the androgen receptor: genetic considerations in the development and treatment of prostate cancer
TRANSCRIPT

Abstract The action of androgens in the development andgrowth of prostate carcinomas is well documented. Theandrogen receptor (AR) facilitates androgen-induced regu-lation of genes involved in cellular proliferation and differ-entiation. Since the early 1940s androgen ablation hasbeen the cornerstone of treatment for metastatic prostatecancer. Although initially highly effective, hormonal thera-py is not curative, and resistant disease will ultimately pre-vail. Mutations that alter AR conformation, function, and
regulation may provide a selective growth advantage forsubpopulations of cells within the tumor that are then ableto proliferate in an androgen-deprived environment. Clini-cally, these mutations are important because they may leadto the growth of androgen-independent tumors and pro-gression to a refractory state. Further characterization ofAR mutations will lead to a more thorough understandingof their role in the development of prostate carcinomas.This information, in addition to discovering which genesare regulated by the AR, can aid in the future developmentof more effective pharmacotherapy for prostate cancer.
Key words Androgen receptor · Prostate cancer · Hormone ablation
Abbreviations AR Androgen receptor ·DHTDihydrotestosterone · SBD Steroid binding domain
K.J. Cude, S.C. Dixon, Y. Guo, J. Lisella, W.D. Figg (✉)Medicine Branch, National Cancer Institute, 9000 Rockville Pike,Bethesda, MD 20892, USAe-mail: [email protected], Tel.: +1-301-4023622, Fax: +1-301-4028606
J Mol Med (1999) 77:419–426 © Springer-Verlag 1999
REVIEW
Kelly J. Cude · Shannon C. Dixon · Yi Guo Jordan Lisella · William D. Figg
The androgen receptor: genetic considerations in the development andtreatment of prostate cancer
Received: 2 November 1998 / Accepted: 8 February 1999
Introduction
The androgen receptor (AR) is a ligand-dependent tran-scription factor that regulates tissue-specific genes in-volved in cellular proliferation and differentiation. AR be-longs to the steroid nuclear receptor superfamily whichincludes the estrogen, glucocorticoid, progesterone, miner-alocorticoid receptor, vitamin D, thyroid, retinoic acid andretinoid X receptors as well as several orphan receptors[1]. AR is highly expressed in muscle, skeletal, neural, andendocrine tissues, including the male urogenital tract. Infact, the spleen is the only tissue that shows a complete ab-sence of AR expression [2]. Its effect on prostate organphysiology is observed as a widespread reduction in cellnumber and volume following orchiectomy [3–6]. AR isactivated through the binding of either testosterone or themore potent agonist dihydrotestosterone (DHT). Due tothe growth-stimulating actions of androgens in both nor-mal and malignant prostate cells, a comprehensive under-standing of the structure, function, and molecular interac-
KELLY J. CUDE
received her B.S. in geneticsfrom the University of Califor-nia at Davis, USA. She is pres-ently a Predoctoral ResearchFellow in the Clinical Pharma-cology Section at the NationalCancer Institute in Bethesda,Md., USA. Her research inter-ests include the investigation oftrinucleotide repeat instabilityand the mechanisms of cellulartransformation.
WILLIAM D. FIGG
received his Pharm.D. fromAuburn University in Birming-ham, Ala., USA. He is present-ly the Head of the ClinicalPharmacology Section at theNational Cancer Institute inBethesda, Md., USA. His re-search interests include the in-vestigation of angiogenesis in-hibitors in the treatment ofhuman tumors and novel thera-peutic agents in the treatmentof prostate cancer.
tions of the AR is vital to the development of new treat-ments for prostatic disease.
Androgen ablation has been the standard therapy forprostate cancer patients with metastases since the pioneer-ing studies of Huggins and Hodges [3] in 1941. Hormonalmanipulation is a multifaceted attack which may involvesurgical removal of androgen-producing organs, luteiniz-ing hormone inhibition (with luteinizing hormone releas-ing hormone agonist), inhibition of androgen synthesis(aminoglutethimide, ketoconazole), inhibition of the test-osterone-converting enzyme 5α-reductase (finasteride), orthe use of receptor antagonists (flutamide, bicalutamide,nilutamide) [7]. Despite these efforts the metastatic pros-tate carcinoma eventually overcomes the growth con-straints of a low-androgen environment by selecting forcells that are able to proliferate under these conditions.This could convey the affect of mutations in the AR, al-tered regulation of its activities, or increased gene copynumber.
Androgen receptor structure and function
The gene
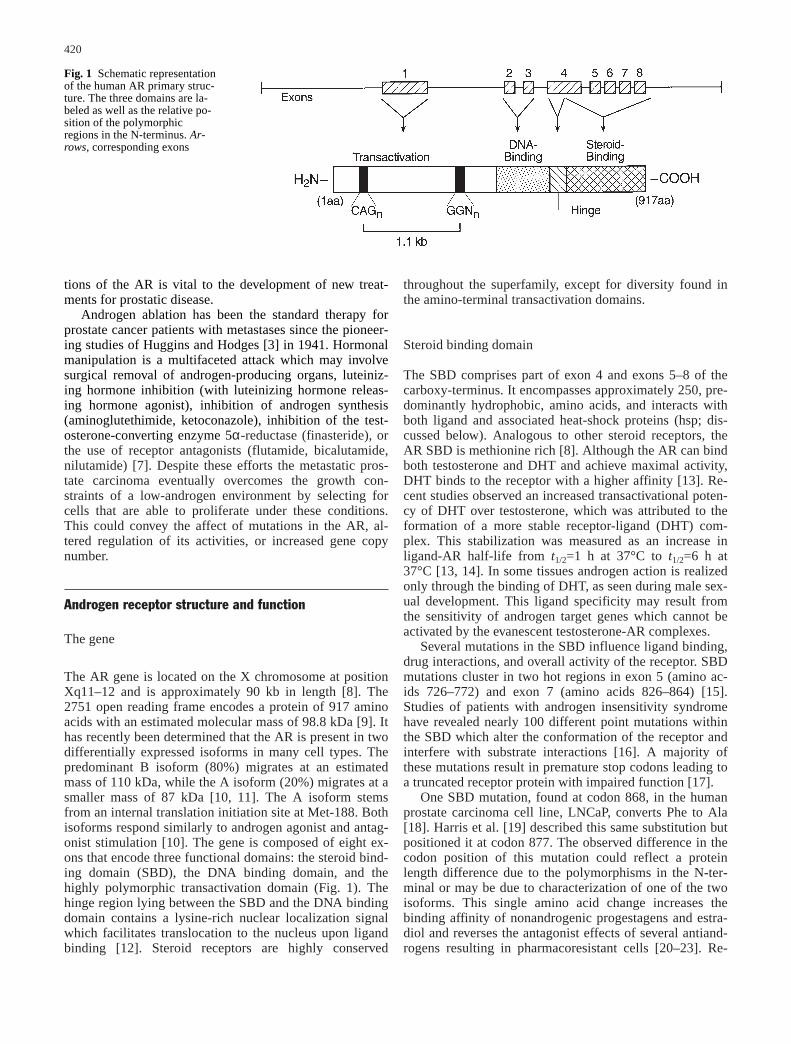
The AR gene is located on the X chromosome at positionXq11–12 and is approximately 90 kb in length [8]. The2751 open reading frame encodes a protein of 917 aminoacids with an estimated molecular mass of 98.8 kDa [9]. Ithas recently been determined that the AR is present in twodifferentially expressed isoforms in many cell types. Thepredominant B isoform (80%) migrates at an estimatedmass of 110 kDa, while the A isoform (20%) migrates at asmaller mass of 87 kDa [10, 11]. The A isoform stemsfrom an internal translation initiation site at Met-188. Bothisoforms respond similarly to androgen agonist and antag-onist stimulation [10]. The gene is composed of eight ex-ons that encode three functional domains: the steroid bind-ing domain (SBD), the DNA binding domain, and thehighly polymorphic transactivation domain (Fig. 1). Thehinge region lying between the SBD and the DNA bindingdomain contains a lysine-rich nuclear localization signalwhich facilitates translocation to the nucleus upon ligandbinding [12]. Steroid receptors are highly conserved
throughout the superfamily, except for diversity found inthe amino-terminal transactivation domains.
