sotiris antoniou consultant pharmacist, cardiovascular ... · new oral anticoagulants sotiris...
TRANSCRIPT
New Oral Anticoagulants
Sotiris Antoniou
Consultant Pharmacist, Cardiovascular Medicine
Barts and the London NHS Trust &
North East London Cardiovascular & Stroke Network
Contents
� Warfarin - summary
� Concerns
� Time In Range (TIR)
� Newer anticoagulants – the evidence base!
� Dabigatran
� Rivaroxaban (not yet published)
� Apixaban
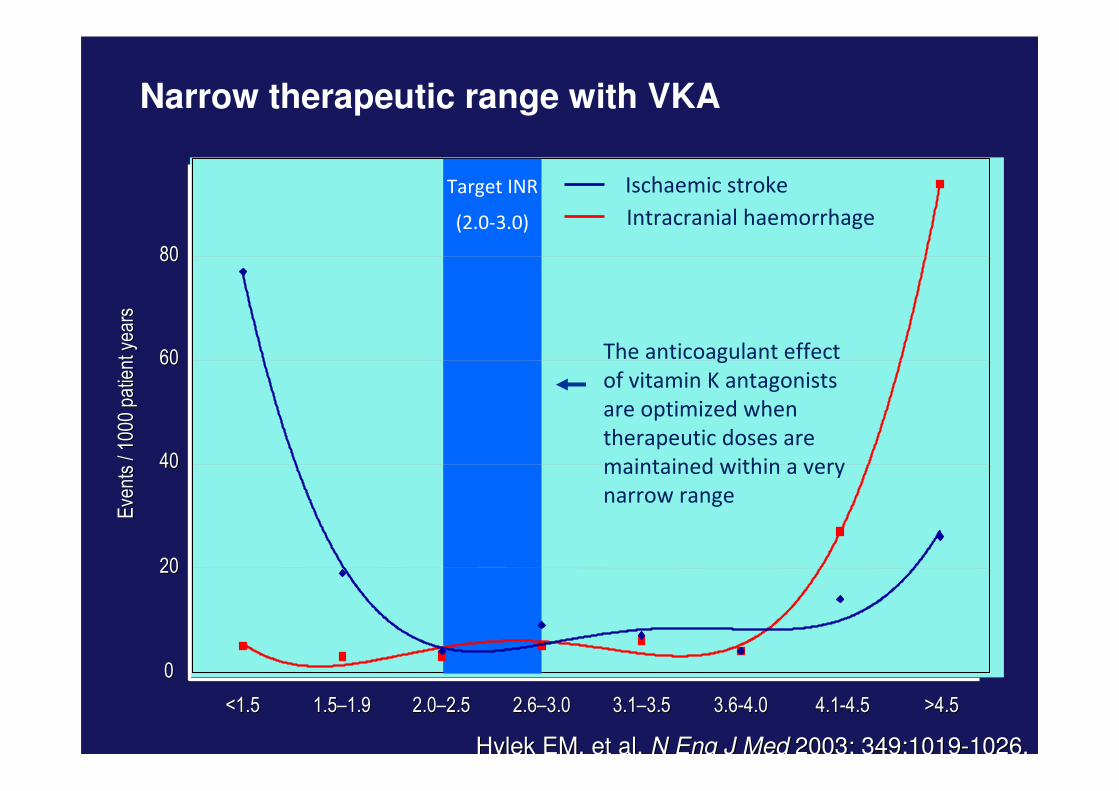
Narrow therapeutic range with VKA
Target INR
(2.0-3.0)
00
2020
4040
6060
8080
Eve
nts
/ 100
0 pa
tient
yea
rsE
vent
s / 1
000
patie
nt y
ears
Intracranial haemorrhage
Ischaemic stroke
<1.5<1.5 1.51.5––1.91.9 2.02.0––2.52.5 2.62.6––3.03.0 3.13.1––3.53.5 3.63.6--4.04.0 4.14.1--4.54.5 >4.5>4.5
The anticoagulant effect
of vitamin K antagonists
are optimized when
therapeutic doses are
maintained within a very
narrow range
Hylek EM, et al. Hylek EM, et al. N Eng J Med N Eng J Med 2003; 349:10192003; 349:1019--1026.1026.
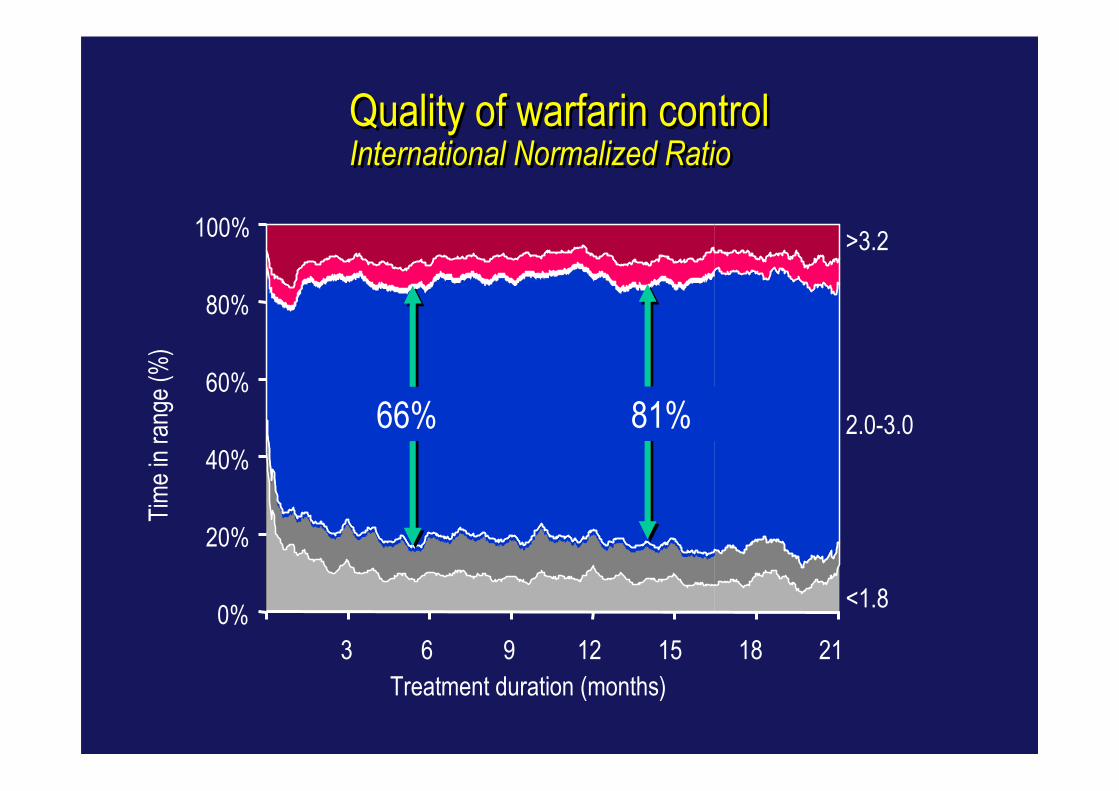
Quality of warfarin controlInternational Normalized Ratio
Quality of warfarin controlInternational Normalized Ratio
0%
20%
40%
60%
80%
100%
3 6 9 12 15 18 21
<1.8
>3.2
2.0-3.0
Treatment duration (months)
Tim
e in
ran
ge (
%)
66% 81%
