splints and casts- indications and methods
TRANSCRIPT
Splints and Casts: Indications and MethodsANNES.BOYD,MD,University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania
HOLLYJ.BENJAMIN,MD,University of Chicago, Chicago, Illinois
CHADASPLUND,MD,The Ohio State University College of Medicine, Columbus, Ohio
Family physicians often make deci-sions about the use of splints andcastsinthemanagementofmuscu-loskeletaldisorders.Becauseofthis,
they need to be familiar with indicationsfor application, proper technique, and thepotentialpitfallsofcastingandsplintingtooptimize patient care when treating com-monorthopedicinjuries.
Splints and casts immobilize musculo-skeletalinjurieswhilediminishingpainandpromoting healing; however, they differ intheirconstruction,indications,benefits,andrisks. When determining whether to applya splintora cast, thephysicianmustmakean accurate diagnosis, as well as assess thestage,severity,andstabilityoftheinjury;thepatient’s functional requirements; and theriskofcomplications(Table 1).1,2
Because splints are noncircumferentialimmobilizers and are, therefore, more for-giving, they allow for swelling in the acutephase. Splinting is useful for a variety ofacute orthopedic conditions such as frac-tures, reduced joint dislocations, sprains,severesofttissueinjuries,andpost-lacerationrepairs.Thepurposeofsplintingacutelyistoimmobilizeandprotecttheinjuredextrem-ity,aidinhealing,andlessenpain.Splinting
during the later phases of injury or forchronic conditions will assist with healing,long-term pain control, and progression ofphysical function, and itwill slowprogres-sionofthepathologicprocess.3,4
Casting involves circumferential applica-tion of plaster or fiberglass to an extrem-ity. Casts provide superior immobilization,butare less forgivingandhavehighercom-plication rates. Therefore, they are usuallyreserved forcomplexand/ordefinitive frac-turemanagement.
Application of any immobilizer comeswith potential complications, includingischemia, heat injury, pressure sores, skinbreakdown, infection, dermatitis, neuro-logic injury, and compartment syndrome.These conditions can occur regardless ofhow longthedevice isused.5Tomaximizebenefits while minimizing complications,theuseofcastsandsplintsisgenerallylim-ited to the short term. Excessive immobi-lization from continuous use of a cast orsplint can lead to chronic pain, joint stiff-ness, muscle atrophy, or more severe com-plications, such as complex regional painsyndrome.6Allpatientswhoareplacedinasplintorcastrequirecarefulmonitoringtoensureproperrecovery.7
Management of a wide variety of musculoskeletal conditions requires the use of a cast or splint. Splints are noncircum-ferential immobilizers that accommodate swelling. This quality makes splints ideal for the management of a variety of acute musculoskeletal conditions in which swelling is anticipated, such as acute fractures or sprains, or for initial stabilization of reduced, displaced, or unstable fractures before orthopedic intervention. Casts are circumferential immobilizers. Because of this, casts provide superior immobilization but are less forgiving, have higher complication rates, and are generally reserved for complex and/or definitive fracture management. To maximize benefits while minimizing complications, the use of casts and splints is generally limited to the short term. Excessive immobiliza-tion from continuous use of a cast or splint can lead to chronic pain, joint stiffness, muscle atrophy, or more severe complications (e.g., complex regional pain syndrome). All patients who are placed in a splint or cast require careful monitoring to ensure proper recovery. Selection of a specific cast or splint varies based on the area of the body being treated, and on the acuity and stability of the injury. Indications and accurate application techniques vary for each type of splint and cast commonly encountered in a primary care setting. This article highlights the different types of splints and casts that are used in various circumstances and how each is applied. (Am Fam Physician. 2009;80(5):491-499. Copyright © 2009 American Academy of Family Physicians.)
The online version of this article includes supple-
mental content at http:// www.aafp.org/afp.
Downloaded from the American Family Physician Web site at www.aafp.org/afp. Copyright © 2009 American Academy of Family Physicians. For the private, noncommercial use of one individual user of the Web site. All other rights reserved. Contact [email protected] for copyright questions and/or permission requests.
Splints and Casts
492 American Family Physician www.aafp.org/afp Volume 80, Number 5 ◆ September 1, 2009
Cast/Splint Choice and ApplicationThis article highlights the different types of splints andcaststhatareusedinvariouscircumstancesandhoweachisapplied.InapreviousarticleinAmerican Family Physician, wediscussedtheprinciplesandrisksofcastingandsplint-ing,aswellaspropertechniquesforsafeapplication.6
Castingandsplintingbothbeginbyplacingtheinjuredextremityinitspositionoffunction.Castingcontinueswith application of stockinette, then circumferentialapplicationoftwoorthreelayersofcottonpadding,andfinally circumferential application of plaster or fiber-glass.Ingeneral,2-inchpaddingisusedforthehands,2- to 4-inch padding for the upper extremities, 3-inchpadding for the feet, and 4- to 6-inch padding for thelowerextremities.
Splinting may be accomplished in a variety of ways.Oneoptionistobeginasifcreatingacastand,withthe
extremityinitspositionoffunction,applystockinette,thenalayerofoverlappingcircumferentialcottonpad-ding.Thewetsplintisthenplacedoverthepaddingandmoldedtothecontoursoftheextremity,andthestocki-netteandpaddingarefoldedbacktocreateasmoothedge(Figure 1).Thedriedsplintissecuredinplacebywrap-pinganelasticbandageinadistaltoproximaldirection.For an average-size adult, upper extremities should besplintedwithsixto10sheetsofcastingmaterial,whereaslowerextremitiesmayrequire12to15sheets.