Steroid binding domain
The SBD comprises part of exon 4 and exons 5–8 of thecarboxy-terminus. It encompasses approximately 250, pre-dominantly hydrophobic, amino acids, and interacts withboth ligand and associated heat-shock proteins (hsp; dis-cussed below). Analogous to other steroid receptors, theAR SBD is methionine rich [8]. Although the AR can bindboth testosterone and DHT and achieve maximal activity,DHT binds to the receptor with a higher affinity [13]. Re-cent studies observed an increased transactivational poten-cy of DHT over testosterone, which was attributed to theformation of a more stable receptor-ligand (DHT) com-plex. This stabilization was measured as an increase inligand-AR half-life from t1/2=1 h at 37°C to t1/2=6 h at37°C [13, 14]. In some tissues androgen action is realizedonly through the binding of DHT, as seen during male sex-ual development. This ligand specificity may result fromthe sensitivity of androgen target genes which cannot beactivated by the evanescent testosterone-AR complexes.
Several mutations in the SBD influence ligand binding,drug interactions, and overall activity of the receptor. SBDmutations cluster in two hot regions in exon 5 (amino ac-ids 726–772) and exon 7 (amino acids 826–864) [15].Studies of patients with androgen insensitivity syndromehave revealed nearly 100 different point mutations withinthe SBD which alter the conformation of the receptor andinterfere with substrate interactions [16]. A majority ofthese mutations result in premature stop codons leading toa truncated receptor protein with impaired function [17].
One SBD mutation, found at codon 868, in the humanprostate carcinoma cell line, LNCaP, converts Phe to Ala[18]. Harris et al. [19] described this same substitution butpositioned it at codon 877. The observed difference in thecodon position of this mutation could reflect a proteinlength difference due to the polymorphisms in the N-ter-minal or may be due to characterization of one of the twoisoforms. This single amino acid change increases thebinding affinity of nonandrogenic progestagens and estra-diol and reverses the antagonist effects of several antiand-rogens resulting in pharmacoresistant cells [20–23]. Re-
420
Fig. 1 Schematic representationof the human AR primary struc-ture. The three domains are la-beled as well as the relative po-sition of the polymorphicregions in the N-terminus. Ar-rows, corresponding exons
cent clinical findings observed in several laboratories showthat withdrawal of flutamide results in declining prostate-specific antigen in approximately one-third of patientswith hormone refractory prostate cancer [20, 24, 25]. Clin-ically, it is important to consider these mutations becausesome antiandrogens given to patients with altered ARsmay stimulate the receptor and accelerate the growth ofandrogen-independent disease. For patients with andro-gen-independent disease the withdrawal of antiandrogensmay provide clinical benefit.
A substitution mutation found in a highly conserved re-gion of SBD converts Val-730 to Met and is believed to in-terfere with binding of hsp 90 by the inactivated AR [26].Analogous mutations found in the highly conserved regionof the glucocorticoid receptor have been shown to abro-gate hsp 90 binding. This results in a cleaved receptor withconstitutive activity one-third of that seen in a normal ste-roid-activated receptor [5]. In a similar manner the ARmutation at site Val-730 discovered by Newmark et al.[26] may enhance disease progression in prostate cancerpatients by rendering the AR constitutively active.
