steffen mitzner 54th asaio conference
TRANSCRIPT

Steffen Mitzner
54 th ASAIO Conference San Francis co
21, 2008June
Univers ity of Ros tockGermany
Albumin Dialys is: MARS
Indications and Clinical Res ults

International MARS Registry

INDICATION n INCLUSION STATUS REMARK
Chirr w HRS 13 AoCLF, HRS Type I
need for RRT
Completed Liver Transpl 2000
AoCLF 24 AoCLF,
Bili > 20mg/dL
Completed Hepatology 2002
ALF 13 HyperALF; HE III/IV Completed Liver Transpl 2003
AoCLF in alcoholic liver disease
16 AoCLF, Bili>15mg/dL,
HE ≥ II°, HRS
Completed Liver Transpl
2004
Hypoxic liver failure post LOF
40 Hypoxic LF,
Bili > 8mg/dL
Completed ASAIO J 2004
Chirr w HE 70 AoCHF, HE III/IV FDA controlled
Completed Hepatology 2007
ALF (FULMAR-trial) 120 ALF (French criteria)
EnrolementCompleted
AoCLF with hyperbili + HE/HRS
(MARS-RELIEF)
230 AoCLF, Bili > 5mg/dL + HE ≥ II° or HRS
Ongoing
- MARS Randomized clinical trials

MARS- Reduction of Albumin bound Toxins
Liver Transplantation, Vol 6, 2000: 603-613
Serum Bilirubin
Start EndHours
umol/l
0 1 2 3 4 5 6 70
100
200
300
400
Serum Bile Acids
Start
0 1 2 3 4 5 6 70
50
100
150
200
umol/l
Hours
P<0,0001 P<0,0001
normal
Serum Bile Acids Serum Bilirubinumol/l
Start Start EndEnd

- Albumin Dialys is MARS Clinical e ffec tsSummary
• ( Cardiovas cular s ys tem SVRI ↑, MAP ↑)
University of Rostock, 2008
• ( QOL pruritus ↓, fatigue ↓)
• ( Liver function PDR ICG ↑, )others
• ( Kidney function Urine output ↑, . Creat ↓)
• (Cerebral function HE↓, ICP↓)
• Organ perfus ion ↑ ( , )brain kidney
• Portal pres s ure ↓

• Liver failure with Hyperdynamic Hypotens ion
Indications for Liver s upport therapy

