textbook impingement syndrome
TRANSCRIPT
By:Gopinath
A Mutmainna RAyustia Risvani Akbar
Nurul MuchlizaHastuti
Fitra Yahya
Advisors:dr. Chaniagodr. Mervin
dr. Ricodr. Arif
Orthopaedic and Traumatology DepartmentFaculty of Medicine
Hasanuddin University2013

a painful disorder which is thought to arise from repetitive compression or rubbing of the tendons (mainly supraspinatus) under the coracoacromial arch
Apley’s System Of Orthopaedics And Fractures 9th Edition

Prevalence: 5% to 10% of the population
Predominant sex: Males more than females
Predominan Age: >40 yr
,Kennedy, John F. Ferri’s Clinical Advisor 2013. Philadelphia: Elsevier.
A combination of: Tendon overload Microvascular compromise Compression by surrounding structures
,Kennedy, John F. Ferri’s Clinical Advisor 2013. Philadelphia: Elsevier.

Netter

Repetitive overhead activity Advanced Aged Trauma
,Kennedy, John F. Ferri’s Clinical Advisor 2013. Philadelphia: Elsevier.

Repetitive compression/ stress / rubbing of tendon compressed and irritated slightly swollen impinging on the acromioclavicular arch
osteophytes on the anterior edge of the acromion
Apley’s System Of Orthopaedics And Fractures 9th Edition

Friction minor tears can develop scaring, fibrocartilaginous metaplasia or calcification in the tendon vascular reaction and local congestion further impingement
Apley’s System Of Orthopaedics And Fractures 9th Edition

Shoulder pain , with subsequent progress depends on age, stage of the disorder, and vigour of healing response.
Three Stages Stage 1:acute
inflammation,edema,hemorrhage Stage 2:fibrosis and tendinitis Stage 3:mechanical disruption of the rotator
cuff tendonsApley’s System Of Orthopaedics And Fractures 9th Edition
Due to vascular congestion, microscopic haemorrhage and oedema
Pain after vigorous or unaccustomed activity ( swimming)
Shoulder looks normal but acutely tender along the anterior edge of acromion
Apley’s System Of Orthopaedics And Fractures 9th Edition
Pain worse at night, the patient cannot lie on the affected side, comfortable to sit up out of bed.
May restrict even simple activities ( hair grooming or dressing) Age 40-50 History of recurrent attacks of subacute tendinitis
Apley’s System Of Orthopaedics And Fractures 9th Edition

Pain settling down with rest or anti inflammatory treatment and recur when more demanding activities resumed
Crepitation over the rotator cuff when shoulder is passively rotated
Small, unsuspected tears are quite often found during arthroscopy or operation
Apley’s System Of Orthopaedics And Fractures 9th Edition

The most advanced stage Resulting in either partial or full
thickness tear Aged over 45 History of refractory shoulder pain with
increasing stifness and weakness
Apley’s System Of Orthopaedics And Fractures 9th Edition
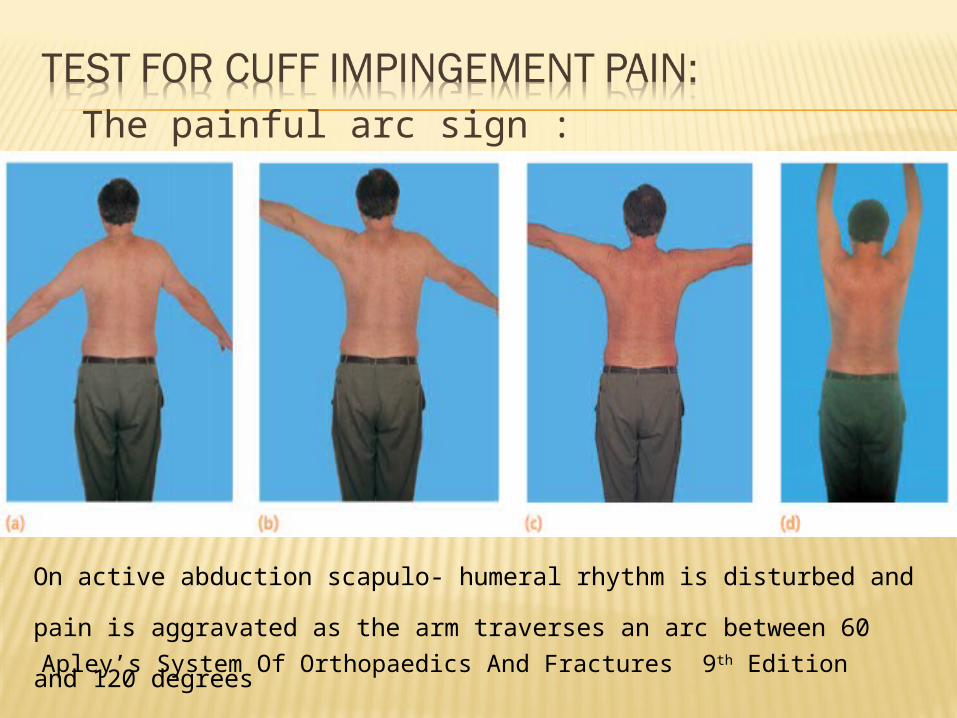
The painful arc sign :
Apley’s System Of Orthopaedics And Fractures 9th Edition
On active abduction scapulo- humeral rhythm is disturbed and pain is aggravated
as the arm traverses an arc between 60 and 120 degrees