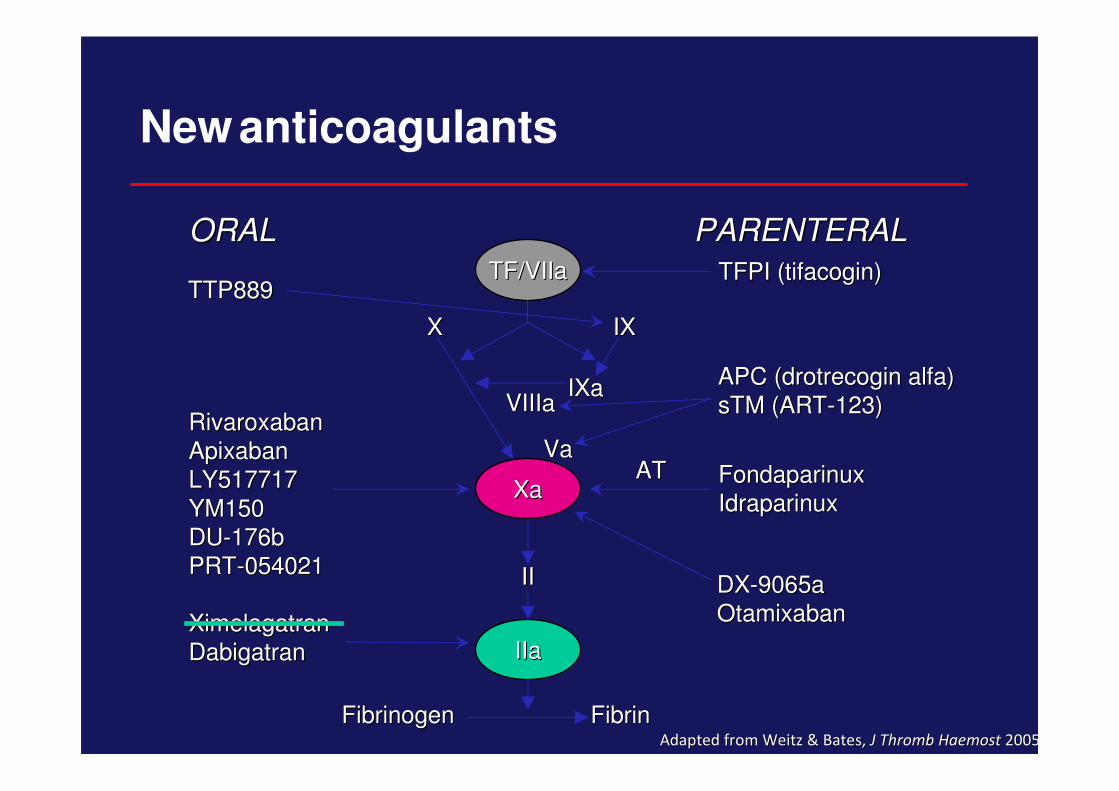
New anticoagulants
FibrinFibrinFibrinogenFibrinogenAdapted from Weitz & Bates,Adapted from Weitz & Bates, J Thromb Haemost J Thromb Haemost 20052005
TFPI (tifacogin)TFPI (tifacogin)
FondaparinuxFondaparinux
IdraparinuxIdraparinux
RivaroxabanRivaroxaban
ApixabanApixaban
LY517717LY517717
YM150YM150
DUDU--176b176b
PRTPRT--054021054021
XimelagatranXimelagatran
DabigatranDabigatran
ORALORAL PARENTERALPARENTERAL
DXDX--9065a9065a
OtamixabanOtamixaban
XaXa
IIaIIa
TF/VIIaTF/VIIa
XX IXIX
IXaIXaVIIIaVIIIa
VaVa
IIII
ATAT
APC (drotrecogin alfa)APC (drotrecogin alfa)
sTM (ARTsTM (ART--123)123)
TTP889TTP889
� 18,113 patients randomised during 2 years1,2
� 50% of enrolled patients were naïve to previous oral AC
� Median treatment duration: 2 years
� 951 centres in 44 countries
� Dec 2005 to March 2009
RE-LY®: Randomised Evaluation of
Long term anticoagulant therapy
1. Ezekowitz MD, et al. Am Heart J 2009;157:805-10.
2. Connolly SJ., et al. NEJM Aug 30th 2009.
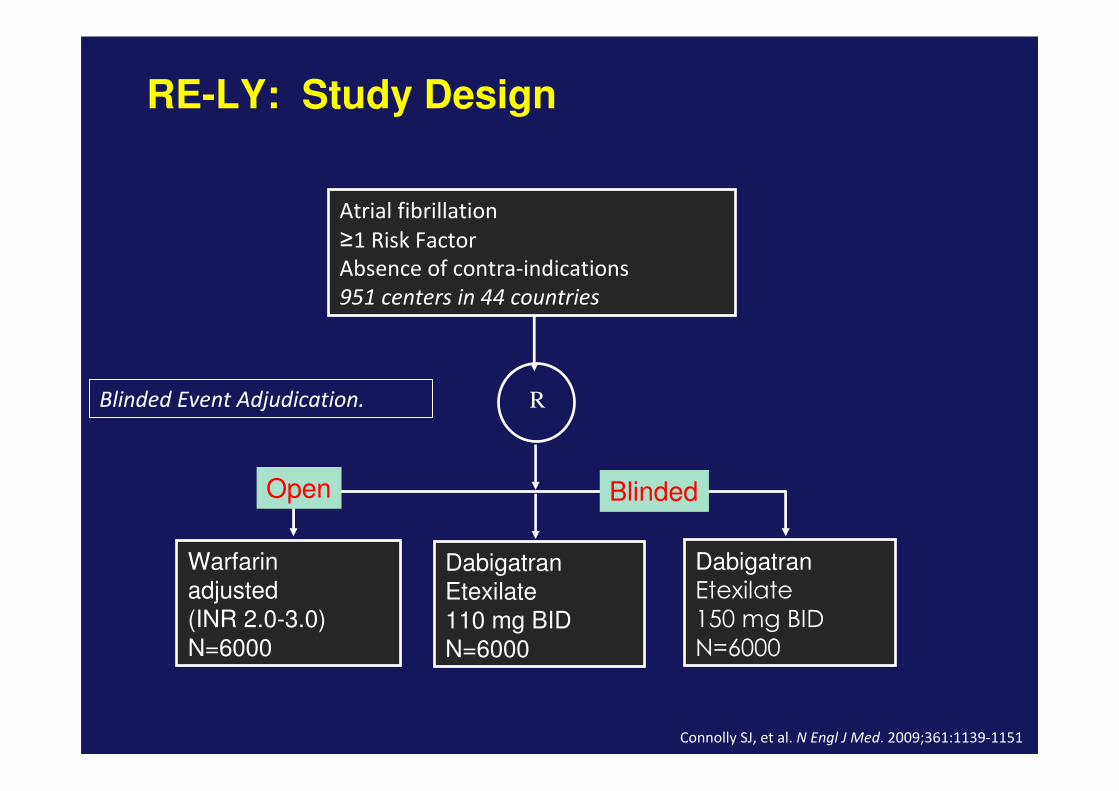
RE-LY: Study Design
Atrial fibrillation
≥1 Risk Factor
Absence of contra-indications
951 centers in 44 countries
R
Warfarin
adjusted
(INR 2.0-3.0)
N=6000
Dabigatran
Etexilate
110 mg BID
N=6000
Dabigatran
Etexilate
150 mg BID
N=6000
Blinded Event Adjudication.
