subjective adverse reactions to metronidazole in patients with amebiasis
TRANSCRIPT

Parasitology International 63 (2014) 698–700
Contents lists available at ScienceDirect
Parasitology International
j ourna l homepage: www.e lsev ie r .com/ locate /par in t
Short communication
Subjective adverse reactions to metronidazole in patients with amebiasis
Kenji Ohnishi a,⁎, Naoya Sakamoto a, Ken-ichiro Kobayashi a, Sentaro Iwabuchi a,Fukumi Nakamura-Uchiyama a,b, Atsushi Ajisawa c, Yuko Yamauchi d, Nozomi Takeshita d,Yasuyuki Yamamoto e, Takafumi Tsunoda f, Yukihiro Yoshimura g, Natsuo Tachikawa g, Tomoko Uehira h
a Department of Infectious Diseases, Tokyo Metropolitan Bokutoh General Hospital, Tokyo 130-8575, Japanb Department of Pathogen, Infection and Immunity, Nara Medical University, Nara 634-8521, Japanc Department of Infectious Diseases, Tokyo Metropolitan Cancer and Infectious Diseases Center Komagome Hospital, Tokyo 113-8677, Japand Department of Disease Control and Prevention Center, National Center for Global Health and Medicine, Tokyo 162-8655, Japane Department of Laboratory Medicine and Molecular Genetics of Coagulation Disorders, Tokyo Medical University Hospital, Tokyo 162-0023, Tokyo, Japanf Department of Infectious Diseases, Tokyo Health Medical Treatments Corporation Ebara Hospital, Tokyo 145-0065, Japang Department of Infectious Diseases, Yokohama Municipal Citizen's Hospital, Yokohama 240-8555, Japanh Department of Infectious Diseases, National Hospital Organization Osaka National Hospital, Osaka 540-0006, Japan
⁎ Corresponding author at: Department of InfectiousBokutoh General Hospital, 4-23-15 Kohtohbashi, SumidTel.: +81 3 3633 6151; fax: +81 3 3633 6173.
E-mail address: [email protected]
http://dx.doi.org/10.1016/j.parint.2014.05.0061383-5769/© 2014 Elsevier Ireland Ltd. All rights reserved
a b s t r a c t
a r t i c l e i n f oArticle history:Received 2 August 2013Received in revised form 22 May 2014Accepted 26 May 2014Available online 12 June 2014
Keywords:AmebiasisMetronidazoleAdverse reactionNausea
Subjective adverse reactions tometronidazole were analyzed in 111 patients with amebiasis. Metronidazole wasadministered to 36 patients at a daily dose of 2250 mg and 75 patients at daily doses lower than 2250 mg. Thereactions reported included nausea without vomiting in 11 (9.9%) patients, nausea with vomiting in 2 (1.8%),dysgeusia in 2 (1.8%), diarrhea in 1 (0.9%), headache in 1 (0.9%), numbness in 1 (0.9%), dizziness in 1 (0.9%),urticaria in 1 (0.9%), exanthema in 1 (0.9%), and discomfort in 1 (0.9%). Nausea was reported by 28% (10/36)of the patients receiving metronidazole at a daily dose of 2250 mg and 4% (3/75) of the patients receivinglower daily doses. The duration of themetronidazole administration in dayswas not associatedwith the appear-ance of nausea. No life-threatening adverse reactions were identified, and good clinical therapeutic effects wereobserved in 96% (107/111) of the patients. While metronidazole appears to be a safe anti-protozoal agent for pa-tients with amebiasis, our results indicate that a daily metronidazole dose of 2250mg is excessive for amebiasis,as it often induces nausea.
© 2014 Elsevier Ireland Ltd. All rights reserved.