Anacceptablealternativeistocreateasplintwithouttheuseofstockinetteorcircumferentialpadding.Sev-erallayersofpaddingthatareslightlywiderandlongerthanthesplintareapplieddirectlytothesmoothed,wetsplint.Together theyaremolded to the extremityandsecuredwithanelasticbandage(Figure 2).Prepackagedsplintsconsistingoffiberglassandpaddingwrappedina
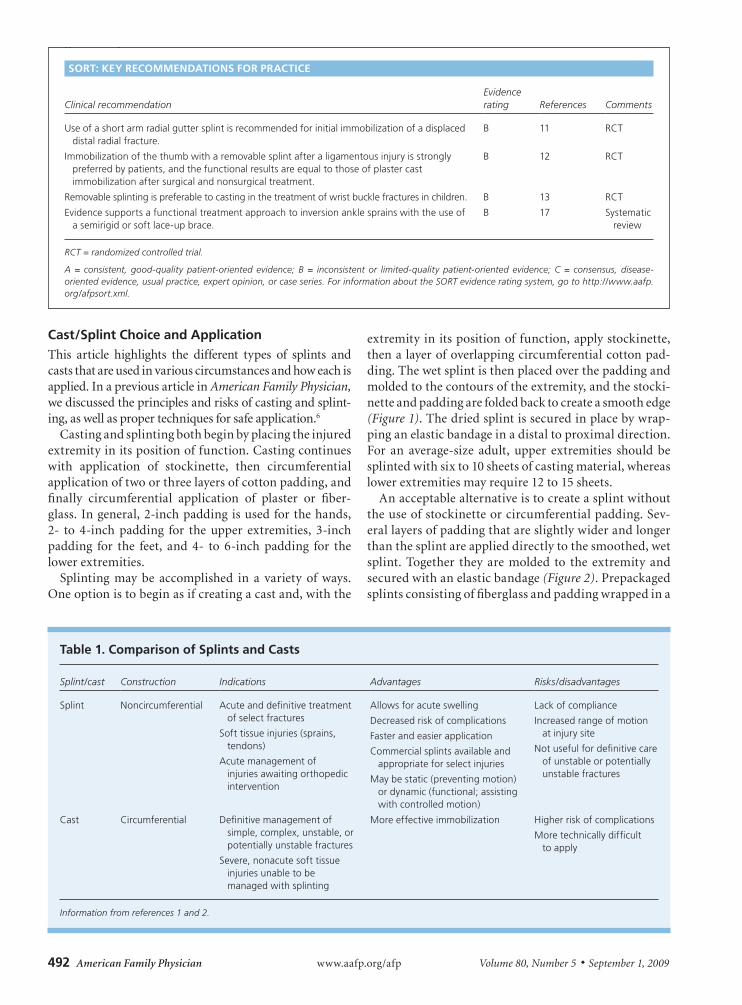
Table 1. Comparison of Splints and Casts
Splint/cast Construction Indications Advantages Risks/disadvantages
Splint Noncircumferential Acute and definitive treatment of select fractures
Soft tissue injuries (sprains, tendons)
Acute management of injuries awaiting orthopedic intervention
Allows for acute swelling
Decreased risk of complications
Faster and easier application
Commercial splints available and appropriate for select injuries
May be static (preventing motion) or dynamic (functional; assisting with controlled motion)
Lack of compliance
Increased range of motion at injury site
Not useful for definitive care of unstable or potentially unstable fractures
Cast Circumferential Definitive management of simple, complex, unstable, or potentially unstable fractures
Severe, nonacute soft tissue injuries unable to be managed with splinting
More effective immobilization Higher risk of complications
More technically difficult to apply
Information from references 1 and 2.
SORT: KEY RECOMMENDATIONS FOR PRACTICE
Clinical recommendationEvidence rating References Comments
Use of a short arm radial gutter splint is recommended for initial immobilization of a displaced distal radial fracture.
B 11 RCT
Immobilization of the thumb with a removable splint after a ligamentous injury is strongly preferred by patients, and the functional results are equal to those of plaster cast immobilization after surgical and nonsurgical treatment.
B 12 RCT
Removable splinting is preferable to casting in the treatment of wrist buckle fractures in children. B 13 RCT
Evidence supports a functional treatment approach to inversion ankle sprains with the use of a semirigid or soft lace-up brace.
B 17 Systematic review
RCT = randomized controlled trial.
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to http://www.aafp.org/afpsort.xml.

Splints and Casts
September 1, 2009 ◆ Volume 80, Number 5 www.aafp.org/afp American Family Physician 493
meshlayeralsoexist.Theseareeasilycutandmoldedtotheinjuredextremity;however,theyaremoreexpensiveand are not always available. Prefabricated and over-the-counter splints are the simplest option, althoughtheyareless“customfit,”andtheirusemaybelimitedbycostoravailability.
The most common types of splints and casts usedin primary care, with information on indications andfollow-up,arediscussedinTables 2 through 4. Allsplintsaredescribedbeforeelasticbandageapplication.
gENERAl FRACTuRE MANAgEMENT PRINCIPlES
Itisimportanttomaintaingoodanatomicfracturealign-ment throughout treatment.Acceptable angulardefor-mityinthehandvariesdependingonthefracturesite.Rotationaldeformityinthehandisneveracceptable.
Stablefracturesaregenerallyreevaluatedwithinonetotwoweeksfollowingcastapplicationtoassesscastfitandcondition,andtoperformradiographytomonitorheal-ingandfracturealignment.Handandforearmfractures,however,areoftenreevaluatedwithinthefirstweek.