Open Blinded
Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151

RE-LY® – inclusion criteria
1) Documented atrial fibrillation and
2) One additional risk factor for stroke:
a) History of previous stroke, TIA, or systemic embolism
b) LVEF less than 40%
c) Symptomatic Heart Failure, NYHA Class II or greater
d) Age of 75 years or more
e) Age of 65 years or more and one of the following additional risk factors: Diabetes mellitus, CAD or Hypertension

RE-LY: Baseline Characteristics
Characteristic Dabigatran 110
mg
Dabigatran 150
mgWarfarin
Randomized 6015 6076 6022
Mean age (years) 71.4 71.5 71.6
Male (%) 64.3 63.2 63.3
CHADS2 score (mean)
0-1 (%)2 (%)
3+ (%)
2.1
32.634.7
32.7
2.2
32.235.2
32.6
2.1
30.937.0
32.1
Prior stroke/TIA (%) 19.9 20.3 19.8
Prior MI (%) 16.8 16.9 16.1
CHF (%) 32.2 31.8 31.9
Baseline ASA (%) 40.0 38.7 40.6
Warfarin Naïve (%) 49.9 49.8 51.4
Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
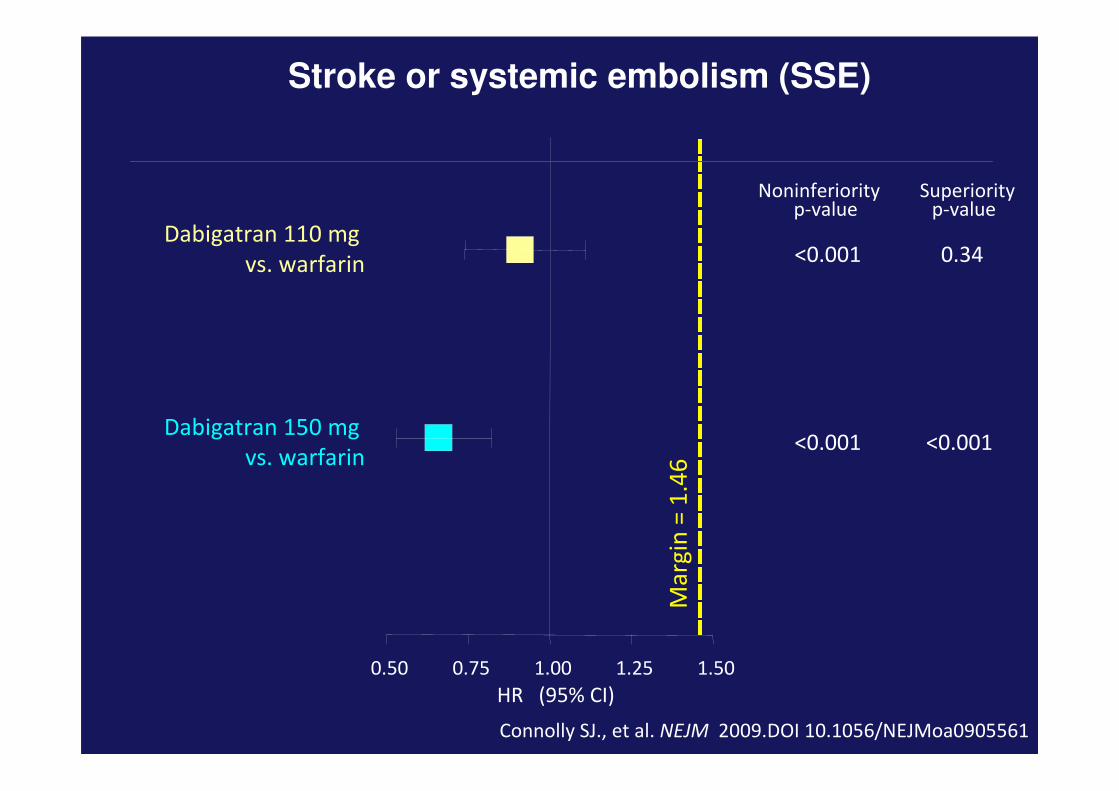
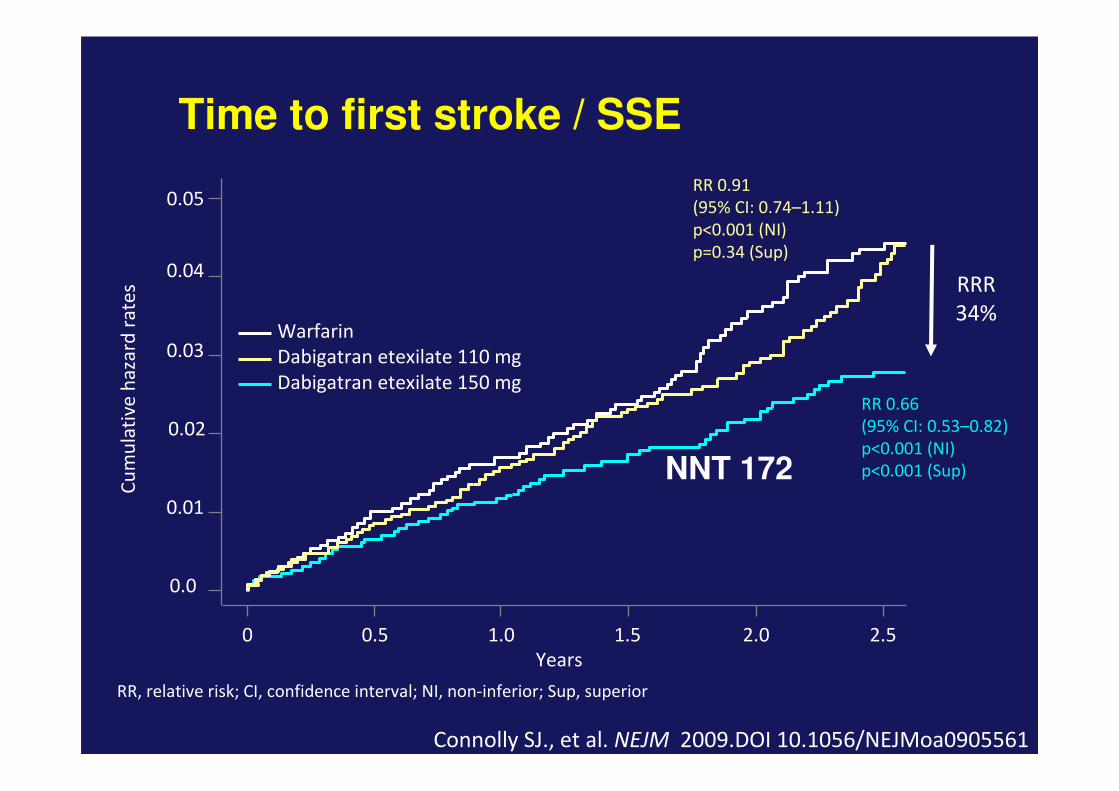
Stroke or systemic embolism (SSE)
0.50 0.75 1.00 1.25 1.50
Dabigatran 110 mg
vs. warfarin