Metronidazole is used widely around the world for the treatment ofamebiasis due to Entamoeba histolytica, with good clinical effects. Thisantiprotozoal agent is now covered for some conditions under Japan'snational health insurance system, but there have been no earlier inves-tigations of adverse reactions to metronidazole in patients with amebi-asis in Japan. We investigated subjective adverse reactions and theclinical therapeutic effect of metronidazole against amebiasis due toE. histolytica in patients treated with metronidazole at several institu-tions throughout Japan between April 1, 2007 and June 30, 2011. Tocollect the data, we sent questionnaires to physicians in charge at thefollowing institutions: Department of Infectious Diseases, TokyoMetro-politan Bokutoh General Hospital (Tokyo); Department of InfectiousDiseases, Tokyo Metropolitan Cancer and Infectious Diseases CenterKomagome Hospital (Tokyo); Department of Disease Control and Pre-vention Center, National Center for Global Health and Medicine
Diseases, Tokyo Metropolitana City, Tokyo 130-8575, Japan.
(K. Ohnishi).
.
(Tokyo); Department of Laboratory Medicine and Molecular Geneticsof Coagulation Disorders, Tokyo Medical University Hospital (Tokyo);Department of Infectious Diseases, Tokyo Health Medical TreatmentsCorporation Ebara Hospital (Tokyo); Department of Infectious Diseases,Yokohama Municipal Citizen's Hospital (Yokohama); and Departmentof Infectious Diseases, National Hospital Organization Osaka NationalHospital (Osaka). We were unable to collect adequate laboratory datain this study, as no uniform method or interval was applied to theblood tests performed at the different institutions.
Amebic colitis was diagnosed when the trophozoites of E. histolyticawere identified in stool or biopsied specimens of colonmucosa, orwhenelevated serum antibodies against E. histolytica were detected in pa-tientswith diarrhea. Amebic liver abscesswas diagnosedwhen elevatedserumantibodies against E. histolyticawere detected or E. histolyticawasfound in the aspirated liver abscess fluid of patients with CT- or ultra-sound-confirmed liver abscesses. All undesirable symptoms foundfrom the start of the metronidazole administration to 1 week after theend of the metronidazole administration were regarded as adverse re-actions to the metronidazole unless the physicians in charge expresslydeemed them to be unrelated to the agent. The treatmentwas regardedto be of good clinical efficacy when symptoms and physical signs
699K. Ohnishi et al. / Parasitology International 63 (2014) 698–700
deemed by the physicians to be causally linked to amebiasis disap-peared in the course of metronidazole administration.
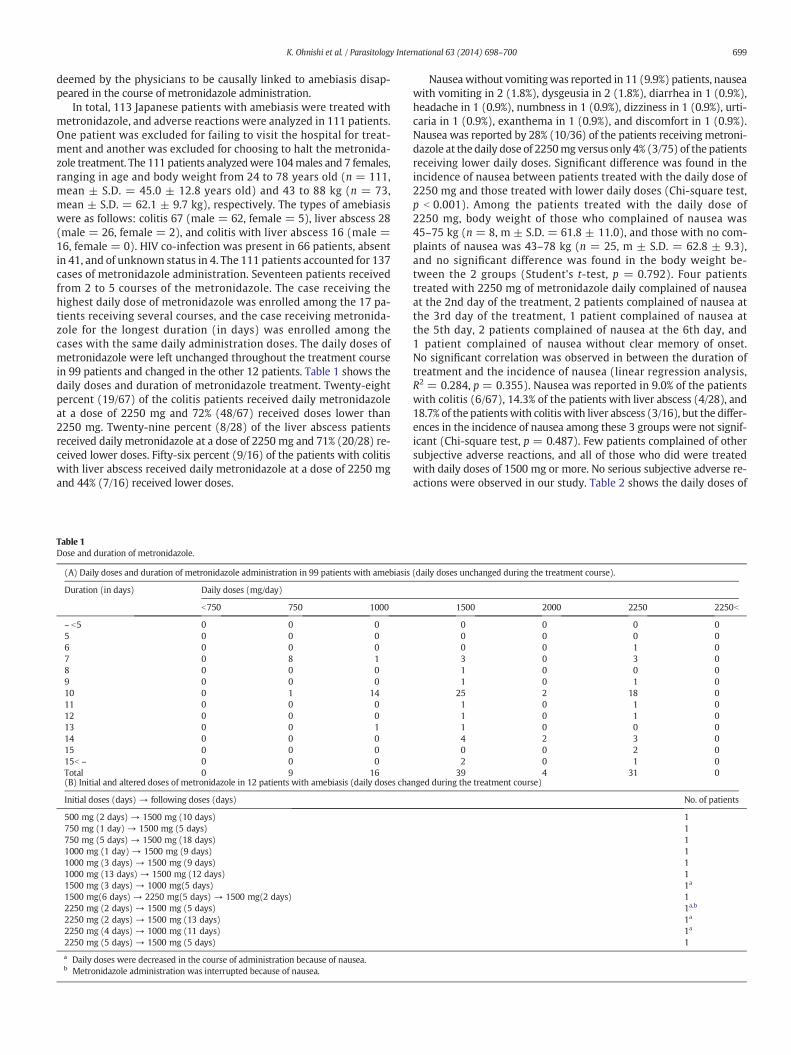
