spiritual, religious, and existential aspects of palliative care
TRANSCRIPT

392
JOURNAL OF PALLIATIVE MEDICINEVolume 8, Number 2, 2005© Mary Ann Liebert, Inc.
Palliative Care ReviewSpiritual, Religious, and Existential Aspects
of Palliative Care
TOMASZ R. OKON, M.D.
INTRODUCTION
EXISTENTIAL, SPIRITUAL, AND RELIGIOUS concernsare fundamental issues in palliative care.
When faced with suffering and the fragility of life,patients frequently articulate spiritual concerns.It is imperative that health care providers under-stand the characteristic problems, obtain appro-priate histories, and facilitate spiritual support ifneeded.
Regardless of one’s particular spiritual orien-tation, every individual has to make a decision asto whether one’s life has meaning and value thatextends beyond self, life, and death. Even a fo-cused and resolute answer negating such mean-ing places one in relation to the transcendent.1
Therefore, examined or not, one’s relation to whatis transcendent is intrinsic to the human condi-tion, a phenomenon acutely manifest at the endof life.
“Spiritual” is from the Latin spiritus, meaningbreath. It may be understood as nonmaterial ormetaphysical, hence pertaining to sacred thingsor the soul, or more broadly, the intellectual andmoral aspects of life. Some authors define spiri-tuality as that which pertains to “ultimate mean-ing and purpose in life.”2 While less controver-sial, such a broad definition necessarily turns into a tautology. Upon a comprehensive review,McSherry and Cash3 concluded that, “the term‘spirituality’ is problematic and in danger of be-coming meaningless,” and that, “a universal def-inition of spirituality may be theoretically andculturally impossible” (Table 1).
The term “existential” derives from Latin ex-sistere, which means to come into being or to havereal being whether material or spiritual. By theexistential philosophy, we do not experience our-selves as our essences or principles, but as indi-viduals living in the world, always facing ourown fragility and mortality. It is precisely this“passionate anxious freedom toward death”4 thatenables us to construct a sense of purpose, free-dom, and authenticity in life, the fundamental ex-istential attributes.
The term “religion” from Latin religare to re-strain, tie back, or hold together, refers to super-natural constraint, sanction, or religious practice.Religious then means relating to or manifestingfaithful devotion to an acknowledged ultimate re-ality or deity through observances and practice.Narrowly, religion provides a set of core beliefsabout life events and establishes an ethical foun-dation for clinical decision-making.5 Against thatview, postmodern theology considers religiousdevotion to complete and exceed philosophy, establishing the primacy of doxology in place of “metaphysics” and the derivative empiricist“method”6 governing biomedical pursuits.
The distinction between the terms referring tothe human relationship with the transcendent isarbitrary. Indeed, even among the psychologi-cally oriented authors the bifurcation of religionand spirituality has been criticized as heuristi-cally useful,7,8 yet theoretically biased and not reflective of common concerns of persons offaith.9,10 Similarly, a sophisticated genealogicalanalysis demonstrates that an opinion that reli-
Department of Palliative Medicine, Marshfield Clinic, Marshfield, Wisconsin.Series Editors: Bob Arnold, M.D. and Solomon Liao, M.D. Authors are asked to review information at the expert
level for physicians practicing as a subspecialist in palliative medicine. Subsequent updates will focus on the mostup-to-date literature that has been published since the last version.

gious spirituality represents a variant of a uni-versal spirituality is an arbitrary choice with anormative aspiration, rather than a disengageddescriptive observation. Therefore, any particu-lar understanding of the spiritual dimension ofcare11 should be seen as an outcome of contin-gent historical forces, political commitments of aparticular society and its medical practitionersand not scientifically grounded truths.12 Pallia-tive care physicians should remain particularlymindful of their own choices in this regard andstrive to develop their own, critical perspective.
EPIDEMIOLOGY
General Trends
Expressed Religious/Spiritual Attitudes in the Gen-eral Population. At least 9 of 10 Americans believein God or a “higher power” and at least twothirds pray regularly and are members of reli-gious congregations.13 This proportion has re-mained stable over several decades.14 Sixty per-cent of U.S. residents consider religion to be very important in their lives, while even more(82%) recognize a need for a personal spiritualgrowth.13,15 The structure of religious beliefs ishighly heterogeneous, mirroring the social andcultural trends of the contemporary pluralistic so-ciety. For instance, in a recent study respondentswere asked to define themselves on a religiosity-spirituality spectrum. Ten percent of respondentsdescribed themselves as spiritual and not reli-gious. The majority considered themselves both
religious and spiritual, while a quarter describedthemselves as neither religious nor spiritual.16
Expressed Religious/Spiritual Attitudes in Ill Per-sons. The attitudes and behaviors expressed in thecontext of an illness follow the trends present inthe general population. Over one half of elderlyinpatients reported some form of religious prac-tices, attitudes, and coping behaviors, while 40%reported that their religious faith was the mostimportant factor that enabled them to cope withthe illness, and nearly 90% indicated they usedreligion to at least a moderate extent to help themcope.17 A study of patients with advanced gyne-cologic cancer revealed that 85% of the patientsidentified themselves as having some connectionwith organized religion, 76% indicated that reli-gion had a serious place in their lives, 49% feltthat they had become more religious since hav-ing cancer (no one becoming less religious).18
Seventy-six percent of a sample of patients withbreast cancer reported praying as a method ofcoping with the illness, thus making prayer themost common alternative therapy technique uti-lized in this sample.19
Physicians’ Own Reported Attitudes and Beliefs.Faith and religious beliefs influence physicians’attitudes towards fundamental aspects of med-ical decision making at the end of life. Amongfamily physicians, religious and spiritual beliefsand practices reach rates comparable with thegeneral population.20 In an older study of men-tal health specialists, however, only 39% of psy-chiatrists and 33% of clinical psychologists agreed
SPIRITUAL, RELIGIOUS, AND EXISTENTIAL ASPECTS 393
TABLE 1. A TAXONOMY OF SPIRITUALITY
Descriptors Description
Theistic Belief in a supreme being, cosmological arguments not necessarily a “God” but a deity.Religious Affiliation—belief in a God, undertaking certain religious practices, customs and rituals.Language Individuals may use certain language when defining spirituality such as inner strength,
inner peace.Cultural, political An individual may subscribe to a particular political position or social ideology that
social ideologies influences, governs their attitudes and behaviors, dependent upon world faith—religious tenants
Phenomenological One learns about life by living and learning from a variety of situations and experienceboth positive and negative.
Existential A semantic philosophy of life and being, finding meaning, purpose and fulfillment in allof life’s events.
Quality of life Although quality of life is not explicit in definition, it is implicit.Mystical Relationship between the transcendent, interpersonal, transpersonal life after death.
Reprinted with permission from McSherry W, Cash K: The language of spirituality: an emerging taxonomy. Int JNurs Stud 2004;41:151–161.

with the statement, “My religious faith is the mostimportant influence in my life.”21 A more recentstudy of physicians in training found that for twothirds of them, God was important in their lives.22
Thus, the degree of disparity between the reli-giosity of the general population and that ofphysicians has not been firmly established.
Existential/spiritual needs of patients and families
Prevalence of Spiritual Needs. A study of an in-patient population documented that 76% of pa-tients at an urban hospital had three or more re-ligious needs, while this number increased to 88% for psychiatric patients.23 In another studyof 202 inpatients of an inner-city hospital, 35% re-quested spiritual care services.24 In a cross-sec-tional study that targeted next of kin during on-going palliative home care and in thebereavement period, 36% of respondents statedthey had experienced existential distress. Theserespondents described episodes of powerlessnessand/or helplessness every day or several timesper week.25
Patient Preferences in Regard to Evaluation of Spir-itual Needs and Physician Involvement in ReligiousPractices and Prayer. These general trends are mir-rored by patient requests regarding spiritual as-sessment and support. Several studies demon-strate that a majority of patients receiving healthcare prefer that their caregivers address their spir-itual concerns.26–28 In one study, 77% of patientswanted physicians to consider their spiritualneeds, 37% preferred that physicians discussthese needs with them more frequently, and 48%wanted physicians to pray with them.29 In an-other sample of patients,30 67% of patients indi-cated they would like their physicians to praywith them. Interestingly, nonreligious patientsfrequently endorse that physicians respectfullyaddress patients’ spiritual needs.27,31 A smallquantitative study documented that patientsvalue highly their physicians’ expressions of em-pathy, notably in an acknowledgment of religiousbeliefs and coping strategies.32
“Religiosity” or “spirituality” and health outcomes
Numerous studies have evaluated the relationbetween spirituality and health-related out-comes. While interpreting these studies, oneneeds to remain alert to the problem of the va-
lidity of instruments utilized in this kind of re-search.33 To what degree various “spirituality”scales measure the same phenomenon, orwhether such measured phenomena are indeedrelated to the individuals’ spirituality cannot bepresently answered for methodological reasons.Nevertheless, several trends and correlationsseem to emerge between measures of demo-graphically and psychologically defined spiritualattitudes, practices, coping behaviors, etc., andvarious health outcomes.
Psychological Well-being and Affective Outcomes.Recently, a well-designed series of studies34,35
demonstrated that spiritual well-being may havea protective effect against end-of-life despair anddepression. Specifically, patients with higherspiritual well-being as measured by the Func-tional Assessment of Chronic Illness Therapy-Spiritual Well-Being (FACIT-SWB) scale exhib-ited less desire for hastened death, suicidalideation, and a sense of hopelessness in the con-text of terminal illness.34 The effect of spiritualwell-being was stronger than any other variablemeasured. Other research groups reported simi-lar results.36,37 Importantly, level of depression,burden of physical symptoms or physical dis-ability, and social support all exerted less impacton the psychological suffering at the end of lifethan spiritual well-being. In a related patient sam-ple,35 researchers observed a strong negative as-sociation between the FACIT-SWB scale and de-pression scores. No such relationship was foundfor FACIT measured levels of religiosity, sug-gesting absence of protective value of (FACITmeasured) religiosity against depression.
Quality of Life, Including Coping Strategies. Qual-ity-of-life of patients at the end of life is uniquelydetermined by their spiritual concerns38–41 andcannot be reduced to other measures of psy-chosocial well-being and coping.42 Religious be-liefs may provide an effective coping frameworkto face the existential crises of life-threatening ill-ness.18,43–47 One study demonstrated that patientswith stable cancer rank prayer as the most im-portant coping strategy.48 A recent meta-analysisof 147 studies, which included a total of 98,975subjects, found that greater religiousness ismildly associated with fewer depressive symp-toms, particularly in people who were undergo-ing stress due to recent life events.49 This positiveeffect did not extend to individuals with extrin-
OKON394

sic religiosity and negative religious coping. Onestudy reported that cancer survivors who haddrawn on spiritual resources reported higher self-esteem and well-being in comparison with sur-vivors characterized by less self-transformativeresources or age-matched counterparts withoutcancer.50 Addressing spiritual needs may benefitcaregivers,51 as well as survivors, and extend intothe bereavement period.52
Medical decision making
Patients. Religious and spiritual convictions in-fluence patients in the process of medical deci-sion making.5,53 A study of patients with lungcancer documented that God is the second mostimportant consideration when deciding on anti-tumor treatment.54 A study of patients with ad-vanced gynecologic cancer revealed that 93% in-dicated that their religious lives helped themsustain their hopes.18 Similarly, 85% of a breastcancer support group respondents indicated thatreligion helped them to cope with their illness,55
a finding supported by empiric studies of copingstrategies in patients with melanoma.46,56 Last,from a denominational perspective, religion-based ethics provides a touchstone for clinical de-cision making of the believers. Palliative clini-cians should be able to locate appropriatereferences57–60 while caring for their diverse pa-tients.
Physicians. In contrast to patients and care-givers, faith is not an important factor in healthcare decisions for many of their physicians. In theemphasis on the significance of faith, patients dif-fer substantially from doctors.54 In a study of 100patients with advanced lung cancer and theircaregivers, patients ranked faith in God second,whereas their oncologists placed it last in the or-der of influences on treatment decisions. Not onlydid physicians differ substantially from their pa-tients in regard to judgment of the importance ofpatients’ faith in the process of medical decision-making, but also the physicians’ own beliefs in-fluence the process of care.
Faith and religious beliefs influence physicians’attitudes toward fundamental aspects of medicaldecision-making at the end of life. Physicians,nurses, and social workers disclosing lower lev-els of religious belief are more likely to endorseassisted suicide than those with higher levels ofbelief.61 Similarly, oncologists who report high or
moderate levels of religious belief are less likelyto perform euthanasia or physician-assisted sui-cide.62 Physicians without religious affiliation aremore likely to assist patients requesting physi-cian-assisted suicide.63
Health Outcomes (Mortality/Morbidity). The mostrigorous review of available studies to date64 doc-ument a reduced incidence of adverse outcomesin healthy populations of individuals attendingchurch regularly, strongly suggesting protectivevalue for non-ill persons. In other words, healthypeople are more likely to maintain their health ifthey also attend church regularly.65,66 On theother hand, increasing depth of religiousness(other than frequent church attendance) does notresult in more health. Furthermore, Powell et al.64
failed to find evidence for positive impact of re-ligion on progression of cancer, all-cause mortal-ity, recovery from acute illness, or a clear effectof intercessory prayer on objective health out-comes in severely ill patients. Another rigorousreview demonstrated evidence for a possiblephysiologic relation between religiosity/spiritu-ality and desirable health states and processes.67
The beneficial relationship between religiosity orspirituality and health status already suggestedby methodologically heterogenous studies, suchas those reviewed in a meta-analysis represent-ing almost 126,000 participants68 and numerousliterature reviews,69–72 warrant further prospec-tive studies.
ASSESSMENT METHODS
Taking spiritual history: recommendations andphysicians’ practice patterns
Regular, ongoing exploration of the spiritualneeds of patients at the end of life is uniformlyadvocated. Research and consensus statementson variables and preferences in the context of life-threatening illness18,73–87 and reflected in medicalcurricula88,89 demonstrate an agreement amongeducators, patients, and their caregivers alike inregard to certain crucial elements, such as skill-ful symptom management, sense of control, effec-tive communication, and contribution to othersalong with spiritual and existential transcen-dence. The World Health Organization guidelinesconsider spirituality an important dimension ofquality of life,90 while the Joint Commission on
SPIRITUAL, RELIGIOUS, AND EXISTENTIAL ASPECTS 395

