teaching breaking bad news using mixed reality simulation
TRANSCRIPT
Journal of Surgical Research 159, 462–467 (2010)doi:10.1016/j.jss.2009.04.032
ASSOCIATION FOR ACADEMIC SURGERY
Teaching Breaking Bad News Using Mixed Reality Simulation
Mark W. Bowyer, M.D.,*,1 Janice L. Hanson, Ph.D.,* Elisabeth A. Pimentel, B.A.,* Amy K. Flanagan, M.F.A.,*Lisa M. Rawn, M.A.,† Anne G. Rizzo, M.D.,* E. Matthew Ritter, M.D.,* and Joseph O. Lopreiato, M.D.*
*National Capital Area Medical Simulation Center of the Uniformed Services University of the Health Sciences, Bethesda, Maryland;and †Center for Experiential Learning and Assessment, Vanderbilt University School of Medicine, Nashville, Tennessee
Submitted for publication January 9, 2009
Background. Our novel teaching approach in-volved having students actively participate in an un-successful resuscitation of a high fidelity humanpatient simulator with a gun shot wound to the chest,followed immediately by breaking bad news (BBN) toa standardized patient wife (SPW) portrayed by anactress.
Methods. Brief education interventions to includeviewing a brief video on the SPIKES protocol on howto break bad news, a didactic lecture plus a demonstra-tion, or both, was compared to no pretraining by divid-ing 553 students into four groups prior to their BBN tothe SPW. The students then self-assessed their abili-ties, and were also evaluated by the SPW on 21 itemsrelated to appearance, communication skills, and emo-tional affect. All received cross-over training.
Results. Groups were equal in prior training(2 h)and belief that this was an important skill to belearned. Students rated the experience highly, anddemonstrated marked improvement of self-assessedskills over baseline, which was maintained for the du-ration of the 12-wk clerkship. Additionally, studentswho received any of the above training prior to BBNwere rated superior to those who had no training onseveral communication skills, and the observation ofthe video seemed to offer the most efficient way ofteaching this skill in a time delimited curriculum.
Conclusion. This novel approach was well receivedand resulted in improvement over baseline. Lessonslearned from this study have enhanced our curricularapproach to this vital component of medical educa-tion. Published by Elsevier Inc.
1 To whom correspondence and reprint requests should be ad-dressed at Department of Surgery, Uniformed Services University,4301 Jones Bridge Road, Bethesda, MD 20814. E-mail: [email protected].
0022-4804/09 $36.00Published by Elsevier Inc.
462
Key Words: breaking bad news; SPIKES; simulation;mixed reality; standardized patient.
INTRODUCTION
Breaking bad news (BBN) is a reality of medical andsurgical care. Healers in ancient times (Hippocrates)were reluctant to disclose bad news, fearing that the pa-tient would take a ‘‘turn to the worse.’’ This position waslikewise adopted by the American Medical Associationin its code of medical ethics in 1847 [1]. In modern his-tory, a survey of American physicians in 1961 revealedthat 88% routinely withheld cancer diagnosis or usedeuphemisms such as ‘‘growth’’ instead of ‘‘cancer’’ [2].With this historic precedent, it is easy to understandwhy many traditionally trained physicians are un-comfortable with (and avoidant of) the job of BBN topatients and their families. Lack of skills and the reluc-tance to deal with the patient’s feelings have beenreported as the main causes for physician’s avoidanceof this task [3]. Avoidance is understandable as break-ing bad news is one of the more difficult tasks thathealth professionals have to undertake. However wellit is done, bad news is bad news. What is clear, however,is that the manner in which bad news is broken canhave a profound effect on both the recipient and thegiver. To do it badly may affect all of a patient’s (andtheir relatives’) future contact with the health care pro-fessionals involved in their treatment, and may impairtheir quality of life and well-being [4, 5].
The prevailing standard for teaching BBN is to ob-serve a peer or supervisor when he or she must deliverbad news to a patient or the family members [4]. This‘‘on the job - see one do one’’ training is highly variableas many of the ‘‘teachers’’ themselves have had no for-mal training, with the lesson being only as good as

FIG. 1. Students participate in an unsuccessful resuscitation ofa penetrating trauma scenario using a high-fidelity human patientsimulator.