In total, 113 Japanese patients with amebiasis were treated withmetronidazole, and adverse reactions were analyzed in 111 patients.One patient was excluded for failing to visit the hospital for treat-ment and another was excluded for choosing to halt the metronida-zole treatment. The 111 patients analyzedwere 104males and 7 females,ranging in age and body weight from 24 to 78 years old (n = 111,mean ± S.D. = 45.0 ± 12.8 years old) and 43 to 88 kg (n = 73,mean ± S.D. = 62.1 ± 9.7 kg), respectively. The types of amebiasiswere as follows: colitis 67 (male = 62, female = 5), liver abscess 28(male = 26, female = 2), and colitis with liver abscess 16 (male =16, female = 0). HIV co-infection was present in 66 patients, absentin 41, and of unknown status in 4. The 111 patients accounted for 137cases of metronidazole administration. Seventeen patients receivedfrom 2 to 5 courses of the metronidazole. The case receiving thehighest daily dose of metronidazole was enrolled among the 17 pa-tients receiving several courses, and the case receiving metronida-zole for the longest duration (in days) was enrolled among thecases with the same daily administration doses. The daily doses ofmetronidazole were left unchanged throughout the treatment coursein 99 patients and changed in the other 12 patients. Table 1 shows thedaily doses and duration of metronidazole treatment. Twenty-eightpercent (19/67) of the colitis patients received daily metronidazoleat a dose of 2250 mg and 72% (48/67) received doses lower than2250 mg. Twenty-nine percent (8/28) of the liver abscess patientsreceived daily metronidazole at a dose of 2250 mg and 71% (20/28) re-ceived lower doses. Fifty-six percent (9/16) of the patients with colitiswith liver abscess received daily metronidazole at a dose of 2250 mgand 44% (7/16) received lower doses.
Table 1Dose and duration of metronidazole.
(A) Daily doses and duration of metronidazole administration in 99 patients with amebiasis
Duration (in days) Daily doses (mg/day)
b750 750 1000
~ b5 0 0 05 0 0 06 0 0 07 0 8 18 0 0 09 0 0 010 0 1 1411 0 0 012 0 0 013 0 0 114 0 0 015 0 0 015b ~ 0 0 0Total 0 9 16(B) Initial and altered doses of metronidazole in 12 patients with amebiasis (daily doses cha
Initial doses (days) → following doses (days)
500 mg (2 days) → 1500 mg (10 days)750 mg (1 day) → 1500 mg (5 days)750 mg (5 days) → 1500 mg (18 days)1000 mg (1 day) → 1500 mg (9 days)1000 mg (3 days) → 1500 mg (9 days)1000 mg (13 days) → 1500 mg (12 days)1500 mg (3 days) → 1000 mg(5 days)1500 mg(6 days) → 2250 mg(5 days) → 1500 mg(2 days)2250 mg (2 days) → 1500 mg (5 days)2250 mg (2 days) → 1500 mg (13 days)2250 mg (4 days) → 1000 mg (11 days)2250 mg (5 days) → 1500 mg (5 days)
a Daily doses were decreased in the course of administration because of nausea.b Metronidazole administration was interrupted because of nausea.
