unique to bipolar
depression.
Despite its limitations, this study represents the
first attempt to our knowledge to identify features of
MDD uniquely associated with bipolarity in a
pediatric population. Severe impairment, poor func-
tioning, suicidality, hospitalization, irritability and
sadness, high levels of comorbidity with CD, ODD
and agoraphobia as well as high rates of psychiatric
disorders in first degree relatives are all features which

J. Wozniak et al. / Journal of Affective Disorders 82S (2004) S59–S69S68
distinguish bipolar from unipolar depression in this
sample of ADHD youth. These features can alert
clinicians to those patients at highest risk of manic
exacerbation when treated with antidepressants.
References
Altshuler, L., Gitlin, M., Mintz, J., Leight, K., Frye, M., 2002.
Subsyndromal depression is associated with functional impair-
ment in patients with bipolar disorder. J. Clin. Psychiatry 63,
807–811.
Altshuler, L., Frye, M., Gitlin, M., 2003a. Acceleration and
augmentation strategies for treating bipolar depression. Biol.
Psychiatry 53, 691–700.
Altshuler, L., Suppes, T., Black, D., Nolen, W.A., Keck Jr., P.E.,
Frye, M.A., McElroy, S., Kupka, R., Grunze, H., Walden, J.,
Leverich, G., Denicoff, K., Luckenbaugh, D., Post, R., 2003b.
Impact of antidepressant discontinuation after acute bipolar
depression remission on rates of depressive relapse at 1-year
follow-up. Am. J. Psychiatry 160, 1252–1262.
Benazzi, F., 1999. Bipolar versus unipolar psychotic outpatient
depression. J. Affect. Disord. 55, 63–66.
Benazzi, F., Kuhs, H., Reschke, D., 1999a. Bipolar II versus
unipolar chronic depression: a 312-case study. Compr. Psychia-
try 40, 418–421.
Benazzi, F., Kuhs, H., Reschke, D., 1999b. Prevalence and clinical
features of atypical depression in depressed outpatients: a 467-
case study. Psychiatry Res. 86, 259–265.
Benazzi, F., Kuhs, H., Reschke, D., 2003. Is there a link between
atypical and early-onset bunipolarQ depression and bipolar II
disorder? Compr. Psychiatry 44, 102–109.
Biederman, J., Faraone, S.V., Keenan, K., Benjamin, J., Krifcher,
B., Moore, C., Sprich-Buckminster, S., Ugaglia, K., Jellinek,
M.S., Steingard, R., Spencer, T., Norman, D., Kolodny, R.,
Kraus, I., Perrin, J., Keller, M.B., Tsuang, M.T., 1992. Further
evidence for family-genetic risk factors in attention deficit
hyperactivity disorder. Patterns of comorbidity in probands and
relatives in psychiatrically and pediatrically referred samples.
Arch. Gen. Psychiatry 49, 728–738.
Biederman, J., Faraone, S.V., Milberger, S., Curtis, S., Chen, L.,
Marrs, A., Ouellette, C., Moore, P., Spencer, T., 1996. Predictors
of persistence and remission of ADHD: results from a four-year
prospective follow-up study of ADHD children. J. Am. Acad.
Child Adolesc. Psych. 35, 343–351.
Biederman, J., Faraone, S., Mick, E., Williamson, S., Wilens, T.,
Spencer, T., Weber, W., Jetton, J., Kraus, I., Pert, J., Zallen,
B., 1999. Clinical correlates of ADHD in females: findings
from a large group of girls ascertained from pediatric and
psychiatric referral sources. J. Am. Acad. Child Adolesc.
Psych. 38, 966–975.
Biederman, J., Mick, E., Spencer, T.J., Wilens, T.E., Faraone, S.V.,
2000. Therapeutic dilemmas in the pharmacotherapy of bipolar
depression in the young. J. Child Adolesc. Psych. 10, 185–192.
Brent, D.A., Perper, J.A., Goldstein, C.E., Kolko, D.J., Allan, M.J.,
Allman, C.J., Zelenak, J.P., 1988. Risk factors for adolescent
suicide: a comparison of adolescent suicide victims with suicidal
inpatients. Arch. Gen. Psychiatry 45, 581–588.
Faraone, S., Biederman, J., Krifcher Lehman, B., Keenan, K.,
Norman, D., Seidman, L., Kolodny, R., Kraus, I., Perrin, J.,
Chen, W., 1993. Evidence for the independent familial trans-
mission of attention deficit hyperactivity disorder and learning
disabilities: results from a family genetic study. Am. J.
Psychiatry 150, 891–895.
Faraone, S., Biederman, J., Milberger, S., 1995. How reliable are
maternal reports of their children’s psychopathology?: one year
recall of psychiatric diagnoses of ADHD children. J. Am. Acad.
Child Adolesc. Psych. 34, 1001–1008.
Faraone, S.V., Biederman, J., Mick, E., Williamson, S., Wilens, T.,
Spencer, T., Weber, W., Jetton, J., Kraus, I., Pert, J., Zallen, B.,
2000. Family study of girls with attention deficit hyperactivity
disorder. Am. J. Psychiatry 157, 1077–1083.