Neer’s impingement sign
Apley’s System Of Orthopaedics And Fractures 9th Edition
the scapula is stabilized with
one hand while with the other
hand the exam- iner raises the
affected arm to the full extent
in pas- sive flexion, abduction
and internal rotation, thus
bringing the greater tuberosity
directly under the
coracoacromial arch. The test
is positive when pain, located
to the subacromial space or
anterior edge of acromion, is
elicited by this manoeuvre.

Neer’s test for impingement
If the previous manoeuvre is positive, it may be repeated after injecting 10 mL of 1 per cent lignocaine into the subacromial space; if the pain is abolished (or sig- nificantly reduced), this will help to confirm the diagnosis.
Apley’s System Of Orthopaedics And Fractures 9th Edition
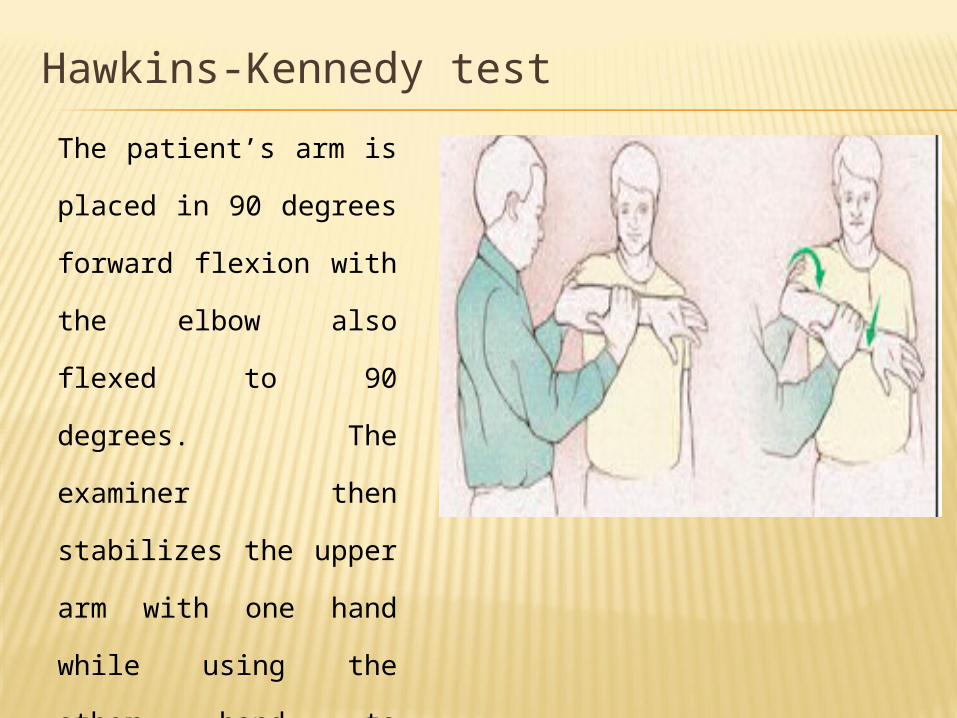
Hawkins-Kennedy testThe patient’s arm is placed
in 90 degrees forward
flexion with the elbow also
flexed to 90 degrees. The
examiner then stabilizes
the upper arm with one
hand while using the other
hand to internally rotate the
arm fully. Pain around the
anterolateral aspect of the
shoulder is noted as a
positive test.
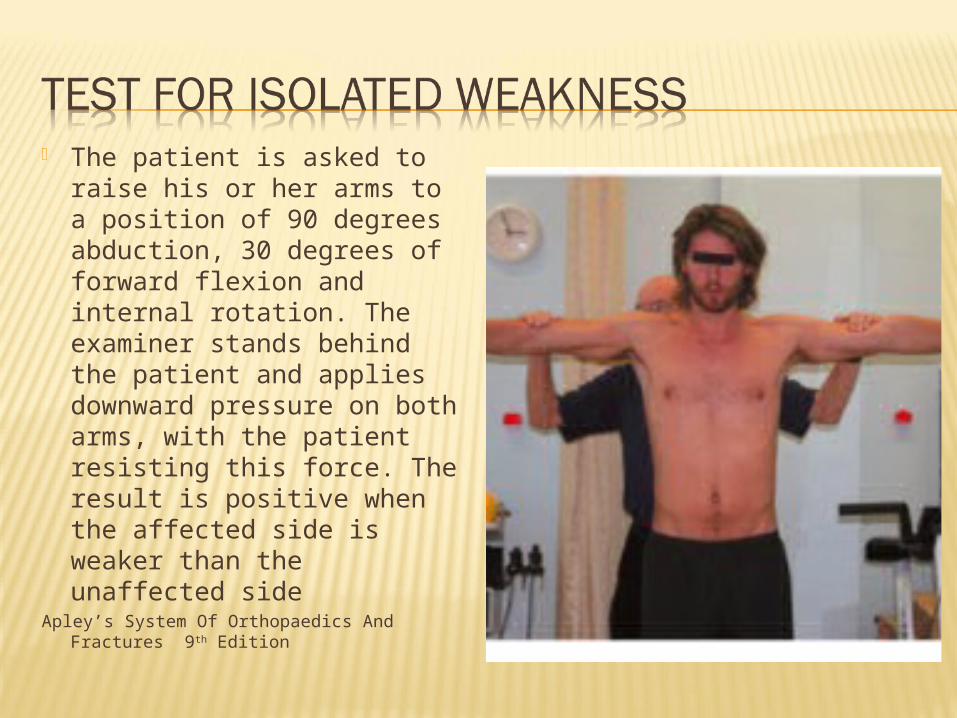
The patient is asked to raise his or her arms to a position of 90 degrees abduction, 30 degrees of forward flexion and internal rotation. The examiner stands behind the patient and applies downward pressure on both arms, with the patient resisting this force. The result is positive when the affected side is weaker than the unaffected side
Apley’s System Of Orthopaedics And Fractures 9th Edition