DNA binding domain
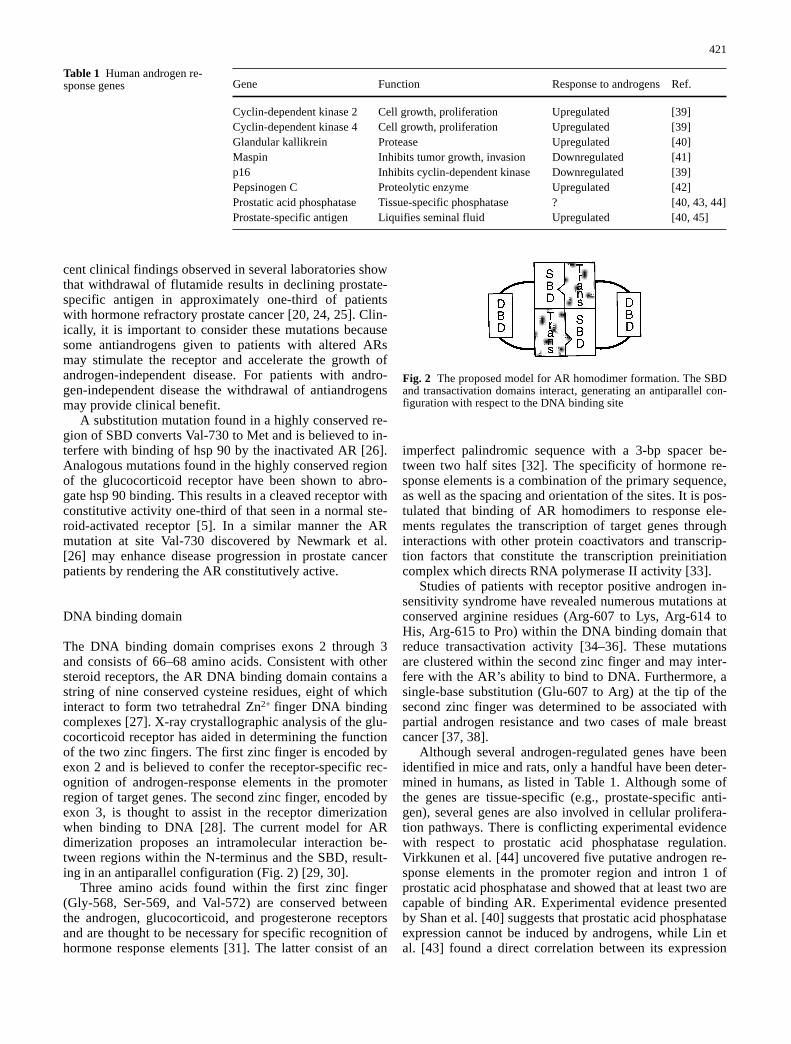
The DNA binding domain comprises exons 2 through 3and consists of 66–68 amino acids. Consistent with othersteroid receptors, the AR DNA binding domain contains astring of nine conserved cysteine residues, eight of whichinteract to form two tetrahedral Zn2+ finger DNA bindingcomplexes [27]. X-ray crystallographic analysis of the glu-cocorticoid receptor has aided in determining the functionof the two zinc fingers. The first zinc finger is encoded byexon 2 and is believed to confer the receptor-specific rec-ognition of androgen-response elements in the promoterregion of target genes. The second zinc finger, encoded byexon 3, is thought to assist in the receptor dimerizationwhen binding to DNA [28]. The current model for ARdimerization proposes an intramolecular interaction be-tween regions within the N-terminus and the SBD, result-ing in an antiparallel configuration (Fig. 2) [29, 30].
Three amino acids found within the first zinc finger(Gly-568, Ser-569, and Val-572) are conserved betweenthe androgen, glucocorticoid, and progesterone receptorsand are thought to be necessary for specific recognition ofhormone response elements [31]. The latter consist of an
imperfect palindromic sequence with a 3-bp spacer be-tween two half sites [32]. The specificity of hormone re-sponse elements is a combination of the primary sequence,as well as the spacing and orientation of the sites. It is pos-tulated that binding of AR homodimers to response ele-ments regulates the transcription of target genes throughinteractions with other protein coactivators and transcrip-tion factors that constitute the transcription preinitiationcomplex which directs RNA polymerase II activity [33].
Studies of patients with receptor positive androgen in-sensitivity syndrome have revealed numerous mutations atconserved arginine residues (Arg-607 to Lys, Arg-614 toHis, Arg-615 to Pro) within the DNA binding domain thatreduce transactivation activity [34–36]. These mutationsare clustered within the second zinc finger and may inter-fere with the AR’s ability to bind to DNA. Furthermore, asingle-base substitution (Glu-607 to Arg) at the tip of thesecond zinc finger was determined to be associated withpartial androgen resistance and two cases of male breastcancer [37, 38].
Although several androgen-regulated genes have beenidentified in mice and rats, only a handful have been deter-mined in humans, as listed in Table 1. Although some ofthe genes are tissue-specific (e.g., prostate-specific anti-gen), several genes are also involved in cellular prolifera-tion pathways. There is conflicting experimental evidencewith respect to prostatic acid phosphatase regulation. Virkkunen et al. [44] uncovered five putative androgen re-sponse elements in the promoter region and intron 1 ofprostatic acid phosphatase and showed that at least two arecapable of binding AR. Experimental evidence presentedby Shan et al. [40] suggests that prostatic acid phosphataseexpression cannot be induced by androgens, while Lin etal. [43] found a direct correlation between its expression
421
Fig. 2 The proposed model for AR homodimer formation. The SBDand transactivation domains interact, generating an antiparallel con-figuration with respect to the DNA binding site
Gene Function Response to androgens Ref.
Cyclin-dependent kinase 2 Cell growth, proliferation Upregulated [39]Cyclin-dependent kinase 4 Cell growth, proliferation Upregulated [39]Glandular kallikrein Protease Upregulated [40]Maspin Inhibits tumor growth, invasion Downregulated [41]p16 Inhibits cyclin-dependent kinase Downregulated [39]Pepsinogen C Proteolytic enzyme Upregulated [42]Prostatic acid phosphatase Tissue-specific phosphatase ? [40, 43, 44]Prostate-specific antigen Liquifies seminal fluid Upregulated [40, 45]
Table 1 Human androgen re-sponse genes

and degree of androgen stimulation. Future research to de-termine androgen-regulated genes will uncover more path-ways involved in androgen action and be vital in the devel-opment of therapeutic agents for prostate cancer.
Transactivation domain
The transactivation domain occupies the N-terminus of theAR gene and is the most diverse among nuclear receptordomains. Comprising more than half the AR, thetransactivation domain is encoded by a single exon (exon1) and consists of over 500 amino acids [31, 32]. Althoughthe exact mechanism of domain action has not been deter-mined, it is postulated that the transactivation domain in-teracts with other accessory proteins to regulate the speci-ficity of targeted genes and the expression of these genes.The diversity of the transactivation domain implicates it asan important determinant in gene activation specificity.This diversity stems largely from two polymorphic regionsof trinucleotide repeats: a 5’ stretch of polyglutamines(CAG) and a 3’ stretch of polyglycines (GGN) [46, 47].The CAG trinucleotide repeats have been implicated in themotor neuron degeneration associated with spinal bulbarmuscular atrophy, or Kennedy’s disease, as well as in-creased risk for prostate cancer. The GGN stretches havealso been associated with increased risk for prostate cancerfor alleles containing 16 or fewer repeats [48, 49]. In thenormal population the number of CAG repeats range from11–31 repeats, with an average of 21±2 [46, 47]. In indi-viduals with spinal bulbar muscular atrophy, this polymor-phic region may contain upwards of 50 repeats [2], result-ing in receptors with blunted transactivation activity [50].
On the other hand, prostate cancer risk is associatedwith the shorter CAG alleles. Racial and ethnic differencesexist for prostate cancer incidence; the incidence amongmen of African descent is twice as high as that amongwhite men in the United States [51]. This racial discrepan-cy in prostate cancer occurrence may in part reflect thresh-old limitations of CAG lengths on receptor function. Afri-can-American men average 18 repeats, whites 21, andAsians, who are in the lowest risk bracket, 22 [46]. The ef-fects of the shorter alleles on receptor function is per-ceived as an increase in transactivation activity [48, 52,53]. Two possible mechanisms may explain this phenome-non. First, the triplet repeat region may act as an inhibitorof transactivation activity, with longer repeat regions act-ing as more effective inhibitors. Alternatively, the receptorwith shorter repeat regions may have a more stable confor-mation in the nucleus, which allows it to escape proteolyt-ic degradation in the cytoplasm.