BOWYER ET AL.: TEACHING BREAKING BAD NEWS USING SIMULATION 463
the physician being observed. Because negative rolemodels for giving bad news are common [6], relianceon such techniques may result in communication pat-terns that are less than optimal. Very few individualshave natural talents in this arena, but research showsthat communication is a skill that can be learned, andmany medical schools have embraced principles of ex-periential learning, and are introducing communica-tion skills training into the curriculum [7, 8].
Much has been written about the skills necessary foreffective delivery of bad news, and consensus guidelineshave been developed [4, 9–13]. The most widely usedmodel for BBN is the setting, perception, invitation,knowledge, empathy, summary and strategy (SPIKES)model developed by Buckman [14]. Based on review ofcurrent BBN literature, the optimal curriculum shouldinclude a model for effective delivery of bad news (e.g.,SPIKES), opportunities for learners to discuss issues,practice, and feedback. Successful strategies for deliv-ering BBN curricula have included didactic lectures,small-group discussions, role playing with peers andSPs, and teaching in the context of patient care (at ornear the bedside) [9]. All of the interventions describedabove have limitations, but have been highly rated bylearners, and have demonstrated impact on learnerself confidence and, in some cases, learner knowledgeand behaviors.
The increased availability and use of standardizedpatients (SPs) to teach medical interviewing and phys-ical exam skills has led to a logical extension to teachingother communication skills, such as BBN. TraditionallySPs, virtual reality part task trainers, and manikinshave been used as separate tools in the teaching arma-mentarium. A natural extension of these tools is to com-bine them in ways to maximize their effectiveness. Thishas alternatively been referred to as blended, hybrid, ormixed reality simulation [15–17]. Mixed reality simula-tion combines SPs with part task trainers or high fidel-ity human patient simulators. For instance, a traineemay be asked to place a urinary catheter into a model,which appears to be part of an actual person (SP).This adds to the experience by training the student incommunication and sensitivity to the patient while heor she performs the procedural skill. This blended ap-proach has also been used to teach skills such as endos-copy [18, 19]. We have previously described a pilotmixed reality approach to teaching medical studentsto BBN in which the student participates in the unsuc-cessful resuscitation of a high fidelity human patientsimulator with gunshot wounds to the chest, followedimmediately by BBN to a standardized patient wife(SPW) portrayed by an actress [20]. This paper de-scribes our further experience with this mixed realityapproach to teaching medical students to BBN, andcompares different ways of delivering the curriculum.
MATERIALS AND METHODS
As part of the third-year Introduction to Surgery Clerkship curric-ulum, 553 third-year medical students participated in a formativeclinical skills laboratory that introduced them to the skills theyneed on the surgical wards. Each student went through a series ofskills stations in groups of four students. One of these stations wasa trauma resuscitation simulation in which the student team wasasked to treat a patient arriving in the trauma bay of the emergencyroom. The patient in this case was a high-fidelity human simulatormanikin moulaged and programmed to portray a multiple gunshotvictim who sustained wounds across the face and to the left chest.The student teams were then asked to evaluate and treat this patientwho was in extremis with airway compromise and profound shock(Fig. 1). Despite their best efforts the patient died. After completingthis scenario, the students were debriefed by one of the faculty andthen informed that the rest of the surgical team was in the operatingroom with another patient, and that the wife of the recently deceasedpatient was in the waiting room demanding information. The stu-dents were then informed that it was their responsibility to speakindividually with the patient’s wife and inform her that her husbandhad died. Just prior to meeting the wife, the students received a 10-min orientation in which they discussed with a faculty facilitatorthe sequence of events during the resuscitation, and were given addi-tional information about the patient and the events of the shooting.
Simulated patient wives (SPWs) were recruited from a very large,well-experienced pool of actors who work frequently in our center asSPs. The actresses were provided a script with detailed written de-scription of the scenario and the role that they were to play, and un-derwent training with practice sessions with one of the faculty(MB). The practice sessions as well as initial student session were vid-eotaped and used for ongoing training of the SPWs. Over the course ofthe study, a total of eight actresses were used. At any given time, onlytwo SPWs were in individual rooms with a student and the otherswere able to observe live time via room mounted cameras. This ledto remarkable standardization of the role to be played by the SPW.The SPWs displayed appropriate and realistic emotional responsesto include shock, grief, and anger (Fig. 2). The SPWs were blindedto the students’ training prior to their encounter and on conclusionevaluated each student using a 5 point Likert scale on 21 items relatedto the student’s appearance, communication skills, and emotionalaffect.