Accreditation of Healthcare Organizations91 ex-plicitly mandates respect for patients’ spiritualvalues. A significant and unique association be-tween spirituality and quality of life has beenshown in a large sample of diverse patients lead-ing to the recommendation of including spiritualassessment in all oncology39 and palliative carepatients.92
Many physicians who infrequently inquireabout patients’ spiritual needs93 fail to considerit an important source of distress94 or refer pa-tients with spiritual needs to chaplains.93,95 In ac-tual practice physicians rarely screen for, or me-thodically address, the spiritual needs of theirpatients,96 in part because physicians frequentlydo not consider spiritual assessment to constitutea part of the standard medical evaluation97–100 orbecause of inadequate training, personal biases,or fear of being perceived as intrusive.93,97,101,102
Clinical assessment of spiritual needs
Two distinct approaches to addressing clini-cally relevant spiritual needs and attitudes exist.One derives from the general method of psy-chology and considers spirituality as a domain ofhuman experience and belief that correlates withmeasurable affective states, coping skills, and at-titudes. Consequently, the existing measurementtools attempt to quantify in a valid and reliablefashion, psychological states related to spiritualor religious beliefs. Developed for research goals,these instruments are not optimized for clinicaluse in the practice of palliative care, however. Forinstance, the authors of a repository of measure-ment tools in palliative care, the Toolkit (�www.chcr.brown.edu/pcoc/Spirit.htm�), upon reviewof the available instruments, rather than routinelyutilizing the existing scales, recommended de-veloping “a composite,” “a scale which is short,easy to answer.”
In contrast to the formalized, instrument-basedassessment, the second approach is based in thetradition of the comprehensive medical inter-view and advocates a consistent taking of spiri-tual history. No claims about psychometric prop-erties are made. Rather, the clinician skillfully addresses crucial elements of the individual’s history.
A choice of assessment method aside, the spir-itual needs of patients at the end of life need tobe explored regularly, while the process is beingcoordinated between various members of the in-
terdisciplinary team and documented such thatunnecessary repetition is avoided. Reevaluationis needed to ascertain efficacy of the counselingand support already provided.
Conceptual Considerations and Research Instru-ments. A recent, comprehensive review103 put for-ward four recurring constructs of religion andspirituality, and identified respective measure-ment tools (Table 2).
Closeness To and Knowledge of God. Closenessto and knowledge of God is a recurrent themeof many religions. Indeed, concepts of a beatificvision or eternal life depend on a degree of par-ticipation in the divine glory.104 Religious faith is helpful to patients in the time before deathbased on reports from relatives.84 Closeness toGod has been operationalized in several in-struments,105,106 frequently utilizing the attach-ment theory.107 Full instruments are too com-plex to be routinely utilized in the practice ofpalliative care. Exemplary questions are listedin Table 3.
Engagement with Everyday Life and Orientingforce. Faith and devotion as a pervading mode ofengagement with everyday life may be under-stood as the fundamental aspect of religiosity. In such a case, the reality of one’s existence isguaranteed by and possible only through an analogous participation in the overabundant lifeof God.108 Religiosity permeates all aspects of life, directs actions, and infuses meaning to oth-erwise nonintelligible life of a believer.109 Psy-chologists have operationalized these notions after observing that sacredness of life may trans-late into sense of meaning,110,111 stability, and empowerment, and hence improved coping ofpatients112,113 and their surviving family mem-bers.114 Religious engagement may translate intoricher decision-making strategies (inclusive ofhope, forgiveness, etc.). Extensive instrumentsare available,113,115–117 the most comprehensiveone extensively validated.118 Illustrative ques-tions are listed in Table 3.
Relationship and Support. According to yet an-other tradition, religiosity is borne and consum-mated in relationships. From the biblical advo-cacy of serving and loving the neighbor throughthe contemporary works of Rosenzweig, Buberand Levinas, congregational living out of love
OKON396

and compassion has been a fundamental compo-nent of many world religions. Psychologists op-erationalized these notions in measures of socialsupport,119,120 companionship, and community,all of which may lead to better coping,113 de-creased depression,119 and improved psycholog-ical adjustment.121 Social and emotional supportreceived in the context of religious participationcan be measured.122 Illustrative questions arelisted in Table 3.
Struggle. Religious and spiritual strugglesmay define the sense of an individual’s reli-giosity, modulate personal development,123,124
and affect medical decision making and care.54
A possibility of the positive,125,126 transforma-tive value of suffering is well illustrated in Pas-cal’s prayer, “In order to ask God for the gooduse of illness,”127 which acknowledges oppor-tunities inherent in ills and disgraces sufferedin the context of God’s mercy. The story of Job
SPIRITUAL, RELIGIOUS, AND EXISTENTIAL ASPECTS 397
TABLE 2. INSTRUMENTS COMMONLY UTILIZED IN CLINICAL RESEARCH
InstrumentsSource of recommended orrecommendation considered helpful Listed advantages of an instrument
Spirituality in A. Systems of Belief A. Examines support from a religious/spiritual community andcancer carea A. Inventory (SBI- A. presence and importance of religious and spiritual beliefs and
A. 15R)b A. practices.B. DRI/DURELc B. Short (5 items); an indicator of religious involvement rather thanC. FACIT-Spd A. spirituality.D. Brief R-COPEe C. Contains 2 factors (faith, and meaning and peace). Good
A. psychometric properties. Does not assume a belief in God on theA. part of respondent. The meaning and peace factor has beenA. shown to have particularly strong associations withA. psychological adjustment.D. Two dimensions: positive religious coping and negative religiousA. coping. Importantly, it identifies spiritual adjustment, i.e., theA. degree to which conflict, self-blame, or anger at God is present.
Toolkit A. Spiritual Well- A. A 20-item self-administered scale measuring spiritual well-beingA. Being Scalef A. in both its religious and existential senses. Sufficient validity forB. The Death A. use as a quality of life indicator.A. Transcendence B. A 25-item self-administered questionnaire with five subscales orA. Scaleg A. modes: religious, mystical, biosocial, creative and nature. TestC. Herth Hope Scaleh A. ways respondents use to transcend death.D. The Meaning of C. A 12-item interviewer administered scale measuring hopefulness.A. Life Scalei A. Useful in palliative care.
D. A 15-item administered by interview. Patient reports his or herA. assessment of the worth of life remaining. The scale is short andA. easy to administer.
aNational Cancer Institute. Spirituality in cancer care.⟨www.nci.nih.gov/cancerinfo/pdq/supportivecare/spirituality/healthprofessional⟩.bHolland JC, Kash KM, Passik S, Gronert MK, Sison A, Lederberg M, Russak SM, Baider L, Fox B: A brief spiritual
beliefs inventory for use in quality of life research in life-threatening illness. Psychooncology 1998;7:460–469.cSherman AC, Plante TG, Simonton S, Adams DC, Harbison C, Burris SK: A multidimensional measure of religious
involvement for cancer patients: the Duke Religious Index. Support Care Cancer 2000;8:102–109.dPeterman AH, Fitchett G, Brady MJ, Hernandez L, Cella D: Measuring spiritual well-being in people with cancer:
the functional assessment of chronic illness therapy—Spiritual Well-being Scale (FACIT-Sp). Ann Behav Med2002;24:49–58.
ePargament KI, Smith BW, Koenig HG, Perez L: Patterns of positive and negative religious coping with major lifestressors. J Sci Stud Relig 1998;37:710–724.
fPaloutzian RF, Ellison CW. Loneliness, spiritual well-being and quality of life. In: Peplau LA, Perlman D (eds):Loneliness: A Sourcebook for Current Theory, Research and Therapy. New York: John Wiley and Sons, 1982.
gVandeCreek L, Nye C. Testing the Death Transcendence Scale. J Sci Stud Relig 1993;32:279–283.hHerth K: Development and refinement of an instrument to measure hope. Scholarly Inquiry Nurs Pract
1991;5:39–51.iWarner SC, Williams JI: The Meaning in Life Scale: determining the reliability and validity of a measure. J Chron
Dis 1987;40:503–512.
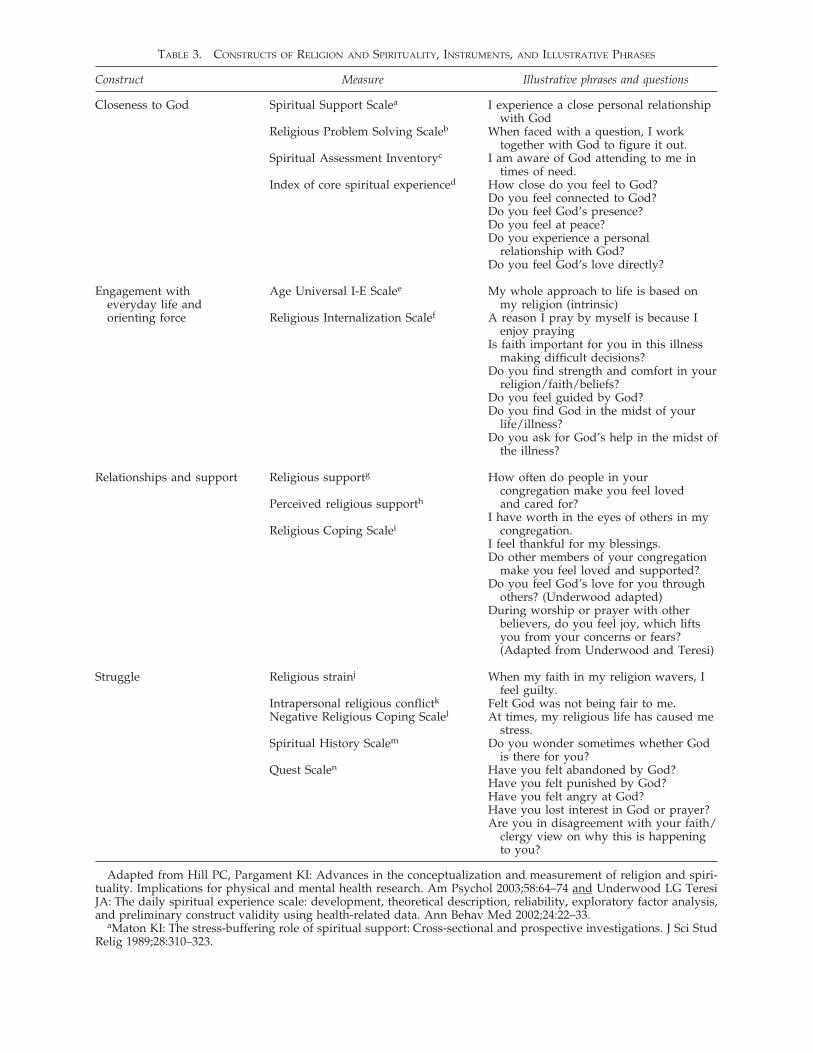
TABLE 3. CONSTRUCTS OF RELIGION AND SPIRITUALITY, INSTRUMENTS, AND ILLUSTRATIVE PHRASES
Construct Measure Illustrative phrases and questions
Closeness to God Spiritual Support Scalea I experience a close personal relationshipwith God
Religious Problem Solving Scaleb When faced with a question, I worktogether with God to figure it out.
Spiritual Assessment Inventoryc I am aware of God attending to me intimes of need.
Index of core spiritual experienced How close do you feel to God?Do you feel connected to God?Do you feel God’s presence?Do you feel at peace?Do you experience a personal
relationship with God?Do you feel God’s love directly?
Engagement with Age Universal I-E Scalee My whole approach to life is based oneveryday life and my religion (intrinsic)orienting force Religious Internalization Scalef A reason I pray by myself is because I
enjoy prayingIs faith important for you in this illness
making difficult decisions?Do you find strength and comfort in your
religion/faith/beliefs?Do you feel guided by God?Do you find God in the midst of your
life/illness?Do you ask for God’s help in the midst of
the illness?
Relationships and support Religious supportg How often do people in yourcongregation make you feel loved
Perceived religious supporth and cared for?I have worth in the eyes of others in my
Religious Coping Scalei congregation.I feel thankful for my blessings.Do other members of your congregation
make you feel loved and supported?Do you feel God’s love for you through
others? (Underwood adapted)During worship or prayer with other
believers, do you feel joy, which liftsyou from your concerns or fears?(Adapted from Underwood and Teresi)
Struggle Religious strainj When my faith in my religion wavers, Ifeel guilty.
Intrapersonal religious conflictk Felt God was not being fair to me.Negative Religious Coping Scalel At times, my religious life has caused me
stress.Spiritual History Scalem Do you wonder sometimes whether God
is there for you?Quest Scalen Have you felt abandoned by God?
Have you felt punished by God?Have you felt angry at God?Have you lost interest in God or prayer?Are you in disagreement with your faith/
clergy view on why this is happeningto you?
Adapted from Hill PC, Pargament KI: Advances in the conceptualization and measurement of religion and spiri-tuality. Implications for physical and mental health research. Am Psychol 2003;58:64–74 and Underwood LG TeresiJA: The daily spiritual experience scale: development, theoretical description, reliability, exploratory factor analysis,and preliminary construct validity using health-related data. Ann Behav Med 2002;24:22–33.
aMaton KI: The stress-buffering role of spiritual support: Cross-sectional and prospective investigations. J Sci StudRelig 1989;28:310–323.