Several in vitro deletion mapping experiments of thetransactivation domain have defined regions that are nec-essary for transactivation activity. Although nearly the en-tire N-terminus was required for maximal transactivation,Simental et al. [54] defined a smaller section between ami-no acids 141 and 338 that is essential for any measurableactivity. Two additional transcription activation units(TAU-1, TAU-5) were defined by Jenster et al. [55] that re-
sponded to the presence of the SBD. Specifically, TAU-1(amino acids 100–370) was active in the presence of theSBD, whereas TAU-5 (amino acids 360–485) was consti-tutively active in the absence of the SBD. Deletion of largesections of the N-terminus may remove specific amino ac-ids that mediate transactivation activity or may cause con-formational changes that reduce AR activity.
Evidence provided by Zhou et al. [14] suggests that thestabilization of AR depends on inhibitory interactions be-tween the N-terminus and the SBD. This interaction facili-tates the slow release of ligand and prevents proteolyticdegradation. Additionally, in vitro deletion of the SBD re-sulted in a constitutively active receptor, both in the pres-ence of a wild-type and partially deleted N-terminus [56].This suggests that the SBD inhibits the ARs interactionwith accessory proteins or other regulatory sites that arenecessary for AR activation.
Regulation of AR functions
Phosphorylation
Steroid hormone receptors are phosphoproteins that areregulated by protein kinase and phosphatase activity [57].The phosphorylation (or dephosphorylation) of specificresidues may be involved in mediating numerous receptorfunctions including: ligand binding, nuclear translocation,receptor dimerization, DNA binding, and protein-proteininteractions [58]. Twenty-one potential phosphorylationsites have been identified in the AR, with 15 lying in theN-terminal transactivation domain [59]. Two residues(Ser-80, Ser-93) in the N-terminal region and one in thehinge (Ser-650) are the only confirmed phosphorylationsites in the AR. Mutations at Ser-80 and Ser-93 have novisible effect on receptor function, whereas a mutation atSer-650 results in a 30% decrease in transcriptional activi-ty [14, 55]. Langley et al. [29] have recently described theinteraction between the SBD and N-terminus in receptordimerization. Six potential phosphorylation sites, situatedin the region of the N-terminus, are proposed to facilitatehomodimer formation. Mutational analysis of these andother potential phosphorylation sites will help to furtherdefine the role of phosphorylation and AR function.
The development of ligand-independent ARs in andro-gen-independent prostate cancer may involve activation ofthe receptor via protein kinase cascades. Recent experi-ments performed by Nazareth and Weigel [60] show ARactivation in the presence of forskolin, a protein kinase A(i.e., cyclic adenosine monophosphate dependent kinase)activator. Forskolin stimulates adenylate cyclase to pro-duce the intracellular second-messenger cyclic adenosinemonophosphate, which then activates protein kinase A.Nazareth and Weigel also saw a decrease in AR activationby forskolin and androgen in the presence of the proteinkinase A inhibitor peptide [6–22] amide [60]. Blok et al.[61] looked for differential phosphorylation of the AR inthe presence of forskolin and found that phosphorylation
422
at Ser-641 and Ser-653 was significantly reduced whencompared to controls. Target gene activation by this de-phosphorylated receptor was also significantly lower thanin controls [61]. This lends evidence to the hypothesis thatphosphorylation of the AR plays a critical role in the regu-lation of its transactivation activity.
Heat-shock proteins
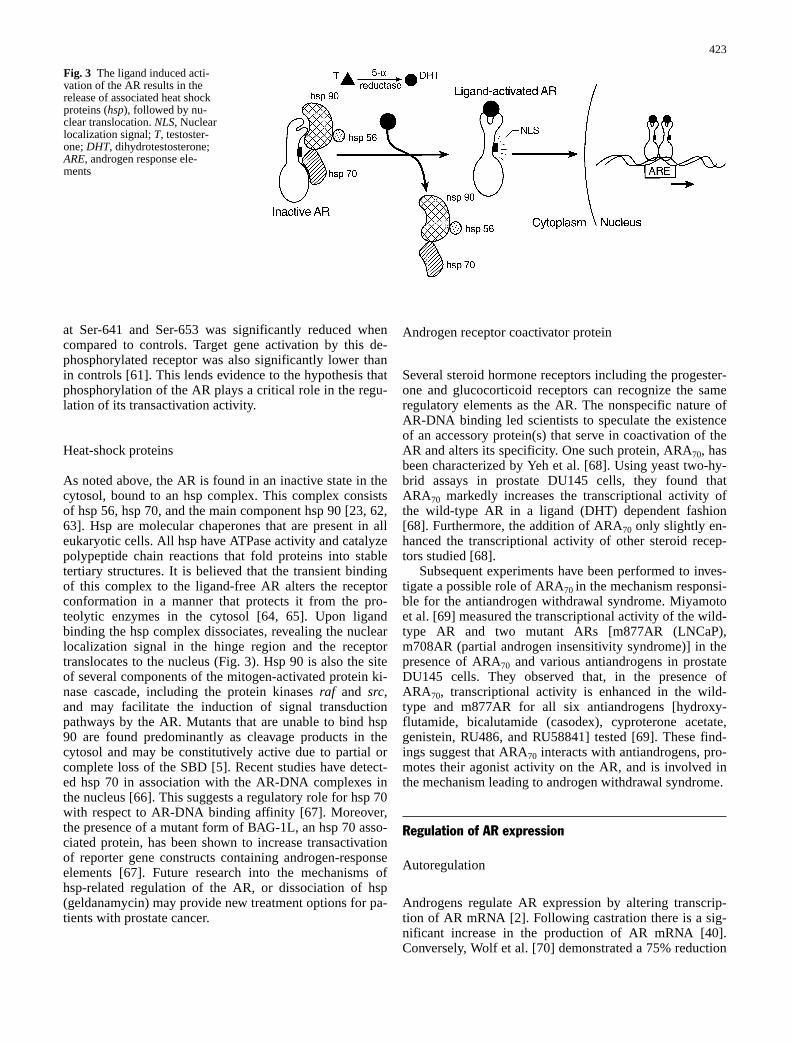
As noted above, the AR is found in an inactive state in thecytosol, bound to an hsp complex. This complex consistsof hsp 56, hsp 70, and the main component hsp 90 [23, 62,63]. Hsp are molecular chaperones that are present in alleukaryotic cells. All hsp have ATPase activity and catalyzepolypeptide chain reactions that fold proteins into stabletertiary structures. It is believed that the transient bindingof this complex to the ligand-free AR alters the receptorconformation in a manner that protects it from the pro-teolytic enzymes in the cytosol [64, 65]. Upon ligandbinding the hsp complex dissociates, revealing the nuclearlocalization signal in the hinge region and the receptortranslocates to the nucleus (Fig. 3). Hsp 90 is also the siteof several components of the mitogen-activated protein ki-nase cascade, including the protein kinases raf and src,and may facilitate the induction of signal transductionpathways by the AR. Mutants that are unable to bind hsp90 are found predominantly as cleavage products in thecytosol and may be constitutively active due to partial orcomplete loss of the SBD [5]. Recent studies have detect-ed hsp 70 in association with the AR-DNA complexes inthe nucleus [66]. This suggests a regulatory role for hsp 70with respect to AR-DNA binding affinity [67]. Moreover,the presence of a mutant form of BAG-1L, an hsp 70 asso-ciated protein, has been shown to increase transactivationof reporter gene constructs containing androgen-responseelements [67]. Future research into the mechanisms ofhsp-related regulation of the AR, or dissociation of hsp(geldanamycin) may provide new treatment options for pa-tients with prostate cancer.