In an effort to determine the best curricular approach to teachingthis important skill to medical students, we designed a study to com-pare various pretraining schemes to no training prior to the studentspeaking to the wife. Institutional Review Board approval wasgranted as well as permission from the Dean of Students and the

FIG. 2. Students must break the bad news to the patient’s wife that despite their best efforts her husband has died. The standardizedpatient wife (SPW), who has been trained specifically for this scenario, displays a range of appropriate and realistic emotions to include shock(left) and grief (right) as depicted above.
FIG. 3. Comparison of the groups pre- and post-encounter, andpost-rotation on self-assessed response (5 point Likert scale) to thequestion–Do you currently feel better prepared to break bad news?The graphs represent the mean of the responses at the time intervalsdescribed with P values coinciding to a Student t-test comparison ofthe two means indicated by the enclosed arrows.
JOURNAL OF SURGICAL RESEARCH: VOL. 159, NO. 1, MARCH 2010464
Commandant to enroll students in the study. For the purpose of thestudy, all 553 students completed a baseline pre-encounter question-naire about their experiences with and preparedness (5 point Likertscale) for delivering bad news to patients, and were then randomlydivided into four groups as follows:
Group 1 (n [ 163)
After participating in the unsuccessful trauma resuscitation andreceiving the orientation as described above, these students weretasked to BBN to the SPW without any pretraining.
Group 2 (n [ 163)
These students were similar to group 1 with the exception that theywatched a 15 min video on the SPIKES model (while group 1 wasspeaking to the SPW) just prior to speaking to the patient’s wife.
Group 3 (n [ 109)
On the day prior to the resuscitation/BBN scenario, these studentsreceived a 45 min didactic lecture on BBN that included the SPIKESprotocol. In addition, in small, proctored groups, they observed anexample of a faculty facilitator informing a woman (SP) that shehad miscarried, using the SPIKES protocol with subsequent discus-sion of the event. On the following day, these students spoke to theSPW immediately after the unsuccessful resuscitation event and brieforientation.
Group 4 (n [ 118)
These students received the same training as group 3, but in addi-tion watched the 15 min SPIKES method video just prior to speakingto the SPW.
Though all four groupswere aware that BBN would be covered in thecurriculum by virtue of it being a skill listed on the schedule, none ofthem were aware of the circumstances in which they would have topractice it until just after the unsuccessful resuscitation exercise.
Immediately after the encounter, all four groups completed a post-encounter questionnaire (5 point Likert scale) that self-assessed theirability to have a plan for, and to break, bad news. In addition, the per-formance of each student while speaking with the SPW was observedreal time by one of the faculty (MB). After the event, a 20 min debrief-ing was performed with the four students in each small group. Eachstudent was evaluated by the SPW they encountered using the 21item checklist previously described. The SPWs were blinded to thestudent groups. All groups received cross-over training, such that
all had the benefit of the didactic lecture, small group demonstrationand discussion, and the SPIKES method video by the end of the 2d curriculum. On the last day of the 12 wk rotation, each student com-pleted a post-rotational questionnaire (5 point Likert scale) that self-assessed their ability to have a plan for, and to break, bad news. Thesepost-rotational results were self-reported, and there was no directobservation of student performance recorded.
Statistical analysis of the responses to the pre-encounter, post-encounter, post-rotation questionnaires, and SPW checklist evaluationof the students was undertaken using the Student’s t-test and one wayrepeated measures ANOVA as appropriate with a set at P < 0.05.
