syphilis - s abrahammeningovascular syphilis 9infectious arteritis-> thrombi & infarcts...
TRANSCRIPT

CASE PRESENTATIONCASE PRESENTATION
S. AbrahamS. Abraham

A.Y, 53yr Indian MaleA.Y, 53yr Indian MaleHxHx: one day history: one day historyTypical chest painTypical chest painGrade NYHA 3Grade NYHA 3--443 pillow orthopnoea3 pillow orthopnoeaClass 2Class 2--3 angina and Grade 2 NYHA dyspnoea3 angina and Grade 2 NYHA dyspnoeafor past 2yearsfor past 2years
PMHx: PMHx: Previous Previous anteroseptalanteroseptal MI with left ventricular MI with left ventricular dysfunction(EFdysfunction(EF 18) and L parietal CVA 18) and L parietal CVA secondary to secondary to intracardiacintracardiac thrombus in 2006.On thrombus in 2006.On Warfarin.Warfarin.Aortic regurgitation diagnosed 2006Aortic regurgitation diagnosed 2006
History cont..History cont..
PSHxPSHx: nil: nilAllergiesAllergies:Nil:NilSocial HxSocial Hx : Smoking history 60pack years: Smoking history 60pack years
Never consumed alcohol or other Never consumed alcohol or other drugsdrugsselfself--employed businessmanemployed businessman
Family historyFamily history--No history IHD No history IHD

ExaminationExamination
Well looking middle aged maleWell looking middle aged maleConscious and coConscious and co--operativeoperativeDistressedDistressedNo pallor, cyanosis, oedemaNo pallor, cyanosis, oedemaNo skin lesions No skin lesions

Examination cont..Examination cont..
BP: 131/54, equal in all limbsBP: 131/54, equal in all limbsPulse: 76/min, regular, low volume, all Pulse: 76/min, regular, low volume, all pulses equal and palpablepulses equal and palpableRESPRESP::RR 28/minRR 28/minIncreased AP diameterIncreased AP diameterHyperinflated,liverHyperinflated,liver dullness 7dullness 7thth ICSICSBibasalBibasal crepitationscrepitations

Examination contExamination cont……..CVSCVSJVP raised 5cmJVP raised 5cmApex 6Apex 6thth ICS ICS AAL,hypodynamicAAL,hypodynamicL L parasternalparasternal heave presentheave presentEDM 2/4 aortic EDM 2/4 aortic area,loudestarea,loudest left left sternalsternalborderborderLoud P2Loud P2

Examination contExamination cont……
ABDABD::Soft ,non tenderSoft ,non tenderShifting dullness presentShifting dullness present
CNSCNS: normal higher mental function: normal higher mental functionno no meningismmeningismno focal no focal motor,sensorymotor,sensory ,motor or ,motor or cerebellarcerebellar signs signs

ECGECG

SummarySummary52 year old male with background of CAD 52 year old male with background of CAD and LV dysfunction and strong smoking and LV dysfunction and strong smoking historyhistoryCongestive cardiac failure in the setting of Congestive cardiac failure in the setting of ACSACSCOPDCOPDAortic regurgitation for further investigationAortic regurgitation for further investigation

ValvularValvularRheumatic heart Rheumatic heart Disease(unlikelyDisease(unlikely))SyphilisSyphilisRheumatoid Rheumatoid spondylosisspondylosisInfective Infective endocarditisendocarditis
Aortic rootAortic rootHPTHPTArtherosclerosisArtherosclerosisSyphilisSyphilisCollagen vascular Collagen vascular dsds--TakayasusTakayasusRheumatoid Rheumatoid AnkylosingAnkylosing spondylosisspondylosis