Androgen receptor coactivator protein
Several steroid hormone receptors including the progester-one and glucocorticoid receptors can recognize the sameregulatory elements as the AR. The nonspecific nature ofAR-DNA binding led scientists to speculate the existenceof an accessory protein(s) that serve in coactivation of theAR and alters its specificity. One such protein, ARA70, hasbeen characterized by Yeh et al. [68]. Using yeast two-hy-brid assays in prostate DU145 cells, they found thatARA70 markedly increases the transcriptional activity ofthe wild-type AR in a ligand (DHT) dependent fashion[68]. Furthermore, the addition of ARA70 only slightly en-hanced the transcriptional activity of other steroid recep-tors studied [68].
Subsequent experiments have been performed to inves-tigate a possible role of ARA70 in the mechanism responsi-ble for the antiandrogen withdrawal syndrome. Miyamotoet al. [69] measured the transcriptional activity of the wild-type AR and two mutant ARs [m877AR (LNCaP),m708AR (partial androgen insensitivity syndrome)] in thepresence of ARA70 and various antiandrogens in prostateDU145 cells. They observed that, in the presence ofARA70, transcriptional activity is enhanced in the wild-type and m877AR for all six antiandrogens [hydroxy-flutamide, bicalutamide (casodex), cyproterone acetate,genistein, RU486, and RU58841] tested [69]. These find-ings suggest that ARA70 interacts with antiandrogens, pro-motes their agonist activity on the AR, and is involved inthe mechanism leading to androgen withdrawal syndrome.
Regulation of AR expression
Autoregulation
Androgens regulate AR expression by altering transcrip-tion of AR mRNA [2]. Following castration there is a sig-nificant increase in the production of AR mRNA [40].Conversely, Wolf et al. [70] demonstrated a 75% reduction
423
Fig. 3 The ligand induced acti-vation of the AR results in therelease of associated heat shockproteins (hsp), followed by nu-clear translocation. NLS, Nuclearlocalization signal; T, testoster-one; DHT, dihydrotestosterone;ARE, androgen response ele-ments

in the level of transcriptional initiation after treating thehuman prostate carcinoma line LNCaP with androgen.This implies the involvement of a feedback mechanism inthe regulation of AR transcription, wherein increased lev-els of DHT may inhibit the conversion of testosterone toDHT or the secretion of testosterone. Of interest is the factthat fluctuating levels of AR mRNA induced by androgenstimulus and withdrawal are not correlated with AR pro-tein levels which are static [70, 71]. This suggests that ARregulation by androgen occurs at multiple levels: those oftranscription, translation, and degradation. Second-mes-senger pathways may also play a role in the regulation ofAR mRNA levels. Experiments performed by Henntu andVihko [72] suggest that the stimulation of protein kinase Cpathways results in a suppression of AR mRNA in LNCaPcells.
Growth factors
Several growth factors influence AR activation by effect-ing second-messenger pathways [2, 73]. Numerous growthfactors have been implicated in androgen-independentgrowth of prostate cells through both paracrine andautocrine mechanisms, including: insulin growth factor,keratinocyte growth factor, fibroblast growth factor, andepidermal growth factor [74–78]. Culig et al. [75] ob-served AR activation in response to insulin, keratinocyte,and epidermal growth factors that was reversed upon addi-tion of bicalutamide. Conversely, transforming growth fac-tor β causes a reduction in AR expression by inducing anuclear to cytoplasmic shift in receptor distribution, fol-lowed by receptor degradation [79]. Nonsteroidal influenc-es on AR activation need to be considered when treatingpatients with hormonal ablation based on their involve-ment in the growth and development of androgen-indepen-dent tumors.
Gene amplification
The formation of androgen-independent tumors requires ameans of adapting to androgen deprivation. This may befacilitated by mutations in the receptor which allow non-specific ligand or ligand-independent activation of the re-ceptor or by an increase in AR copy number. AR gene am-plification provides a mechanism by which tumor cells cancompensate for low amounts of circulating androgen. Vis-korpi et al. [80] observed gene amplification in 7 of 23(30%) recurrent prostate tumors following androgen depri-vation that was not present in the original tumor. In addi-tion, a study by Koivisto et al. [81] found gene amplifica-tion present in 15 of 54 (28%) recurrent prostatecarcinomas, with individual tumor cells having between 5and 60 AR genes. In both studies the identified gene am-plification was correlated with an increase in AR expres-sion. Gene amplification was observed only following hor-monal ablation, which suggests that amplification confersa selective growth advantage for tumor cells, allowing
them to compensate for low levels of circulating androgen[33].