provides an excellent example of suffering andstruggle with God, which, questioning divinejustice and benevolence, also admits the possi-bility of mercy and providence.128 However, re-ligious struggles may also be associated with anunequivocally negative impact129 on health out-comes. A recent study showed that depressionwas associated with feelings of alienation fromGod and suicidality was associated with reli-gious fear and guilt,130,131 while religious strug-gles delayed recovery during the medical reha-bilitation process,132 increased mortality inelderly ill patients,133 and increased length ofhospitalization.134 Illustrative questions arelisted in Table 3.
Collections of Measurement Tools and InstrumentsMost Commonly Utilized in Clinical Research. Com-prehensive repositories of measurement tools are available (�www.chcr.brown.edu/pcoc/Spirit.htm�).135,136 Global measures of daily spiritual ex-perience118 or appraisals of spiritual well-being,such as the FACIT scale,34,35,39 have been vali-dated and thus proved appropriate for clinical re-search. Various authors list a diverse list of help-ful instruments (see Table 2).
Taking Spiritual History: a Therapeutic Interventionin Palliative Care. In order to appreciate the im-portance of spiritual history in the practice of pal-liative care, one needs to first turn the gaze to the nature of the patient–physician relationship.In a self-evident fashion, the patient–physician en-counter that subsequently leads to a therapeuticrelation is a fundamental phenomenon of clinicalmedicine. Following Pellegrino, one may constructa clinical encounter in a relational mode as a meet-ing of “doctors and patients whose lived worldsintersect in the moment of clinical truth.”137 In-habiting the language of hopes and suffering, thetherapeutic narrative becomes a “joint construc-tion,”138,139 a result of collaboration between pa-tient and physician rather than a gathering of “ob-jective” instrumental data characteristics of thepsychometrically focused psychology or of princi-plist and casuist ethics. Indeed, the position of theAssociation of American Medical Colleges re-vealed in its Medical School Objectives Project88 isthat clinicians are to “seek to understand the mean-ing of the patients’ stories in the contexts of the pa-tients’ beliefs, and family and cultural values.”
The clinical process of diagnosis, prognosis,therapy, and education presupposes a human
SPIRITUAL, RELIGIOUS, AND EXISTENTIAL ASPECTS 399
TABLE 3. CONSTRUCTS OF RELIGION AND SPIRITUALITY, INSTRUMENTS, AND ILLUSTRATIVE PHRASES (CONT’D)
Construct Measure Illustrative phrases and questions
bPargament KI, Kennell J, Hathaway W, Grevengoed N, Newman J, Jones W: Religion and the problem-solvingprocess: three styles of coping. J Sci Stud Relig 1988;27:90–104.
cHall TW, Edwards KJ: The initial development and factor analysis of the Spiritual Assessment Inventory. J Psy-chol Theol 1996;24:233–246.
dKass JD, Friedman R, Lesserman J, Zuttermeister P, Benson H: Health outcomes and a new index of spiritual ex-perience. J Sci Stud Relig 1991;30:203–211.
eGorsuch RL, Venable GD: Development of an “age universal” I-E scale. J Sci Stud Relig 1983;22:181–187.fRyan RM, Rigby S, King K: Two types of religious internalization and their relations to religious orientations and
mental health. J Pers Soc Psychol 1993;65:586–596.gKrause N: Religious support long form, religious support short form. In: Fetzer Institute. Multidimensional mea-
surement of religiousness/spirituality for use in health research. Kalamazoo, MI: Fetzer Institute 1999;57–63 ⟨www.fetzer.org/Resources/resources_multidimens.htm⟩.
hFiala WE, Bjorck JP, Gorsuch RL: The Religious Support Scale: Construction, validation, and cross-validation. AmJ Commun Psychol 2002;30:761–786.
iPargament KI, Koenig HG, Perez LM: The many methods of religious coping: development and initial validationof the RCOPE. J Clin Psychol 2000;56:519–543.
jExline JJ, Yali AM, Sanderson WC: Guilt, discord, and alienation: the role of religious strain in depression and sui-cidality. J Clin Psychol 2000;56:1481–1496.
kTrenholm P, Trent J, Compton WC: Negative religious conflict as a predictor of panic disorder. J Clin Psychol1998;54:59–65.
lPargament KI, Zinnbauer BJ, Scott AB, Butter EM, Zerowin J, Stanik P: Red flags and religious coping: Identifyingsome religious warning signs among people in crisis. J Clin Psychol 1998;54:77–89.
mHays JC, Meador KG, Branch PS, George LK: The Spiritual History Scale in four dimensions (SHS-4): validity andreliability. Gerontologist 2001;41:239–249.
nBatson CD, Schoenrade P, Ventis WL: Religion and the Individual: A Social-Psychological Perspective. New York:Oxford University Press. 1993.

relation between two persons, a patient and aphysician. The joint, even if silent, constructionof the individual narrative of suffering has longbeen recognized as a supreme form of effectiveministry to the sick. In a commentary on Job,Piper128 reminds us that
Through seven days they sat,And wept with Job, so broken thatThey could not speak. Job felt the powerOf silent love, and every hourWas like a gift.
Indeed the analytic tradition confirms thatdeath and agony are always a mystery, the endof the world. “[In death] the world does notchange, but ceases.”140 An aporia and mystery,death is not suited for solution, but for being to-wards a transformation or a narrative dwelling.Indeed, a cardinal feature of palliative medicineis that the physician is called to face and ac-knowledge the suffering of the other. It is in thisobservant manner that the physician learns of the
patient’s concerns while developing a unique re-lationship in which the diagnostic evaluation it-self becomes a part of the therapeutic interven-tion.141
Nowhere is this “diagnosis as treatment” par-adigm more prominent than in the physician’sresponding to existential and spiritual concernsof patients at the end of life. For, as a scholar onspiritual assessment noted, the “caring part ofthe doctor/patient relationship is enacted”through bilateral participation in the respectivespiritual or existential resources of patient anddoctor.142 Given these conceptual considera-tions, as well as the documented association be-tween a physician’s own spiritual beliefs andclinical practice style, including the willingnessto allow or prohibit euthanasia or physician-as-sisted suicide,62,63 it is imperative that palliativecare physicians are equally aware of their ownbeliefs and emotions.
The process of clinical assessment of spiritualneeds may take two distinct forms, open-endedand structured.
Taking Spiritual History—Open-Ended Format. Inthe open-ended format, the dialogue is initiatedwith a general question (Table 4). The initial in-quiry allows the physician to glimpse at the roleof faith in a patient and anticipate the characterof further dialog and intervention. Following thepatient lead, the physician allows the conversa-tion to unfold by its own dynamics while re-sponding to the other person.
OKON400
TABLE 4. OPENING QUESTIONS IN THE OPEN-ENDED
FORMAT OF OBTAINING SPIRITUAL HISTORY
Is faith important in your life?What roles does spirituality or religion play in your
life?Does life feel like a gift or like a burden as you go
through this illness?What brings meaning and purpose to your life?
TABLE 5. OBTAINING SPIRITUAL HISTORY
CENTERED AROUND PRACTICE OF PRAYER, SEMISTRUCTURED INTERVIEW GUIDE
1. What is prayer? Tell me more about it. (Probes: How would you describe what prayer is? Why is prayerimportant to you? What does prayer mean to you?)
2. Describe how you pray. (Probes: What things do you do before, during, or after prayer? What assists you topray? Do you have any special strategy/format you use when you pray?)
3. What do you pray for? What do you pray about? Tell me more. (Probe: Can you give me an example of one ofyour recent prayers?)
4. How did you learn to pray (over your life-time)? (Probe: Have there been certain times in your life when youlearned something about prayer?)
5. What do you expect will happen as a result of your prayers? (Probes: You pray, and then what happens?Some people pray for answers, do you? What answers/solutions do you pray for?)
6. Has your praying changed since your illness? How has it changed? How has prayer influenced your cancerexperience? If illness were somehow to influence the way you pray, how might it? (Probes: How has yourillness affected your praying? Your beliefs about prayer? Has your illness interfered with how you pray?)
7. When you were told you had cancer, did you pray about it? Would you tell me about it now? What did youexpect as a result of your prayers?
8. Describe how prayer makes you feel. Describe one time when you had such a feeling.
Adapted from Taylor EJ, Outlaw FH: Use of prayer among persons with cancer. Holist Nurs Pract 2002;16:46–60.(Reprinted with permission.)