Dabigatran 150 mg
vs. warfarin
Noninferiorityp-value
<0.001
<0.001
Superiorityp-value
0.34
<0.001
Ma
rgin
= 1
.46
HR (95% CI)
Connolly SJ., et al. NEJM 2009.DOI 10.1056/NEJMoa0905561
0.01
0.02
0.03
0.05
0.04
Cu
mu
lati
ve
ha
zard
ra
tes
RR 0.91
(95% CI: 0.74–1.11)
p<0.001 (NI)
p=0.34 (Sup)
RR 0.66
(95% CI: 0.53–0.82)
p<0.001 (NI)
p<0.001 (Sup)
Years
0 0.5 1.0 1.5 2.0 2.5
0.0
Warfarin
Dabigatran etexilate 110 mg
Dabigatran etexilate 150 mg
RR, relative risk; CI, confidence interval; NI, non-inferior; Sup, superior
Time to first stroke / SSE
RRR
34%
Connolly SJ., et al. NEJM 2009.DOI 10.1056/NEJMoa0905561
NNT 172
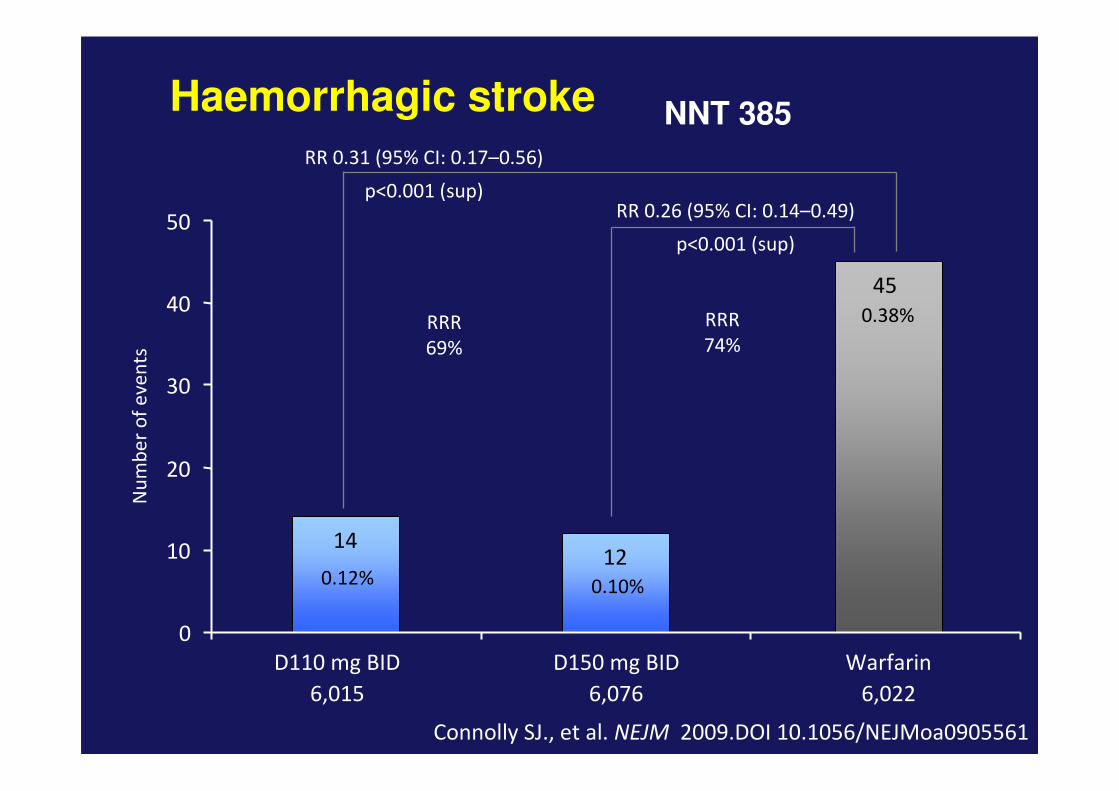
RR 0.26 (95% CI: 0.14–0.49)
p<0.001 (sup)
Haemorrhagic stroke
Connolly SJ., et al. NEJM 2009.DOI 10.1056/NEJMoa0905561
RR 0.31 (95% CI: 0.17–0.56)
p<0.001 (sup)
Nu
mb
er
of
eve
nts
6,015 6,076 6,022
1412
45
0
10
20
30
40
50
D110 mg BID D150 mg BID Warfarin
0.10%
0.38%RRR
69%
RRR
74%
0.12%
NNT 385

3.75 3.64
4.13
0.00
1.00
2.00
3.00
4.00
D110 mg BID D150 mg BID Warfarin
RR 0.88 (95% CI: 0.77–1.00)
p=0.051 (sup)
All cause mortalityRR 0.91 (95% CI: 0.80–1.03)
