surgical margins in the treatment of nonmelanoma skin cancer and mohs micrographic surgery
TRANSCRIPT
O
SNM
J
DG
Tigapbasggtst©
Ksn
I
Smnmncpa6aswe
CHj
5
RIGINAL REPORTS
urgical Margins in the Treatment ofonmelanoma Skin Cancer and Mohsicrographic Surgery
oshua E. Lane, MD, and David E. Kent, MD
ivision of Dermatology, Department of Internal Medicine, Mercer University School of Medicine, Macon,
eorgiamfi
tmmatp
N
BtsaAcrSmrcnwutsemApAcwc
raditional surgical treatment of nonmelanoma skin cancerncludes excision with subsequent evaluation of surgical mar-ins, either via frozen sections intraoperatively or after excisionnd closure. Accurate communication between surgeon andathologist regarding the meaning of surgical margins shoulde confirmed. Recurrences of tumor growth may in part bettributed to asymmetrical tumor growth patterns with exten-ion of tumor in an unanticipated direction. Mohs micro-raphic surgery is an outpatient procedure that maximizes sur-ical margin evaluation while minimizing the amount of tissuehat must be excised. This article will discuss the concept ofurgical margins in excisions of nonmelanoma skin cancer andhe role of Mohs micrographic surgery. (Curr Surg 62:518-526.
2005 by the Association of Program Directors in Surgery.)
EY WORDS: : Mohs micrographic surgery, surgical margins,urgical excision, nonmelanoma skin cancer, basal cell carci-oma, squamous cell carcinoma
NTRODUCTION
kin cancer (melanoma and nonmelanoma) is the most com-on type of cancer.1 Nonmelanoma skin cancer is composed of
umerous types of malignant skin tumors; however, approxi-ately 95% consist of basal cell and squamous cell carci-
oma.2,3 Other less common types of nonmelanoma skinancer include Merkel cell carcinoma, dermatofibrosarcomarotuberans, atypical fibroxanthoma, angiosarcoma, and otherdnexal/glandular carcinomas.2 Previous reports estimated over00,000 new cases of nonmelanoma skin cancers are diagnosednd treated annually in the United States alone.1 More recenttudies report numbers approaching 1.3 million cases annually,hich reflect the increasing prevalence.4 The annual Medicare
xpenditure for nonmelanoma skin cancer is estimated at $562
orrespondence: Inquiries to Joshua E. Lane, MD, Dermatologic Surgery Specialists, 330
vospital Drive, Building C, Suite 208, Macon, GA 31217; fax: (478) 745-2623; e-mail:
CURRENT SURGERY • © 2005 by the Association of Program DirPublished by Elsevier Inc.
18
illion or 4.5% of all cancer expenditures, which makes this thefth most costly cancer.5,6
Although advances in molecular genetics have localized mu-ations for numerous nonmelanoma skin cancers, the cause re-ains both multifactorial and complex.7 In addition, environ-ental (ultraviolet radiation) and lifestyle factors, as well as an
ging population, certainly play a key part.3,7 Mutations inumor suppressor genes and oncogenes have been identified tolay a role in some nonmelanoma skin cancers.
ONMELANOMA SKIN CANCER
asal cell and squamous cell carcinoma are the most commonypes of cancer.2 These two types of skin cancer can both causeignificant local destruction. Basal cell carcinoma is rarely met-static, with a reported incidence of 0.0028% to 0.55%.8-10
lthough variable, the risk of metastasis for squamous cell car-inoma is greater and estimated to approximate 5%, with aange of 0.5% to 6%, and some reports ranging up to 16%.11-13
quamous cell carcinoma of the lip carries a greater risk ofetastasis, with rates of 15% reported.14 Although mortality
ates are low for both, they are significantly higher for squamousell carcinoma than for basal cell carcinoma.15 The incidence ofonmelanoma skin cancer varies based on geographic location,ith the highest rate of 1% to 2% per year in regions of highltraviolet exposure, such as Australia.16 Basal cell carcinomasend to develop on the head and neck and other sun-exposedites. Squamous cell carcinomas also tend to develop in sun-xposed sites—both basal cell and squamous cell carcinomasay, however, also develop on non-sun-exposed sites as well.lthough skin cancer is certainly more common in Caucasianersons and those with lighter complexions, it may also occur infrican-Americans.17-19 The most common locations for basalell carcinoma are sun-exposed areas of the head and neck,hereas squamous cell carcinoma are more common on nonfa-
ial sites.Squamous cell carcinoma bears a strong association with ad-
anced age (�40 years) and ultraviolet exposure. Squamous cell
ectors in Surgery 0149-7944/05/$30.00doi:10.1016/j.cursur.2005.01.003
cttildaborcIstmar
scndpaba2drvsscmcssTs
lmccagmtmttu
cs
iiaodiclsrs
S
Tmctigmt
mat1trgtivtscc
C
arcinoma is categorized as in situ or invasive, representing fullhickness epidermal invasion versus dermal invasion, respec-ively. Although dermal invasion from in situ lesions may occurn the absence of treatment, this is uncommon. The anatomicocation influences tumor aggressiveness. The mucosal varianteserves special attention because of its high propensity to recurnd metastasize.14 Squamous cell carcinoma of the ear alsoears special mention as it represents one of the most commonrigins for metastasis and is the anatomic site with the highestate of recurrence (18.7%).20 Mortality from squamous cellarcinoma is frequently secondary to metastases from the ear.15
n addition to the morbidity and mortality associated withquamous cell carcinoma of the ear, squamous cell carcinoma ofhe lip carries the highest rate of metastasis (13.7%).21 Squa-ous cell carcinoma originating in a scar or sites of prior radi-
tion therapy also represent an aggressive tumor subtype andequire special attention.