the patient stands holding his or her arms close to the body and the elbows flexed to 90 degrees. He or she is instructed to externally rotate both arms while the examiner applies resistance; lack of power on one side signifies weakness of infraspinatus.
Apley’s System Of Orthopaedics And Fractures 9th Edition
Apley’s System Of Orthopaedics And Fractures 9th Edition
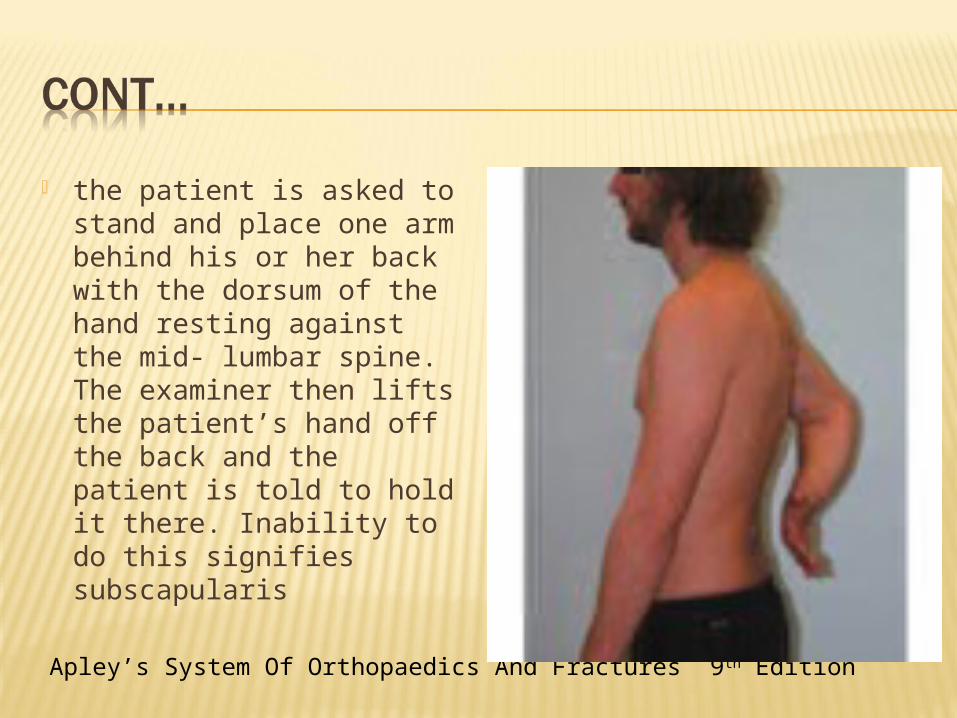
the patient is asked to stand and place one arm behind his or her back with the dorsum of the hand resting against the mid- lumbar spine. The examiner then lifts the patient’s hand off the back and the patient is told to hold it there. Inability to do this signifies subscapularis

X-ray Usually normal in early stages Chronic tendiitis : there may be erosion,
sclerosis or cyst formation In chronic cases: roughening or overgrowht
of anterior edge at the caudal tilt view Older patient and late cases: osteoarthritis
of the acromioclavicular joint
Apley’s System Of Orthopaedics And Fractures 9th Edition
USGIDENTIFYING AND MEASURING THE SIZE OF FULL THICKNESS AND PARTIAL THICKNESS ROTATOR CUFF TEARS
Apley’s System Of Orthopaedics And Fractures 9th Edition
Non-operative Operative
Apley’s System Of Orthopaedics And Fractures 9th Edition
Rest without overhead activity Physical Therapy NSAIDs for 7-10 days Subacromial glucocorticoid injections

Open AcromioplastyThrough an anterior incision the deltoid muscle is split and the part arising from the anterior edge of the acromion is dissected free, exposing the coracoacro- mial ligament, the acromion and the acromioclavicu- lar joint.The coracoacromial ligament is excised and the anteroinferior portion of the acromion is removed by an undercutting osteotomy.
Apley’s System Of Orthopaedics And Fractures 9th Edition

Excres- cences on the undersurface of the a cromioclavicular joint are pared down.
If the joint is hypertrophic, the outer 1cm of clavicle is removed; this last step exposes even more of the cuff and permits recon- struction of larger defects.
An important step is care- ful reattachment of the deltoid to the acromion, if necessary by suturing through drill holes in the acromion; failure to obtain secure attachment may lead to postoperative pain and weakness. After the operation, shoulder movements are commenced as soon as pain subsides.
Apley’s System Of Orthopaedics And Fractures 9th Edition
Apley’s System Of Orthopaedics And Fractures 9th Edition

Arthroscopic SurgeryThe underside of the acromion must be trimmed and the coracoacromial ligament divided or removed. This procedure has now become the gold standard and allows earlier rehabilitation than open acromio- plasty because detachment of the deltoid is not per- formed. Arthroscopic acromioplasty should achieve the same basic objectives as open acromioplasty Arthroscopy allows good visualization inside the gleno-humeral joint and therefore the detection of other abnormalities which may cause pain
Apley’s System Of Orthopaedics And Fractures 9th Edition

THANK YOU