p=0.13 (sup)
446 / 6,015 438 / 6,076 487 / 6,022
% p
er
ye
ar
Connolly SJ., et al. NEJM 2009.DOI 10.1056/NEJMoa0905561
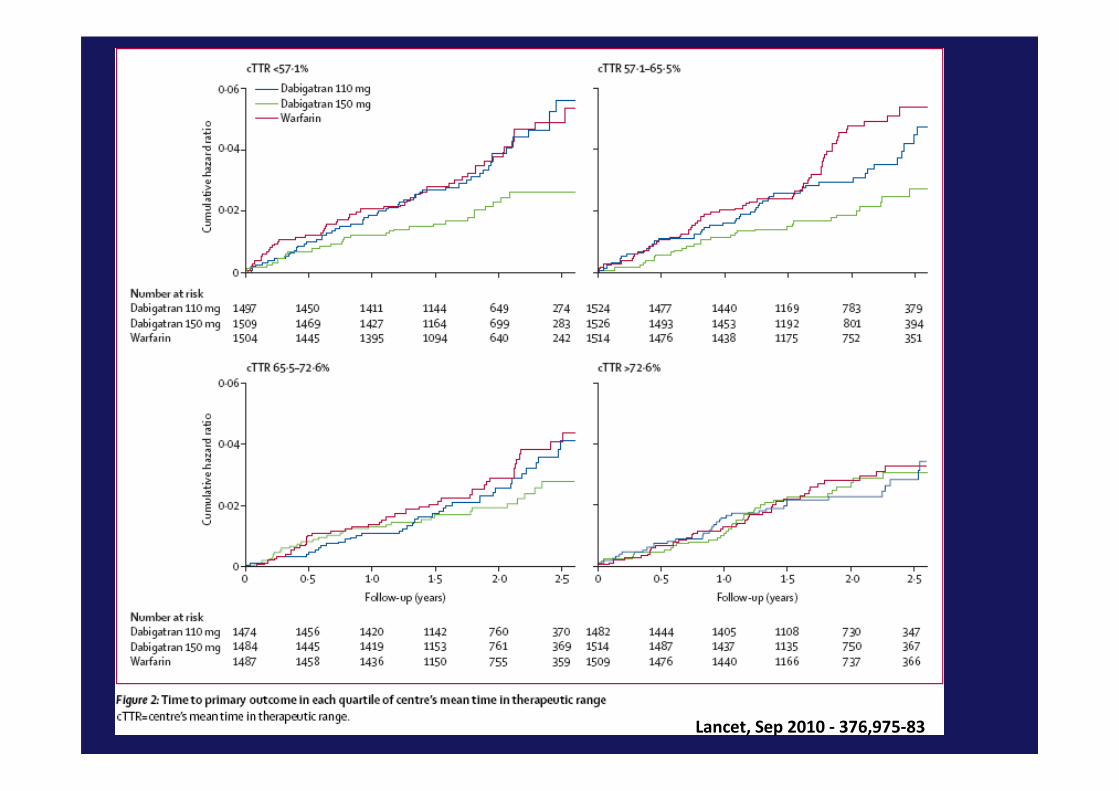
Lancet, Sep 2010 - 376,975-83
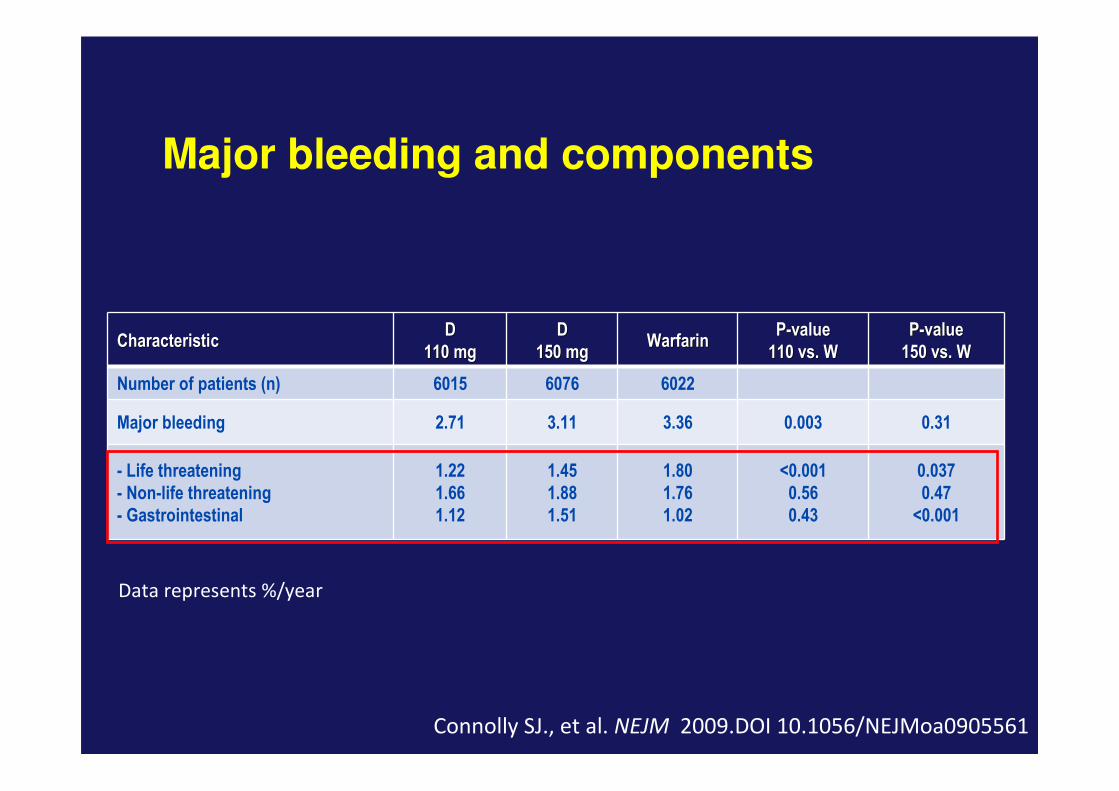
Major bleeding and components
CharacteristicCharacteristicDD
110 mg110 mgDD
150 mg150 mgWarfarinWarfarin
PP--valuevalue
110 vs. W110 vs. WPP--valuevalue
150 vs. W150 vs. W
Number of patients (n) 6015 6076 6022
Major bleeding 2.71 3.11 3.36 0.003 0.31
- Life threatening
- Non-life threatening
- Gastrointestinal
1.22
1.66
1.12
1.45
1.88
1.51
1.80
1.76
1.02
<0.001
0.56
0.43
0.037
0.47
<0.001
Data represents %/year
Connolly SJ., et al. NEJM 2009.DOI 10.1056/NEJMoa0905561
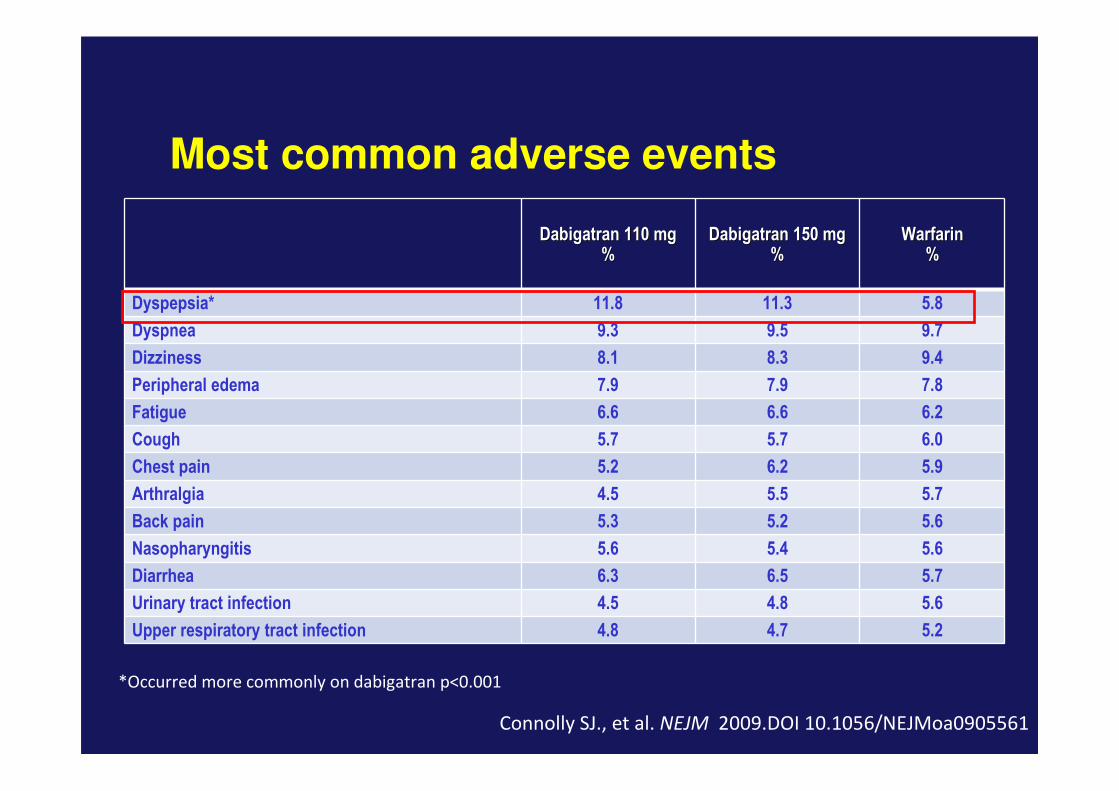
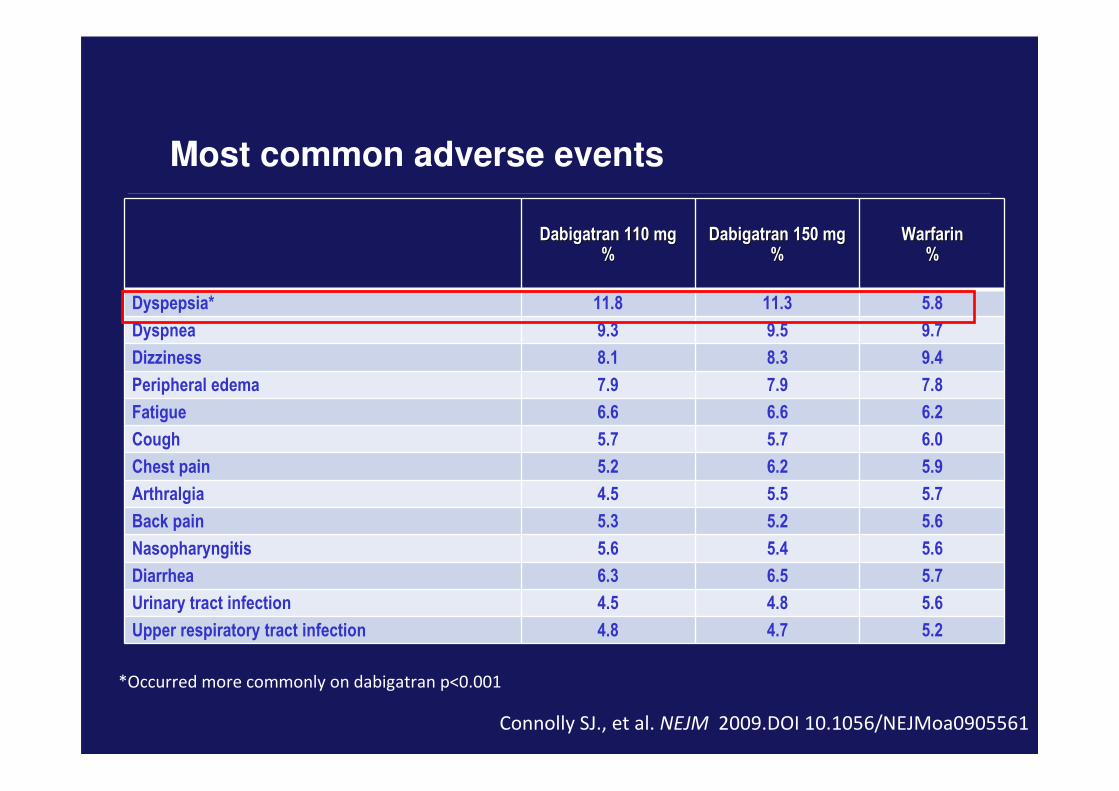
Most common adverse events
Dabigatran 110 mgDabigatran 110 mg%%
Dabigatran 150 mgDabigatran 150 mg%%
WarfarinWarfarin%%
Dyspepsia* 11.8 11.3 5.8
Dyspnea 9.3 9.5 9.7
Dizziness 8.1 8.3 9.4
Peripheral edema 7.9 7.9 7.8
Fatigue 6.6 6.6 6.2
Cough 5.7 5.7 6.0
Chest pain 5.2 6.2 5.9
Arthralgia 4.5 5.5 5.7