Displacedfracturesrequireclosedreduction,followedby post-reduction radiography to confirm bone align-ment.Bothdisplacedandunstablefracturesshould be monitored vigilantly to ensuremaintainedpositioning.Ifreductionorposi-tioningisnotmaintained,urgentreferraltoanorthopedicsubspecialistiswarranted.8-10
upper Extremity Splints and CastsulNAR guTTER SPlINT
Common Uses. Nondisplaced,stablefracturesof thehead,neck,andshaftof the fourthorfifthmetacarpalwithmildangulationandnorotational deformities; nondisplaced, non-rotatedshaftfracturesandserioussofttissueinjuries of the fourth or fifth, proximal ormiddlephalanx;boxer’sfractures(distalfifthmetacarpalfractures,themostcommoninjuryforwhichulnarguttersplint/castused).
Application. Thesplintbeginsattheproxi-malforearmandextendstojustbeyondthedistalinterphalangeal(DIP)joint(Figure 1).Castpaddingisplacedbetweenthefingers.
Position of Function. The wrist is slightly extended,with the metacarpophalangeal (MCP) joints in 70 to90degreesofflexion,andtheproximalinterphalangeal(PIP)andDIPjointsin5to10degreesofflexion.
ulNAR guTTER CAST
Common Uses. Definitive or alternative treatment ofinjuriescommonlytreatedwithulnarguttersplint.8
Application. Ideally,thecastisapplied24to48hoursormoreaftertheinitialinjurytoallowswellingtodecrease.Placementof the castingmaterials is similar to thatoftheulnarguttersplint,excepttheplasterorfiberglassiswrappedcircumferentially(Figure 3).
RADIAl guTTER SPlINT
Common Uses. Nondisplacedfracturesofthehead,neck,and shaft of the second or third metacarpal withoutangulation or rotation; nondisplaced, nonrotated shaftfractures and serious injuries of the second or third,proximal or middle phalanx; initial immobilization ofdisplaceddistalradiusfractures.11
Application. The splint runs along the radial aspectoftheforearmtojustbeyondtheDIPjointoftheindex
Figure 1. Ulnar gutter splint with underlying stockinette and circumferential padding. Figure 2. Padded thumb spica splint.
Table 2. Commonly used Splints and Casts
Area of injury Type of splint Type of cast
Hand/finger Ulnar gutter, radial gutter, thumb spica, finger
Ulnar gutter, radial gutter, thumb spica
Forearm/wrist Volar/dorsal forearm, single sugar-tong
Short arm, long arm
Elbow/forearm Long arm posterior, double sugar-tong
Long arm
Knee Posterior knee, off-the-shelf immobilizer
Long leg
Tibia/fibula Posterior ankle (mid-shaft and distal fractures), bulky Jones
Long leg (proximal fracture), short leg (mid-shaft and distal)
Ankle Posterior ankle (“post-mold”), stirrup, bulky Jones, high-top walking boot
Short leg
Foot
Posterior ankle with or without toe box, hard-soled shoe, high-top walking boot
Short leg, short leg with toe box for phalanx fracture
Splints and Casts
494 American Family Physician www.aafp.org/afp Volume 80, Number 5 ◆ September 1, 2009
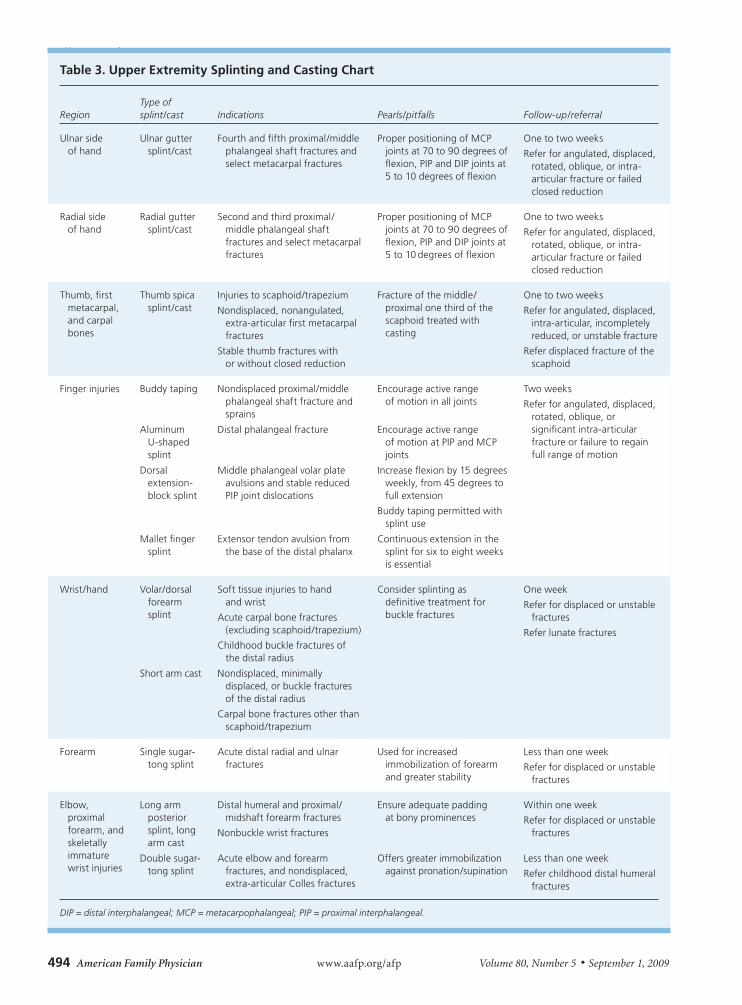
Table 3. upper Extremity Splinting and Casting Chart
RegionType of splint/cast Indications Pearls/pitfalls Follow-up/referral
Ulnar side of hand
Ulnar gutter splint/cast
Fourth and fifth proximal/middle phalangeal shaft fractures and select metacarpal fractures
Proper positioning of MCP joints at 70 to 90 degrees of flexion, PIP and DIP joints at 5 to 10 degrees of flexion
One to two weeks
Refer for angulated, displaced, rotated, oblique, or intra-articular fracture or failed closed reduction
Radial side of hand
Radial gutter splint/cast
Second and third proximal/middle phalangeal shaft fractures and select metacarpal fractures
Proper positioning of MCP joints at 70 to 90 degrees of flexion, PIP and DIP joints at 5 to 10 degrees of flexion
One to two weeks
Refer for angulated, displaced, rotated, oblique, or intra-articular fracture or failed closed reduction
Thumb, first metacarpal, and carpal bones
Thumb spica splint/cast
Injuries to scaphoid/trapezium
Nondisplaced, nonangulated, extra-articular first metacarpal fractures
Stable thumb fractures with or without closed reduction
Fracture of the middle/proximal one third of the scaphoid treated with casting
One to two weeks
Refer for angulated, displaced, intra-articular, incompletely reduced, or unstable fracture
Refer displaced fracture of the scaphoid
Finger injuries Buddy taping Nondisplaced proximal/middle phalangeal shaft fracture and sprains
Encourage active range of motion in all joints
Two weeks
Refer for angulated, displaced, rotated, oblique, or significant intra-articular fracture or failure to regain full range of motion