InvestigationsInvestigations
FBC: WCC 6.7/Hb 13.8/MCV 93/Plts 173FBC: WCC 6.7/Hb 13.8/MCV 93/Plts 173U&E: Na 137/K 4.6/Cl 108/CO2 24/U&E: Na 137/K 4.6/Cl 108/CO2 24/UU12.5/Creat 12912.5/Creat 129Clotting profile :Clotting profile :INR 5.32INR 5.32Cardiac enzymes: Cardiac enzymes: Trop I >100,CK 894Trop I >100,CK 894LFTsLFTs: ALP 49/Tbil 15/TP 61/Alb 36/GGT : ALP 49/Tbil 15/TP 61/Alb 36/GGT 32/ALT 4932/ALT 49Lipid Lipid profile:Tgprofile:Tg 1.03/Chol 4.5/HDL 1.03/Chol 4.5/HDL 0.68/LDL 3.40.68/LDL 3.4

Investigations contInvestigations cont……
HIV negativeHIV negativeRPR RPR positive(Titrepositive(Titre 1:64)1:64)Lung function testsLung function testsFEV1/FVCFEV1/FVC--(1.47/2.09) (1.47/2.09) 70 % with no 70 % with no reversibilityreversibility

CXRCXR

EchoEcho
EECCHHOO::
NNPVPVDilated 60mmDilated 60mmLALA
Dilated, EF 40,EDD 89, Dilated, EF 40,EDD 89, ESD 70, FS 18ESD 70, FS 18
LVLV
Min thickening, mod AR, Min thickening, mod AR, SystSyst peak flow1.5m/s,Ao peak flow1.5m/s,Ao root 30mmroot 30mm
Ao VAo V
Minimal thickening, trace Minimal thickening, trace MRMR
MVMV
NNPericPeric
N,PAS 34N,PAS 34TVTV
Mildly dilatedMildly dilatedRARA
DilatedDilatedRVRV

Management and progressManagement and progress
Managed as Non ST elevation Myocardial Managed as Non ST elevation Myocardial infarction`andinfarction`and diuresisdiuresis optimisedoptimised..Subsequent angiogram showed normal Subsequent angiogram showed normal coronaries with global hypokinesiscoronaries with global hypokinesisTPHA positive and treated with TPHA positive and treated with BenzathineBenzathine Penicillin 2.4 MU weekly for 3 Penicillin 2.4 MU weekly for 3 weeksweeks
LP done LP done ––normal normal PolysPolys nil/ nil/ LympLymp nil/TP 0.26/Globulin no nil/TP 0.26/Globulin no increase/increase/GluGlu 3.26/ VDRL and 3.26/ VDRL and FTAFTA--AB pending AB pending
Presented to IALCH for Presented to IALCH for AVRAVR notnot for for surgerysurgery

52 year old male with Tertiary Syphilis 52 year old male with Tertiary Syphilis with Cardiovascular complicationswith Cardiovascular complicationsAortic regurgitationAortic regurgitationCoronary artery involvementCoronary artery involvementCOPDCOPD

TERTIARY SYPHILISTERTIARY SYPHILIS

SYPHILISSYPHILIS
Chronic infectious disease caused by Chronic infectious disease caused by TreponemaTreponema pallidumpallidumManagement is based on 3 stages of disease:Management is based on 3 stages of disease:EARLY: primary/ secondary/latentEARLY: primary/ secondary/latentLATE OR TERTIARY: LATE OR TERTIARY: -- CardiovascularCardiovascular-- GummatousGummatous syphilissyphilis-- NeurosyphilisNeurosyphilis

EPIDEMIOLOGYEPIDEMIOLOGY
Common in Common in preantibioticpreantibiotic era in 20era in 20--30% of 30% of pts with syphilispts with syphilis
Currently common in patients with HIV Currently common in patients with HIV --often have early often have early neurosyphilisneurosyphilis, most , most commonly asymptomatic and symptomatic commonly asymptomatic and symptomatic meningitis, with ocular diseasemeningitis, with ocular disease