Although not formally structured, the open-ended dialog frequently includes certain charac-teristic themes (Table 3). The initial question aimsat an understanding of the general character oftranscendent beliefs. If religious faith is impor-tant to the patient, the four basic constructs offaith as a source of (1) God’s closeness, love, pres-ence; (2) a sense of call, meaning, and intelligi-bility of one’s life story; (3) a personal relation-ship and support from God, as well as a sense ofjoy and hope; and finally (4) transformation andforgiveness versus struggle, doubt, guilt, andpunishment are all explored in a respectful andconsiderate dialogue. A recent phenomenologicanalysis of the use of prayer to cope among per-sons with cancer suggests how such data can beused in clinical practice to conceptualize and in-quire about a patient’s prayer disposition143 andlead to an effective communication. A semistruc-tured interview guide has been proposed as a re-sult of this investigation (Table 5). If religiousfaith is not a prominent aspect of the patient’s be-liefs, topics of meaning, legacy, gratitude, hope,forgiveness, and trust are likely to be more promi-nent (Table 6).
Taking Spiritual History—A Structured Format.The formal process of obtaining a spiritual his-tory can be structured in several ways (Table 7).Although developed independently, the varioustools share common themes. Guided by a uniquemnemonic, the interviewer is prompted to ad-dress each of the following domains: (1) the char-acter of transcendent beliefs (religious/spiri-tual/denominational/atheistic, etc.), (2) religiousaffiliation/membership, (3) personal meaningand importance of faith and spiritual sources ofstrength, as well as (4) the impact of beliefs onmedical decision-making and process of care.
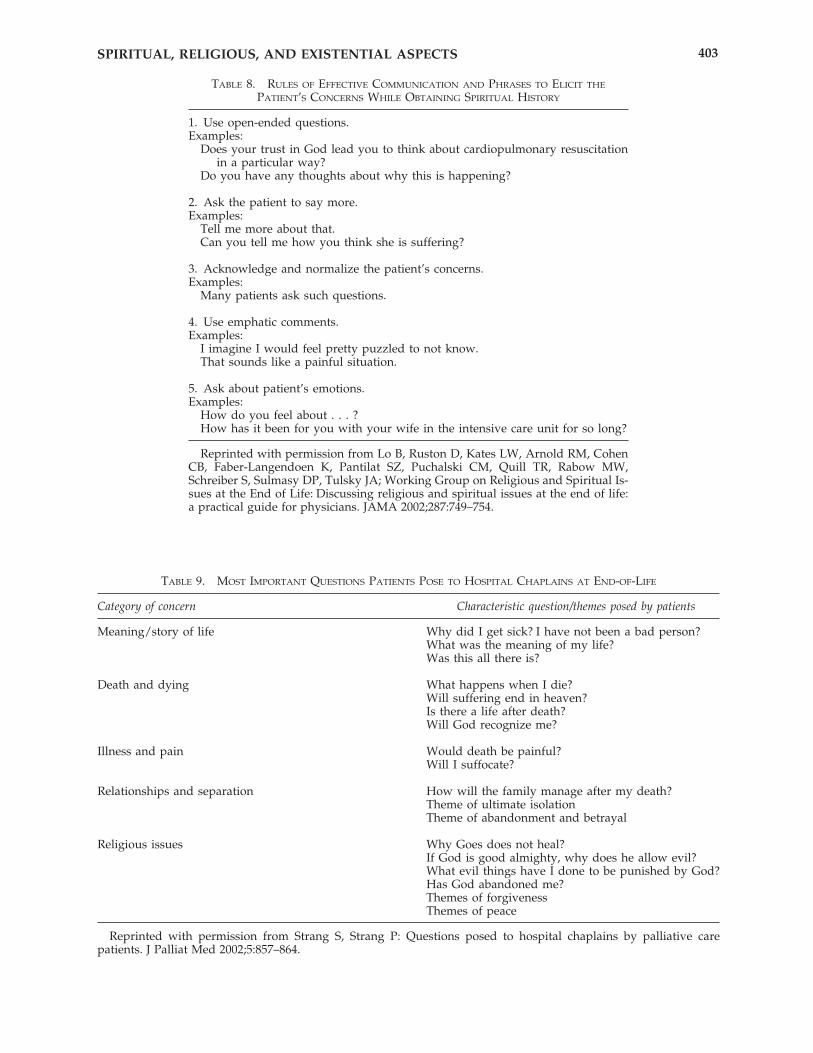
Regardless of a particular format chosen by thepatient and physician to communicate about spir-itual issues, the accepted rules of effective clini-cal communication (Table 8) and conversationaldevices other than questions139 should be uti-lized. Another important communication tech-nique is to align basic concerns and goals of care.In the context of an incurable disease, the initialformulation of desired goals of the patient or thefamily may be at odds with that of a physician,opening a potential for a conflict. However, byaligning the broad, primary concerns (“The most
SPIRITUAL, RELIGIOUS, AND EXISTENTIAL ASPECTS 401
TABLE 6. THEMES OF EXISTENTIALLY-FOCUSED HISTORY
Theme/construct Examples of exploratory questions
Meaning What is it like to go through this illness? Doesanything bring sense to your illness/experience? Whatbrings comfort to your life? Are you at peace? Do youfeel a void in your life? What brings purpose to yourlife?
Hopes, identity, and continuity What do you hope for? What are your dreams andgoals? What are the things/projects you still want toachieve/complete? What is still possible? What doyou still enjoy doing?
Legacy How would you like to be remembered (by peopleyou care about)? Have you had a sense of servingothers? Have you ever had causes you fought orworked for? Is there anything or anyone whose needsyou would put above yours? What are you especiallyproud of?
Trust, support, and caring relationships Who are you the closest to? Who is your closestconfidante? What role have you been playing in yourfamily? What brings fun and laughter to your life?
Life review: experience of pain and forgiveness or Are there any conflicts you wish to resolve? Are thereestrangement and reconciliation any people you have not seen in a long time whom
you wish to contact/talk to? Do you feel in need toreconcile with somebody? Do you feel burdened by asense of guilt?
Resilience and self-efficacy What makes you strong in the midst of this illness?Do you feel in control? What can you do to helpyourself? What can you do to still make a differencein your life?

important reason for my becoming involved is toensure that your loved one receives the best andmost appropriate care”), the provider avoids un-necessary confrontation and creates a conditionfor developing trust, as well as a sense of em-powerment and choice on the part of familymembers.
CLINICAL PRESENTATIONS
Characteristics of spiritual needs
A national survey using an open-ended ques-tionnaire to define the three most important ques-tions patients posed to hospital chaplains at the
end of life was carried out recently in Sweden.144
The main domains that emerged after contentanalysis were meaning (34%), death and dying(21%), pain and illness (13%), and relationships(15%) (Table 9). Patients primarily posed ques-tions of a general existential nature regardingdeath and dying. Only 8% of the issues were ex-plicitly religious.
Older, more severely ill patients who considerthemselves more religious request pastoral ser-vices more often.24 Interestingly, patients consid-ered being at risk for spiritual injury or psy-chosocial stress asked for spiritual care much lessfrequently than those already enjoying high lev-els of religious and spiritual support. The authorssuggested that targeting patients for pastoral sup-
OKON402
TABLE 7. STRUCTURED APPROACHES TO OBTAINING SPIRITUAL HISTORY
Tool Domains Examples of content
HOPEa H: sources of hope H: What gives you hope (or strength or comfortO: organized religion O: or peace) in the time of illness?P: personal spirituality and O: Are you a part/member of religious orP: practices O: spiritual community? Does it help you?E: effect on medical care and O: How?P: end-of-life issues P: What aspects of your spiritual beliefs do you
O: find most helpful and meaningful personally?E: How do your beliefs affect the kind ofO: medical care you would like me to provideO: over the next few days/weeks/months.
FICA: F: Faith F: What is your faith? “Do you consider yourselfSpiritual I: Importance/influence O: spiritual or religious?”historyb C: Community I: What importance does your faith or belief
A: Address/apply O: have in your life?C: Are you part of a religious community?A: How would you like me as your provider toO: address these issues in your care?
SPIRITc S: Spiritual belief system; S: Do you have a formal religious affiliation? Do P: Personal spirituality; O: you have a spiritual life that is important toI: Integration with a spiritual O: you?I: community; P: In what ways is your spirituality important toR: Ritualized practices and O: you?R: restrictions; I: Do you belong to any religious or spiritualI: Implications for medical O: groups or communities?I: care; R: What specific practices do you carry out asT: Terminal events planning O: part of religious or spiritual life?
I: Would you like to discuss religious or spiritualO: implications of health care?T: Are there particular aspects of medical careO: that you wish to forgo or have withheldO: because of your religion/spirituality?
aAnandarajah G, Hight E: Spirituality and medical practice: Using the HOPE questions as a practical tool for spir-itual assessment. Am Fam Physician 2001;63:81–89.
bPuchalski CM, Romer AL: Taking a spiritual history allows clinicians to understand patients more fully. J PalliatMed 2000;3:129–137.
cMaugans TA: The SPIRITual history. Arch Fam Med 1996;5:11–16. (Reprinted with permission.)
SPIRITUAL, RELIGIOUS, AND EXISTENTIAL ASPECTS 403
TABLE 8. RULES OF EFFECTIVE COMMUNICATION AND PHRASES TO ELICIT THE
PATIENT’S CONCERNS WHILE OBTAINING SPIRITUAL HISTORY
1. Use open-ended questions.Examples:
Does your trust in God lead you to think about cardiopulmonary resuscitationin a particular way?
Do you have any thoughts about why this is happening?
2. Ask the patient to say more.Examples:
Tell me more about that.Can you tell me how you think she is suffering?
3. Acknowledge and normalize the patient’s concerns.Examples:
Many patients ask such questions.
4. Use emphatic comments.Examples:
I imagine I would feel pretty puzzled to not know.That sounds like a painful situation.
5. Ask about patient’s emotions.Examples:
How do you feel about . . . ?How has it been for you with your wife in the intensive care unit for so long?
Reprinted with permission from Lo B, Ruston D, Kates LW, Arnold RM, CohenCB, Faber-Langendoen K, Pantilat SZ, Puchalski CM, Quill TR, Rabow MW,Schreiber S, Sulmasy DP, Tulsky JA; Working Group on Religious and Spiritual Is-sues at the End of Life: Discussing religious and spiritual issues at the end of life:a practical guide for physicians. JAMA 2002;287:749–754.
TABLE 9. MOST IMPORTANT QUESTIONS PATIENTS POSE TO HOSPITAL CHAPLAINS AT END-OF-LIFE
Category of concern Characteristic question/themes posed by patients
Meaning/story of life Why did I get sick? I have not been a bad person?What was the meaning of my life?Was this all there is?
Death and dying What happens when I die?Will suffering end in heaven?Is there a life after death?Will God recognize me?
Illness and pain Would death be painful?Will I suffocate?
Relationships and separation How will the family manage after my death?Theme of ultimate isolationTheme of abandonment and betrayal
Religious issues Why Goes does not heal?If God is good almighty, why does he allow evil?What evil things have I done to be punished by God?Has God abandoned me?Themes of forgivenessThemes of peace
Reprinted with permission from Strang S, Strang P: Questions posed to hospital chaplains by palliative care patients. J Palliat Med 2002;5:857–864.