Conclusion
A vast amount of information has accumulated on thestructure and function of the AR. It represents a classic ex-ample of the way in which different mutations within asingle gene can yield multiple phenotypes. Mutationswithin the AR are associated with several disorders, in-cluding androgen insensitivity syndrome, spinal bulbarmuscular atrophy, and prostate cancer. Its role as a propo-nent of cell growth in prostate cancer makes it the centralfocus of research for metastatic disease, primarily in anandrogen-independent setting. Following hormone abla-tion, there is an initial period of tumor regression, fol-lowed by an eventual state of androgen independence.Several genetic factors may increase the occurrence of an-drogen-independent tumors; these include mutations thatalter ligand specificity, mutations that alter regulation ofthe AR and its functions, mutations that affect associatedhsp, and AR gene amplification. Whereas gene amplifica-tion may be the direct result of hormonal ablation, it isproposed that a subset of androgen-independent cells pre-exist within tumors which are clonally selected in responseto a low androgen environment. Conversely, AR mutationsmay arise spontaneously in response to the stress of andro-gen ablation. To better understand the effects of AR muta-tions in tumor development it is crucial to determinewhich genes are regulated by the AR. As more experimen-tal evidence is gathered, and the genes regulated by andro-gen action are unveiled, more practical and effective phar-macological approaches can be designed.
References
1. Tsai MJ, O’Malley BW (1994) Molecular mechanisms of actionof steroid/thyroid receptor superfamily members. Annu RevBiochem 63:451–486
2. Lindzey J, Kumar MV, Grossman M, Young C, Tindall DJ(1994) Molecular mechanisms of androgen action. Vitam Horm49:383–431
3. Huggins C, Hodges CV (1941) The effect of castration, ofoestrogen and of androgen injection on serum phosphatases inmetastatic carcinoma of the prostate. Cancer Res 1:942
4. Rauch F, Polzar B, Stephan J, Zanotti S, Paddengerg R,Mannherz HG (1997) Androgen ablation leads to anupregulation and intranuclear accumulation of deoxyribonu-clease I in rat prostate epithelial cells paralleling their apoptoticelimination. J Cell Biol 137:909–923
5. Housley PR, Sanchez ER, Danielsen M, Ringold GM, Pratt WB(1990) Evidence that the conserved region in the steroid bindingdomain of the glucocorticoid receptor is required for both opti-mal binding of hsp 90 and protection from proteolytic cleavage.J Biol Chem 265:12778–12781
6. Kypriana N, English HF, Isaacs JT (1990) Programmed celldeath during the regression of PC-82 human prostate followingandrogen ablation. Cancer Res 50:3748
7. Middleman MN, Lush RM, Sartor O, Reed E, Figg WD (1996)Treatment approaches for metastatic cancer of the prostate basedon recent molecular evidence. Cancer Treat Rev 22:105–118
424
8. Chang C, Kokontis J, Liao S (1988) Structural analysis of com-plementary DNA and amino acid sequences of human and ratandrogen receptors. Proc Natl Acad Sci USA 85:7211–7215
9. Brinkmann AO, Faber PW, van Rooj HCJ, Kuiper GGJ, Ris C,Klaassen P, van der Korput JAGM, Voorhorst MM, van Laar JJ,Mulder E, Trapman J (1989) The human androgen receptor: do-main, structure, genomic organization and regulation of expres-sion. J Steroid Biochem Mol Biol 34:307–310
10. Gao T, McPhaul MJ (1998) Functional activities of the A and Bforms of the human androgen receptor in resonse to androgen re-ceptor agonists and antagonists. Mol Endocrinol 12:654–663
11. Wilson JD, McPhaul MJ (1994) A and B forms of the androgenreceptor are present in genital skin fibroblasts. Proc Natl AcadSci USA 91:1234–1238
12. Zhou Z-X, Wong C-I, Sar M, Wilson EM (1994) The androgenreceptor: an overview. Recent Prog Horm Res 49:249–274
13. Deslypere JP, Young M, Wilson JD, McPhaul MJ (1992) Test-osterone and 5 alpha- dihydrotestosterone interact differentlywith the androgen receptor to enhance transcription of theMMTV-CAT reporter gene. Mol Cell Endocrinol 88:15–22
14. Zhou ZX, Lane MV, Kemppainen JA, French FS, Wilson EM(1995) Specificity of ligand-dependent androgen receptor stabili-zation: receptor domain interactions influence ligand dissocia-tion and receptor stability. Mol Endocrinol 9:208–218
15. McPhaul MJ, Marcelli M, Zoppi S, Wilson CM, Griffin JE, Wil-son JD (1992) Mutations in the ligand-binding domain of the an-drogen receptor gene cluster in two regions of the gene. J ClinInvest 90:2097–2101
16. Sultan C, Lumbroso S, Poujol N, Belon C, Boudon C, LobaccaroJ-M (1993) Mutations of androgen receptor gene in androgen in-sensitivity syndromes. J Steroid Biochem Mol Biol 46:519–530
17. McPhaul MJ, Marcelli M, Zoppi S, Griffin JE, Wilson JD (1993)Genetic basis of endocrine disease. IV. The spectrum of muta-tions in the androgen receptor gene that causes androgen resis-tance. J Clin Endocrinol Metab 76:17–23
18. Vedscholte J, Ris-Staplers C, Kuiper, GGJM, Jenster G, Berrevo-ets C, Claassen E, Van Rooij HCJ, Trapman J, Brinkmann AO,Mulder E (1990) A mutation in the ligand binding domain of theandrogen receptor of human LNCaP cells affects steroid bindingcharacteristics and response to antiandrogens. Biochem BiophysRes Commun 173:534–540
19. Harris SE, Rong Z, Harris MA, Lubahn DE (1991) Androgen re-ceptor in human prostate carcinoma LNCaP/ADEP cells con-tains a mutation which alters the specificity of the steroid-depen-dent transcriptional activation region. Endocrinolgy 126[Suppl]:93
20. Figg WD, McCall N, Reed E, Sartor O (1994) The in vitro re-sponse of four antisteroid receptor agents on the hormone-re-sponsive prostate cancer cell line LNCaP. Oncol Rep 2:295–298
21. Veldscholte J, Voorhorst-Ogink MM, Bolt-de Vries J, Rooy, HCJVan, Trapman J, Mulder E (1990) Unusual specificity of the an-drogen receptor in the human prostate tumor cell line LNCaP:high affinity for progestagenic and estrogenic steroids. BiochimBiophys Acta 1052:187–194