Attention should be given to the histologic classification ofquamous cell carcinoma. Histologic grading of squamous cellarcinoma informs the surgeon of potential tumor aggressive-ess. Classic histologic grading is based on the degree of cellularifferentiation as represented by keratinization, which includesoorly differentiated, undifferentiated, moderately differenti-ted, and well differentiated.22 The degree of differentiation haseen correlated with tumor aggressiveness, as poorly differenti-ted squamous cell carcinoma has a reported recurrence rate of8.6% and a metastatic rate of 32.8%, whereas that for well-ifferentiated squamous cell carcinoma is 13.6% and 9.2%,espectively.21 More recent classification schemes also includeariants such as spindle cell, acantholytic, desmoplastic, adeno-quamous, and cystic squamous cell carcinoma. Spindle cellquamous cell carcinoma must be distinguished from spindleell melanoma and atypical fibroxanthoma, as their manage-ent and metastatic potential differs. Standard immunohisto-
hemical stains help to determine the correct diagnosis. Baso-quamous carcinoma describes a nonmelanoma skin cancerharing features of both squamous cell and basal cell carcinoma.umor thickness has also been shown to correlate with meta-
tatic rates.Basal cell carcinoma is a slow-growing tumor that is corre-
ated with ultraviolet exposure. It is also categorized into nu-erous histologic subtypes, including superficial, nodular, mi-
ronodular, and morpheaform.23 As with squamous cellarcinoma, subtyping allows prediction of tumor aggressivenessnd may dictate surgical technique. Those that comprise ag-ressive growth patterns include micronodular, infiltrative, andorpheaform (sclerosing) basal cell carcinoma, which is impor-
ant as it informs the surgeon of potential growth patterns. Asentioned, basosquamous carcinoma is characterized by fea-
ures of both basal cell and squamous cell carcinoma. Theseumors are more aggressive and have metastatic rates reportedp to 7.4%.24
Perineural involvement of both basal cell and squamous cellarcinoma confers greater aggressiveness with the potential for
pread to variable distances from the clinically apparent tumorFm
URRENT SURGERY • Volume 62/Number 5 • September/October 200
n an unpredictable manner.25-27 The incidence of perineuralnvasion in basal cell carcinoma has been reported to be as highs 6.7% and up to 15% for cutaneous squamous cell carcinomaf the face.27,28 This high rate translates into a larger surgicalefect than tumors without perineural invasion.27 When excis-
ng tumors with perineural invasion, the surgeon must obtain alear margin without perineural tumor or inflammation, as theatter may indicate persistent tumor. Also, the clear marginshould show normal sectioned nerve. Adjuvant postoperativeadiation should be strongly considered to treat potential per-istent perineural involvement and prevent recurrence.
URGICAL MARGINS
he concept of surgical margins is central in the surgical treat-ent of cutaneous neoplasms. Confusion regarding this con-
ept results in a lack of consistency in the histologic interpreta-ion of surgical margins.29-32 This problem stresses themportance of communication between surgeon and patholo-ist.29-32 Multiple methods exist for grossing histologic speci-ens; it is therefore important for the surgeon to be aware of
hese methods and their implications.The term “margin” must be explicitly defined as it can haveultiple meanings. A clinical margin refers to the clinically
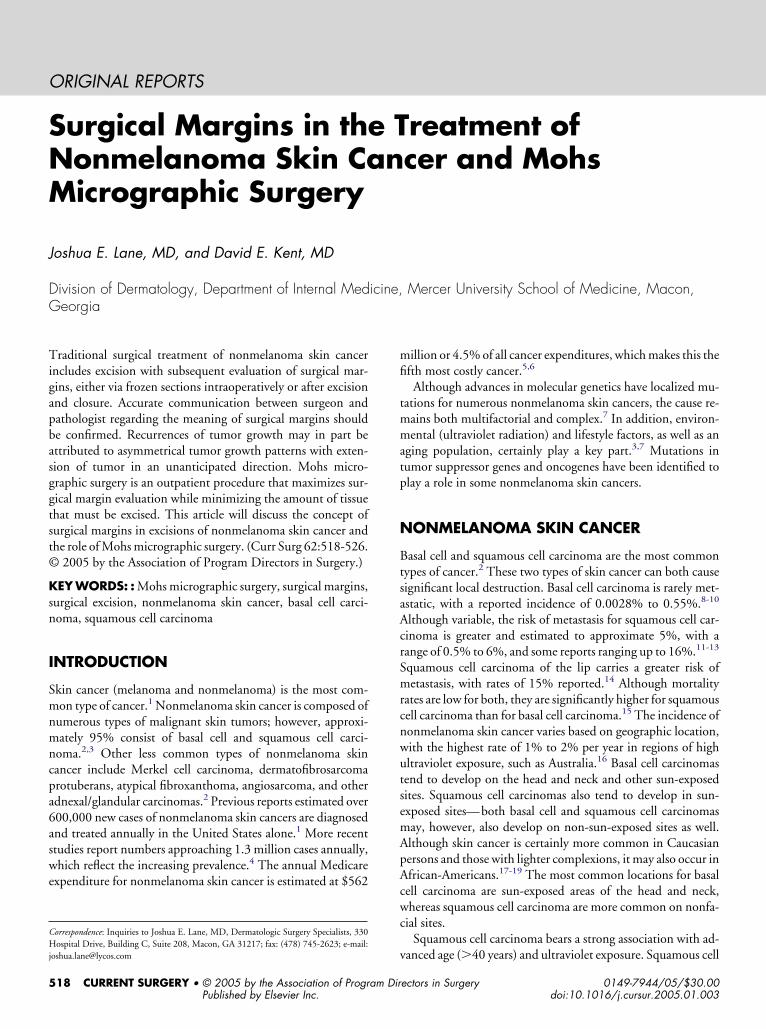
pparent edge of a lesion, whereas a surgical margin is defined ashe specific measurement of tissue surrounding a lesion (Fig.).31 Bennett31 addressed the ambiguity of the term “close tohe margin.” Although this term is common, it is relative andequires mutual understanding between pathologist and sur-eon. Abide et al30 surveyed a group of pathologists regardingheir definition of “close” in standard pathology reports. Vary-ng definitions of “close” surgical margins included tumor in-olvement within a few cells to 0.1 to 5 mm adjacent to theumor edge.30 Interpretation of “close” surgical margins re-ulted in reexcision for squamous cell carcinoma but not basalell carcinoma and reexcision for both squamous cell and basalell carcinoma with involvement of the margins.30 Thus, the
IGURE 1. Fusiform excision shows clinical (tumor edge) and surgicalargins (circle around tumor).
5 519
srs
ovsb2ssaho
alttLst
fT
sbtpspscs
hns
smtmtm
Ft
5
urgeon must be aware of this term and its meaning to accu-ately interpret pathology reports and to determine the neces-ity of subsequent surgical therapy.