port by employing spiritual risk screening meth-ods145,146 might result in the greatest counselingbenefit.
“Red Flags” and Reasons for Referral. Physiciansneed to remain vigilant for clues of spiritual andexistential suffering.147 The ultimate standard ofcare for patients with significant burdens is a re-ferral to spiritual services or psychological coun-seling. If a patient articulates or suggests distress(Table 10), an empathic, respectful, open-endeddialogue may help elucidate the nature of theconcern. However, under these circumstances itis mandatory to refer the patient to professionalpastoral or psychological counseling, as the pro-vision of comprehensive spiritual support usu-ally exceeds the professional competencies ofeven the most thoughtful physician.
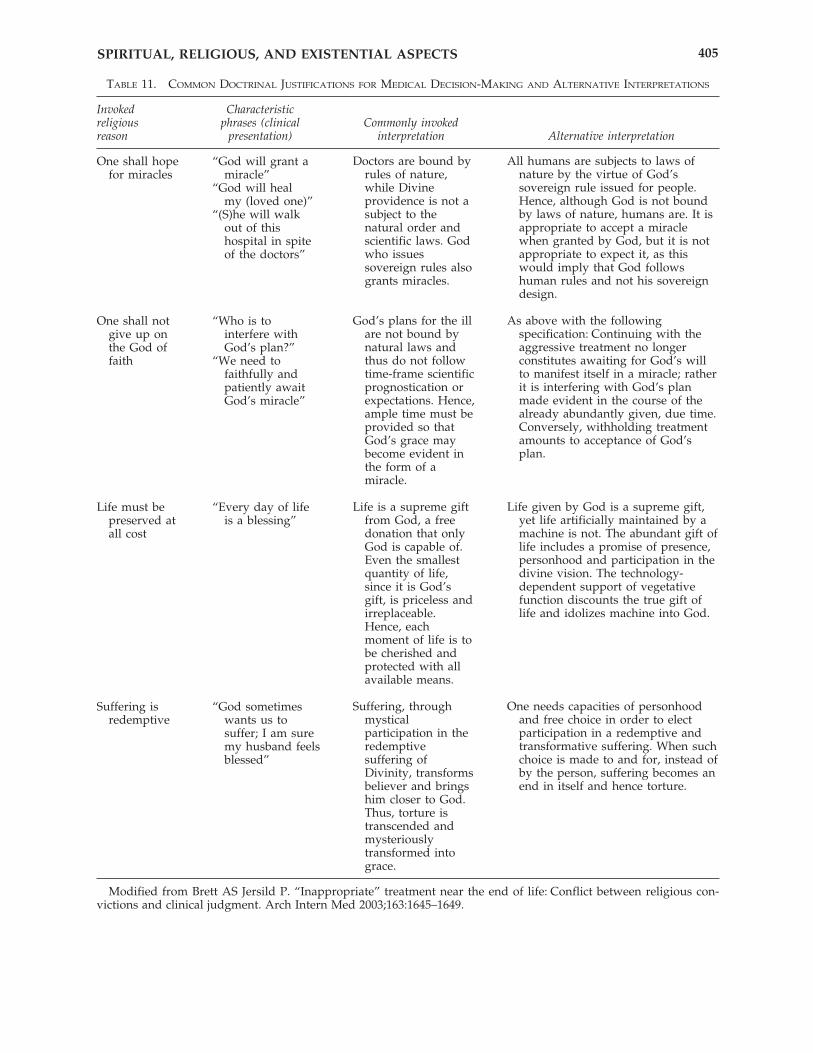
Spirituality and Futility: Doctrinal Justifications ofMedical Decision-Making. In the context of life-limiting illness, patients and families sometimesinvoke doctrinal justification for their medical decision-making. Most commonly, this clinicalpresentation involves the dilemma of futility ver-sus benefit of continuing care, and may bephrased in various ways (Table 11, column 2).Four categories of such theologically inspired rea-soning have been recently described,148 alongwith ways of responding to such statements uti-lizing alternative interpretations (Table 11). It isnecessary to recognize that offering these or otherinterpretative alternatives in a way of serious de-liberation of theological beliefs is, by the very na-ture of such an act, a polemical or an exegeticalactivity, and thus must be left to trained chap-lains or theologians. Furthermore, invoking doc-trinal justifications may result from non-spiritualand non-theological distress. It is imperative that
the physician examines the state of communica-tion about the illness, as well as the emotionalburden of the disease, and utilizes rules of effec-tive communication (Table 8) and counseling asthe primary therapeutic approach. Nevertheless,a rudimentary knowledge of common doctrinallyphrased justifications might prove helpful whileattempting to comprehend or respond to dog-matically driven requests for medical care.
Responding to Request for Prayer. Explicit prayerinvolving a physician should not be carried outwithout the patient’s request and permission.149
However, physicians can respectfully respond torequests for prayer in ways that may enhance thetherapeutic relationship.150 The support shouldbe carried out without compromising the physi-cian’s own religious and spiritual beliefs or pro-fessional roles. For instance, a physician may con-sider remaining present and standing silentlywhile the patient and the family is praying. De-pending on the individual character of the pa-tient-physician relationship, any combination of(1) disclosing an element of the physician’s ownbeliefs (I am not a Muslim . . . ) and, (2) offeringpassive support ( . . . but I believe that prayer isimportant; let me leave now so that you can praytogether in a community of faithful), or (3) activesupport ( . . . but I will gladly remain with youin silence) and (4) joining in prayer consistentwith doctor’s own beliefs ( . . . and quietly prayalong with you in the way peace finds a way tomy heart), or (5) joining in praise and petition ( . . . and worship the Lord together so that hemay bless those who are ill and in need) mightbe appropriate. In regard to allowing religiousand spiritual practices in the hospital, institu-tional guidelines regarding religious ceremoniesshould be phrased as liberally as possible. How-ever, good care both for the patient for whom theritual is offered and for other patients within thefacility should remain the primary concern whiledeveloping such guidelines.
Responding to Inquiry about Physician’s Religion.There is no professional mandate for a physicianto disclose his religion.151 However, a questionabout the doctor’s faith may be an expression ofa need for spiritual support rather than a matterof curiosity, or a need to identify with a healthcare provider on a denominational level. Fur-thermore, such a question also may be the pa-tient’s attempt to initiate a discussion related to
OKON404
TABLE 10. INTERVIEW CLUES SIGNIFYING POTENTIALLY
UNANSWERED SPIRITUAL OR EXISTENTIAL NEEDS
I’m wondering if God is here for me right now.It feels as though God were punishing me.I am angry that God did not hear my prayers.I just don’t understand.Why is this happening to me?I’ve been a believer all my life, but . . . (phrase
frequently left open), or: but I gave up trying.I feel abandoned.God has not been fair to me.I am worried that my son/daughter is not going to
remember who I was.I failed God.
SPIRITUAL, RELIGIOUS, AND EXISTENTIAL ASPECTS 405
TABLE 11. COMMON DOCTRINAL JUSTIFICATIONS FOR MEDICAL DECISION-MAKING AND ALTERNATIVE INTERPRETATIONS
Invoked Characteristicreligious phrases (clinical Commonly invokedreason presentation) interpretation Alternative interpretation
One shall hope “God will grant afor miracles miracle”
“God will healmy (loved one)”
“(S)he will walkout of thishospital in spiteof the doctors”
One shall not “Who is togive up on interfere withthe God of God’s plan?”faith “We need to
faithfully andpatiently awaitGod’s miracle”
Life must be “Every day of lifepreserved at is a blessing”all cost
Suffering is “God sometimesredemptive wants us to
suffer; I am suremy husband feelsblessed”
Modified from Brett AS Jersild P. “Inappropriate” treatment near the end of life: Conflict between religious con-victions and clinical judgment. Arch Intern Med 2003;163:1645–1649.
All humans are subjects to laws ofnature by the virtue of God’ssovereign rule issued for people.Hence, although God is not boundby laws of nature, humans are. It isappropriate to accept a miraclewhen granted by God, but it is notappropriate to expect it, as thiswould imply that God followshuman rules and not his sovereigndesign.
As above with the followingspecification: Continuing with theaggressive treatment no longerconstitutes awaiting for God’s willto manifest itself in a miracle; ratherit is interfering with God’s planmade evident in the course of thealready abundantly given, due time.Conversely, withholding treatmentamounts to acceptance of God’splan.
Life given by God is a supreme gift,yet life artificially maintained by amachine is not. The abundant gift oflife includes a promise of presence,personhood and participation in thedivine vision. The technology-dependent support of vegetativefunction discounts the true gift oflife and idolizes machine into God.
One needs capacities of personhoodand free choice in order to electparticipation in a redemptive andtransformative suffering. When suchchoice is made to and for, instead ofby the person, suffering becomes anend in itself and hence torture.
Doctors are bound byrules of nature,while Divineprovidence is not asubject to thenatural order andscientific laws. Godwho issuessovereign rules alsogrants miracles.
God’s plans for the illare not bound bynatural laws andthus do not followtime-frame scientificprognostication orexpectations. Hence,ample time must beprovided so thatGod’s grace maybecome evident inthe form of amiracle.
Life is a supreme giftfrom God, a freedonation that onlyGod is capable of.Even the smallestquantity of life,since it is God’sgift, is priceless andirreplaceable.Hence, eachmoment of life is tobe cherished andprotected with allavailable means.
Suffering, throughmysticalparticipation in theredemptivesuffering ofDivinity, transformsbeliever and bringshim closer to God.Thus, torture istranscended andmysteriouslytransformed intograce.

existential concerns. Hence, rather than uni-formly exercising a right to withhold this infor-mation (“I’d rather focus on you, and your con-cerns”), the palliative care physician shouldexplore the motivation behind the question. Thisis best accomplished by further probing the pa-tient’s concerns: “I am Druid, but I wonder whyyou are asking?,” or simply “I wonder why youasked?” Such a clarification allows for a better un-derstanding of the patient’s actual dilemma andopens a potential for a therapeutic response. Asis the case with any discussion involving exis-tential or spiritual matters, physicians must rec-ognize their limitations in regard to exegetics,hermeneutics, and professional counseling andrefer to the chaplaincy when needed.
THERAPEUTIC OPTIONS
Physician/interdisciplinary team member driven support
Within the context of inconclusive, usually preliminary data derived from relatively smallsamples, recommendations for physician–driveninterventions for spiritual distress suggest a re-spectful and self-reflected approach, which ob-serves standard principles of the therapeutic re-lationship.
According to a position statement of a Work-ing Group on Religious and Spiritual Issues at theEnd of Life151 on the role of physicians in at-tending to the spiritual needs of patients, the fol-lowing principles should be observed:
• Respect the patient’s views and follow the pa-tient’s lead.
• Collaborate and connect with patients by lis-tening carefully and acknowledging the pa-tient’s concerns, but stay away from theologi-cal discussions or engaging in specific religiousrituals.
• Maintain one’s own integrity in regard to one’sown religious beliefs and practices.
• Identify common goals for care.• Utilize appropriate professional resources of
support for the patient, such as referral to achaplain or encouraging contact with the pa-tient’s own clergy.
Notably, the members of the Working Groupcondoned neither physicians providing pastoral
support or counseling nor leading therapy, un-less they are formally trained to do so. Indeedqualitative data suggest that naïve, proselytizingor unskilled conversations about prayer with pa-tients with cancer may result in exacerbation ofspiritual suffering.143
Pastoral Consultation: Areas of Competence andProfessional Boundaries
In contemporary Western medicine, the pro-fessional roles of chaplains and physicians arekept separate. Since the times of Osler and Cabot,hospital chaplains, unlike physicians, have beenregarded as a most appropriate resource to assistpatients with their spiritual needs.24,97,149,152–154
In one study94 over 85% of both physicians andregistered nurses felt that ideally a chaplainshould address spiritual issues. In spite of the ex-plicit acceptance of the pastoral support amongthe majority of health providers, the actual refer-ral patterns vary. Most family physicians sur-veyed in one study accepted clergy and pastoralprofessionals in the care of their patients,155 whileanother survey documented infrequent referralsof hospitalized patients to chaplains.93 Far fromdiscounting the referring and adjuvant role ofphysicians in the process of counseling, the au-thors of a Swedish national survey of hospitalchaplains concluded that professional pastoraland counseling competence is essential in exis-tential discussions with patients in crisis.144 Uti-lizing specialized knowledge and skills to mobi-lize spiritual resources, pastoral counselors assistpatients with developing more effective copingskills.156
Chaplains provide supportive spiritual carethrough empathic listening while emphasizinga healing potential of religious faith. They en-courage life review as well as an exploration offeelings such as guilt or remorse. Spiritual coun-selors facilitate reconciliation and support prac-tical application of the patient’s own faith con-structs and spiritual resources. They help withestablishing a sense of legacy through assistingwith telling life stories and recovering themesof meaning and worth. With an understandingthat proselytizing is universally prohibited,they are charged with a professional obligationto protect patients from unwelcome spiritual ordevotional intrusion. The pastoral services playa particularly important role in supporting pa-tients in spiritual distress.24
OKON406

Therapy
At the present time there is no empiric evidencethat an existing, structured, reproducible inter-vention aimed at improving symptom control orquality of life while specifically targeting spiri-tual needs or despair of patients while utilizingtherapy or counseling is effective at the end oflife. However, there is a growing evidence thataddressing spiritual well-being may eventuallylead to the development of effective techniques.
In a large sample of patients with cancer, spir-itual well-being was found to be related to theability to enjoy life in spite of physical symptomburden. This and other similar studies provideempirical support to a hypothesis that the spiri-tual well-being domain may be an importanttherapeutic target.34,39 A study in patients withbreast cancer that compared standard group sup-port with an alternative support utilizing medi-tation, affirmation, imagery and ritual, failed to demonstrate a difference in psychosocial outcomes between the interventions.43 A pilotstudy157 designed to integrate spiritual issues and
assist participants in drawing on spiritual re-sources in the course of supportive therapy hasnot led to conclusive, published data on the effectiveness of this approach (K. Pargament, personal communication, March 2004). A smallquasiexperimental, partial randomization, pref-erence trial utilizing a support group based onself-transcendence theory showed transient im-provement in the sense of well-being in patientswith breast cancer during active involvement inthe therapy. These effects did not last after dis-continuation of the support.158 In a pilot study ofmeaning-centered therapy at the conclusion ofthe support intervention, participants scoredhigher on the meaning subscale of the FACITscale.159 However, multiple trials showed thatstandard supportive-expressive psychotherapythat encourages expression of emotions aboutvarious aspects of life, including spiritual con-cerns, results in significant improvement in paincontrol160 and mood160–162 in patients with ad-vanced breast cancer. A meta-analysis163 of arange of supportive psychosocial interventionssuggested a benefit for emotional and functional
SPIRITUAL, RELIGIOUS, AND EXISTENTIAL ASPECTS 407
TABLE 12. MEANING CENTERED PSYCHOTHERAPY INTERVENTION
Session Topic Exemplary task or exercise
1 Concepts and sources of meaning: List one or two experiences or moments when lifeexperimental exercises has felt particularly meaningful to you
2 Cancer and meaning: experiential Write down 4 answers to the question, “Who am I?”exercises How has cancer affected your answers?
3 Meaning and historical context Tell us the story of your name.of life: exercises Tell us about your life and the history of your
family.4 Meaning and historical context What are your most important accomplishments,
of life: exercises and what do you feel most proud of?What have you learned about life that you would
want to pass on to others?5 Meaning and attitudinal values: Since your diagnosis, have you felt a sense of a loss
limitations, finiteness of life of meaning in life? That life is not worth living?”Thoughts about what are a “good” or “meaningful”
death.Thoughts about what happens after death?
6 Meaning derived from creative What are your responsibilities?values and responsibility What are the tasks you have for your life?
Who are you responsible to and for?What is your unfinished business?
7 Meaning and experiential values: List and discuss three things that strike you as beautifulnature, art, beauty, humor and still make you feel alive.
List three things that still make you laugh8 Review and termination Review of memoirs, legacy project
Review sources of meaningHopes for future—list three hopes for the futureSaying good-bye
Adapted from Breitbart W: Spirituality and meaning in supportive care: Spirituality- and meaning-centered grouppsychotherapy interventions in advanced cancer. Support Care Cancer 2002;10:272–280.