22. Veldscholte J, Berrevoets CA, Ris-Staplpers C, Kuiper, GGJM,Jenster G, Trapman J, Brinkmann AO, Mulder E (1991) The an-drogen receptor in LNCap cells contains a mutation in the ligandbinding domain which affects steroid binding characteristics andresponse to antiandrogens. J Steroid Biochem Mol Biol 665–669
23. Veldscholte J, Berrevoets CA, Brinkmann AO, Grootegoed JA,Mulder E (1992) Anti-androgens and the mutated androgen re-ceptor of LNCaP cells: differential effects on binding affinity,heat-shock protein interaction, and transcription activation. Bio-chemistry 31:2393–2399
24. Figg WD, Sartor MD, Cooper MR, Thibault A, Bergen RC,Dawson N, Reed E, Myers CE (1995) Prostate specific antigendecline following the discontinuation of flutamide in patientswith stage D2 prostate cancer. Am J Med 98:412–414
25. Scher H, Kelly WK (1993) Flutamide withdrawal syndrome: itsimpact on clinical trials in hormone-refractory prostate cancer. JClin Oncol 11:566–572
26. Newmark JR, Hardy DO, Tonb DC, Carter B, Epstein JI, IsaacsWB, Brown TR, Barrack ER (1992) Androgen receptor genemutations in human prostate cancer. Proc Natl Acad Sci USA89:6319–6323
27. Janne OA, Palvimo JJ, Kallio P, Mehto M (1993) Androgen re-ceptor and mechanism of androgen action. Ann Med 25:83–89
28. Luisi BF, Xu WX, Otwinowski Z, Freedman LP, Yamamoto KR,Sigler PB (1991) Crystallographic analysis of the interaction ofthe glucocorticoid receptor with DNA. Nature 352:497–505
29. Langley E, Shou ZX, Wilson EM (1995) Evidence for an anti-parallel orientation of the ligand-activated human androgen re-ceptor dimer. J Biol Chem 270:29983–29990
30. Wong C-I, Zhou ZX, Sar M, Wilson EM (1993) Steroid require-ments for androgen receptor dimerization and DNA binding.Modulation by intramolecular interactions between the NH2-ter-minal and steroid-binding domains. J Biol Chem 268:1004–1012
31. Quigley CA, De Bellis A, Marschke KB, el-Awady MK, FrenchFS (1995) Androgen receptor defects: historical, clinical, andmolecular perspectives. Endocr Rev 16:271–321
32. Trapman J, Cleutjes KBJM (1997) Androgen-regulated gene ex-pression in prostate cancer. Semin Cancer Biol 8:29–36
33. Trapman J, Brinkmann AO (1996) The androgen receptor inprostate cancer. Pathol Res Pract 192:752–760
34. Mowszowic I, Lee HJ, Chen HT, Mestaryer C, Portiois MC,Cabrol S, Mauvais-Jarvis P, Chang C (1993) A point mutation inthe second zinc finger of the DNA-binding domain of the andro-gen receptor gene causes complete androgen insensitivity in twosiblings with receptor-positive androgen resistance. MolEndocrinol 7:861–869
35. Saunders PTK, Padayachi T, Tincello DG, Shalet SM, Wu FCU(1992) Point mutations detected in the androgen receptor gene ofthree men with partial androgen insensitivity syndrome. Am JHum Genet 46:1095–1100
36. Zoppi S, Marcelli M, Deslypere JP, Griffin JE, Wilson J,McPhaul MJ (1992) Amino acid substitutions in the DNA-bind-ing positive androgen resistance. Mol Endocrinol 6:409–415
37. Couture P, Theriault C, Simard J, Labrie F (1993) Androgenreceptor-mediated stimulation of 17 beta-hydroxydihydro-testosterone and medroxyprogesterone acetate in ZR-75-1 hu-man breast cancer cells. Endocrinology 132:179–185
38. Wooster R, Mangion J, Eeles E (1992) A germline mutation inthe androgen receptor in two families with Reifenstein syn-drome. Nat Genet 2:132–134
39. Lu S, Tsai SY, Tsai M-J (1997) Regulation of androgen-depen-dent prostatic cancer cell growth: androgen regulation of CDK2,CDK4, and CKI p16 genes. Cancer Res 57:4511–4516
40. Shan J-D, Porvari K, Ruokonen M, Karhu A, Launonen V, Hed-berg P, Oikarinene J, Nihko P (1997) Steroid-involved transcrip-tional regulation of human genes encoding prostatic acid phos-phatase, prostate-specific antigen, and prostate-specificglandular kallikrein. Endocrinology 138:3764–3770
41. Zhang M, Magit D, Sager R (1997) Expression of maspin inprostate cells is regulated by a positive Ets element and a nega-tive hormonal responsive element site recognized by androgenreceptor. Proc Natl Acad Sci USA 94:5673–5678
42. Balbin M, Lopez-Otin C (1996) Hormonal regulation of the hu-man pepsinogen C gene in breast cancer cells. J Biol Chem271:15175–15181
43. Lin MF, Meng TC, Rao PS, Chang C, Schonthal AH, Lin FF(1998) Expression of human prostatic acid phosphatase corre-lates with androgen-stimulated cell proliferation in prostate can-cer cell lines. J Biol Chem 273:5939–5947
44. Virkkunen P, Hedberg P, Palvimo JJ, Birr E, Porvari K, Ruoko-nen M, Taavitsainen P, Janne OA, Vihko P (1994) Structuralcomparison of human and rate prostate- specific acid phos-phatase genes and their promoters: identification of putative an-drogen response elements. Biochem Biophys Res Commun202:49–57
45. Cleutjens KBMJ, van Eekelen CCEM, van der Korput HAGM,Brinkmann AO, Trpaman J (1996) Two androgen response re-gions cooperate in steroid hormone regulated activity of theprostate-specific antigen promoter. J Biol Chem 217:6379- 6388
425
46. Coetzee A, Ross RK (1994) Re: prostate cancer and the andro-gen receptor. J Natl Cancer Inst 86:872–873
47. Schoneberg MP, Hakimi JM, Wang S, Bova GS, Epstein JI, Fis-hcbeck KH, Isaacs WB, Walsh PC, Barrack ER (1994)Microsatellite mutation (CAG24–18) in the androgen receptorgene in human prostate cancer. Biochem Biophys Res Commun198:74–80
48. Irvine RA, Yu MC, Ross RK, Coeztee GA (1995) The CAG andGGC microsatellites of the androgen receptor gene are in linkagedisequilibrium in men with prostate cancer. Cancer Res55:1937–1940
49. Stanford JL, Just JJ, Gibbs M Wicklund K, Neal CL, Blumen-stein BA, Ostrander EA (1997) Polymorphic repeats in the an-drogen receptor gene: molecular markers of prostate cancer risk.Cancer Res 57:1994–1998