MARS in Hyperacute ALF
SVRI MAP
Schmidt et al., Liver Transplantation 2003;9:290-297
Hypothermia MARS
-200
0
200
400
600
0 1 2 3 4 5 6 7
Time in hours
SVR
I cha
nge
in d
yn s
/cm
E5/m
E2
p = 0.004
p < 0.0001
-5
0
5
10
15
0 1 2 3 4 5 6 7
Time in hours
MA
P ch
ange
in m
mH
g
p < 0.0001
N.S.
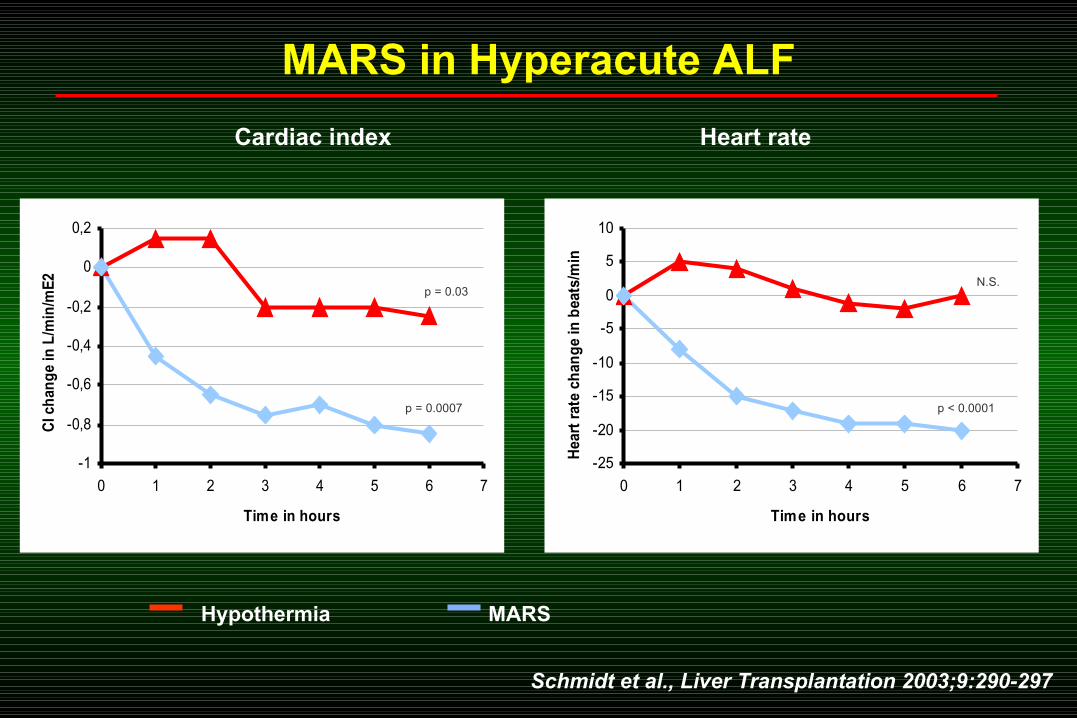
Cardiac index Heart rate
-1
-0,8
-0,6
-0,4
-0,2
0
0,2
0 1 2 3 4 5 6 7
Time in hours
CI c
han
ge
in L
/min
/mE
2
p = 0.0007
p = 0.03
-25
-20
-15
-10
-5
0
5
10
0 1 2 3 4 5 6 7
Time in hours
Hea
rt r
ate
chan
ge
in b
eats
/min
p < 0.0001
N.S.
Schmidt et al., Liver Transplantation 2003;9:290-297
Hypothermia MARS
MARS in Hyperacute ALF

Main Visit Number
MA
P c
han
ge
fro
m b
as
elin
e/ m
mH
g
De
cre
ase
Incre
ase
-40
-30
-20
-10
0
10
20
30
Standard Medical TherapyMARS plus Standard Medical Therapy
85,5+14
77,6+11
Baseline
p=0,04 *p=0,06
(Baseline)
1 2 3 4 5
n.s. p=0,011 * p=0,013 *
p=0,021 *
Time MARS was adminis tred
Heemann U. et al Hepatology 2002; 36: 949-58
MARS in Acute Decompensation of Chronic Liver FailureProspective randomized two- center trial

BEFORE AFTER45
50
55
60
65
70
75
80
85
67.3
76.3
BEFORE AFTER45
50
55
60
65
70
75
80
85
69.3 68.8
BEFORE AFTER45
50
55
60
65
70
75
80
85
71.5
66.2
Liver support: Effect on mean arterial pressure
SMT MARS
PROMETHEUS
P = 0.050 P = 0.014
P = 0.844
. 2006;10: 108Laleman W et al Crit Care R

Liver support: Effect on systemic vascular resistance index
SMT MARS
PROMETHEUS
P = 0.389 P = 0.036
P = 0.120
VOOR NA600
700
800
900
1000
1100
1200
1300
1400
1500
1600
1700
SV
RI (d
yn
es.s
ec.c
m-5
.m2
)
1008 977.5
VOOR NA600
700
800
900
1000
1100
1200
1300
1400
1500
1600
1700
SV
RI
(dyne.s
ec.c
m-5
.m2)
1088
1219
VOOR NA600
700
800
900
1000
1100
1200
1300
1400
1500
1600
1700
SV
RI
(dyne
.sec.c
m-5
.m2)
934.2841.5
. 2006;10: 108Laleman W et al Crit Care R