Aluminum U-shaped splint
Distal phalangeal fracture Encourage active range of motion at PIP and MCP joints
Dorsal extension-block splint
Middle phalangeal volar plate avulsions and stable reduced PIP joint dislocations
Increase flexion by 15 degrees weekly, from 45 degrees to full extension
Buddy taping permitted with splint use
Mallet finger splint
Extensor tendon avulsion from the base of the distal phalanx
Continuous extension in the splint for six to eight weeks is essential
Wrist/hand Volar/dorsal forearm splint
Soft tissue injuries to hand and wrist
Acute carpal bone fractures (excluding scaphoid/trapezium)
Childhood buckle fractures of the distal radius
Consider splinting as definitive treatment for buckle fractures
One week
Refer for displaced or unstable fractures
Refer lunate fractures
Short arm cast Nondisplaced, minimally displaced, or buckle fractures of the distal radius
Carpal bone fractures other than scaphoid/trapezium
Forearm Single sugar-tong splint
Acute distal radial and ulnar fractures
Used for increased immobilization of forearm and greater stability
Less than one week
Refer for displaced or unstable fractures
Elbow, proximal forearm, and skeletally immature wrist injuries
Long arm posterior splint, long arm cast
Distal humeral and proximal/midshaft forearm fractures
Nonbuckle wrist fractures
Ensure adequate padding at bony prominences
Within one week
Refer for displaced or unstable fractures
Double sugar-tong splint
Acute elbow and forearm fractures, and nondisplaced, extra-articular Colles fractures
Offers greater immobilization against pronation/supination
Less than one week
Refer childhood distal humeral fractures
DIP = distal interphalangeal; MCP = metacarpophalangeal; PIP = proximal interphalangeal.

Splints and Casts
September 1, 2009 ◆ Volume 80, Number 5 www.aafp.org/afp American Family Physician 495
finger,leavingthethumbfree(Online Figure A).Castpaddingisplacedbetweenthefingers.
Position of Function. The wrist is placed in slightextension,with theMCPjoints in70 to90degreesofflexion,andthePIPandDIPjoints in5to10degreesofflexion.
RADIAl guTTER CAST
Common Uses. Definitive or alternative treatment offracturesinitiallymanagedwitharadialguttersplint.
Application. Placementofthecastingmaterialsissimi-lartothatoftheradialguttersplint,excepttheplaster
orfiberglassiswrappedcircumferentially(Figure 4).Thecastisusuallyplacedtwotosevendaysaftertheinitialinjurytoallowforresolutionofswelling.
Pearls and Pitfalls. Minimalangulationorrotationatthefracturesitemaycausefunctionalproblems,suchasdifficulty with grasp, pinch, or opposition. Therefore,meticulousevaluationandfollow-upareessential.
ThuMb SPICA SPlINT
Common Uses. Suspectedinjuriestothescaphoid;stableligamentousinjuriestothethumb;initialtreatmentofnonangulated, nondisplaced, extra-articular fractures
Table 4. lower Extremity Splinting and Casting Chart
Region Type of splint/cast Indications Pearls/pitfalls Follow-up/referral
Ankle Posterior ankle splint (“post-mold”)
Severe sprains
Isolated, nondisplaced malleolar fractures
Acute foot fractures
Splint ends 2 inches distal to fibular head to avoid common peroneal nerve compression
Less than one week
Refer for displaced or multiple fractures or significant joint instability
Ankle Stirrup splint Ankle sprains
Isolated, nondisplaced malleolar fractures
Mold to site of injury for effective compression
Less than one week
Lower leg, ankle, and foot
Short leg cast Isolated, nondisplaced malleolar fractures
Foot fractures—tarsals and metatarsals
Compartment syndrome most commonly associated with proximal mid-tibial fractures, so care is taken not to over-compress
Weight-bearing status important; initially non–weight bearing with tibial injuries
Two to four weeks
Refer for displaced or angulated fracture or proximal first through fourth metatarsal fractures
Knee and lower leg
Posterior knee splint
Acute soft tissue and bony injuries of the lower extremity
If ankle immobilization is necessary, as with tibial shaft injuries, the splint should extend to include the metatarsals
Days
Foot
Short leg cast with toe plate extension
Distal metatarsal and phalangeal fractures
Useful technique for toe immobilization
Often used when high-top walking boots are not available
Two weeks
Refer for displaced or unstable fractures
Figure 3. Ulnar gutter cast. Figure 4. Radial gutter cast.