Geller, B., Fox, L., Clark, K., 1994. Rate and predictors of
prepubertal bipolarity during follow-up of 6- to 12-year-old
depressed children. J. Am. Acad. Child Adolesc. Psych. 33,
461–468.
Geller, B., Zimerman, B., Williams, M., Bolhofner, K., Craney, J.L.,
2001. Bipolar disorder at prospective follow-up of adults who
had prepubertal major depressive disorder. Am. J. Psychiatry
158, 125–127.
Goodwin, F., Jamison, K., 1990. Manic-Depressive Illness. Oxford
University Press, New York.
Hollingshead, A.B., 1975. Four Factor Index of Social Status. Yale
Press, New Haven.
John, K., Gammon, G.D., Prusoff, B.A., Warner, V., 1987. The
Social Adjustment Inventory for Children and Adolescents
(SAICA): testing of a new semistructured interview. J. Am.
Acad. Child Adolesc. Psych. 26, 898–911.
Kuhs, H., Reschke, D., 1992. Psychomotor activity in uni-
polar and bipolar depressive patients. Psychopathology 25,
109–116.
Luby, J.L., Mrakotsky, C., 2003. Depressed preschoolers with
bipolar family history: a group at high risk for later
switching to mania? J. Child Adolesc. Psych. 13, 187–197.
Mitchell, P.B., Wilhelm, K., Parker, G., Austin, M.P., Rutgers, P.,
Malhi, G.S., 2001. The clinical features of bipolar depression: a
comparison with matched major depressive disorder patients.
J. Clin. Psychiatry 62, 212–216. (quiz 217).
Orvaschel, H., Puig-Antich, J., 1987. Schedule for Affective
Disorders and Schizophrenia for School-Age Children: Epide-
miologic Version. Nova University, Fort Lauderdale, FL.
Post, R.M., Stoddard, F.J., Gillin, J.C., Buchsbaum, M.S., Runkle,
D.C., Black, K.E., Bunney, W.E., 1977. Alterations in motor
activity, sleep, and biochemistry in a cycling manic-depressive
patient. Arch. Gen. Psychiatry 34, 470–477.
Post, R., Altshuler, L., Frye, M., Suppes, T., Rush, A., Keck, P.J.,
McElroy, S., Denicoff, K., Leverich, G., Kupka, R., Nolen, W.,
2001. Rate of switch in bipolar patients prospectively treated
with second-generation antidepressants as augmentation to
mood stabilizers. Bipolar Disord. 3, 259–265.

J. Wozniak et al. / Journal of Affective Disorders 82S (2004) S59–S69 S69
Post, R., Leverich, G., Nolen, W., Kupka, R., Altshuler, L., Frye,
M., Suppes, T., McElroy, S., Keck, P., Grunze, H., Walden, J.,
2003. A re-evaluation of the role of antidepressants in the
treatment of bipolar depression: data from the Stanley Founda-
tion Bipolar Network. Bipolar Disord. 5, 396–406.
Spitzer, R.L., Williams, J.B., Gibbon, M., First, M.B., 1990.
Structured Clinical Interview for DSM-III-R: Non-Patient
Edition (SCID-NP, Version 1.0). American Psychiatric Press,
Washington, DC.
Strober, M., 1992. Relevance of early age-of-onset in genetic
studies of bipolar affective disorder. J. Am. Acad. Child
Adolesc. Psych. 31, 606–610.
Strober, M., Carlson, G., 1982. Predictors of bipolar illness in
adolescents with major depression: a follow-up investigation.
Adolesc. Psych. 10, 299–319.
Strober, M., Morrell, W., Burroughs, J., Lampert, C., Danforth, H.,
Freeman, R., 1988. A family study of bipolar I disorder in
adolescence: early onset of symptoms linked to increased familial
loading and lithium resistance. J. Affect. Disord. 15, 255–268.
Strober, M., Lampert, C., Schmidt, S., Morrell, W., 1993. The
course of major depressive disorder in adolescents: I. Recovery
and risk of manic switching in a follow-up of psychotic and
non-psychotic subtypes. J. Am. Acad. Child Adolesc. Psych.
32, 34–42.
Waechter, F., 2003. Paroxetine must not be given to patients under
18. BMJ 326, 1282.
Wechsler, D., 1991. Manual for the Wechsler Intelligence Scale for
Children. The Psychological, (Third edition)Harcourt Brace
Jovanovich, San Antonio.
Wozniak, J., Biederman, J., Faraone, S.V., Blier, H., Monuteaux,
M.C., 2001. Heterogeneity of childhood conduct disorder:
further evidence of a subtype of conduct disorder linked to
bipolar disorder. J. Affect. Disord. 64, 121–131.
Wozniak, J., Biederman, J., Monuteaux, M.C., Richards, J.,
Faraone, S.V., 2002. Parsing the comorbidity between bipolar
disorder and anxiety disorders: a familial risk analysis. J. Child
Adolesc. Psych. 12, 101–111.