RESULTS
The groups were equal in terms of their self-reportedprevious breaking bad news training (mean 2.45 6
2.37 h, with a range of 0–10 h). It is notable that 97 stu-dents (17.5%) self-reported 0 h of training in spite ofBBN being included in the first year curriculum aspart of communication skills. Of the 377 students whohad completed at least one clinical rotation, 17% (64)had been placed in a situation where they, as a third
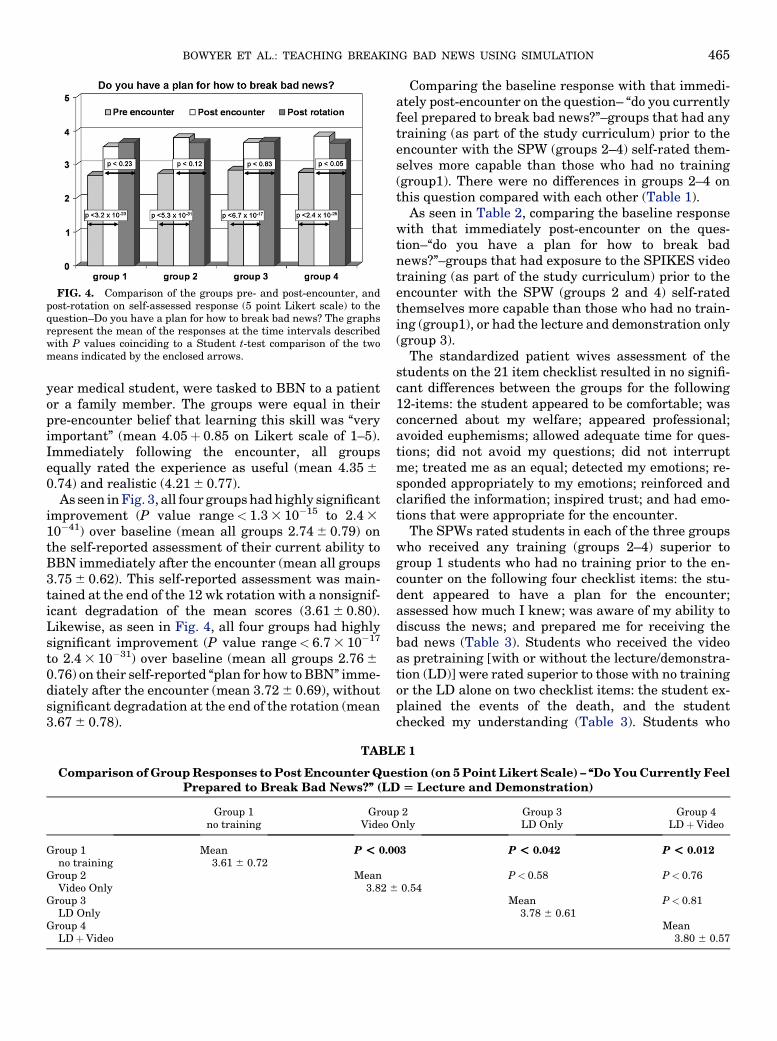
FIG. 4. Comparison of the groups pre- and post-encounter, andpost-rotation on self-assessed response (5 point Likert scale) to thequestion–Do you have a plan for how to break bad news? The graphsrepresent the mean of the responses at the time intervals describedwith P values coinciding to a Student t-test comparison of the twomeans indicated by the enclosed arrows.
BOWYER ET AL.: TEACHING BREAKING BAD NEWS USING SIMULATION 465
year medical student, were tasked to BBN to a patientor a family member. The groups were equal in theirpre-encounter belief that learning this skill was ‘‘veryimportant’’ (mean 4.05þ 0.85 on Likert scale of 1–5).Immediately following the encounter, all groupsequally rated the experience as useful (mean 4.35 6
0.74) and realistic (4.21 6 0.77).As seen in Fig. 3, all four groups had highly significant
improvement (P value range< 1.3 3 10�15 to 2.4 3
10�41) over baseline (mean all groups 2.74 6 0.79) onthe self-reported assessment of their current ability toBBN immediately after the encounter (mean all groups3.75 6 0.62). This self-reported assessment was main-tained at the end of the 12 wk rotation with a nonsignif-icant degradation of the mean scores (3.61 6 0.80).Likewise, as seen in Fig. 4, all four groups had highlysignificant improvement (P value range< 6.7 3 10�17
to 2.4 3 10�31) over baseline (mean all groups 2.76 6
0.76) on their self-reported ‘‘plan for how to BBN’’ imme-diately after the encounter (mean 3.72 6 0.69), withoutsignificant degradation at the end of the rotation (mean3.67 6 0.78).
TABL
Comparison of Group Responses to Post Encounter QuePrepared to Break Bad News?’’ (LD
Group 1no training
GrouVideo O
Group 1no training
Mean3.61 6 0.72
P < 0.0
Group 2Video Only
Mean3.82 6
Group 3LD Only
Group 4LDþVideo
Comparing the baseline response with that immedi-ately post-encounter on the question– ‘‘do you currentlyfeel prepared to break bad news?’’–groups that had anytraining (as part of the study curriculum) prior to theencounter with the SPW (groups 2–4) self-rated them-selves more capable than those who had no training(group1). There were no differences in groups 2–4 onthis question compared with each other (Table 1).