Splints and Casts
496 American Family Physician www.aafp.org/afp Volume 80, Number 5 ◆ September 1, 2009
ofthebaseofthefirstmetacarpal;deQuervaintenosy-novitis;firstcarpometacarpaljointarthritis.
Application. Thesplintcoverstheradialaspectoftheforearm, from the proximal one third of the forearmtojustdistaltotheinterphalangealjointofthethumb,encirclingthethumb(Figure 2).
Position of Function. Theforearmisintheneutralposi-tionwiththewristextendedto25degreesandthethumbinapositionoffunction(i.e.,“holdingasodacan”).
Pearls and Pitfalls. Immobilizationofthethumbwitharemovablesplintafteraligamentousinjuryisstronglypreferredbypatients,andthefunctionalresultsareequaltothoseofplastercastimmobilizationaftersurgicalandnonsurgicaltreatment.12
ThuMb SPICA CAST
Common Uses. Suspected or nondisplaced, distal frac-turesofthescaphoid;nonangulated,nondisplaced,extra-articularfracturesofthebaseofthefirstmetacarpal.
Application. Thecastusesthesamepositionoffunctionasdescribedforathumbspicasplint,butrequirescircum-ferentialapplicationofcastingmaterials(Figure 5).
Pearls and Pitfalls. Becausethesetypesoffracturesareoftenseriousandhaveahighrateofcomplications,long-termsplintingisnotanappropriatedefinitivetreatment.Angulated, displaced, incompletely reduced, or intra-articularfracturesofthefirstmetacarpalbaseshouldbereferred for orthopedic subspecialist evaluation.8 Non-displaceddistalfracturesofthescaphoidhaveagreaterpotentialtohealandmaybeplacedinashortarmthumbspicacastandreevaluatedoutofthecastbyradiographyin two weeks.2,9 Nondisplaced fractures of the middleorproximalonethirdofthescaphoidaretreatedwithalongarmthumbspicacastinitiallyandrequirevigilantmonitoringfornonunion.2
buDDY TAPINg (DYNAMIC SPlINTINg)
Common Uses. Minor finger sprains; stable, nondis-placed,nonangulatedshaftfracturesoftheproximalormiddlephalanx.7,8
Application. Theinjuredfingeristapedtotheadjacentfingerforprotectionandtoallowmovement(Online Figure B).
DORSAl ExTENSION-blOCK SPlINT
Common Uses. Larger,middlephalangealvolaravulsionswithpotentialfordorsalsubluxation;reduced,stablePIPjointdorsaldislocations.
Application. Inreduced,volaravulsion fractures, thesplintisappliedwiththePIPjointat45degreesofflexionand secured at the proximal finger, allowing flexion at
thePIPjoint(Figure 6).Withweeklylateralradiography,the flexion is decreased 15 degrees until reaching fullextensionoverfourweeks.Buddytapingshouldfollow.Treatment of reduced PIP joint dislocations is similar,butrequiresastartingangleof20degrees.
AluMINuM u-ShAPED SPlINT
Common Uses.Distalphalangealfractures.Application. Thealuminumsplintwrapsfromthedor-
salfingertiparoundtothevolarfingertipandimmobilizesonlytheDIPjointinextension(Online Figure C).
MAllET FINgER SPlINTS
Common Uses. Avulsionoftheextensortendonfromthebaseofthedistalphalanx(withorwithoutanavulsionfracture).
Figure 5. Thumb spica cast.
Figure 6. Dorsal extension-block splint.
Splints and Casts
September 1, 2009 ◆ Volume 80, Number 5 www.aafp.org/afp American Family Physician 497
Application. TheDIPjointisplacedinslighthyperex-tensionwithapaddeddorsalsplint,anunpaddedvolarsplint,oraprefabricatedmalletfingersplint.Continuousextensioninthesplintforsixtoeightweeksisessential,evenwhenchangingthesplint.Compliance isassessedeverytwoweeks.Nightsplintingforanadditionaltwotothreeweeksisrecommended.
vOlAR/DORSAl FOREARM SPlINT
Common Uses. Softtissueinjuriesofthehandandwrist;temporary immobilization of carpal bone dislocationsorfractures(excludingscaphoidandtrapezium).