Back pain 5.3 5.2 5.6
Nasopharyngitis 5.6 5.4 5.6
Diarrhea 6.3 6.5 5.7
Urinary tract infection 4.5 4.8 5.6
Upper respiratory tract infection 4.8 4.7 5.2
*Occurred more commonly on dabigatran p<0.001
Connolly SJ., et al. NEJM 2009.DOI 10.1056/NEJMoa0905561
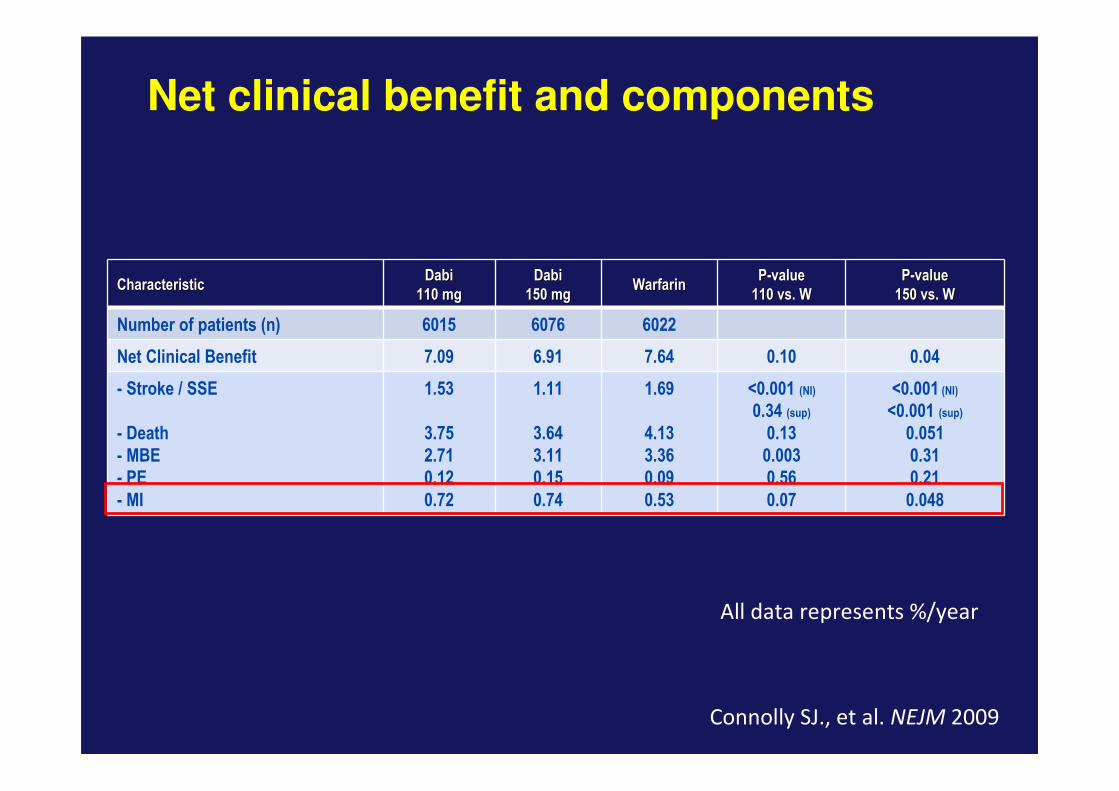
Net clinical benefit and components
CharacteristicCharacteristicDabiDabi
110 mg110 mgDabiDabi
150 mg150 mgWarfarinWarfarin
PP--valuevalue
110 vs. W110 vs. WPP--valuevalue
150 vs. W150 vs. W
Number of patients (n) 6015 6076 6022
Net Clinical Benefit 7.09 6.91 7.64 0.10 0.04
- Stroke / SSE
- Death
- MBE
- PE
- MI
1.53
3.75
2.71
0.12
0.72
1.11
3.64
3.11
0.15
0.74
1.69
4.13
3.36
0.09
0.53
<0.001 (NI)
0.34 (sup)
0.13
0.003
0.56
0.07
<0.001 (NI)
<0.001 (sup)
0.051
0.31
0.21
0.048
All data represents %/year
Connolly SJ., et al. NEJM 2009
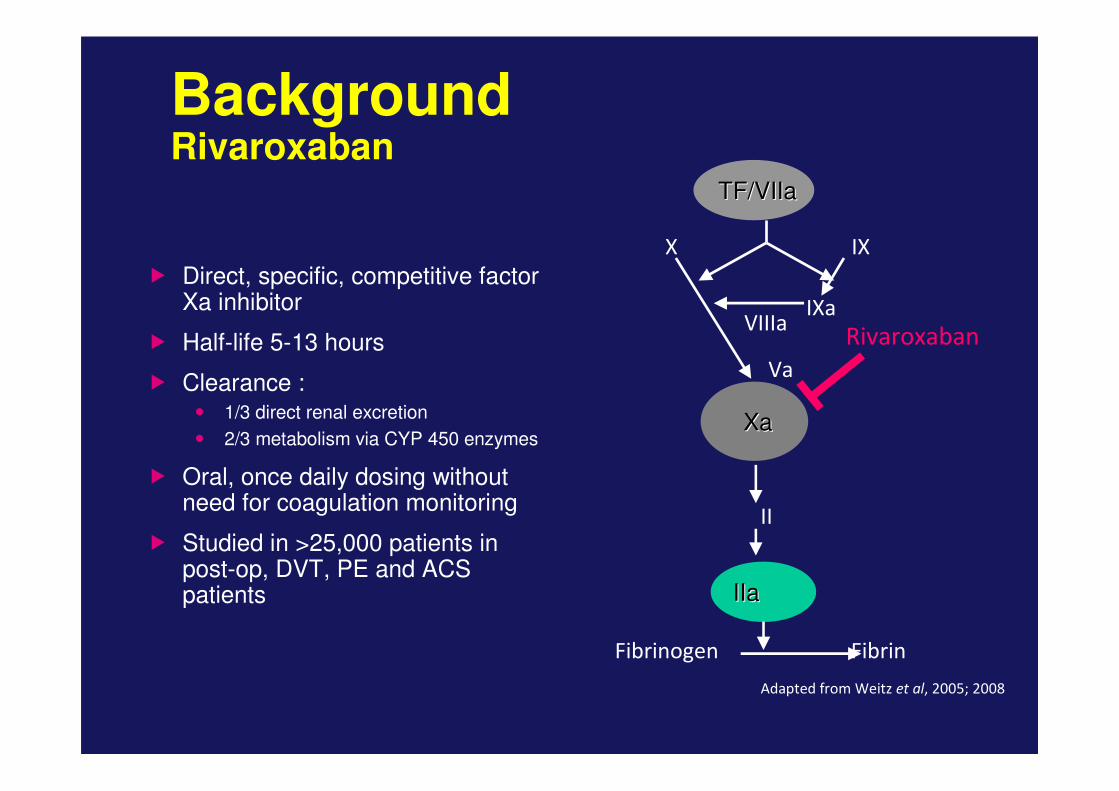
BackgroundRivaroxaban
� Direct, specific, competitive factor Xa inhibitor
� Half-life 5-13 hours
� Clearance :� 1/3 direct renal excretion
� 2/3 metabolism via CYP 450 enzymes
� Oral, once daily dosing without need for coagulation monitoring