As seen in Table 2, comparing the baseline responsewith that immediately post-encounter on the ques-tion–‘‘do you have a plan for how to break badnews?’’–groups that had exposure to the SPIKES videotraining (as part of the study curriculum) prior to theencounter with the SPW (groups 2 and 4) self-ratedthemselves more capable than those who had no train-ing (group1), or had the lecture and demonstration only(group 3).
The standardized patient wives assessment of thestudents on the 21 item checklist resulted in no signifi-cant differences between the groups for the following12-items: the student appeared to be comfortable; wasconcerned about my welfare; appeared professional;avoided euphemisms; allowed adequate time for ques-tions; did not avoid my questions; did not interruptme; treated me as an equal; detected my emotions; re-sponded appropriately to my emotions; reinforced andclarified the information; inspired trust; and had emo-tions that were appropriate for the encounter.
The SPWs rated students in each of the three groupswho received any training (groups 2–4) superior togroup 1 students who had no training prior to the en-counter on the following four checklist items: the stu-dent appeared to have a plan for the encounter;assessed how much I knew; was aware of my ability todiscuss the news; and prepared me for receiving thebad news (Table 3). Students who received the videoas pretraining [with or without the lecture/demonstra-tion (LD)] were rated superior to those with no trainingor the LD alone on two checklist items: the student ex-plained the events of the death, and the studentchecked my understanding (Table 3). Students who
E 1
stion (on 5 Point Likert Scale) – ‘‘Do You Currently Feel[ Lecture and Demonstration)
p 2nly
Group 3LD Only
Group 4LDþVideo
03 P < 0.042 P < 0.012
0.54P< 0.58 P< 0.76
Mean3.78 6 0.61
P< 0.81
Mean3.80 6 0.57
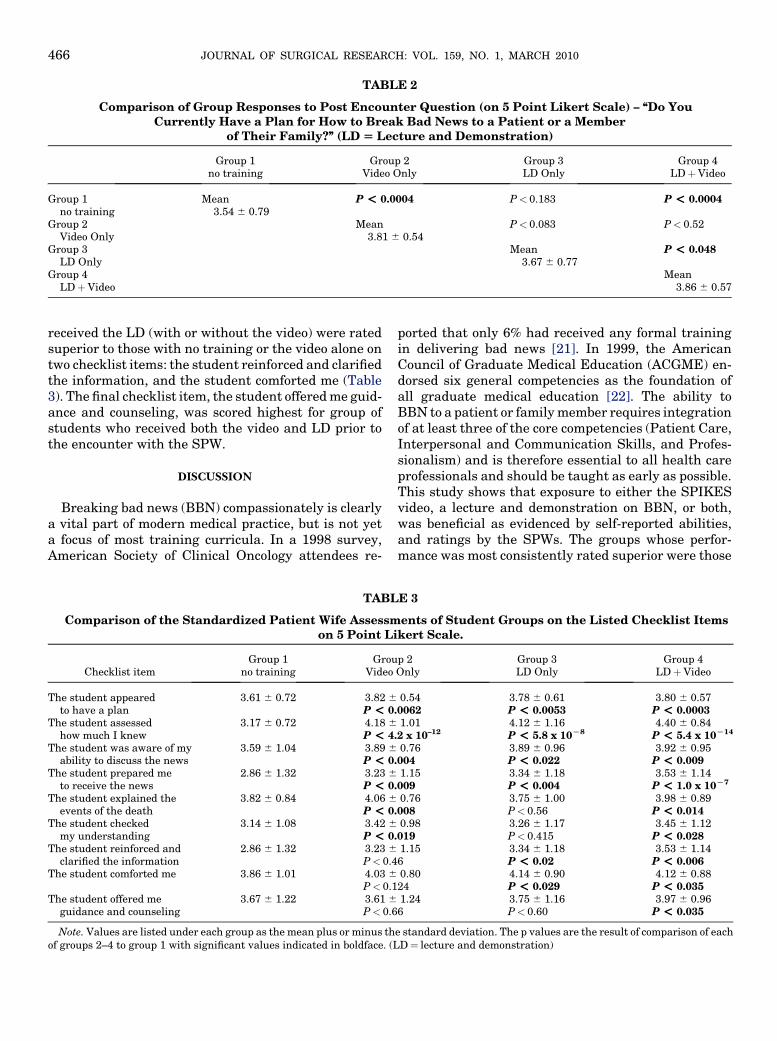
TABLE 2
Comparison of Group Responses to Post Encounter Question (on 5 Point Likert Scale) – ‘‘Do YouCurrently Have a Plan for How to Break Bad News to a Patient or a Member
of Their Family?’’ (LD [ Lecture and Demonstration)
Group 1no training
Group 2Video Only
Group 3LD Only
Group 4LDþVideo
Group 1no training
Mean3.54 6 0.79
P < 0.0004 P< 0.183 P < 0.0004
Group 2Video Only
Mean3.81 6 0.54
P< 0.083 P< 0.52
Group 3LD Only
Mean3.67 6 0.77
P < 0.048
Group 4LDþVideo
Mean3.86 6 0.57
JOURNAL OF SURGICAL RESEARCH: VOL. 159, NO. 1, MARCH 2010466
received the LD (with or without the video) were ratedsuperior to those with no training or the video alone ontwo checklist items: the student reinforced and clarifiedthe information, and the student comforted me (Table3). The final checklist item, the student offered me guid-ance and counseling, was scored highest for group ofstudents who received both the video and LD prior tothe encounter with the SPW.