Liver support: Changes in endogenous vasoactive substances: Effect on nitric oxide
*
*P < 0.001 vs SMT and PROM
-90
-80
-70
-60
-50
-40
-30
-20
-10
0
0 100 200 300 400
P=0.016
Delta SVRI (dyne.s.cm-5.m-2)
Del
ta N
Ox
(nM
)NOx (µM)
-80
-60
-40
-20
0
20
40
De
lta
ch
an
ge 6
SMT
-50.6
MARS
10.9
PROM
. 2006;10: 108Laleman W et al Crit Care R
*

0 5 10 15 20 250
5
10
15
20
25
mm
Hg
Time (hr)
MARS SMT
MARS: Impact on Portal PressureMARS: Impact on Portal Pressure
MARS
. ., . 2005Jalan R et al J Hepato l

• Liver failure with increas ed ( )Intracranial Pres s ure ICP
Indications for Liver s upport therapy


(% c
han
ge f
rom
baseli
ne)
0 1 2 3 4 5 6 750
100
150
200
250
300
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
SHAM
ALF
MARS
ICP
P < 0.05
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
SHAM
ALF
MARS
Time (hours)
ICP
P < 0.05
(% c
han
ge f
rom
baseli
ne)
0 1 2 3 4 5 6 750
100
150
200
250
300
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
SHAM
ALF
MARS
ICP
P < 0.05
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
SHAM
ALF
MARS
Time (hours)
ICP
P < 0.05
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
SHAM
ALF
MARS
ICP
P < 0.05
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
SHAM
ALF
MARS
Time (hours)
ICP
P < 0.05
(% c
han
ge f
rom
baseli
ne)
0 1 2 3 4 5 6 750
100
150
200
250
300
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
SHAM
ALF
MARS
ICP
P < 0.05
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
SHAM
ALF
MARS
Time (hours)
ICP
P < 0.05
(% c
han
ge f
rom
baseli
ne)
0 1 2 3 4 5 6 750
100
150
200
250
300
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
SHAM
ALF
MARS
ICP
P < 0.05
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
SHAM
ALF
MARS
Time (hours)
ICP
P < 0.05
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
SHAM
ALF
MARS
ICP
P < 0.05
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
0 1 2 3 4 5 6 750
100
0 1 2 3 4 5 6 750
100
150
200
250
300
SHAM
ALF
MARS
Time (hours)
ICP
P < 0.05
MARS: Impact on Intracranial PressureMARS: Impact on Intracranial Pressure
Sen S. et al., Crit. Care Med. 2006
Pig model of ALF

• Liver failure with Renal Ins uffic iency Hepatorenal Syndrome
Indications for Liver s upport therapy

: MARS in HRS Type I MAP and Urine volume
0
20
40
60
80
100
120
MAP Urine volume
MA
P (
mm
Hg
)
0
200
400
600
800
1000
1200
uri
ne
vo
lum
e (
ml/d
ay)
MARS pre treatment MARS post treatment HDF pre treatment HDF post treatment
p < 0,05
Mitzner et al. Liver Transplantation 2000; 6: 277-86

SMT group(n=11)
MARS group
(n=12)
P-value
In-hospital deaths 6 1 < 0.05
Worsening of hepatic encephalopathy (° IV) 3 0 < 0.05
Severe hypotension 2 3 NS
Worsening of renal function (HRS) 7 1 < 0.05
Developing electrolyte disorders 10 4 < 0.05
New formation of ascites 1 0 NS
Coagulopathy 3 4 NS
Variceal bleed 1 0 NS
Heemann et al.: Hepatology 2002;36:949-958
: MARS in AoCHF Impact on renal function

• Liver failure with Hepatic Encephalopathy
Indications for Liver s upport therapy