Tissue may be examined in the horizontal, vertical, and/orblique planes. Traditional histopathologic grossing involvesertical planes much like the slices in a loaf of bread. Verticalection variants include breadloaf sectioning, cross-sectioning,readloaf/cross-sectioning, and peripheral sectioning (Figs.-5).31 Horizontal and oblique sectioning is seldom used byurgeons except in Mohs micrographic surgery and scalp biop-ies for the evaluation of alopecia (Fig. 6). Although a compar-tive study is beyond the scope of this study, numerous authorsave compared these various histologic sectioning meth-ds.29-32
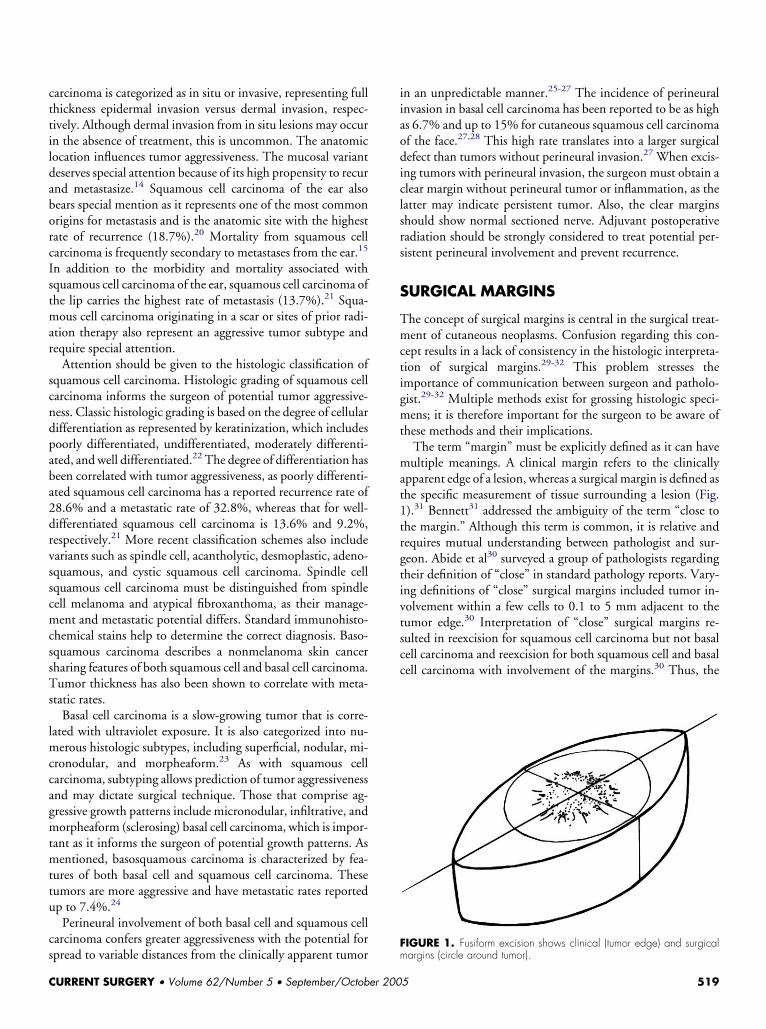
The cross-sectioning method (Fig. 2) samples tissue from 4reas of a tissue specimen. In this method, 1 section is cutengthwise in addition to 2 perpendicular sections. Althoughhis process provides an overall view of the tumor and diagnos-ic capabilities, it leaves most surgical margin unaccounted for.ateral and/or deep tumor invasion may not be noted on theelected sections, which thus potentially provides a false-nega-ive surgical margin.
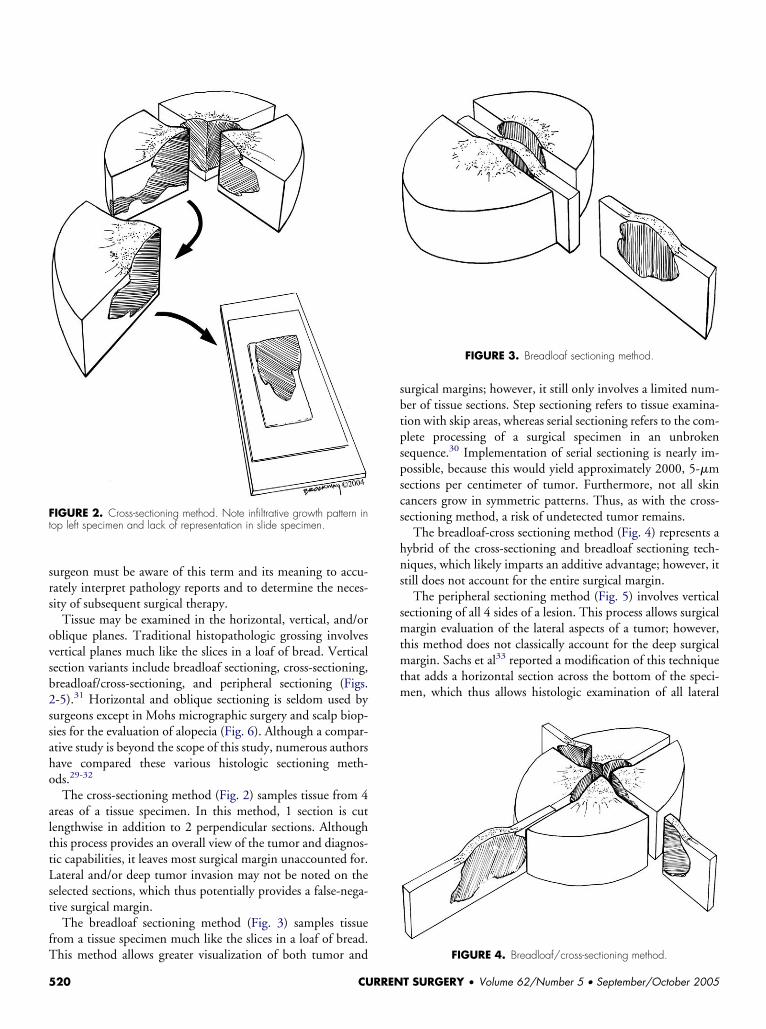
The breadloaf sectioning method (Fig. 3) samples tissuerom a tissue specimen much like the slices in a loaf of bread.