DISCUSSION
Breaking bad news (BBN) compassionately is clearlya vital part of modern medical practice, but is not yeta focus of most training curricula. In a 1998 survey,American Society of Clinical Oncology attendees re-
TABL
Comparison of the Standardized Patient Wife Assessmon 5 Point Li
Checklist itemGroup 1
no trainingGrou
Video
The student appearedto have a plan
3.61 6 0.72 3.82 6
P < 0The student assessed
how much I knew3.17 6 0.72 4.18 6
P < 4The student was aware of my
ability to discuss the news3.59 6 1.04 3.89 6
P < 0The student prepared me
to receive the news2.86 6 1.32 3.23 6
P < 0The student explained the
events of the death3.82 6 0.84 4.06 6
P < 0The student checked
my understanding3.14 6 1.08 3.42 6
P < 0The student reinforced and
clarified the information2.86 6 1.32 3.23 6
P< 0.4The student comforted me 3.86 6 1.01 4.03 6
P< 0.1The student offered me
guidance and counseling3.67 6 1.22 3.61 6
P< 0.6
Note. Values are listed under each group as the mean plus or minus thof groups 2–4 to group 1 with significant values indicated in boldface. (L
ported that only 6% had received any formal trainingin delivering bad news [21]. In 1999, the AmericanCouncil of Graduate Medical Education (ACGME) en-dorsed six general competencies as the foundation ofall graduate medical education [22]. The ability toBBN to a patient or family member requires integrationof at least three of the core competencies (Patient Care,Interpersonal and Communication Skills, and Profes-sionalism) and is therefore essential to all health careprofessionals and should be taught as early as possible.This study shows that exposure to either the SPIKESvideo, a lecture and demonstration on BBN, or both,was beneficial as evidenced by self-reported abilities,and ratings by the SPWs. The groups whose perfor-mance was most consistently rated superior were those
E 3
ents of Student Groups on the Listed Checklist Itemskert Scale.
p 2Only
Group 3LD Only
Group 4LDþVideo
0.54.0062
3.78 6 0.61P < 0.0053
3.80 6 0.57P < 0.0003
1.01.2 x 10–12
4.12 6 1.16P < 5.8 x 10L8
4.40 6 0.84P < 5.4 x 10L14
0.76.004
3.89 6 0.96P < 0.022
3.92 6 0.95P < 0.009
1.15.009
3.34 6 1.18P < 0.004
3.53 6 1.14P < 1.0 x 10L7
0.76.008
3.75 6 1.00P< 0.56
3.98 6 0.89P < 0.014
0.98.019
3.26 6 1.17P< 0.415
3.45 6 1.12P < 0.028
1.156
3.34 6 1.18P < 0.02
3.53 6 1.14P < 0.006
0.8024
4.14 6 0.90P < 0.029
4.12 6 0.88P < 0.035
1.246
3.75 6 1.16P< 0.60
3.97 6 0.96P < 0.035
e standard deviation. The p values are the result of comparison of eachD¼ lecture and demonstration)

BOWYER ET AL.: TEACHING BREAKING BAD NEWS USING SIMULATION 467
that watched the SPIKES video immediately prior tospeaking to the SPW. The addition of the didactic lec-ture and observation of a demonstration enhanced theexperience in a less pronounced fashion and requiredsignificant additional time in the curriculum. The opti-mal tool and curriculum for teaching this importantskill remains to be defined. It is clear from this studythat students benefit from formal training in how toBBN, and with a time-limited curriculum, the exposureto the SPIKES video provided the ‘‘most bang for thebuck.’’ There is little doubt that more time spent ondemonstrations, lectures, small group discussion, andmentored practice with extensive debriefing would bebeneficial and enhance the experience, but is impracti-cal in this clerkship setting. There may well be a role fordevoting more time to this skill earlier in the medicalschool curriculum as well as reinforcing it during eachof the clinical rotations in a more formal way. Thisstudy was limited by the practicalities of a time-limitedcurriculum and, unfortunately, further measures of du-rability such as re-examining the students at the end ofthe rotation in another simulated experience, observingthe student perform in a real life setting, and obtaininglonger term follow-up, were not feasible. It is hoped thatthese factors, in addition to including other clinical sit-uations in which students might have to break BBN,might be addressed in further studies of this topic.