MARS in End Stage Liver Disease and Advanced HE:Prospective, controlled, randomized multi- center trial
Baseline data / Results
- 70 pat. in 8 centers (6 USA and 2 European)
- Age 52.7 ± 10.9, 44% female
MELD 31 ± 10, CTP 12.7 ± 1.3, HE grade III 56%, HE grade IV 44%
- HE-assessment every 12 hours for 5 days (10 per pat.)
-”Responder”: 2-grade-improvement
- primary endpoint: Improvement proportion %
Hassanein T et al. Hepatology 2007; 46: 1853-62
- ITT analysis: SMT (n=31) vs. MARS (n=39) 38 vs. 62% (p=0.04)- PP analysis: SMT (n=29) vs. MARS (n=33) 38 vs. 70% (p=0.007)- MARS group had signif. improvement in serum ammonia, total bilirubin,
bile acids, creatinine, and aromatic acids
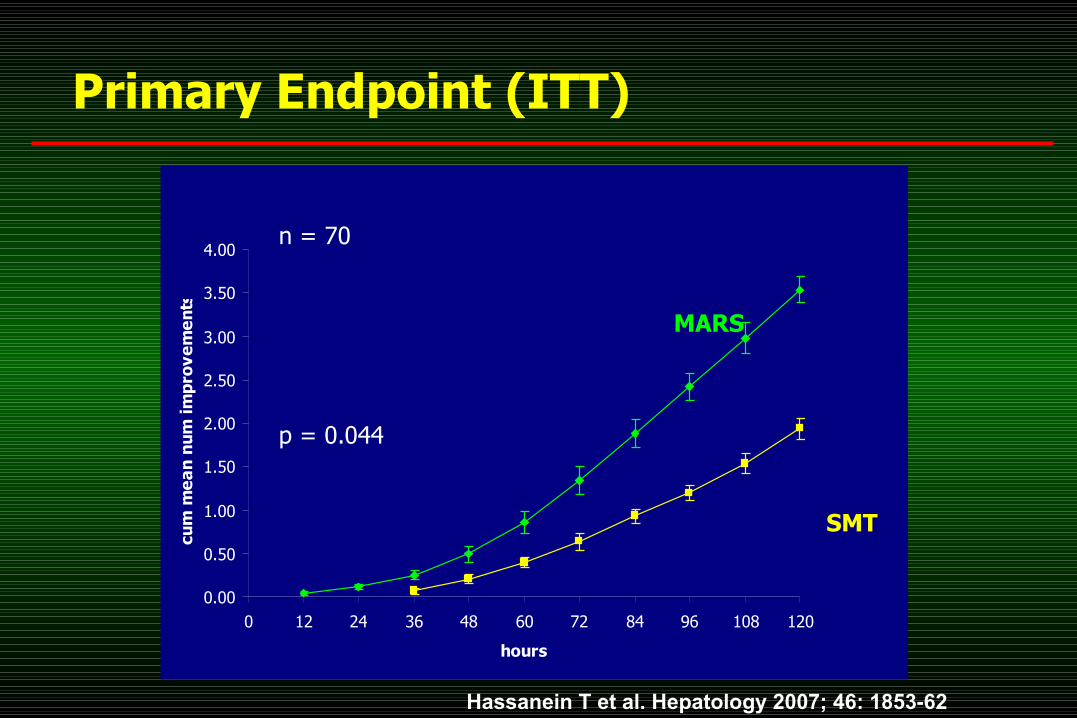
Primary Endpoint (ITT)
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
0 12 24 36 48 60 72 84 96 108 120
hours
cum
me
an
nu
m i
mp
rov
em
en
ts
MARS
SMT
p = 0.044
n = 70
Hassanein T et al. Hepatology 2007; 46: 1853-62

• Supportive Therapy prior to Liver Trans plantation
Indications for Liver s upport therapy

MARS before Liver Trans plantation
Koivusalo AM et al. Transpl Proceed 2005;37:3315-17
56 (29 , 22 , 5 )patients with ALF toxic unknown other . All pats fullfilled TX criteria or had inges ted a le thal dos e of a known
( . . , )toxic agent e g paracetamol Amanita phallo ides 3 ., 22 /Mean number of Rx per pat target duration h s es s ion
6 : 88%, 1 84%month s urvival year s urvival 30 (1 : 79%) Recovery of native function in pats y s urvival
17 (1 : 94%)Succes s ful LTx in pats y s urvival