IGURE 2. Cross-sectioning method. Note infiltrative growth pattern inop left specimen and lack of representation in slide specimen.
his method allows greater visualization of both tumor and
20 CURREN
urgical margins; however, it still only involves a limited num-er of tissue sections. Step sectioning refers to tissue examina-ion with skip areas, whereas serial sectioning refers to the com-lete processing of a surgical specimen in an unbrokenequence.30 Implementation of serial sectioning is nearly im-ossible, because this would yield approximately 2000, 5-�mections per centimeter of tumor. Furthermore, not all skinancers grow in symmetric patterns. Thus, as with the cross-ectioning method, a risk of undetected tumor remains.
The breadloaf-cross sectioning method (Fig. 4) represents aybrid of the cross-sectioning and breadloaf sectioning tech-iques, which likely imparts an additive advantage; however, ittill does not account for the entire surgical margin.
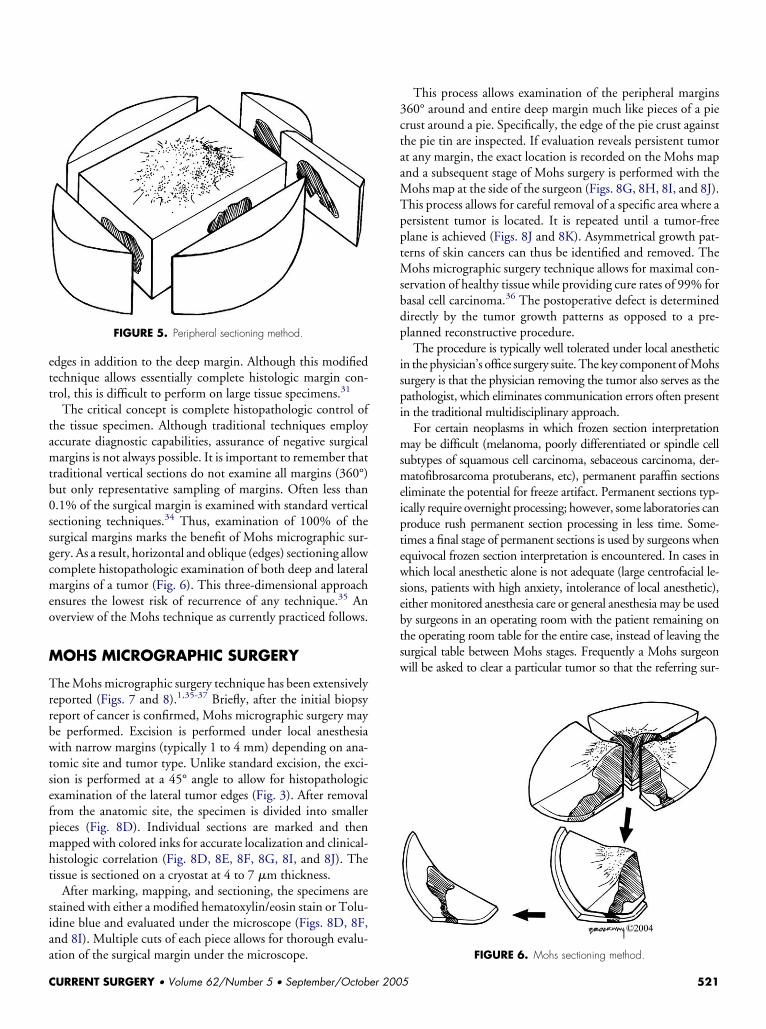
The peripheral sectioning method (Fig. 5) involves verticalectioning of all 4 sides of a lesion. This process allows surgicalargin evaluation of the lateral aspects of a tumor; however,
his method does not classically account for the deep surgicalargin. Sachs et al33 reported a modification of this technique
hat adds a horizontal section across the bottom of the speci-en, which thus allows histologic examination of all lateral
FIGURE 3. Breadloaf sectioning method.
FIGURE 4. Breadloaf/cross-sectioning method.
T SURGERY • Volume 62/Number 5 • September/October 2005
ett
tamtb0ssgcmeo
M
Trrbwtsefpmht
siaa
3ctaaMTpptMsbdp
ispi
msmeiptewsebtsw
C
dges in addition to the deep margin. Although this modifiedechnique allows essentially complete histologic margin con-rol, this is difficult to perform on large tissue specimens.31
The critical concept is complete histopathologic control ofhe tissue specimen. Although traditional techniques employccurate diagnostic capabilities, assurance of negative surgicalargins is not always possible. It is important to remember that
raditional vertical sections do not examine all margins (360°)ut only representative sampling of margins. Often less than.1% of the surgical margin is examined with standard verticalectioning techniques.34 Thus, examination of 100% of theurgical margins marks the benefit of Mohs micrographic sur-ery. As a result, horizontal and oblique (edges) sectioning allowomplete histopathologic examination of both deep and lateralargins of a tumor (Fig. 6). This three-dimensional approach
nsures the lowest risk of recurrence of any technique.35 Anverview of the Mohs technique as currently practiced follows.