� Studied in >25,000 patients in post-op, DVT, PE and ACS patients
Rivaroxaban
XaXa
IIaIIa
TF/VIIaTF/VIIa
X IX
IXaVIIIa
Va
II
FibrinFibrinogen
Adapted from Weitz et al, 2005; 2008
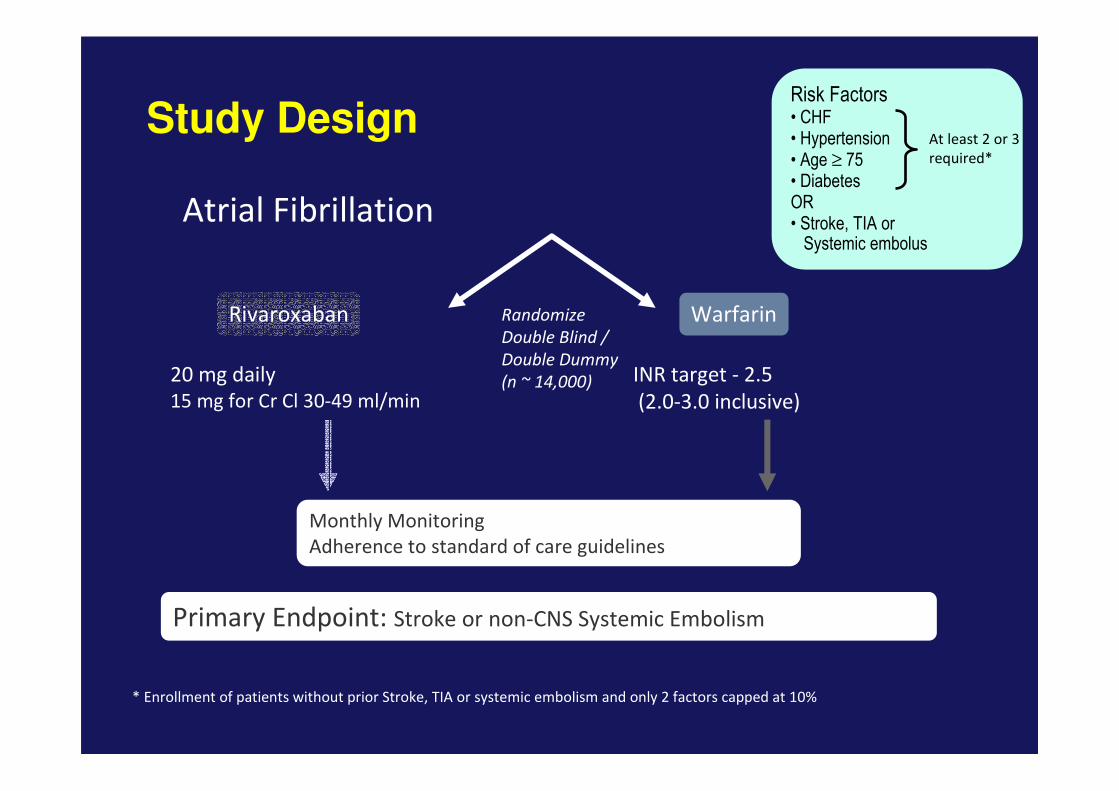
Rivaroxaban Warfarin
Primary Endpoint: Stroke or non-CNS Systemic Embolism
INR target - 2.5
(2.0-3.0 inclusive)
20 mg daily
15 mg for Cr Cl 30-49 ml/min
Atrial Fibrillation
Randomize
Double Blind /
Double Dummy
(n ~ 14,000)
Monthly Monitoring
Adherence to standard of care guidelines
Study Design
* Enrollment of patients without prior Stroke, TIA or systemic embolism and only 2 factors capped at 10%
Risk Factors• CHF • Hypertension • Age ≥ 75 • Diabetes OR• Stroke, TIA or
Systemic embolus
At least 2 or 3
required*
Rocket AF - Preliminary demographics
� 14,269 patients randomised
� Over 1,100 sites in 45 countries
� Median age 73 yrs
� 40% female
� 35% VKA naïve at time of randomisation
Fox K et al. Abstract 89267 presented at ESC 2009
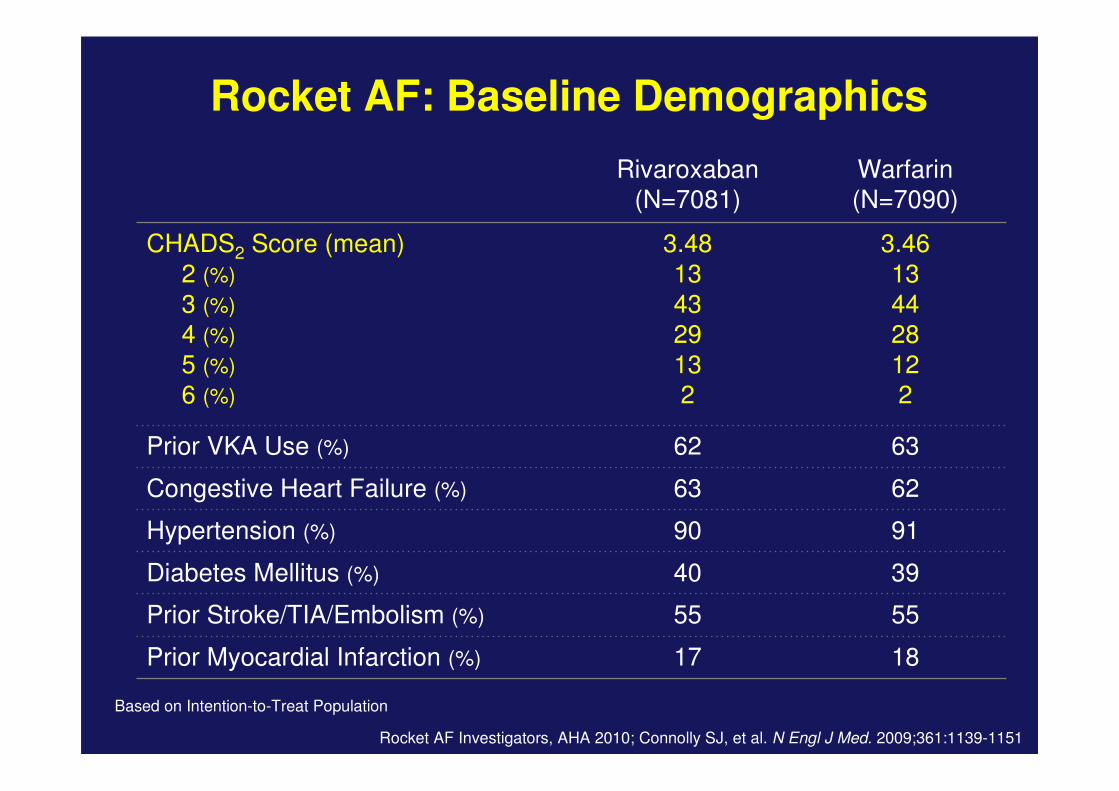
Rivaroxaban (N=7081)
Warfarin (N=7090)
CHADS2 Score (mean)
2 (%)
3 (%)
4 (%)