PATHOGENESISPATHOGENESISCellular immunity plays a roleCellular immunity plays a role
Waning immunity with age allows reactivation of Waning immunity with age allows reactivation of the spirochete that have sequestered in these the spirochete that have sequestered in these sites.sites.
Alternatively re infection occurs in a partially Alternatively re infection occurs in a partially immune hypersensitive host leading to a chronic immune hypersensitive host leading to a chronic inflammatory inflammatory response.(gummasresponse.(gummas))
Small vessel Small vessel vasculitisvasculitis

GUMMATOUS SYPHILISGUMMATOUS SYPHILIS
Skin, bones, or internal organs Skin, bones, or internal organs Range from small to very large Range from small to very large Visceral Visceral gummasgummas may present as a mass may present as a mass lesion lesion
CARDIOVASCULAR SYPHILISCARDIOVASCULAR SYPHILIS
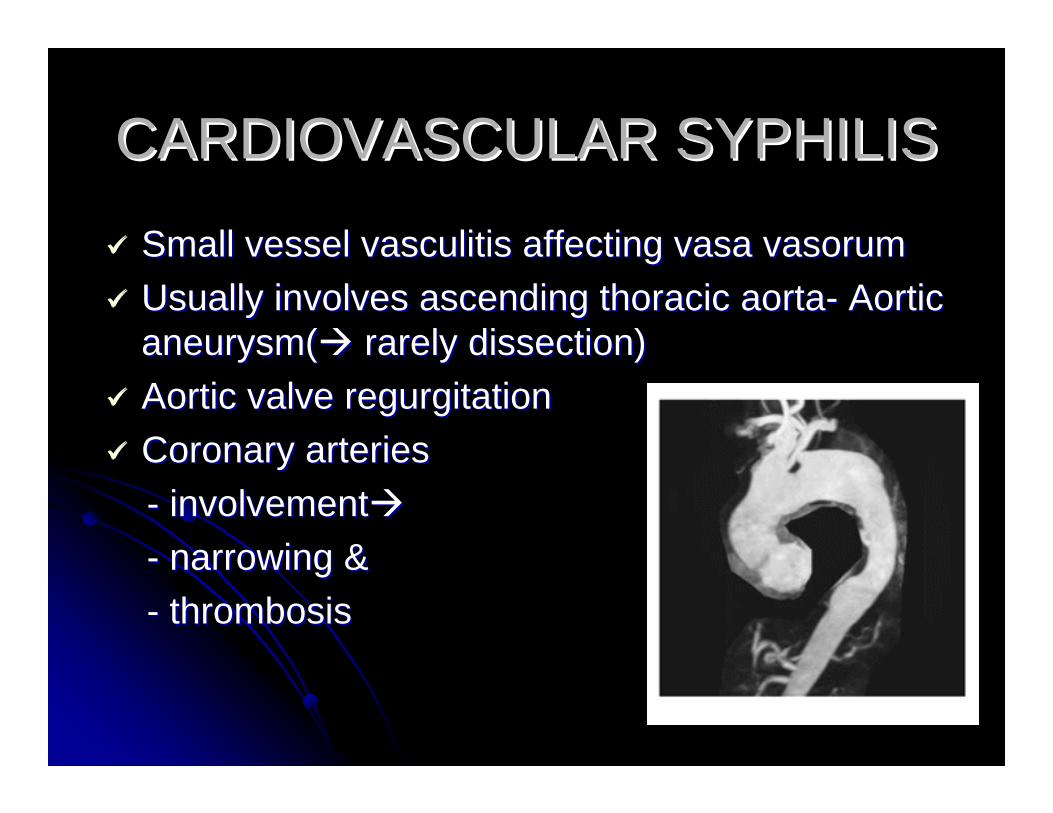
Small vessel Small vessel vasculitisvasculitis affecting affecting vasavasa vasorumvasorumUsually involves ascending thoracic aortaUsually involves ascending thoracic aorta-- Aortic Aortic aneurysm(aneurysm( rarely dissection) rarely dissection) Aortic valve regurgitationAortic valve regurgitationCoronary arteries Coronary arteries -- involvementinvolvement-- narrowing &narrowing &-- thrombosisthrombosis