50. Mhatre AN, Trifiro MA, Kaufman M, Kazemi-Esfarjani P, Fig-lewicz D, Rouleau G, Pinsky L (1993) Reduced transcriptionalregulatory competence of the androgen receptor in X-linked spi-nal and bulbar muscular atrophy. Nat Genet 5:184- 188
51. Ross RK (1990) The hormonal basis of prostate cancer (ab-stract). Proc Am Assoc Cancer Res 31:457–458
52. Kazemi-Esfarjani P, Trifiro MA, Pinsky L (1995) Evidence for arepressive function of the long polyglutamine tract in the humanandrogen receptor: possible pathogenetic relevance for the(CAG)n-expanded neuronopathies. Hum Mol Genet 4:523–527
53. Gerber HP, Seipel K, Georgiev O, Hofferer M, Hug M, RusconiS, Schaffner W (1994) Transcriptional activation modulated byhomopolymeric glutamine and proline stretches. Science 263:808–811
54. Simental JA, Madhabanda S, Wilson EM (1992) Domain func-tions of the androgen receptor. J Steroid Biochem Mol Biol43:37–41
55. Jenster G, van der Korput JAGM, Trapman J, Brinkmann AO(1995) Identification of two transcription activation units in theN-terminal domain of the human androgen receptor. J BiolChem 270:7341–7346
56. Gao T, Marcelli M, McPhaul MJ (1996) Transcriptional activa-tion and transient expression of the human androgen receptor. JSteroid Biochem Mol Biol 59:9–20
57. Kemppainen JA, Lanee MV, Sar M, Wilson EM (1992) Andro-gen receptor phosphorylation, turnover, nuclear transport, andtranscriptional activation. Specificity for steroids and antihormo-nes. J Biol Chem 267:968–974
58. Blok LJ, de Ruiter PE, Brinkmann AO (1996) Androgen recep-tor phosphorylation. Endocr Res 22:197–219
59. Kuiper GGJM, de Ruiter PE, Trapman J, Boersma WJA, Groot-egoed JA, Brinkmann AO (1993) Localization and hormonalstimulation of phosphorylation sites in the LNCaP-cell androgenreceptor. Biochemistry 291:95–101
60. Nazareth LV, Weigel NL (1996) Activation of the human andro-gen receptor through a protein kinase A signaling pathway. JBiol Chem 271:19900–19907
61. Blok LJ, de Ruiter PE, Brinkmann AO (1998) Forskolin-induceddephosphorylation of the androgen receptor impairs ligand bind-ing. Biochemistry 37:3850–3857
62. Kuil CS, Berrevoets CA, Mulder E (1995) Ligand-induced con-formational alterations of the androgen receptor analyzed bylimited trypsinization. Studies on the mechanism of antian-drogen action. J Biol Chem 270:27569–27576
63. Sanchez ER, Faber LE, Henzel WJ, Pratt, WB (1990) The 56–59kilodalton protein identified in untransformed men steroid recep-tor complexes is a unique protein that exists in the cytosol in acomplex with both the 70- and 90-kilodalton heat shock pro-teins. Biochemistry 29:5245–5252
64. Caamano CA, Morano MI, Dalman FC, Pratt WB, Akil H (1998)A conserved proline in the binding region of the glucocorticoidreceptor is required for hsp90 heterocomplex stabilization andreceptor signaling. J Biol Chem 273:20473–20480
65. Pratt WB (1993) The role of heat shock proteins in regulatingthe function, folding and trafficking of the glucocorticoid recep-tor. J Biol Chem 268:21455–21458
66. Landel CC, Kushner PJ, Greene GL (1994) The interaction ofhuman estrogen receptor with DNA is modulated by receptor-as-sociated proteins. Mol Endocrinol 8:1407–1419
67. Froesch BA, Takayama S, Reed JC (1998) BAG-1L protein en-hances androgen receptor function. J Biol Chem 237:11660–11666
68. Yeh S, Chang C (1996) Cloning and characterization of a specif-ic coactivator, ARA70, for the androgen receptor in human pros-tate cells. Proc Natl Acad Sci USA 93:5517–5521
69. Miyamoto H, Yeh S, Wilding G, Chang C (1998) Promotion ofagonist activity of antiandrogens by the androgen receptorcoactivator, ARA70, in human prostate cancer DU145 cells. ProcNatl Acad Sci USA 95:7379–7384
70. Wolf DA, Herzinger T, Hermeking H, Blaschke D, Horz W(1993) Transcriptional and posttransriptional regulation of hu-man androgen receptor expression by androgen. Mol Endocrinol7:924–936
71. Syms AJ, Nag A, Norris JS, Smith RG (1987) Glucocorticoid ef-fects on growth, and androgen regulated prostate gene. Mol CellBiochem 84:3–15
72. Henntu P, Vihko P (1993) Prostatic gene expression is modulatedby protein kinase C in LNCaP cancer cells (abstract). EndocrSoc Program, June, p 364
73. Wilson JD, Smithe EP (1987) Growth factors in the prostate.Prog Clin Biol Res 239:205–223
74. Ittman M, Mansukhani A (1997) Expression of fibroblast growthfactors (FGF’s) and FGF receptors in human prostate. J Urol157:351–356
75. Culig Z, Hobich A, Cronauer MV, Radmayr C, Trapman J, Hitt-mair A, Bartsch G, Klocker H (1994) Androgen receptor activa-tion in prostatic tumor cell lines by insulin- like growth factor-1,keratinocyte growth factor, and epidermal growth factor. CancerRes 54:5474–5478
76. Maddy SA, Chisholm GD, Hawkins RA, Habib HK (1987) Lo-calization of epidermal growth factor receptors in the humanprostate by biochemical and immunocytchemical methods. JEndocrinol 133:311–315
77. Morris GL, Dodd JG (1990) Epidermal growth factor receptormRNA levels in human prostatic tumours and cell lines. J Urol143:1272–1274
78. Schmidt JF, Hearn MT, Risbrider GP (1996) Expression of fibro-blast growth factor- 8 in adult rat tissues and human prostate car-cinoma cells. J Steroid Biochem Mol Biol 57:173–178
79. Geredes MJ, Dang TD, Larsen M, Rowley DR (1998) Trans-forming growth factor- beta1 induces nuclear to cytoplasmic dis-tribution of androgen receptor and inhibits androgen response inprostate smooth muscle cells. Endocrinology 139:3569–3577
80. Visakorpi T, Hyytinen E, Koivisto P, Tanner, M, Keinanen R,Palmberg C Palotie A, Tammela T, Isola J, Kallioniemi O-P(1995) In vivo amplification of the androgen receptor gene andprogression of human prostate cancer. Nat Genet 2:132- 134
81. Koivisto P, Kononen J, Palmberg C, Tammela T, Hyytinen E,Isola J, Trapman J, Cleutijens K, Noordzij A, Visakorpi T,Kallioniemi O (1997) Androgen receptor gene amplification: apossible molecular mechanism for androgen deprivation therapyfailure in prostate cancer. Cancer Res 57:314–319
426