adjustment and symptom control in a generaladult cancer population. A small qualitativestudy of adjuvant psychological therapy that ad-dresses both basic coping issues and spiritualconcerns and healing using a combination ofgroup exploration, meditation, prayer, and otherspiritually oriented exercises164 suggested a pos-itive relationship to survival in patients with metastatic cancers. On the other hand, a trial ofstandard supportive-expressive therapy (encour-aging expression of emotions about various as-pects of life, including spiritual concerns) failedto improve health-related quality of life.165 A smallstudy of religious patients with grief and be-reavement demonstrated faster recovery when areligious psychotherapy was added to a cogni-tive-behavioral approach.52
Two novel approaches166,167 to therapy havebeen recently described: meaning centered anddignity psychotherapies. Awaiting more rigorousevaluation, they represent an excellent source ofvaluable techniques of support and counselingwhich the members of the interdisciplinary teamcan facilitate.
Meaning Centered Psychotherapy. An ongoingtrial168 is exploring the feasibility and efficacyof this new and unique psychotherapy inter-vention for advanced cancer patients. It aims atenhancing psychological and spiritual well-be-ing and quality of life while comparing it to astandard supportive group psychotherapy. This8-week long process (one session per week) uti-lizing a profound, emotional experiential exer-cise centers on learning about experiences re-lated to meaning. Each session combinesdidactic and conceptual elements with one ortwo experiential exercises that illustrate the con-cepts (Table 12).
Dignity Psychotherapy. Dignity refers to thesense of esteem and worth inalienable from thevery being of an individual.169 Patients at the endof life whose personal psychological, spiritual,and physical needs are successfully met may besaid to have achieved a sense of dignity.170,171 Un-fortunately, the idiomatic usage of this term isfraught with a broad range of connotations lead-ing to conflicting interpretations.
OKON408
TABLE 13. DIGNITY PSYCHOTHERAPY QUESTIONS
Can you tell me a little about your life history, particularly those parts that you either remember most or thinkare the most important?
When did you feel most alive?
Are there specific things that you would want your family to know about you, and are there particular thingsyou would want them to remember?
What are the most important roles (e.g., family, vocational, community service) you have played in life?
Why are they so important to you, and what do you think you accomplished in those roles?
What are your most important accomplishments, and what do you feel most proud of?
Are there particular things that you feel still need to be said to your loved ones, or things that you would wantto take the time to say once again?
What are your hopes and dreams for your loved ones?
What have you learned about life that you would want to pass along to others?
What advice or words of guidance would you wish to pass along to your (son, daugther, husband, wife,parent, other[s])?
Are there words or perhaps even instructions you would like to offer your family, in order to provide them withcomfort or solace?
In creating this permanent record, are there otherthings that you would like included?
Reprinted with permission from Chochinov HM: Dignity-conserving care—A new model for palliative care: Help-ing the patient feel valued. JAMA 2002;287:2253–2260.

Contradictory goals of care, including on theone hand meticulous care and preservation of life,and euthanasia on the other63,172 might be bothderived from and claimed to foster dignity. Ac-cording to one model, this terminological confu-sion might be resolved, however, if one accountsfor differences between the intrinsic and attrib-uted dignities of a person.173 Intrinsic dignityrefers to the value one has simply because one ishuman, a member of the only species we knowthat is capable of love, rationality, moral discern-ment and agency, as well as the sense of beautyand creativity. Attributed dignity refers to othernecessary conditions and components of humanflourishing and excellence. Because attributeddignities presuppose the intrinsic dignity ac-cording to this model, physicians are counseledagainst euthanasia or physician-assisted suicideas this undermines the fundamentally necessary(i.e., intrinsic dignity of a person). Recently at-tempts have been made to focus an integratedprocess of palliative care on conserving dignity.
Spiritual comfort is prominently included inone comprehensive, empirically derived model ofdignity-conserving palliative care.171 The modelexplicitly acknowledges that fostering connec-tions with religious communities and expressionof spiritual/religious beliefs may facilitate thespiritual comfort.46,171 Patients enrolled in dig-nity psychotherapy are asked to record variousaspects of life they would most want remem-bered. They respond to a series of questions(Table 13) which focus on things they feel aremost important and that they would most wanttheir loved one(s) to remember. The recordedtape is transcribed, edited, and given back to thepatients. This intervention can engender a senseof legacy, coherence, enhanced identity, and emo-tional reconciliation.171
CONCLUSIONS
Life-threatening illness opens immense chal-lenges in the lives of patients and their families.When facing death, our patients turn to the mostfundamental values and practices; they trust in-tuitions that allow them to transform tragedy into possibilities for growth and peace. No singlepredetermined scheme of communication can besufficient to learn the truth of pain despair, ortransformation. Nevertheless, we remain profes-sionally and morally obliged to recognize, ad-
dress and study transcendent concerns as theyare bound to remain ours and our patients’ com-panions in the times of health and illness.
ACKNOWLEDGMENTS
The author thanks Marshfield Clinic ResearchFoundation and Marshfield Clinic for its supportthrough the assistance of Linda Weis, Alice Star-gardt, Graig Eldred, and Barb Bartkowiak in thepreparation of this manuscript and Dan Sulmasyfor his helpful remarks on the notion of dignity.
REFERENCES
1. Sulmasy DP: Is medicine a spiritual practice? AcadMed 1999;74:1002–1005.
2. Puchalski CM, Larson DB, Post SG: Physicians andpatient spirituality. Ann Intern Med 2000;133:748–749.
3. McSherry W, Cash K: The language of spirituality:An emerging taxonomy. Int J Nurs Stud 2004;41:151–161.
4. Heidegger M, Stambaugh J (trans), Stanbaugh J (trans:Being and Time: A Translation of Sein and Zeit (SUNY se-ries in Contemporary Continental Philosophy). Albany,NY: State University of New York Press, 1996.
5. O’Connell LJ: Religious dimensions of dying anddeath. West J Med 1995;163:231–235.
6. Pickstock C: After Writing: On the Liturgical Consum-mation of Philosophy (Challenges in Contemporary The-ology). Malden, MA: Blackwell Publishers, 1997.
7. Hill PC, Pargament KI, Hood RW, McCullough ME,Swyers JP, Larson DB, Zinnbauer BJ: Conceptualiz-ing religion and spirituality: Points of commonality,points of departure. J Theory Soc Beh 2000;30:51–77.
8. Pargament KI: The psychology of religion and spir-ituality? Yes and no. Int J Psychol Relig 1999;9:3–16.
9. Marler PL, Hadaway CK: “Being religious” or “be-ing spiritual” in America: A zero-sum proposition?J Sci Stud Rel 2002;41:289–300.
10. Zinnbauer BJ, Pargament KI, Cole BC, Rye MS, But-ter EM, Belavich TG, Hipp KM, Scott AB, Kadar JL:Religion and spirituality: Unfuzzying the fuzzy. J SciStud Rel 1997;36:549–564.
11. Bradshaw A: The spiritual dimension of hospice: Thesecularization of an ideal. Soc Sci Med 1996;43:409–419.
12. Foucault M: Discipline and Punish: The Birth of theModern Prison. New York, NY: Pantheon Books,1977.
13. Gallup G, Lindsay DM: Surveying the Religious Land-scape: Trends in U.S. Beliefs. Harrisburg, PA: More-house Publishing, 1999.
14. Gallup G: Religion in America, 50 years: 1935–1985.Princeton, NJ: Princeton Religious Research, 1985.
15. Myers DG: The American Paradox: Spiritual Hunger in
SPIRITUAL, RELIGIOUS, AND EXISTENTIAL ASPECTS 409
an Age of Plenty. New Haven, CT: Yale UniversityPress, 2000.
16. Shahabi L, Powell LH, Musick MA, Pargament KI,Thoresen CE, Williams D: Correlates of self-percep-tions of spirituality in American adults. Ann BehavMed 2002;24:59–68.
17. Koenig HG: Religious beliefs and practices of hos-pitalized medically ill older adults. Int J Geriatr Psy-chiatry 1998;13:213–224.
18. Roberts JA, Brown D, Elkins T, Larson DB: Factorsinfluencing the views of patients with gynecologiccancer about end-of-life decisions. Am J Obstet Gy-necol 1997;176:166–172.
19. VandeCreek L, Rogers E, Lester J: Use of alternativetherapies among breast cancer outpatients comparedwith the general population. Altern Ther HealthMed 1999;5:71–76.
20. Daaleman TP, Frey B: Spiritual and religious beliefsand practices of family physicians: A national sur-vey. J Fam Pract 1999;48:98–104.
21. Bergin AE, Jensen JP: Religiosity of psychothera-pists: A national survey. Psychotherapy 1990;27:3–7.
22. McCarthy MK, Peteet JR: Teaching residents aboutreligion and spirituality. Harv Rev Psychiatry 2003;11:225–228.
23. Fitchett G, Burton LA, Sivan AB: The religious needsand resources of psychiatric patients. J Nerv MentalDis 1997;185:320–326.
24. Fitchett G, Meyer PM, Burton LA: Spiritual care inthe hospital: Who requests it? Who needs it? J Pas-toral Care 2000;54:173–186.
25. Milberg A, Strang P, Jakobsson M: Next of kin’s experience of powerlessness and helplessness in palliative home care. Support Care Cancer 2004;12:120–128.
26. Daaleman TP, Nease DE: Patient attitudes regardingphysician inquiry into spiritual and religious issues.J Fam Pract 1994;39:564–568.
27. Ehman JW, Ott BB, Short TH, Ciampa RC, Hansen-Flaschen J: Do patients want physicians to inquireabout their spiritual or religious beliefs if they be-come gravely ill? Arch Intern Med 1999;159:1803–1806.
28. Anderson JM, Anderson LJ, Felsenthal G: Pastoralneeds and support within an inpatient rehabilitationunit. Arch Phys Med Rehabil 1993;74:574–578.
29. King DE, Bushwick B: Beliefs and attitudes of hos-pital inpatients about faith healing and prayer. J FamPract 1994;39:349–352.
30. Oyama O, Koenig HG: Religious beliefs and practicesin family medicine. Arch Fam Med 1998;7:431–435.
31. Moadel A, Morgan C, Fatone A, Grennan J, CarterJ, Laruffa G, Skummy A, Dutcher J: Seeking mean-ing and hope: Self-reported spiritual and existentialneeds among an ethnically-diverse cancer patientpopulation. Psychooncology 1999;8:378–385.
32. Hebert RS, Jenckes MW, Ford DE, O’Connor DR,Cooper LA: Patient perspectives on spirituality andthe patient-physician relationship. J Gen Intern Med2001;16:685–692.
33. Sulmasy DP: A biopsychosocial-spiritual model forthe care of patients at the end of life. Gerontologist2002;42 (Spec No 3):24–33.
34. McClain CS, Rosenfeld B, Breitbart W: Effect of spir-itual well-being on end-of-life despair in terminally-ill cancer patients. Lancet 2003;361:1603–1607.
35. Nelson CJ, Rosenfeld B, Breitbart W, Galietta M:Spirituality, religion, and depression in the termi-nally ill. Psychosomatics 2002;43:213–220.
36. Peterman AH, Fitchett G, Brady MJ, Hernandez L,Cella D: Measuring spiritual well-being in peoplewith cancer: The functional assessment of chronic ill-ness therapy—Spiritual Well-being Scale (FACIT-Sp). Ann Behav Med 2002;24:49–58.
37. Ganzini L, Johnston WS, McFarland BH, Tolle SW,Lee MA: Attitudes of patients with amyotrophic lat-eral sclerosis and their care givers toward assistedsuicide. N Engl J Med 1998;339:967–973.
38. Cohen SR, Mount BM, Bruera E, Provost M, Rowe J,Tong K: Validity of the McGill Quality of Life Ques-tionnaire in the palliative care setting: A multi-cen-tre Canadian study demonstrating the importance ofthe existential domain. Palliat Med 1997;11:3–20.
39. Brady MJ, Peterman AH, Fitchett G, Mo M, Cella D:A case for including spirituality in quality of lifemeasurement in oncology. Psychooncology 1999;8:417–428.
40. Costantini M, Mencaglia E, Giulio PD, Cortesi E, RoilaF, Ballatori E, Tamburini M, Casali P, Licitra L, Can-dis DD, Massidda B, Luzzani M, Campora E, PlacidoSD, Palmeri S, Angela PM, Baracco G, Gareri R, Mar-tignetti A, Ragosa S, Zoda L, Ionta MT, Bulletti S, Pa-store L: Cancer patients as ‘experts’ in defining qual-ity of life domains. A multicentre survey by the ItalianGroup for the Evaluation of Outcomes in Oncology(IGEO). Qual Life Res 2000;9:151–159.
41. Hermann CP: Spiritual needs of dying patients: Aqualitative study. Oncol Nurs Forum 2001;28:67–72.
42. Cohen SR, Mount BM, Tomas JJ, Mount LF: Exis-tential well-being is an important determinant ofquality of life. Evidence from the McGill Quality ofLife Questionnaire. Cancer 1996;77:576–586.
43. Targ EF, Levine EG: The efficacy of a mind-body-spirit group for women with breast cancer: A ran-domized controlled trial. Gen Hosp Psychiatry 2002;24:238–248.
44. Feher S, Maly C: Coping with breast cancer in laterlife: The role of religious faith. Psychooncology1999;8:408–416.
45. Koenig HG, Pargament KI, Nielsen J: Religious cop-ing and health status in medically ill hospitalizedolder adults. J Nerv Ment Dis 1998;186:513–521.
46. Holland JC, Passik S, Kash KM, Russak SM, GronertMK, Sison A, Lederberg M, Fox B, Baider L: The roleof religious and spiritual beliefs in coping with ma-lignant melanoma. Psychooncology 1999;8:14–26.
47. Raleigh ED: Sources of hope in chronic illness. On-col Nurs Forum 1992;19:443–448.
48. Halstead MT, Fernsler JI: Coping strategies of long-term cancer survivors. Cancer Nurs 1994;17:94–100.
OKON410