Nausea without vomitingwas reported in 11 (9.9%) patients, nauseawith vomiting in 2 (1.8%), dysgeusia in 2 (1.8%), diarrhea in 1 (0.9%),headache in 1 (0.9%), numbness in 1 (0.9%), dizziness in 1 (0.9%), urti-caria in 1 (0.9%), exanthema in 1 (0.9%), and discomfort in 1 (0.9%).Nausea was reported by 28% (10/36) of the patients receiving metroni-dazole at the daily dose of 2250mg versus only 4% (3/75) of the patientsreceiving lower daily doses. Significant difference was found in theincidence of nausea between patients treated with the daily dose of2250 mg and those treated with lower daily doses (Chi-square test,p b 0.001). Among the patients treated with the daily dose of2250 mg, body weight of those who complained of nausea was45–75 kg (n = 8, m ± S.D. = 61.8 ± 11.0), and those with no com-plaints of nausea was 43–78 kg (n = 25, m ± S.D. = 62.8 ± 9.3),and no significant difference was found in the body weight be-tween the 2 groups (Student's t-test, p = 0.792). Four patientstreated with 2250 mg of metronidazole daily complained of nauseaat the 2nd day of the treatment, 2 patients complained of nausea atthe 3rd day of the treatment, 1 patient complained of nausea atthe 5th day, 2 patients complained of nausea at the 6th day, and1 patient complained of nausea without clear memory of onset.No significant correlation was observed in between the duration oftreatment and the incidence of nausea (linear regression analysis,R2 = 0.284, p = 0.355). Nausea was reported in 9.0% of the patientswith colitis (6/67), 14.3% of the patients with liver abscess (4/28), and18.7% of the patientswith colitis with liver abscess (3/16), but the differ-ences in the incidence of nausea among these 3 groups were not signif-icant (Chi-square test, p = 0.487). Few patients complained of othersubjective adverse reactions, and all of those who did were treatedwith daily doses of 1500 mg or more. No serious subjective adverse re-actions were observed in our study. Table 2 shows the daily doses of