OHS MICROGRAPHIC SURGERY
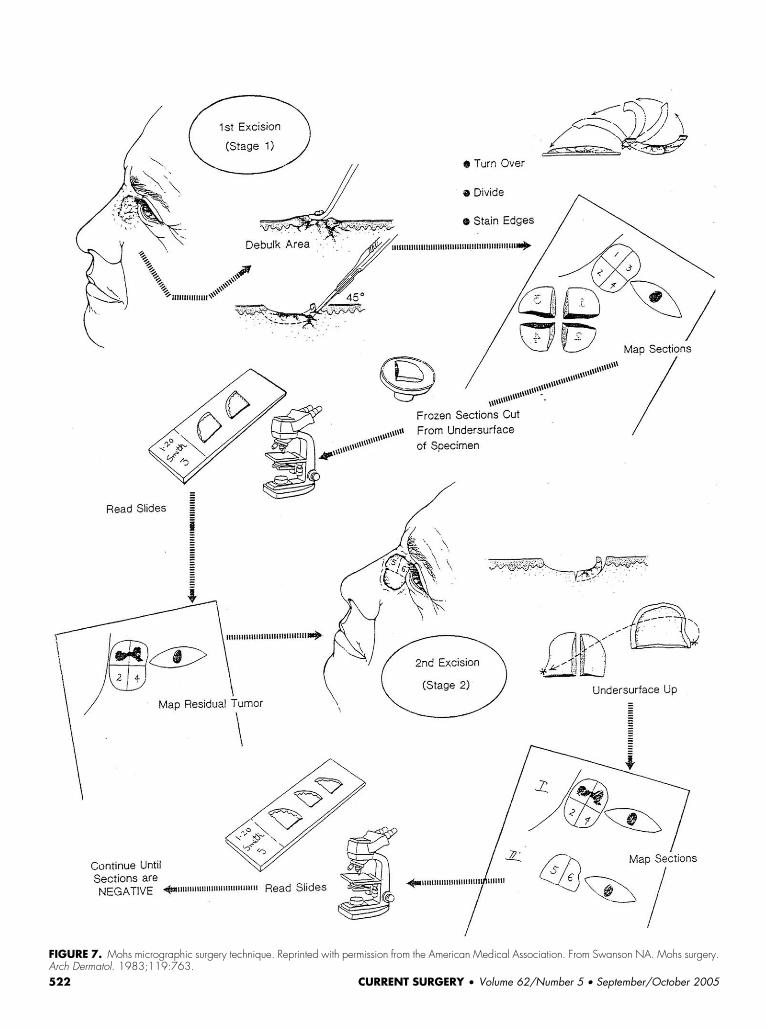
he Mohs micrographic surgery technique has been extensivelyeported (Figs. 7 and 8).1,35-37 Briefly, after the initial biopsyeport of cancer is confirmed, Mohs micrographic surgery maye performed. Excision is performed under local anesthesiaith narrow margins (typically 1 to 4 mm) depending on ana-
omic site and tumor type. Unlike standard excision, the exci-ion is performed at a 45° angle to allow for histopathologicxamination of the lateral tumor edges (Fig. 3). After removalrom the anatomic site, the specimen is divided into smallerieces (Fig. 8D). Individual sections are marked and thenapped with colored inks for accurate localization and clinical-
istologic correlation (Fig. 8D, 8E, 8F, 8G, 8I, and 8J). Theissue is sectioned on a cryostat at 4 to 7 �m thickness.
After marking, mapping, and sectioning, the specimens aretained with either a modified hematoxylin/eosin stain or Tolu-dine blue and evaluated under the microscope (Figs. 8D, 8F,nd 8I). Multiple cuts of each piece allows for thorough evalu-
FIGURE 5. Peripheral sectioning method.
tion of the surgical margin under the microscope.
URRENT SURGERY • Volume 62/Number 5 • September/October 200
This process allows examination of the peripheral margins60° around and entire deep margin much like pieces of a pierust around a pie. Specifically, the edge of the pie crust againsthe pie tin are inspected. If evaluation reveals persistent tumort any margin, the exact location is recorded on the Mohs mapnd a subsequent stage of Mohs surgery is performed with the
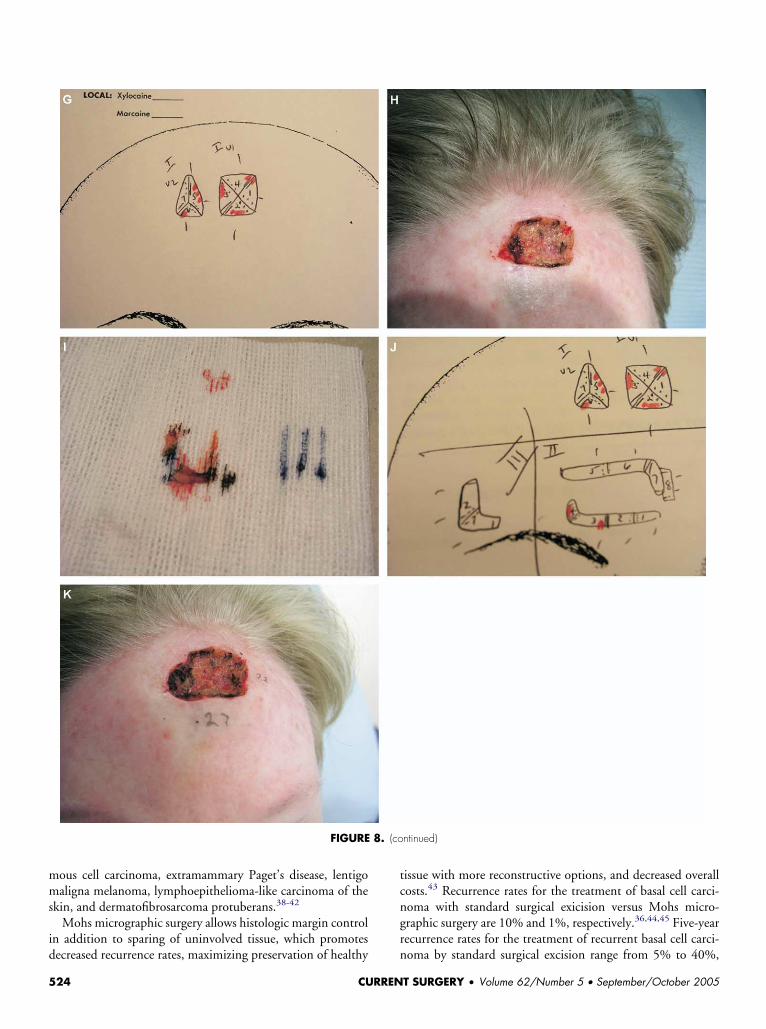
ohs map at the side of the surgeon (Figs. 8G, 8H, 8I, and 8J).his process allows for careful removal of a specific area where aersistent tumor is located. It is repeated until a tumor-freelane is achieved (Figs. 8J and 8K). Asymmetrical growth pat-erns of skin cancers can thus be identified and removed. The
ohs micrographic surgery technique allows for maximal con-ervation of healthy tissue while providing cure rates of 99% forasal cell carcinoma.36 The postoperative defect is determinedirectly by the tumor growth patterns as opposed to a pre-lanned reconstructive procedure.The procedure is typically well tolerated under local anesthetic
n the physician’s office surgery suite. The key component of Mohsurgery is that the physician removing the tumor also serves as theathologist, which eliminates communication errors often presentn the traditional multidisciplinary approach.