49. Smith TB, McCullough ME, Poll J: Religiousness anddepression: Evidence for a main effect and the mod-erating influence of stressful life events. Psychol Bull2003;129:614–636.
50. Carpenter JS, Brockopp DY, Andrykowski MA: Self-transformation as a factor in the self-esteem andwell-being of breast cancer survivors. J Adv Nurs1999;29:1402–1411.
51. Burgener SC: Predicting quality of life in caregiversof Alzheimer’s patients: The role of support fromand involvement with the religious community. JPastoral Care 1999;53:433–446.
52. Azhar MZ, Varma SL: Religious psychotherapy asmanagement of bereavement. Acta Psychiatr Scand1995;91:233–235.
53. Grodin MA: Religious advance directives: The con-vergence of law, religion, medicine, and public health.Am J Public Health 1993;83:899–903.
54. Silvestri GA, Knittig S, Zoller JS, Nietert PJ: Impor-tance of faith on medical decisions regarding cancercare. J Clin Oncol 2003;21:1379–1382.
55. Johnson SC, Spilka B: Coping with breast cancer: The roles of clergy and faith. J Relig Health 1991;30:21–33.
56. Baider L, Russak SM, Perry S, Kask K, Gronert M,Fox B, Holland J, Kaplan-Denour A: The role of re-ligious and spiritual beliefs in coping with malignantmelanoma: An Israeli sample. Psychooncology 1999;8:27–35.
57. Dorff E: A Jewish approach to end-stage medicalcare. Conserv Jud 1990;43:3–51.
58. General Assembly of Unitarian Universalists: TheRight to Die with Dignity: Proceedings of General As-sembly. Boston, MA: Unitarian Universalist Associa-tion, 1988.
59. National Conference of Catholic Bishops: Ethical andReligious Directives for Catholic Health Care Services.Washington, D.C.: United States Catholic Confer-ence, 1994
60. Dubose ER: Physician Assisted Suicide: Religious andPublic Policy Perspectives. Chicago, IL: Park RidgeCenter, 1999.
61. Portenoy RK, Coyle N, Kash KM, Brescia F, ScanlonC, O’Hare D, Misbin RI, Holland J, Foley KM: De-terminants of the willingness to endorse assisted sui-cide. A survey of physicians, nurses, and socialworkers. Psychosomatics 1997;38:277–287.
62. Emanuel EJ, Daniels ER, Fairclough DL, ClarridgeBR: The practice of euthanasia and physician-as-sisted suicide in the United States: Adherence to pro-posed safeguards and effects on physicians. JAMA1998;280:507–513.
63. Meier DE, Emmons CA, Wallenstein S, Quill T, Mor-rison RS, Cassel CK: A national survey of physician-assisted suicide and euthanasia in the United States.N Engl J Med 1998;338:1193–1201.
64. Powell LH, Shahabi L, Thoresen CE: Religion andspirituality. Linkages to physical health. Am Psychol2003;58:36–52.
65. Strawbridge WJ, Cohen RD, Shema SJ, Kaplan GA:
Frequent attendance at religious services and mor-tality over 28 years. Am J Public Health 1997;87:957–961.
66. Helm HM, Hays JC, Flint EP, Koenig HG, Blazer DG:Does private religious activity prolong survival? Asix-year follow-up study of 3,851 older adults. JGerontol A Biol Sci Med Sci 2000;55:M400–405.
67. Seeman TE, Dubin LF, Seeman M: Religiosity/spir-ituality and health. A critical review of the evidencefor biological pathways. Am Psychol 2003;58:53–63.
68. McCullough ME, Hoyt WT, Larson DB, Koenig HG,Thoresen C: Religious involvement and mortality: A meta-analytic review. Health Psychol 2000;19:211–222.
69. George LK, Ellison CG, Larson DB: Exploring the relationships between religious involvement andhealth. Psychol Inquiry 2002;13:190–200.
70. Koenig HG, McCullough ME, Larson DB: Handbookof Religion and Health. New York: Oxford UniversityPress, 2001.
71. Seybold KS, Hill PC: The role of religion and spiri-tuality in mental and physical health. Curr Dir Psy-chol Sci 2001;10:21–24.
72. Thoresen CE: Spirituality and health: Is there a rela-tionship? J Health Psychol 1999;4:291–300.
73. Lo B, Quill T, Tulsky J: Discussing palliative carewith patients. ACP-ASIM End-of-Life Care Consen-sus Panel. American College of Physicians-AmericanSociety of Internal Medicine. Ann Intern Med1999;130:744–749.
74. Wheeler HB: Shattuck lecture—Healing and hero-ism. N Engl J Med 1990;322:1540–1548.
75. Byock IR: Conceptual models and the outcomes ofcaring. J Pain Symptom Manage 1999;17:83–92.
76. Curtis JR, Wenrich MD, Carline JD, Shannon SE,Ambrozy DM, Ramsey PG: Understanding physi-cians’ skills at providing end-of-life care: Perspec-tives of patients, families, and health care workers.J Gen Intern Med 2001;16:41–49.
77. Cassel CK, Foley KM: Principles for Care of Patients atthe End of Life: An Emerging Consensus Among the Spe-cialties of Medicine. New York: Millbank MemorialFund, 1999. �www.milbank.org/endoflife/� (Last ac-cessed May 24, 2004).
78. Thomason CL, Brody H: Inclusive spirituality. J FamPract 1999;48:96–97.
79. Emanuel EJ, Emanuel LL: The promise of a gooddeath. Lancet 1998;351:SII21–29.
80. Field MJ, Cassel CK (ed): Approaching Death: Im-proving Care at the End-of-Life. Washington, D.C.: Na-tional Academy Press, 1997. �www.nap.edu/books/0309063728/html/index.html� (Last accessed on May24, 2004).
81. Committee on Quality of Health Care in America,Institute of Medicine: Crossing the Quality Chasm: ANew Health System for the 21st Century. Washington,D.C.: National Academy Press, 2001. �www.nap.edu/books/0309072808/html/� (Last accessed May24, 2004).
82. Steinhauser KE, Christakis NA, Clipp EC, McNeilly
SPIRITUAL, RELIGIOUS, AND EXISTENTIAL ASPECTS 411
M, McIntyre L, Tulsky JA: Factors considered im-portant at the end-of-life by patients, family, physi-cians, and other care providers. JAMA 2000;284:2476–2482.
83. Steinhauser KE, Clipp EC, McNeilly M, ChristakisNA, McIntyre LM, Tulsky JA: In search of a gooddeath: Observations of patients, families, andproviders. Ann Intern Med 2000;132:825–832.
84. Cartwright A: Is religion a help around the time ofdeath? Public Health 1991;105:79–87.
85. Delbanco TL: Enriching the doctor-patient relation-ship by inviting the patient’s perspective. Ann In-tern Med 1992;116:414–418.
86. McBride JL, Arthur G, Brooks R, Pilkington L: Therelationship between a patient’s spirituality andhealth experiences. Fam Med 1998;30:122–126.
87. Hamilton DG: Believing in patients’ beliefs: Physi-cian attunement to the spiritual dimension as a pos-itive factor in patient healing and health. Am J HospPalliat Care 1998;15:276–279.
88. Association of American Medical Colleges: Report I:Learning objectives for medical school education:Guidelines for medical schools. Washington, D.C.:Association of American Medical Colleges, 1998.�www.aamc.org/meded/msop/msop1.pdf� (Lastaccessed on May 24, 2004).
89. American Medical Association: Graduate Medical Ed-ucation Directory 1995–1996. Chicago, IL: AmericanMedical Association, 1995.
90. The World Health Organization Quality of Life as-sessment (WHOQOL): Position Paper from theWorld Health Organization. Soc Sci Med 1995;41:1403–1409.
91. Joint Commission on Accreditation of HealthcareOrganization: CAMH Refreshed Core. January, RI1,1998.
92. National Consensus Project for Quality PalliativeCare: Clinical Practice Guidelines for Quality Pallia-tive Care. �nationalconsensusproject.org� (Last ac-cessed May 24, 2004).
93. Ellis MR, Vinson DC, Ewigman B: Addressing spir-itual concerns of patients: Family physicians’ atti-tudes and practices. J Fam Pract 1999;48:105–109.
94. Kristeller JL, Zumbrun CS, Schilling RF: “I would ifI could”: How oncologists and oncology nurses ad-dress spiritual distress in cancer patients. Psychoon-cology 1999;8:451–458.
95. Sulmasy DP, Geller G, Levine DM, Faden R: Thequality of mercy: Caring for patients with ‘do not re-suscitate’ orders. JAMA 1992;267:682–686.
96. Maugans TA, Wadland WC: Religion and familymedicine: A survey of physicians and patients. J FamPract 1991;32:210–213.
97. Sloan RP, Bagiella E, VandeCreek L, Hover M, Casa-lone C, Jinpu Hirsch T, Hasan Y, Kreger R, PoulosP: Should physicians prescribe religious activities?N Engl J Med 2000;342:1913–1916.
98. Thiel MM, Robinson MR: Physicians’ collaborationwith chaplains: Difficulties and benefits. J Clin Ethics1997;8:94–103.
99. Post SG, Puchalski CM, Larson DB: Physicians andpatient spirituality: Professional boundaries, com-petency, and ethics. Ann Intern Med 2000;132:578–583.
100. Larson DB, Hohmann AA, Kessler LG, Meador KG,Boyd JH, McSherry E: The couch and the cloth: Theneed for linkage. Hosp Community Psychiatry 1988;39:1064–1069.
101. Larson DB: Are religion and spirituality clinicallyrelevant in health care? Mind Body Med 1995;1:147–157.
102. Graner J: Physicians and patient spirituality. Ann In-tern Med 2000;133:748–749.
103. Hill PC, Pargament KI: Advances in the conceptual-ization and measurement of religion and spiritual-ity. Implications for physical and mental health re-search. Am Psychol 2003;58:64–74.
104. Saint Augustine: Soliloquies and Immortality of theSoul. Warminster, England: Aris & Phillips, 1990.
105. Hall TW, Edwards KJ: The initial development andfactor analysis of the spiritual assessment inventory.J Psychol Theol 1996;24:233–246.
106. Hall TW, Edwards KJ: The Spiritual Assessment In-ventory: A theistic model and measure for assessingspiritual development. J Sci Study Relig 2002;41:341–357.
107. Kirkpatrick LA: Attachment theory and religious ex-perience. In: Hood RW Jr. (ed): Handbook of ReligiousExperience. Birmingham, AL: Religious EducationPress, 1995, pp. 446–475.
108. Milbank J: The Word Made Strange: Theology, Lan-guage, Culture. Cambridge, MA: Blackwell Publish-ers, 1997.
109. Eliade M: The Sacred and the Profane: The Nature of Re-ligion. New York: Harcourt Brace Jovanovich, 1959.
110. Emmons RA, Cheung C, Tehrani K: Assessing spir-ituality through personal goals: Implications for re-search on religion and subjective well-being. Soc In-dic Res 1998;45:391–422.
111. Tarakeshwar N, Swank AB, Pargament KI, MahoneyA: The sanctification of nature and theological con-servatism: A study of opposing correlates of envi-ronmentalism. Rev Relig Res 2001;42:387–404.
112. Pargament KI, Olsen H, Reilly B, Falgout K, EnsingDS, Van Haitsma K: God help me (II): The relation-ship of religious orientations to religious coping with negative life events. J Sci Study Relig 1992;31:504–513.
113. Pargament KI, Koenig HG, Perez LM: The manymethods of religious coping: Development and ini-tial validation of the RCOPE. J Clin Psychol 2000;56:519–543.
114. Rabins PV, Fitting MD, Eastham J, Zabora J: Emo-tional adaptation over time in caregivers for chron-ically ill elderly people. Age Ageing 1990;19:185–190.
115. Gorsuch RL, Venable GD: Development of an “ageuniversal” I-E scale. J Sci Stud Relig 1983;22:181–187.
116. Ryan RM, Rigby S, King K: Two types of religiousinternalization and their relations to religious orien-
OKON412
tations and mental health. J Pers Soc Psychol 1993;65:586–596.
117. VandeCreek L, Ayres S, Bassham M: Using IN-SPIRIT to conduct spiritual assessments. J PastoralCare 1995;49:83–89.
118. Underwood LG, Teresi JA: The daily spiritual expe-rience scale: Development, theoretical description,reliability, exploratory factor analysis, and prelimi-nary construct validity using health-related data.Ann Behav Med 2002;24:22–33.
119. Fiala WE, Bjorck JP, Gorsuch RL: The ReligiousSupport Scale: Construction, validation, and cross-validation. Am J Community Psychol 2002;30:761–786.
120. Krause N: Religious support. In: Fetzer Institute/National Institute on Aging Working Group (ed):Multidimensional Measurement of Religiousness/Spiri-tuality for Use in Health Research: A Report of the Fet-zer Institute/National Institute on Aging WorkingGroup. Kalamazoo, MI: Fetzer Institute, 1999, pp.57–64.
121. VandeCreek L, Pargament K, Belavich T, Cowell B,Friedel L: The unique benefits of religious supportduring cardiac bypass surgery. J Pastoral Care 1999;53:19–29.
122. Taylor RJ, Chatters LM: Church members as a sourceof informal social support. Rev Relig Res 1988;30:193–203.
123. Taylor EJ, Outlaw FH, Bernardo TR, Roy A: Spiri-tual conflicts associated with praying about cancer.Psychooncology 1999;8:386–394.
124. Batson CD, Schoenrade P, Ventis WL: Religion andthe Individual: A Social-Psychological Perspective. NewYork: Oxford University Press, 1993.
125. Calhoun LG, Cann A, Tedeschi RG, McMillan J: Acorrelational test of the relationship between post-traumatic growth, religion, and cognitive process-ing. J Trauma Stress 2000;13:521–527.
126. Ventis WL: The relationships between religion andmental health. J Social Issues 1995;51:33–48.
127. Pascal B: Prière pour demander à Dieu le bon usagedes maladies. In: L’Oeuvre de Pascal (Bibliothèque de laPléiade). Paris: Gallimard, 1950.
128. Piper J: The Misery of Job and the Mercy of God.Wheaton, IL: Crossway Books, 2002.
129. Franks K, Templer DI, Cappelletty GG, Kauffman I:Exploration of death anxiety as a function of reli-gious variables in gay men with and without AIDS.Omega 1990–1991;22:43–50.
130. Exline JJ, Yali AM, Sanderson WC: Guilt, discord,and alienation: The role of religious strain in de-pression and suicidality. J Clin Psychol 2000;56:1481–1496.
131. Hays JC, Meador KG, Branch PS, George LK: The Spir-itual History Scale in four dimensions (SHS-4): Valid-ity and reliability. Gerontologist 2001;41:239–249.
132. Fitchett G, Rybarczyk BD, DeMarco GA, Nicholas JJ:The role of religion in medical rehabilitation out-comes: A longitudinal study. Rehabil Psychol 1999;44:333–353.
133. Pargament KI, Koenig HG, Tarakeshwar N, Hahn J:Religious struggle as a predictor of mortality amongmedically ill elderly patients: A two-year longitudi-nal study. Arch Intern Med 2001;161:1881–1885.
134. Berg GE, Fonss N, Reed AJ, VandeCreek L: The im-pact of religious faith and practice on patients suf-fering from a major affective disorder: A cost anal-ysis. J Pastoral Care 1995;49:359–363.
135. Hill PC, Hood RW: Measures of Religiosity. Birming-ham, AL: Religious Education Press, 1999.
136. Fetzer Institute/National Institute on Aging Work-ing Group: Multidimensional Measurement of Reli-giousness/Spirituality for Use in Health Research: A Report of the Fetzer Institute/National Institute on Ag-ing Working Group. Kalamazoo, MI: Fetzer Institute,1999. �www.fetzer.org/resources/FETZER_BOOK.pdf� (Last accessed May 24, 2004).
137. Pellegrino ED: The internal morality of clinicalmedicine: A paradigm for the ethics of the helpingand healing professions. J Med Philos 2001;26:559–579.
138. Brody H: “My story is broken: Can you help me fixit?” Medical ethics and the joint construction of nar-rative. Lit Med 1994;13:79–92.
139. Haidet P, Paterniti DA: “Building” a history ratherthan “taking” one: A perspective on informationsharing during the medical interview. Arch InternMed 2003;163:1134–1140.
140. Wittgenstein L: Tractatus Logico-Philosophicus (Rout-ledge Classics). London: Routledge, 2001.
141. Okon TR, Gomez CF: Patient evaluation in palliativecare. In: Rose BD (ed): UpToDate. Wellesley, MA,2002–2003. �www.uptodate.com� (Last accessed May2, 2003).
142. Romer A: Taking a Spiritual History Allows Clini-cians to Understand Patients More Fully: An Inter-view with Dr. Christina Puchalski. Spirituality andEnd-of-Life Care 1999;1. �www2.edc.org/lastacts/archives/archivesNov99/featureinn.asp� (Last ac-cessed March 30, 2004).
143. Taylor EJ, Outlaw FH: Use of prayer among personswith cancer. Holist Nurs Pract 2002;16:46–60.
144. Strang S, Strang P: Questions posed to hospital chap-lains by palliative care patients. J Palliat Med 2002;5:857–864.
145. Fitchett G: Screening for spiritual risk. ChaplaincyToday 1999;15:2–12.
146. Fitchett G: Selected resources for screening for spir-itual risk. Chaplaincy Today 1999;15:13–26.
147. Pargament KI, Zinnbauer BJ, Scott AB, Butter EM,Zerowin J, Stanik P: Red flags and religious coping:Identifying some religious warning signs amongpeople in crisis. J Clin Psychol 1998;54:77–89.
148. Brett AS, Jersild P: “Inappropriate” treatment nearthe end of life: Conflict between religious convictionsand clinical judgment. Arch Intern Med 2003;163:1645–1649.
149. Dagi TF: Prayer, piety, and professional propriety:Limits on religious expression in hospitals. J ClinEthics 1995;6:274–279.
SPIRITUAL, RELIGIOUS, AND EXISTENTIAL ASPECTS 413