CVS contCVS cont……..
Most present with asymptomatic murmur, Most present with asymptomatic murmur, or left heart failureor left heart failureOccur 15Occur 15--30 yrs from initial Ix30 yrs from initial IxCXRCXR calcification ascending arch of calcification ascending arch of aorta (not seen with aorta (not seen with arterosclerosisarterosclerosis))Coronary Coronary ostialostial stenosisstenosis may be found on may be found on catheterization catheterization

NEUROSYPHILISNEUROSYPHILIS
Can occur any time after initial infectionCan occur any time after initial infectionEarly disease involves: CSF, Early disease involves: CSF, meningesmeninges, and , and vasculature vasculature
-- Asymptomatic meningitisAsymptomatic meningitis-- Symptomatic meningitisSymptomatic meningitis-- MeningovascularMeningovascular diseasedisease
Late disease involves brain and spinal cordLate disease involves brain and spinal cord-- General paresis of insaneGeneral paresis of insane-- TabesTabes dorsalisdorsalis

Asymptomatic Meningitis Asymptomatic Meningitis
No symptoms or signs of CNSNo symptoms or signs of CNS
Can occur within wks Can occur within wks –– months after Ix, months after Ix, uncommonly >2yrs after Ixuncommonly >2yrs after Ix
CSF: CSF: lymphocyticlymphocytic pleocytosispleocytosis >20cells >20cells //ulul, protein (0.46, protein (0.46--1), positive VDRL1), positive VDRL

Symptomatic meningitisSymptomatic meningitis
Often occurs within 1Often occurs within 1stst yr after Ix yr after Ix uncommonly yrs lateruncommonly yrs laterSymptoms: headache, confusion, N & V, Symptoms: headache, confusion, N & V, and stiff neck and stiff neck UveitisUveitis, retinitis, or optic neuritis, retinitis, or optic neuritisLeptomeningitis,GummaLeptomeningitis,GummaCranial neuropathy common: CNII, CNVII, Cranial neuropathy common: CNII, CNVII, CNVIIICNVIIIHydrocephalusHydrocephalus
ArteritisArteritis of of small,mediumsmall,medium or large vesselsor large vessels
SeizuresSeizures
Uncommonly affects Spinal Cord: Uncommonly affects Spinal Cord: meningomyelitismeningomyelitis, , polyradiculopathypolyradiculopathy, , hyperplastichyperplasticpachymeningitispachymeningitis
CSF CSF AbNAbN: lymphocyte <> 200: lymphocyte <> 200--400, protein <> 400, protein <> 100100--200mg/dl, VDRL always +200mg/dl, VDRL always +
Imaging: features of meningitis &/or Imaging: features of meningitis &/or gummasgummas

MeningovascularMeningovascular syphilis syphilis Infectious Infectious arteritisarteritis--> thrombi & infarcts> thrombi & infarcts
Onset any time from 1sr monthsOnset any time from 1sr months-- 11stst few years, few years, average 7yrsaverage 7yrs
May be seen as stroke in young personMay be seen as stroke in young person
ProdromalProdromal symptoms presentsymptoms present
Acute or chronic stroke usually of MCA branches, Acute or chronic stroke usually of MCA branches, rarely Ant spinal A.rarely Ant spinal A.--> SC infarct> SC infarct
CSF CSF abNabN: lymphocyte : lymphocyte pleocytosispleocytosis <> 10<> 10--100 & 100 & protein <>100protein <>100--200, VDRL usually positive200, VDRL usually positive

General paresisGeneral paresis
Progressive Progressive dementingdementing illnessillnessusually 10usually 10--25 yrs after Ix25 yrs after Ixchronic progressive chronic progressive frontotemporalfrontotemporalmeningoencephalitismeningoencephalitis with loss of with loss of cortical functioncortical functionearly stage: forgetfulnessearly stage: forgetfulnesslate stage : severe dementialate stage : severe dementia