(daily doses unchanged during the treatment course).
1500 2000 2250 2250b
0 0 0 00 0 0 00 0 1 03 0 3 01 0 0 01 0 1 0
25 2 18 01 0 1 01 0 1 01 0 0 04 2 3 00 0 2 02 0 1 0
39 4 31 0nged during the treatment course)
No. of patients
1111111a
11a,b
1a
1a
1
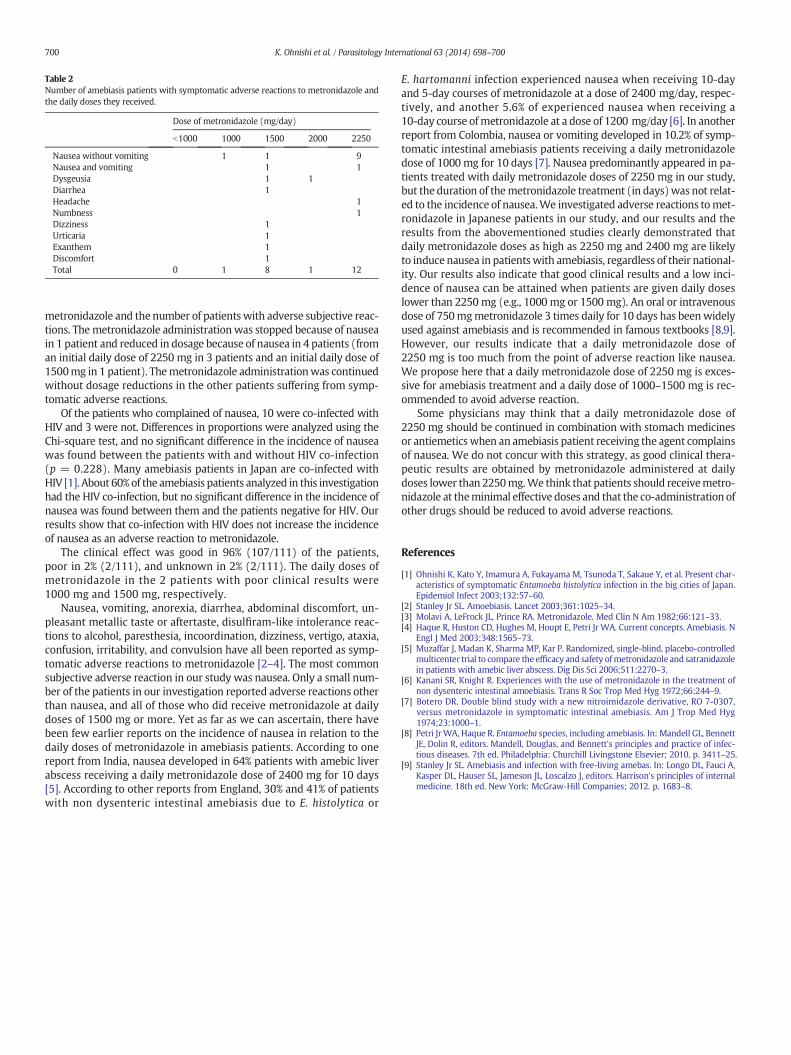
Table 2Number of amebiasis patients with symptomatic adverse reactions to metronidazole andthe daily doses they received.
Dose of metronidazole (mg/day)
b1000 1000 1500 2000 2250
Nausea without vomiting 1 1 9Nausea and vomiting 1 1Dysgeusia 1 1Diarrhea 1Headache 1Numbness 1Dizziness 1Urticaria 1Exanthem 1Discomfort 1Total 0 1 8 1 12
700 K. Ohnishi et al. / Parasitology International 63 (2014) 698–700
metronidazole and the number of patients with adverse subjective reac-tions. Themetronidazole administrationwas stopped because of nauseain 1 patient and reduced in dosage because of nausea in 4 patients (froman initial daily dose of 2250 mg in 3 patients and an initial daily dose of1500mg in 1 patient). Themetronidazole administrationwas continuedwithout dosage reductions in the other patients suffering from symp-tomatic adverse reactions.
Of the patients who complained of nausea, 10 were co-infected withHIV and 3 were not. Differences in proportions were analyzed using theChi-square test, and no significant difference in the incidence of nauseawas found between the patients with and without HIV co-infection(p = 0.228). Many amebiasis patients in Japan are co-infected withHIV [1]. About 60% of the amebiasis patients analyzed in this investigationhad the HIV co-infection, but no significant difference in the incidence ofnausea was found between them and the patients negative for HIV. Ourresults show that co-infection with HIV does not increase the incidenceof nausea as an adverse reaction to metronidazole.
The clinical effect was good in 96% (107/111) of the patients,poor in 2% (2/111), and unknown in 2% (2/111). The daily doses ofmetronidazole in the 2 patients with poor clinical results were1000 mg and 1500 mg, respectively.