For certain neoplasms in which frozen section interpretationay be difficult (melanoma, poorly differentiated or spindle cell
ubtypes of squamous cell carcinoma, sebaceous carcinoma, der-atofibrosarcoma protuberans, etc), permanent paraffin sections
liminate the potential for freeze artifact. Permanent sections typ-cally require overnight processing; however, some laboratories canroduce rush permanent section processing in less time. Some-imes a final stage of permanent sections is used by surgeons whenquivocal frozen section interpretation is encountered. In cases inhich local anesthetic alone is not adequate (large centrofacial le-
ions, patients with high anxiety, intolerance of local anesthetic),ither monitored anesthesia care or general anesthesia may be usedy surgeons in an operating room with the patient remaining onhe operating room table for the entire case, instead of leaving theurgical table between Mohs stages. Frequently a Mohs surgeonill be asked to clear a particular tumor so that the referring sur-
FIGURE 6. Mohs sectioning method.
5 521
FA5
IGURE 7. Mohs micrographic surgery technique. Reprinted with permission from the American Medical Association. From Swanson NA. Mohs surgery.
rch Dermatol. 1983;119:763.22 CURRENT SURGERY • Volume 62/Number 5 • September/October 2005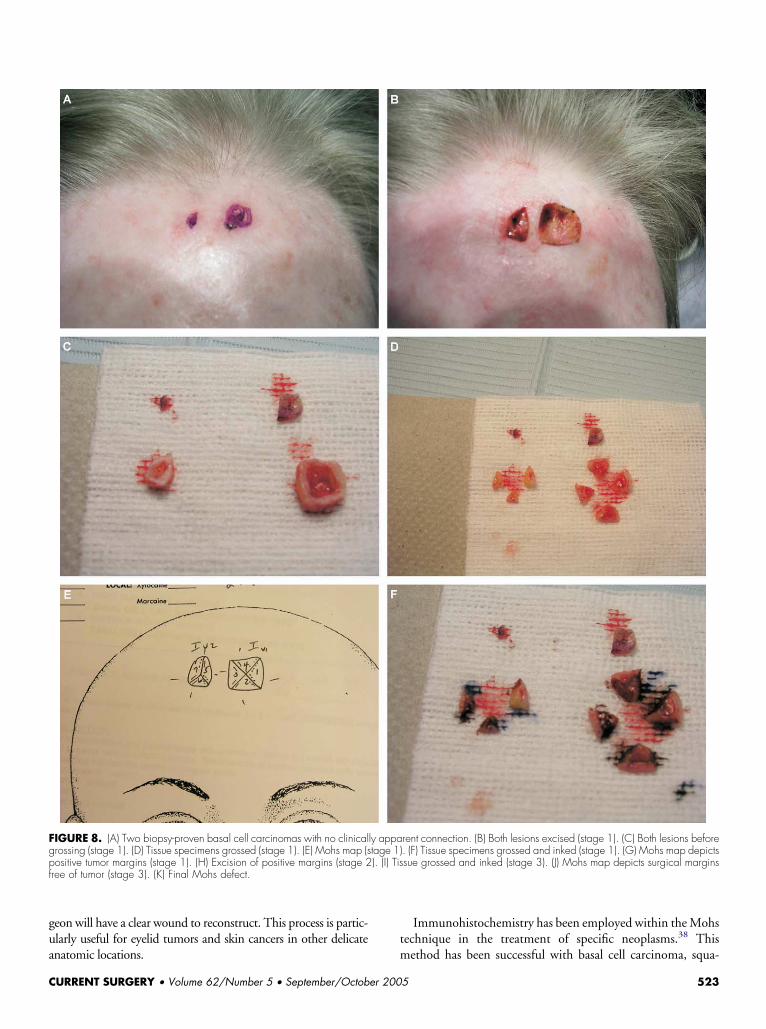
gua
t
Fgp ). (I) Tisf
C
eon will have a clear wound to reconstruct. This process is partic-larly useful for eyelid tumors and skin cancers in other delicate
IGURE 8. (A) Two biopsy-proven basal cell carcinomas with no clinicalrossing (stage 1). (D) Tissue specimens grossed (stage 1). (E) Mohs map (sositive tumor margins (stage 1). (H) Excision of positive margins (stage 2
ree of tumor (stage 3). (K) Final Mohs defect.
natomic locations. m
URRENT SURGERY • Volume 62/Number 5 • September/October 200
Immunohistochemistry has been employed within the Mohsechnique in the treatment of specific neoplasms.38 This
rent connection. (B) Both lesions excised (stage 1). (C) Both lesions before. (F) Tissue specimens grossed and inked (stage 1). (G) Mohs map depictssue grossed and inked (stage 3). (J) Mohs map depicts surgical margins
ly appatage 1)
ethod has been successful with basal cell carcinoma, squa-
5 523
mms
id
tcngr
8. (co
5
ous cell carcinoma, extramammary Paget’s disease, lentigoaligna melanoma, lymphoepithelioma-like carcinoma of the
kin, and dermatofibrosarcoma protuberans.38-42
Mohs micrographic surgery allows histologic margin controln addition to sparing of uninvolved tissue, which promotes
FIGURE
ecreased recurrence rates, maximizing preservation of healthy n
24 CURREN
issue with more reconstructive options, and decreased overallosts.43 Recurrence rates for the treatment of basal cell carci-oma with standard surgical exicision versus Mohs micro-raphic surgery are 10% and 1%, respectively.36,44,45 Five-yearecurrence rates for the treatment of recurrent basal cell carci-
ntinued)
oma by standard surgical excision range from 5% to 40%,
T SURGERY • Volume 62/Number 5 • September/October 2005
wt
mmdTTtbcc
scc
talc
S
Aoaameetn
A
WDVt
R
1
1
1
1
1
1
1
T
C
hereas that after Mohs micrographic surgery ranges from 3%o 8%.36,44,46,47
Mohs micrographic surgery is best suited for cutaneous anducosal neoplasms with a contiguous growth pattern and littleetastatic potential.48 Tumors that are less contiguous and
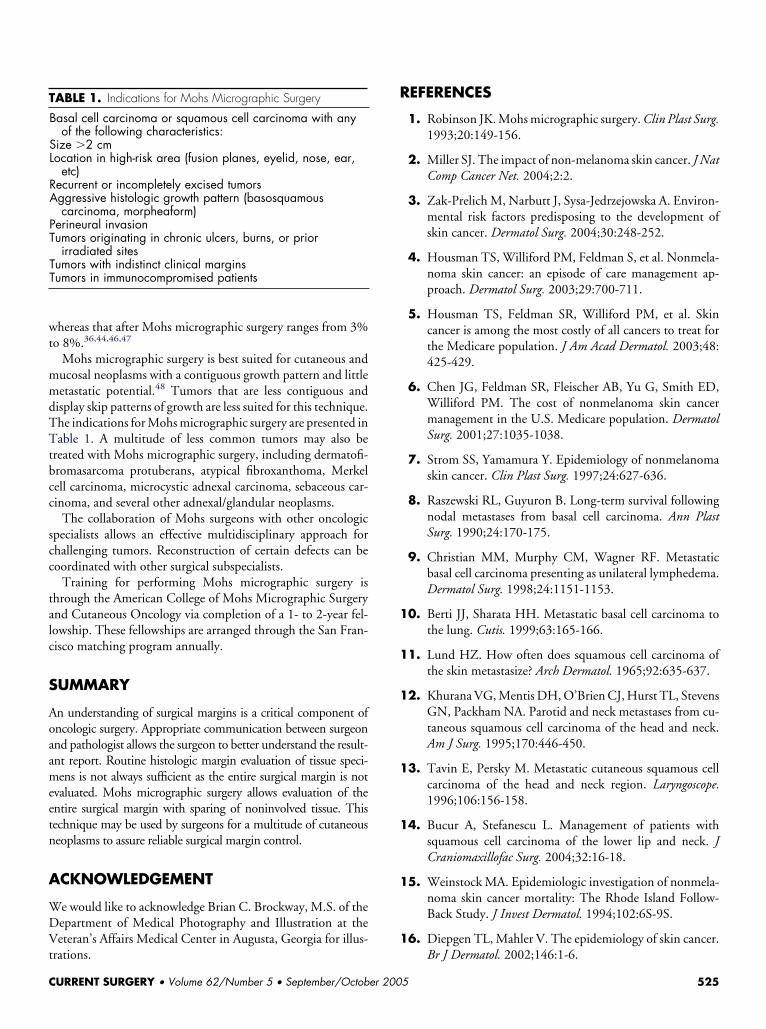
isplay skip patterns of growth are less suited for this technique.he indications for Mohs micrographic surgery are presented inable 1. A multitude of less common tumors may also be