• Improvement of Survival
Indications for Liver s upport therapy
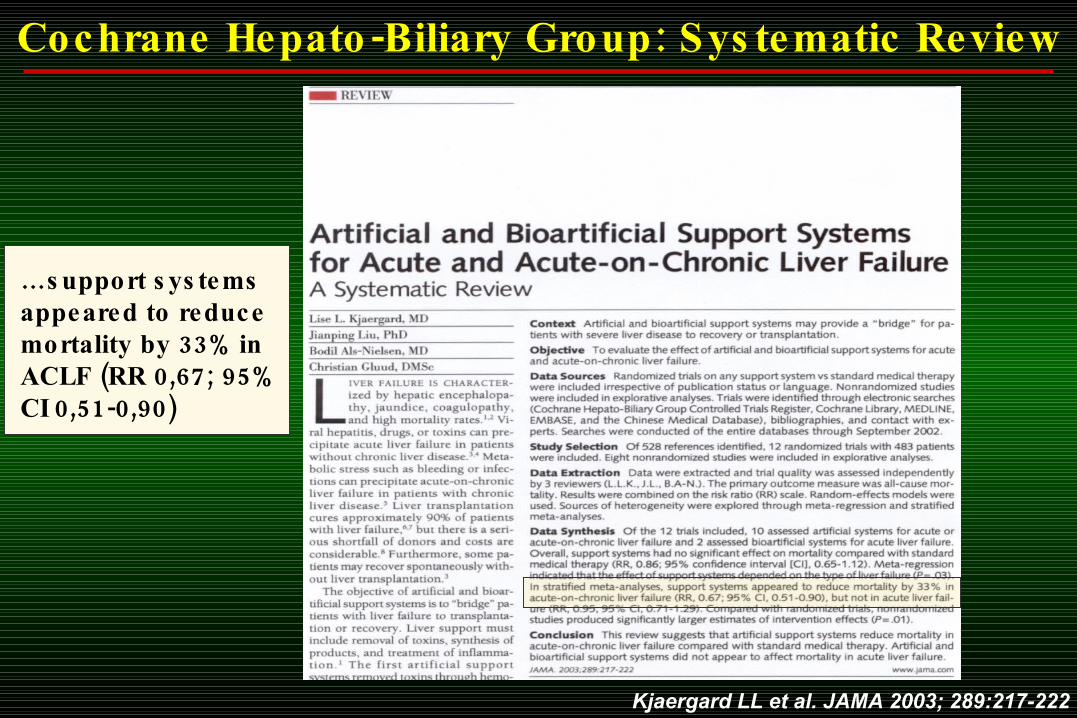
Kjaergard LL et al. JAMA 2003; 289:217-222
- : Cochrane Hepato Biliary Group Sys tematic Review
… s upport s ys tems appeared to reduce 33% mortality by in
( 0,67; 95%ACLF RR 0,51-0,90)CI

0
0,2
0,4
0,6
0,8
1
0 5 10 15 20 25 30
treatment days
cu
mu
lati
ve s
urv
ival
MARS(n=8) HDF(n=5)
p = 0,0123
MARS in Hepatorenal Syndrome
Survivalrates
Mitzner S et al. Liver Transplantation 2000; 6: 277-86

Survival rates
0 5 10 15 20 25 30 350,0
0,2
0,4
0,6
0,8
1,0 MARS (n=12)
Control (n=12)
Survival
Days
<0,05p
Hepatology 2002; 36: 949- 58
MARS in Acute Decompensation of chronic liver failure
Prospective randomized two- center trial

Conclusions
•MARS is in clinical use since 1998. It is the best studied liver support system at present time.
•Indications treated include ACLF, ALF, PNF, postop. LF, HRS, pruritus and others in adults and pediatric cases.
•The system successfully removes albumin-bound as well as water-soluble substances.
•Clinical effects include improvement of hemodynamic, cerebral, kidney, and liver function.
•Increased survival in the MARS-group could be demonstrated in several RCTs.
•Patient selection should be strict. Early onset of treatment ensures best clinical results at reasonable costs.

WELCOME
to the ISAD 2008
September 12-14, 2008Rostock, Germany
www.albumin-dialysis.org