CONCLUSION
This novel approach to teaching BBN to third-yearmedical students was well received by the students,and resulted in marked improvement of self-assessedskills over baseline. Lessons learned from this studyhave enhanced our curricular approach to this vitalcomponent of medical education.
REFERENCES
1. Schoefl R. Breaking bad news. Dig Dis 2008;26:56.
2. Oken D. What to tell cancer patients: A study of medical atti-tudes. JAMA 1961;175:1120.
3. Dosanjh S, Barnes J, Bhandari M. Barriers to breaking bad newsamong medical and surgical residents. Med Educ 2001;35:197.
4. Ptacek JT, Eberhardt TL. Breaking bad news: A review of theliterature. JAMA 1996;276:496.
5. Garg A, Buckman R, Kason Y. Teaching medical students tobreak bad news. Can Med Assoc J 1997;156:1159.
6. Fallowfield L, Jenkins V. Communicating sad, bad, and difficultnews in medicine. Lancet 2004;363:312.
7. Kalet A, Pugnaire MP, Cole-Kelly K, et al. Teaching communica-tion in clinical clerkships: Models from the Macy initiative inhealth communications. Acad Med 2004;79:511.
8. Wagner PJ, Lentz L, Heslop SD. Teaching communication skills:A skills-based approach. Acad Med 2002;77:1164.
9. Rosenbaum ME, Ferguson KJ, Lobas JG. Teaching medicalstudents and residents skills for delivering bad news: A reviewof strategies. Acad Med 2004;79:107.
10. Girgis A, Sanson-Fisher RW. Breaking bad news: Consensusguidelines for medical practitioners. J Clin Oncol 1995;13:2449.
11. Buckman R. Breaking bad news: Why is it so difficult? Br Med J1984;288:1597.
12. Rabow MW, McPhee SJ. Beyond breaking bad news: How to helppatients who suffer. West J Med 1999;171:260.
13. Ellis PM, Tattersall MH. How should doctors communicate thediagnosis of cancer to patients? Ann Med 1999;31:336.
14. Baile WF, Buckman R, Lenzia R, et al. SPIKES—A six-step pro-tocol for delivering bad news: Application to the patient withcancer. Oncologist 2000;5:302.
15. Hughes CE, Stapleton CB, Hughes DE, et al. Mixed reality in ed-ucation, entertainment, and training. IEEE Comput Graph Appl2005;25:24.
16. Noeller TP, Smith MD, Holmes L, et al. A theme-based hybridsimulation model to train and evaluate emergency medicineresidents. Acad Emerg Med 2008;15:1199.
17. Seagull FJ, Moses G, Park AE. Integration of virtual reality andconventional skills trainers: A mixed resource model. StudHealth Technol Inform 2008;132:446.
18. Kneebone RL, Nestel D, Moorthy K, et al. Learning the skills offlexible sigmoidoscopy —the wider perspective. Med Educ 2003;37(Suppl 1):50.
19. Kneebone RL, Kidd J, Nestel D, et al. Blurring the boundaries:scenario-based simulation in a clinical setting. Med Educ 2005;39:580.
20. Bowyer MW, Rawn L, Hanson J, et al. Combining high-fidelityhuman patient simulators with a standardized family member:A novel approach to teaching breaking bad news. Stud HealthTechnol Inform 2006;119:67.
21. Arnold SJ, Koczwara B. Breaking bad news: Learning throughexperience. J Clin Oncol 2006;24:5098.
22. http://www.acgme.org/outcome/comp/compMin.asp.