reated with Mohs micrographic surgery, including dermatofi-romasarcoma protuberans, atypical fibroxanthoma, Merkelell carcinoma, microcystic adnexal carcinoma, sebaceous car-inoma, and several other adnexal/glandular neoplasms.
The collaboration of Mohs surgeons with other oncologicpecialists allows an effective multidisciplinary approach forhallenging tumors. Reconstruction of certain defects can beoordinated with other surgical subspecialists.
Training for performing Mohs micrographic surgery ishrough the American College of Mohs Micrographic Surgerynd Cutaneous Oncology via completion of a 1- to 2-year fel-owship. These fellowships are arranged through the San Fran-isco matching program annually.
UMMARY
n understanding of surgical margins is a critical component ofncologic surgery. Appropriate communication between surgeonnd pathologist allows the surgeon to better understand the result-nt report. Routine histologic margin evaluation of tissue speci-ens is not always sufficient as the entire surgical margin is not
valuated. Mohs micrographic surgery allows evaluation of thentire surgical margin with sparing of noninvolved tissue. Thisechnique may be used by surgeons for a multitude of cutaneouseoplasms to assure reliable surgical margin control.
CKNOWLEDGEMENT
e would like to acknowledge Brian C. Brockway, M.S. of theepartment of Medical Photography and Illustration at theeteran’s Affairs Medical Center in Augusta, Georgia for illus-
ABLE 1. Indications for Mohs Micrographic Surgery
Basal cell carcinoma or squamous cell carcinoma with anyof the following characteristics:
Size �2 cmLocation in high-risk area (fusion planes, eyelid, nose, ear,
etc)Recurrent or incompletely excised tumorsAggressive histologic growth pattern (basosquamous
carcinoma, morpheaform)Perineural invasionTumors originating in chronic ulcers, burns, or prior
irradiated sitesTumors with indistinct clinical marginsTumors in immunocompromised patients
rations.
URRENT SURGERY • Volume 62/Number 5 • September/October 200
EFERENCES
1. Robinson JK. Mohs micrographic surgery. Clin Plast Surg.1993;20:149-156.
2. Miller SJ. The impact of non-melanoma skin cancer. J NatComp Cancer Net. 2004;2:2.
3. Zak-Prelich M, Narbutt J, Sysa-Jedrzejowska A. Environ-mental risk factors predisposing to the development ofskin cancer. Dermatol Surg. 2004;30:248-252.
4. Housman TS, Williford PM, Feldman S, et al. Nonmela-noma skin cancer: an episode of care management ap-proach. Dermatol Surg. 2003;29:700-711.
5. Housman TS, Feldman SR, Williford PM, et al. Skincancer is among the most costly of all cancers to treat forthe Medicare population. J Am Acad Dermatol. 2003;48:425-429.
6. Chen JG, Feldman SR, Fleischer AB, Yu G, Smith ED,Williford PM. The cost of nonmelanoma skin cancermanagement in the U.S. Medicare population. DermatolSurg. 2001;27:1035-1038.
7. Strom SS, Yamamura Y. Epidemiology of nonmelanomaskin cancer. Clin Plast Surg. 1997;24:627-636.
8. Raszewski RL, Guyuron B. Long-term survival followingnodal metastases from basal cell carcinoma. Ann PlastSurg. 1990;24:170-175.
9. Christian MM, Murphy CM, Wagner RF. Metastaticbasal cell carcinoma presenting as unilateral lymphedema.Dermatol Surg. 1998;24:1151-1153.
0. Berti JJ, Sharata HH. Metastatic basal cell carcinoma tothe lung. Cutis. 1999;63:165-166.
1. Lund HZ. How often does squamous cell carcinoma ofthe skin metastasize? Arch Dermatol. 1965;92:635-637.
2. Khurana VG, Mentis DH, O’Brien CJ, Hurst TL, StevensGN, Packham NA. Parotid and neck metastases from cu-taneous squamous cell carcinoma of the head and neck.Am J Surg. 1995;170:446-450.