150. Lo B, Kates LW, Ruston D, Arnold RM, Cohen CB,Puchalski CM, Pantilat SZ, Rabow MW, SchreiberRS, Tulsky JA: Responding to requests regardingprayer and religious ceremonies by patients near theend of life and their families. J Palliat Med 2003;6:409–415.
151. Lo B, Ruston D, Kates LW, Arnold RM, Cohen CB,Faber-Langendoen K, Pantilat SZ, Puchalski CM,Quill TR, Rabow MW, Schreiber S, Sulmasy DP, Tul-sky JA, Working Group on Religious and SpiritualIssues at the End of Life: Discussing religious andspiritual issues at the end of life: A practical guidefor physicians. JAMA 2002;287:749–754.
152. Osler W: A Way of Life, and Selected Writings of SirWilliam Osler, 12 July 1849 to 29 December 1919.Franklin AW (ed): New York, NY: Dover Publica-tions, 1951, pp. 237–249.
153. Cabot RC, Dicks RL: The Art of Ministering to the Sick.New York: MacMillan, 1936.
154. Handzo G: Where do chaplains fit in the world ofcancer care? J Health Care Chaplain 1992;4:29–44.
155. Daaleman TP, Frey B: Prevalence and patterns ofphysician referral to clergy and pastoral careproviders. Arch Fam Med 1998;7:548–553.
156. The HealthCare Chaplaincy. Providing passionatespiritual care to people of all faiths. �www.health-carechaplaincy.org� (Last accessed April 24, 2004).
157. Cole B, Pargament K: Re-creating your life: A spiri-tual/psychotherapeutic intervention for people di-agnosed with cancer. Psychooncology 1999;8:395–407.
158. Coward DD: Facilitation of self-transcendence in abreast cancer support group: II. Oncol Nurs Forum2003;30:291–300.
159. Breitbart W: MCP pilot results. Presented at theAmerican Academy of Hospice and Palliative Med-icine Meeting, Phoenix, AZ; January 2004.
160. Goodwin PJ, Leszcz M, Ennis M, Koopmans J, Vin-cent L, Guther H, Drysdale E, Hundleby M, Chochi-nov HM, Navarro M, Speca M, Hunter J: The effectof group psychosocial support on survival in meta-static breast cancer. N Engl J Med 2001;345:1719–1726.
161. Edelman S, Bell DR, Kidman AD: A group cognitivebehaviour therapy programme with metastatic breastcancer patients. Psychooncology 1999;8:295–305.
162. Classen C, Butler LD, Koopman C, Miller E, DiM-iceli S, Giese-Davis J, Fobair P, Carlson RW, Krae-mer HC, Spiegel D: Supportive-expressive grouptherapy and distress in patients with metastaticbreast cancer: A randomized clinical interventiontrial. Arch Gen Psychiatry 2001;58:494–501.
163. Meyer TJ, Mark MM: Effects of psychosocial inter-
ventions with adult cancer patients: A meta-analy-sis of randomized experiments. Health Psychol 1995;14:101–108.
164. Cunningham AJ, Edmonds CV, Phillips C, Soots KI,Hedley D, Lockwood GA: A prospective, longitudi-nal study of the relationship of psychological workto duration of survival in patients with metastaticcancer. Psychooncology 2000;9:323–339.
165. Bordeleau L, Szalai JP, Ennis M, Leszcz M, Speca M,Sela R, Doll R, Chochinov HM, Navarro M, ArnoldA, Pritchard KI, Bezjak A, Llewellyn-Thomas HA,Sawka CA, Goodwin PJ: Quality of life in a ran-domized trial of group psychosocial support in met-astatic breast cancer: Overall effects of the interven-tion and an exploration of missing data. J Clin Oncol2003;21:1944–1951.
166. Breitbart W: Spirituality and meaning in supportivecare: Spirituality- and meaning-centered group psy-chotherapy interventions in advanced cancer. Sup-port Care Cancer 2002;10:272–280.
167. Chochinov HM, Hack T, McClement S, KristjansonL, Harlos M: Dignity in the terminally ill: A devel-oping empirical model. Soc Sci Med 2002;54:433–443.
168. National Center for Complementary and AlternativeMedicine. Meaning-centered psychotherapy in ad-vanced cancer. �clinicaltrials.gov/show/NCT00067288� (Last accessed April 8, 2004).
169. Pullman D: Human dignity and the ethics and aes-thetics of pain and suffering. Theor Med Bioeth 2002;23:75–94.
170. Madan TN: Dying with dignity. Soc Sci Med 1992;35:425–432.
171. Chochinov HM: Dignity-conserving care—A newmodel for palliative care: Helping the patient feelvalued. JAMA 2002;287:2253–2260.
172. Chin AE, Hedberg K, Higginson GK, Fleming DW:Legalized physician-assisted suicide in Oregon—The first year’s experience. N Engl J Med 1999;340:577–583.
173. Sulmasy DP: Death, dignity, and the theory of value.Ethical Perspect 2002;9:103–118.
Address reprint requests to:Tomasz R. Okon, M.D.
Department of Palliative MedicineMarshfield Clinic
1000 North Oak AvenueMarshfield, WI 54449
E-mail: [email protected]
OKON414