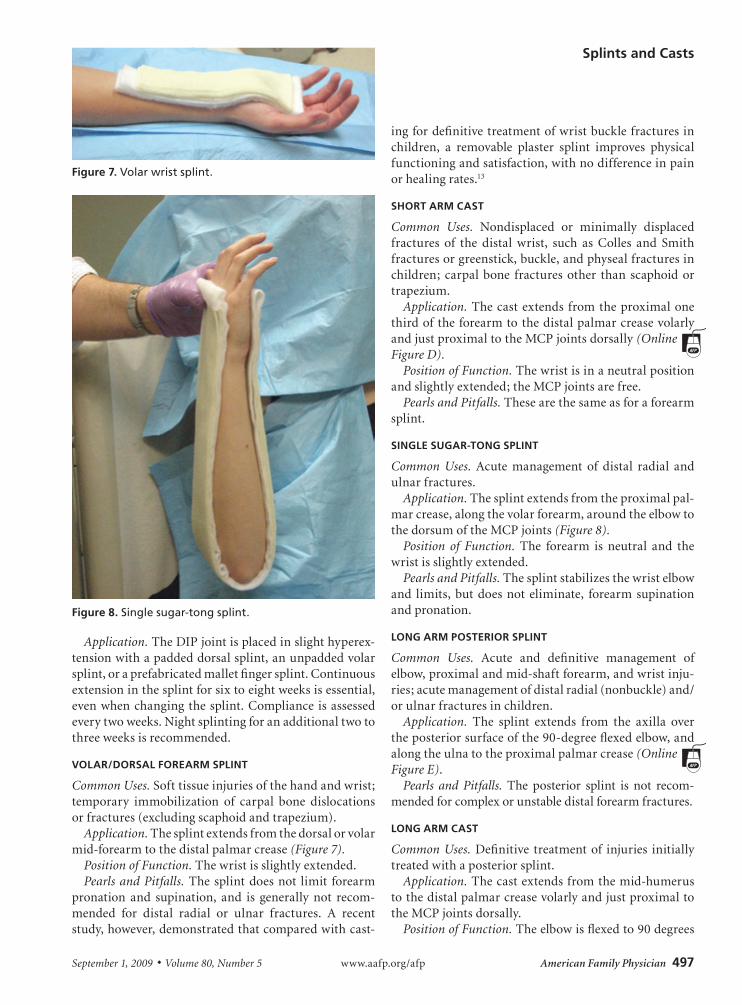
Application. Thesplintextendsfromthedorsalorvolarmid-forearmtothedistalpalmarcrease(Figure 7).
Position of Function. Thewristisslightlyextended.Pearls and Pitfalls. Thesplintdoesnot limit forearm
pronation and supination, and is generally not recom-mended for distal radial or ulnar fractures. A recentstudy,however,demonstratedthatcomparedwithcast-
ingfordefinitivetreatmentofwristbucklefracturesinchildren, a removable plaster splint improves physicalfunctioningandsatisfaction,withnodifferenceinpainorhealingrates.13
ShORT ARM CAST
Common Uses. Nondisplaced or minimally displacedfractures of the distal wrist, such as Colles and Smithfracturesorgreenstick,buckle,andphysealfracturesinchildren; carpalbone fracturesother than scaphoidortrapezium.
Application. ThecastextendsfromtheproximalonethirdoftheforearmtothedistalpalmarcreasevolarlyandjustproximaltotheMCPjointsdorsally(Online Figure D).
Position of Function. Thewristisinaneutralpositionandslightlyextended;theMCPjointsarefree.
Pearls and Pitfalls. Thesearethesameasforaforearmsplint.
SINglE SugAR-TONg SPlINT
Common Uses. Acute management of distal radial andulnarfractures.
Application. Thesplintextendsfromtheproximalpal-marcrease,alongthevolarforearm,aroundtheelbowtothedorsumoftheMCPjoints(Figure 8).
Position of Function. The forearm is neutral and thewristisslightlyextended.
Pearls and Pitfalls. Thesplintstabilizesthewristelbowand limits,butdoesnoteliminate, forearmsupinationandpronation.
lONg ARM POSTERIOR SPlINT
Common Uses. Acute and definitive management ofelbow,proximalandmid-shaftforearm,andwristinju-ries;acutemanagementofdistalradial(nonbuckle)and/orulnarfracturesinchildren.
Application. The splint extends from the axilla overtheposteriorsurfaceofthe90-degreeflexedelbow,andalongtheulnatotheproximalpalmarcrease(Online Figure E).
Pearls and Pitfalls. The posterior splint is not recom-mendedforcomplexorunstabledistalforearmfractures.
lONg ARM CAST
Common Uses. Definitive treatmentof injuries initiallytreatedwithaposteriorsplint.
Application. Thecastextendsfromthemid-humerustothedistalpalmarcreasevolarlyandjustproximaltotheMCPjointsdorsally.
Position of Function. Theelbowisflexedto90degrees
Figure 7. Volar wrist splint.
Figure 8. Single sugar-tong splint.
Splints and Casts
498 American Family Physician www.aafp.org/afp Volume 80, Number 5 ◆ September 1, 2009
withthewristinaneutral,slightlyextendedposition(Online Figure F).