3. Tavin E, Persky M. Metastatic cutaneous squamous cellcarcinoma of the head and neck region. Laryngoscope.1996;106:156-158.
4. Bucur A, Stefanescu L. Management of patients withsquamous cell carcinoma of the lower lip and neck. JCraniomaxillofac Surg. 2004;32:16-18.
5. Weinstock MA. Epidemiologic investigation of nonmela-noma skin cancer mortality: The Rhode Island Follow-Back Study. J Invest Dermatol. 1994;102:6S-9S.
6. Diepgen TL, Mahler V. The epidemiology of skin cancer.
Br J Dermatol. 2002;146:1-6.5 525
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
5
7. Halder RM, Bridgeman-Shah S. Skin cancer in African-Americans. Cancer. 1995;75:667-673.
8. Halder RM, Bang KM. Skin cancer in blacks in theUnited States. Derm Clin. 1988;6:397-405.
9. Mora RG, Perniaciaro C, Lee B. Cancer of the skin inblacks: a review of nineteen black patients with Bowen’sdisease. J Am Acad Dermatol. 1984;11:557-562.
0. Chu A, Osguthorpe JD. Nonmelanoma cutaneous malig-nancy with regional metastasis. Otolaryngol Head NeckSurg. 2003;128:663-673.
1. Rowe DE, Carroll RJ, Day CL Jr. Prognostic factors forlocal recurrence, metastasis, and survival rates in squa-mous cell carcinoma of the skin, ear, and lip. Implicationsfor treatment modality selection. J Am Acad Dermatol.1992;26:976-990.
2. Kwa RE, Campana K, Moy RL. Biology of cutaneoussquamous cell carcinoma. J Am Acad Dermatol. 1992;26:1-26.
3. Preston DS, Stern RS. Nonmelanoma cancers of the skin.N Engl J Med. 1992;327:1649-1662.
4. Bowman PH, Ratz JL, Knoepp TG, Barnes CJ, FinleyEM. Basosquamous carcinoma. Dermatol Surg. 2003;29:830-832.
5. Niazi ZB, Lamberty BJ. Perineural infiltration in basal cellcarcinomas. Br J Plast Surg. 1993;46:156-157.
6. Terashi H, Kurata S, Tadokoro T, et al. Perineural andneural involvement in skin cancers. Dermatol Surg. 1997;23:259-264.
7. Ratner D, Lowe L, Johnson TM, Fader DJ. Perineuralspread of basal cell carcinomas treated with Mohs micro-graphic surgery. Cancer. 2000;88:1605-1613.
8. Goepfert H, Dichtel WJ, Medina JE, Lindberg RD, LunaMD. Perineural invasion in squamous cell carcinoma ofthe head and neck. Am J Surg. 1984;148:542-547.
9. Freeman RG. Handling of pathologic specimens for grossand microscopic examination in dermatologic surgery. JDermatol Surg Oncol. 1982;8:673-679.
0. Abide JM, Nahai F, Bennett RG. The meaning of surgicalmargins. Plast Reconstr Surg. 1984;73:492-496.
1. Bennett RG. The meaning and significance of tissue mar-gins. Adv Dermatol. 1989;4:343-355.
2. Rapini RP. Comparison of methods for checking surgicalmargins. J Am Acad Dermatol. 1990;23:288-294.
3. Sachs W, Sachs PM, Atkinson SC. Peripheral, or five
point, method of skin biopsy. JAMA. 1950;142:902-903.26 CURREN
4. Davidson TM, Nahum AM, Haghighi P, et al. The biopsyof head and neck cancer. Arch Otololaryngol. 1984;11:193.
5. Hruza GJ. Mohs micrographic surgery. Otolaryngol ClinNorth Am. 1990;23:845-864.
6. Swanson NA. Mohs surgery. Arch Dermatol. 1983;119:761-773.
7. Shriner DL, McCoy DK, Goldberg DJ, Wagner RF.Mohs micrographic surgery. J Am Acad Dermatol. 1998;39:79-97.
8. Zalla MK, Lim KK, DiCaudo DJ, Gagnot MM. Mohsmicrographic excision of melanoma using immunostains.Dermatol Surg. 2000;26:771-784.
9. Zachary CB, Rest EB, Furlong SM, Arcedo PN, Mc-George BC, Kist DA. Rapid cytokeratin stains enhancethe sensitivity of Mohs micrographic surgery for squa-mous cell carcinoma. J Dermatol Surg Oncol. 1994;20:530-535.
0. Ramnarain ND, Walker NP, Markey AC. Basal cell car-cinoma: rapid techniques using cytokeratin markers toassist treatment by micrographic (Mohs’) surgery. Br JBiomed Sci. 1995;52:184-187.
1. Jimenez F, Clark FE, Buchanan MD, Kamino H. Lym-phoepithelioma-like carcinoma of the skin treated withMohs micrographic surgery in combination with immunestaining for cytokeratins. J Am Acad Dermatol. 1995;32:878-881.
2. Jimenez FJ, Grichnik JM, Buchanan MD, Clark RE. Im-munohistochemical techniques in Mohs micrographicsurgery: their potential use in the detection of neoplasticcells masked by inflammation. J Am Acad Dermatol. 1995;32:89-94.
3. Cook J, Zitelli JA. Mohs micrographic surgery: a costanalysis. J Am Acad Dermatol. 1998;39:698-703.
4. Robins P. Chemosurgery: my 15 years of experience. JDermatol Surg Oncol. 1981;7:779.
5. Rowe DE, Carroll RJ, Day CL. Long-term recurrencerates in previously untreated (primary) basal cell carci-noma: Implications for patient follow-up. J Dermatol SurgOncol. 1989;15:315.
6. Menn H, Robins P, Kopf AW, et al. The recurrent basalcell epithelioma. Arch Dermatol. 1971;103:628.
7. Rowe DE, Carroll RJ, Day CL. Mohs surgery is the treat-ment of choice for recurrent (previously treated) basal cellcarcinoma. J Dermatol Surg Oncol. 1989;15:424.
8. Lang PG, Osguthorpe JD. Indications and limitations ofMohs micrographic surgery. Dermatol Clin. 1989;7:627-
644.T SURGERY • Volume 62/Number 5 • September/October 2005