P P –– personalitypersonalityA A –– affectaffectR R –– reflexes (brisk)reflexes (brisk)E E –– eye (Argyll Robertson pupil)eye (Argyll Robertson pupil)S S –– sensoriumsensorium (illusions, delusions)(illusions, delusions)I I –– intellect (memory, calculation, intellect (memory, calculation,
orientation, orientation, judgementjudgement, insight), insight)S S –– Speech (Speech (dysarthricdysarthric))

MRI:MRI:
frontocorticalfrontocortical atrophy, frontal highatrophy, frontal high--signal signal lesions, cerebral atrophy lesions, cerebral atrophy mesiotemporalmesiotemporal T2 T2 hyperintensityhyperintensityventriculomegalyventriculomegalypathological T2 pathological T2 hypointensityhypointensity of Basal of Basal ganglia & thalamusganglia & thalamusdiffuse white matter T2 diffuse white matter T2 hyperintensityhyperintensity

TabesTabes dorsalisdorsalisDisease of the posterior columns of the spinal Disease of the posterior columns of the spinal
cord and the dorsal roots.cord and the dorsal roots.
Longest latent period average 20 yrs.Longest latent period average 20 yrs.
CSF : normal/mild CSF : normal/mild lymphocyticlymphocytic pleocytosispleocytosis with with 10 to 50 cells/10 to 50 cells/µµL and protein concentrations of L and protein concentrations of 0.45 to 0.75 .1/4 cases VDRL non reactive. 0.45 to 0.75 .1/4 cases VDRL non reactive.

Triad of SymptomsTriad of Symptoms-- LancinatingLancinating pains pains -- Bladder incontinence / sexual dysfunctionBladder incontinence / sexual dysfunction-- AtaxiaAtaxiaTriad of SignsTriad of Signs-- Argyll Robertson pupilArgyll Robertson pupil-- Loss of reflexesLoss of reflexes-- Loss of Loss of proprioceptionproprioception, vibration sense, vibration sense

DiagnosisDiagnosisDarkfieldDarkfield microscopy (3x),DFAmicroscopy (3x),DFA--TPTP
SerologicalSerologicalNonNon--specific specific –– titrestitres reflect disease activityreflect disease activityRPR/RPR/VDRL(positiveVDRL(positive titrestitres>1:32)>1:32)
Specific Specific –– confirm nonconfirm non--specific testsspecific testsFTFT--ABs,MHAABs,MHA
CSFCSF--VDRL,FTA ABVDRL,FTA AB

TreatmentTreatment
AimAim toto prevent progression of diseaseprevent progression of disease
GummatousGummatousBenzathineBenzathine penicillin 2.4 MU once wkly x 3penicillin 2.4 MU once wkly x 3Alternatives: Alternatives: Doxycycline,CeftriaxoneDoxycycline,Ceftriaxone
CardiovascularCardiovascularBenzathineBenzathine PenicillinPenicillinAlternatives:CeftriaxoneAlternatives:Ceftriaxone

Treatment contTreatment cont……
NeurosyphilisNeurosyphilisIV Penicillin G 10IV Penicillin G 10--14 days14 daysAlternatives(notAlternatives(not recommended) recommended)
-- Procaine penicillin plus Procaine penicillin plus ProbenecidProbenecid-- AmoxycillinAmoxycillin plus plus probenecidprobenecid-- DoxycyclineDoxycycline
Same regimen for ocular/auditorySame regimen for ocular/auditory

FollowupFollowup ……
Serum VDRL at 3 and 6 Serum VDRL at 3 and 6 months,thereaftermonths,thereafter6 monthly for 2 years6 monthly for 2 yearsDrop in Drop in titrestitres fourfold serum VDRLfourfold serum VDRLCSF 6monthly until cell count CSF 6monthly until cell count normalisesnormalisesAll sexual contacts should be treatedAll sexual contacts should be treated

ReferencesReferences
Harrison 16Harrison 16thth editeditUp to dateUp to date