Pearls and Pitfalls. Adequate padding at the olecra-non, ulnar styloid, and antecubital fossa prevents skinbreakdown. Physicians should avoid applying the edgeofthecastingtapeovertheantecubitalfossa,particularlywiththeinitiallayer.Longarmcastsareusedmostoftenin childhood because of the frequency of distal radial,ulnar,anddistalhumeralfractures.2,10,14
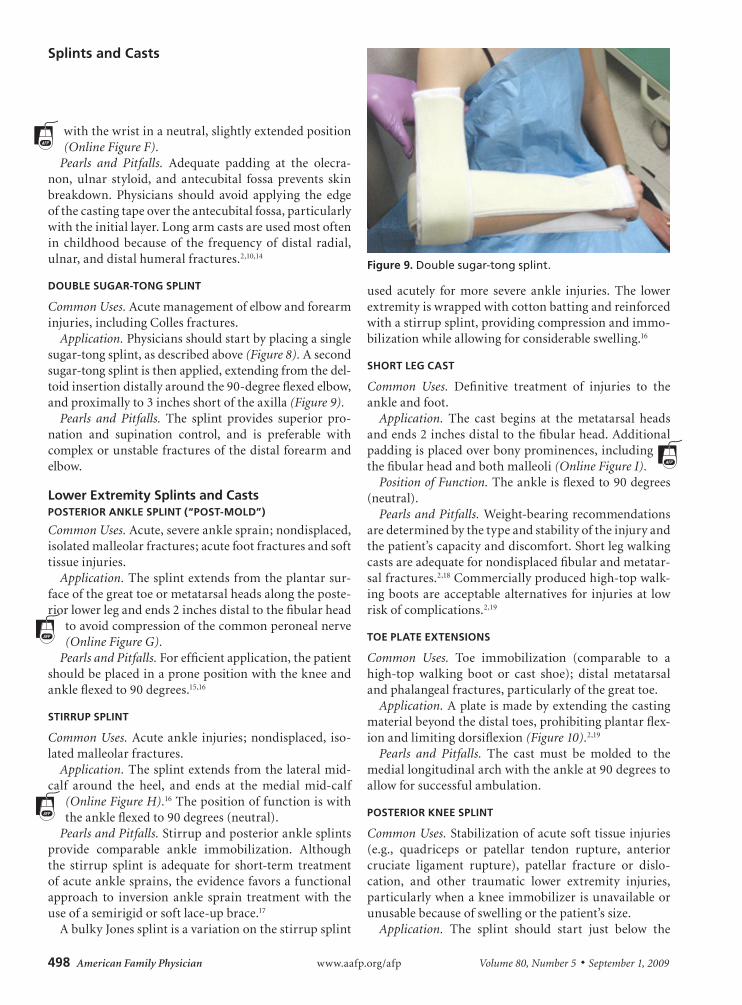
DOublE SugAR-TONg SPlINT
Common Uses. Acutemanagementofelbowandforearminjuries,includingCollesfractures.
Application. Physiciansshouldstartbyplacingasinglesugar-tongsplint,asdescribedabove(Figure 8).Asecondsugar-tongsplintisthenapplied,extendingfromthedel-toidinsertiondistallyaroundthe90-degreeflexedelbow,andproximallyto3inchesshortoftheaxilla(Figure 9).
Pearls and Pitfalls. The splint provides superior pro-nation and supination control, and is preferable withcomplexorunstablefracturesofthedistalforearmandelbow.
lower Extremity Splints and CastsPOSTERIOR ANKlE SPlINT (“POST-MOlD”)
Common Uses. Acute,severeanklesprain;nondisplaced,isolatedmalleolarfractures;acutefootfracturesandsofttissueinjuries.
Application. Thesplintextendsfromtheplantarsur-faceofthegreattoeormetatarsalheadsalongtheposte-riorlowerlegandends2inchesdistaltothefibularhead
toavoidcompressionofthecommonperonealnerve(Online Figure G).
Pearls and Pitfalls. Forefficientapplication,thepatientshouldbeplacedinapronepositionwiththekneeandankleflexedto90degrees.15,16
STIRRuP SPlINT
Common Uses. Acuteankle injuries;nondisplaced, iso-latedmalleolarfractures.
Application. Thesplintextendsfromthelateralmid-calf around the heel, and ends at the medial mid-calf
(Online Figure H).16Thepositionoffunctioniswiththeankleflexedto90degrees(neutral).
Pearls and Pitfalls. Stirrupandposterioranklesplintsprovide comparable ankle immobilization. Althoughthe stirrup splint is adequate for short-term treatmentofacuteanklesprains,theevidencefavorsafunctionalapproach to inversion ankle sprain treatment with theuseofasemirigidorsoftlace-upbrace.17
AbulkyJonessplintisavariationonthestirrupsplint
used acutely for more severe ankle injuries. The lowerextremityiswrappedwithcottonbattingandreinforcedwithastirrupsplint,providingcompressionandimmo-bilizationwhileallowingforconsiderableswelling.16
ShORT lEg CAST
Common Uses. Definitive treatment of injuries to theankleandfoot.
Application. The cast begins at the metatarsal headsandends2inchesdistaltothefibularhead.Additionalpaddingisplacedoverbonyprominences,includingthefibularheadandbothmalleoli(Online Figure I).
Position of Function. Theankleisflexedto90degrees(neutral).
Pearls and Pitfalls. Weight-bearingrecommendationsaredeterminedbythetypeandstabilityoftheinjuryandthepatient’scapacityanddiscomfort.Shortlegwalkingcastsareadequatefornondisplacedfibularandmetatar-salfractures.2,18Commerciallyproducedhigh-topwalk-ingbootsareacceptablealternatives for injuriesat lowriskofcomplications.2,19
TOE PlATE ExTENSIONS
Common Uses. Toe immobilization (comparable to ahigh-top walking boot or cast shoe); distal metatarsalandphalangealfractures,particularlyofthegreattoe.
Application. Aplateismadebyextendingthecastingmaterialbeyondthedistaltoes,prohibitingplantarflex-ionandlimitingdorsiflexion(Figure 10).2,19
Pearls and Pitfalls. The cast must be molded to themediallongitudinalarchwiththeankleat90degreestoallowforsuccessfulambulation.
POSTERIOR KNEE SPlINT
Common Uses. Stabilizationofacutesofttissueinjuries(e.g., quadriceps or patellar tendon rupture, anteriorcruciate ligament rupture), patellar fracture or dislo-cation, and other traumatic lower extremity injuries,particularlywhenakneeimmobilizer isunavailableorunusablebecauseofswellingorthepatient’ssize.