Nausea, vomiting, anorexia, diarrhea, abdominal discomfort, un-pleasant metallic taste or aftertaste, disulfiram-like intolerance reac-tions to alcohol, paresthesia, incoordination, dizziness, vertigo, ataxia,confusion, irritability, and convulsion have all been reported as symp-tomatic adverse reactions to metronidazole [2–4]. The most commonsubjective adverse reaction in our study was nausea. Only a small num-ber of the patients in our investigation reported adverse reactions otherthan nausea, and all of those who did receive metronidazole at dailydoses of 1500 mg or more. Yet as far as we can ascertain, there havebeen few earlier reports on the incidence of nausea in relation to thedaily doses of metronidazole in amebiasis patients. According to onereport from India, nausea developed in 64% patients with amebic liverabscess receiving a daily metronidazole dose of 2400 mg for 10 days[5]. According to other reports from England, 30% and 41% of patientswith non dysenteric intestinal amebiasis due to E. histolytica or
E. hartomanni infection experienced nausea when receiving 10-dayand 5-day courses of metronidazole at a dose of 2400 mg/day, respec-tively, and another 5.6% of experienced nausea when receiving a10-day course ofmetronidazole at a dose of 1200 mg/day [6]. In anotherreport from Colombia, nausea or vomiting developed in 10.2% of symp-tomatic intestinal amebiasis patients receiving a daily metronidazoledose of 1000 mg for 10 days [7]. Nausea predominantly appeared in pa-tients treated with daily metronidazole doses of 2250 mg in our study,but the duration of themetronidazole treatment (in days)was not relat-ed to the incidence of nausea.We investigated adverse reactions tomet-ronidazole in Japanese patients in our study, and our results and theresults from the abovementioned studies clearly demonstrated thatdaily metronidazole doses as high as 2250 mg and 2400 mg are likelyto induce nausea in patientswith amebiasis, regardless of their national-ity. Our results also indicate that good clinical results and a low inci-dence of nausea can be attained when patients are given daily doseslower than 2250 mg (e.g., 1000 mg or 1500 mg). An oral or intravenousdose of 750mgmetronidazole 3 times daily for 10 days has beenwidelyused against amebiasis and is recommended in famous textbooks [8,9].However, our results indicate that a daily metronidazole dose of2250 mg is too much from the point of adverse reaction like nausea.We propose here that a daily metronidazole dose of 2250 mg is exces-sive for amebiasis treatment and a daily dose of 1000–1500 mg is rec-ommended to avoid adverse reaction.
Some physicians may think that a daily metronidazole dose of2250 mg should be continued in combination with stomach medicinesor antiemetics when an amebiasis patient receiving the agent complainsof nausea. We do not concur with this strategy, as good clinical thera-peutic results are obtained by metronidazole administered at dailydoses lower than 2250mg.We think that patients should receivemetro-nidazole at theminimal effective doses and that the co-administration ofother drugs should be reduced to avoid adverse reactions.
References
[1] Ohnishi K, Kato Y, Imamura A, Fukayama M, Tsunoda T, Sakaue Y, et al. Present char-acteristics of symptomatic Entamoeba histolytica infection in the big cities of Japan.Epidemiol Infect 2003;132:57–60.
[2] Stanley Jr SL. Amoebiasis. Lancet 2003;361:1025–34.[3] Molavi A, LeFrock JL, Prince RA. Metronidazole. Med Clin N Am 1982;66:121–33.[4] Haque R, Huston CD, Hughes M, Houpt E, Petri Jr WA. Current concepts. Amebiasis. N
Engl J Med 2003;348:1565–73.[5] Muzaffar J, Madan K, Sharma MP, Kar P. Randomized, single-blind, placebo-controlled
multicenter trial to compare the efficacy and safety ofmetronidazole and satranidazolein patients with amebic liver abscess. Dig Dis Sci 2006;511:2270–3.
[6] Kanani SR, Knight R. Experiences with the use of metronidazole in the treatment ofnon dysenteric intestinal amoebiasis. Trans R Soc Trop Med Hyg 1972;66:244–9.
[7] Botero DR. Double blind study with a new nitroimidazole derivative, RO 7-0307,versus metronidazole in symptomatic intestinal amebiasis. Am J Trop Med Hyg1974;23:1000–1.
[8] Petri JrWA, Haque R. Entamoeba species, including amebiasis. In: Mandell GL, BennettJE, Dolin R, editors. Mandell, Douglas, and Bennett's principles and practice of infec-tious diseases. 7th ed. Philadelphia: Churchill Livingstone Elsevier; 2010. p. 3411–25.
[9] Stanley Jr SL. Amebiasis and infection with free-living amebas. In: Longo DL, Fauci A,Kasper DL, Hauser SL, Jameson JL, Loscalzo J, editors. Harrison's principles of internalmedicine. 18th ed. New York: McGraw-Hill Companies; 2012. p. 1683–8.