Application. The splint should start just below the
Figure 9. Double sugar-tong splint.

Splints and Casts
September 1, 2009 ◆ Volume 80, Number 5 www.aafp.org/afp American Family Physician 499
glutealcreaseandend justproximal tothemalleoli(Online Figure J).
Position of Function. Theknee ispositioned in slightflexion.
Pearls and Pitfalls. If ankle immobilization is neces-sary,aswithtibialshaftinjuries,thesplintshouldextendtoincludethemetatarsals.
The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the U.S. Army or the U.S. Army Medical Service at large.
The Authors
ANNE S. BOYD, MD, FAAFP, is an assistant professor of family medicine at the University of Pittsburgh (Pa.) School of Medicine, and director of the primary care sports medicine fellowship program at the University of Pittsburgh Medical Center, St. Margaret.
HOLLY J. BENJAMIN, MD, FAAP, FACSM, is an associate professor of pediatrics and orthopedic surgery at the University of Chicago (Ill.), and director of the primary care sports medicine program. She serves on the board of directors for the American Medical Society for Sports Medicine, is part of the executive committee for the American Academy of Pediatrics Council on Sports Medicine and Fitness, and is a fellow of the American College of Sports Medicine.
CHAD ASPLUND, MD, is currently a clinical assistant professor of family medicine at The Ohio State University College of Medicine, Columbus. At the time this article was written, he was a clinical faculty member of the Eisenhower Army Medical Center in Fort Gordon, Ga.
Address correspondence to Anne S. Boyd, MD, FAAFP, Lawrenceville Family Health Center, 3937 Butler St., Pittsburgh, PA 15201. Reprints are not available from the authors.
Author disclosure: Nothing to disclose.
REFERENCES
1. Chudnofsky CR, Byers S. Splinting techniques. In: Roberts JR, Hedges JR, Chanmugam AS, eds. Clinical Procedures in Emergency Medicine. 4th ed. Philadelphia, Pa.: Saunders; 2004:989.
2. Eiff MP, Hatch R, Calmbach WL, eds. Fracture Management for Primary Care. 2nd ed. Philadelphia, Pa.: Saunders; 2003:1-70.
3. Parmelee-Peters K, Eathorne S. The wrist: common injuries and man-agement. Prim Care. 2005;32(1):35-70.
4. Hong E. Hand injuries in sports medicine. Prim Care. 2005;32(1):91-103.
5. General principles. In: Simon RR, Sherman SC, Koenigsknecht SJ, eds. Emergency Orthopedics: The Extremities. 5th ed. New York, NY: McGraw-Hill; 2007:1-29.
6. Boyd AS, Benjamin HJ, Asplund C. Principles of casting and splinting. Am Fam Physician. 2009;79(1):16-22.
7. Benjamin HJ, Mjannes JM, Hang BT. Getting a grasp on hand injuries in young athletes. Contemp Pediatr. 2008;25(3):49-63.
8. Lee SG, Jupiter JB. Phalangeal and metacarpal fractures of the hand. Hand Clin. 2000;16(3):323-332.
9. Slade JF, Magit DP, Geissler WB. Scaphoid fractures in athletes. Atlas Hand Clin. 2006;11(1):27-44.
10. Overly F, Steele DW. Common pediatric fractures and dislocations. Clin Pediatr Emerg Med. 2002;3(2):106.
11. Bong MR, Egol KA, Leibman M, Koval KJ. A comparison of immediate postreduction splinting constructs for controlling initial displacement of fractures of the distal radius: a prospective randomized study of long-arm versus short-arm splinting. J Hand Surg [Am]. 2006;31(5):766-770.
12. Sollerman C, Abrahamsson SO, Lundborg G, Adalbert K. Functional splinting versus plaster cast for ruptures of the ulnar collateral ligament of the thumb. A prospective randomized study of 63 cases. Acta Orthop Scand. 1991;62(6):524-526.
13. Plint AC, Perry JJ, Correll R, Gaboury I, Lawton L. A randomized, con-trolled trial of removable splinting versus casting for wrist buckle frac-tures in children. Pediatrics. 2006;117(3):691-697.
14. Benjamin HJ, Hang BT. Common acute upper extremity injuries in sports. Clin Pediatr Emerg Med. 2007;8(1):15-30.
15. Haller PR, Harris CR. The tibia and fibula. In: Ruiz E, Cicero JJ, eds. Emergency Management of Skeletal Injuries. St Louis, Mo.: Mosby-Year Book; 1995:499-517.
16. Roberts DM, Stallard TC. Emergency department evaluation and treatment of knee and leg injuries. Emerg Med Clin North Am. 2000;18(1):67-84.
17. Kerkhoffs GM, Struijs PA, Marti RK, Assendelft WJ, Blankevoort L, van Dijk CN. Different functional treatment strategies for acute lateral ankle ligament injuries in adults. Cochrane Database Syst Rev. 2002;(3):CD002938.
18. Court-Brown CM. Fractures of the tibia and fibula. In: Rockwood CA, Green DP, Buchholz RW, eds. Rockwood and Green’s Fractures in Adults. 6th ed. Philadelphia, Pa.: Lippincott Williams and Wilkins; 2006:2079-2146.
19. LaBella CR. Common acute sports-related lower extremity injuries in children and adolescents. Clin Pediatr Emerg Med. 2007;8(1):31-42.
Figure 10. Short leg cast with toe plate extension.