5 (%)
6 (%)
3.48
13
4329
132
3.46
13
4428
122
Prior VKA Use (%) 62 63
Congestive Heart Failure (%) 63 62
Hypertension (%) 90 91
Diabetes Mellitus (%) 40 39
Prior Stroke/TIA/Embolism (%) 55 55
Prior Myocardial Infarction (%) 17 18
Based on Intention-to-Treat Population
Rocket AF: Baseline Demographics
Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
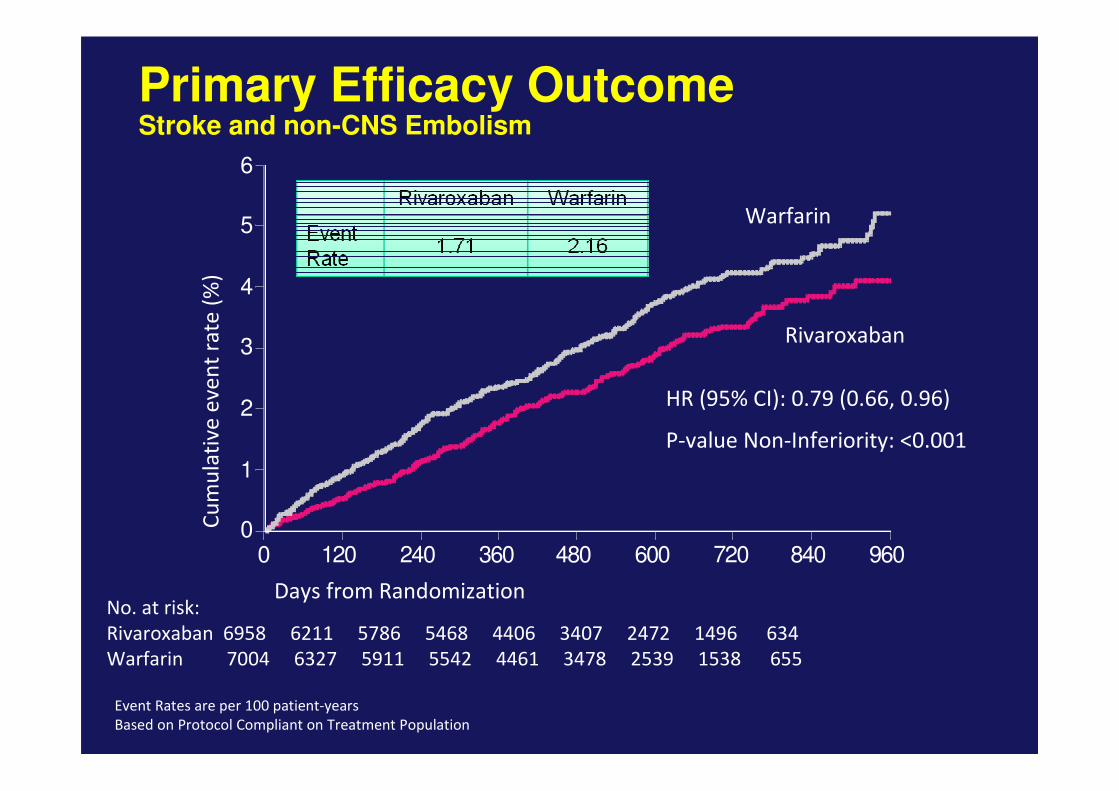
Primary Efficacy OutcomeStroke and non-CNS Embolism
Event Rates are per 100 patient-years
Based on Protocol Compliant on Treatment Population
0
1
2
3
4
5
6
0 120 240 360 480 600 720 840 960
No. at risk:
Rivaroxaban 6958 6211 5786 5468 4406 3407 2472 1496 634
Warfarin 7004 6327 5911 5542 4461 3478 2539 1538 655
Warfarin
HR (95% CI): 0.79 (0.66, 0.96)
P-value Non-Inferiority: <0.001
Days from Randomization
Cu
mu
lati
ve
ev
en
t ra
te (
%)
Rivaroxaban
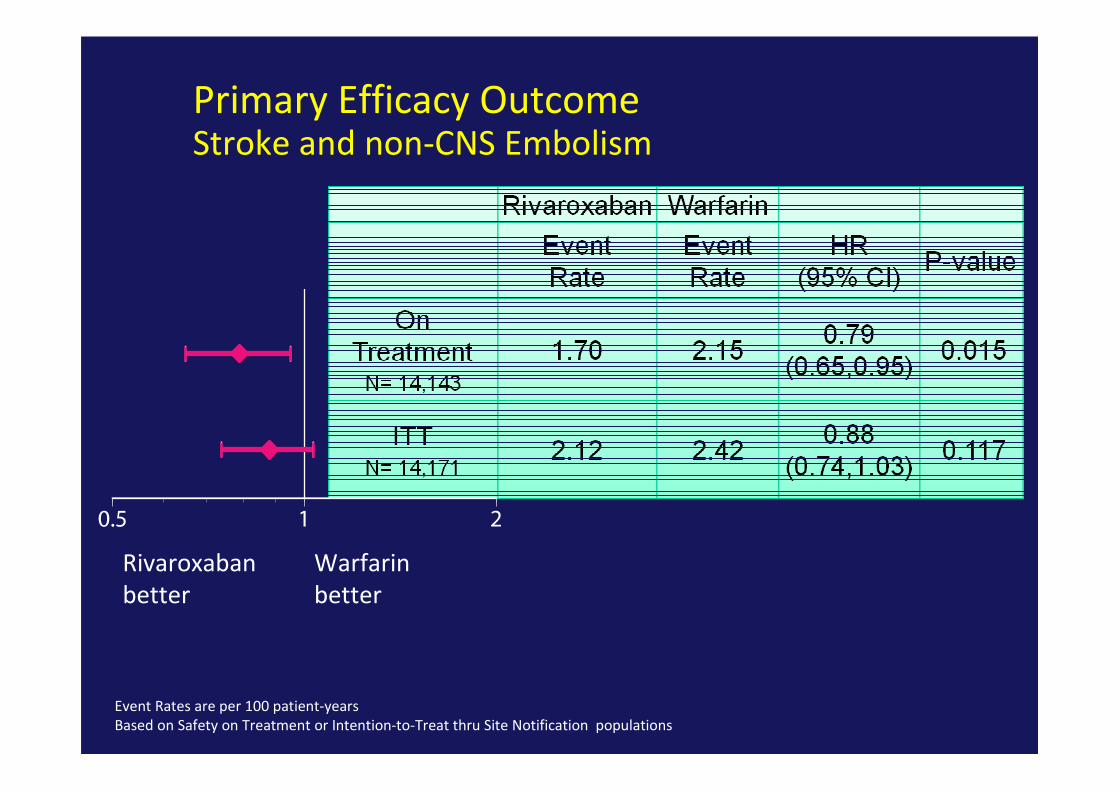
Rivaroxaban
better
Warfarin
better
Primary Efficacy OutcomeStroke and non-CNS Embolism
Event Rates are per 100 patient-years
Based on Safety on Treatment or Intention-to-Treat thru Site Notification populations
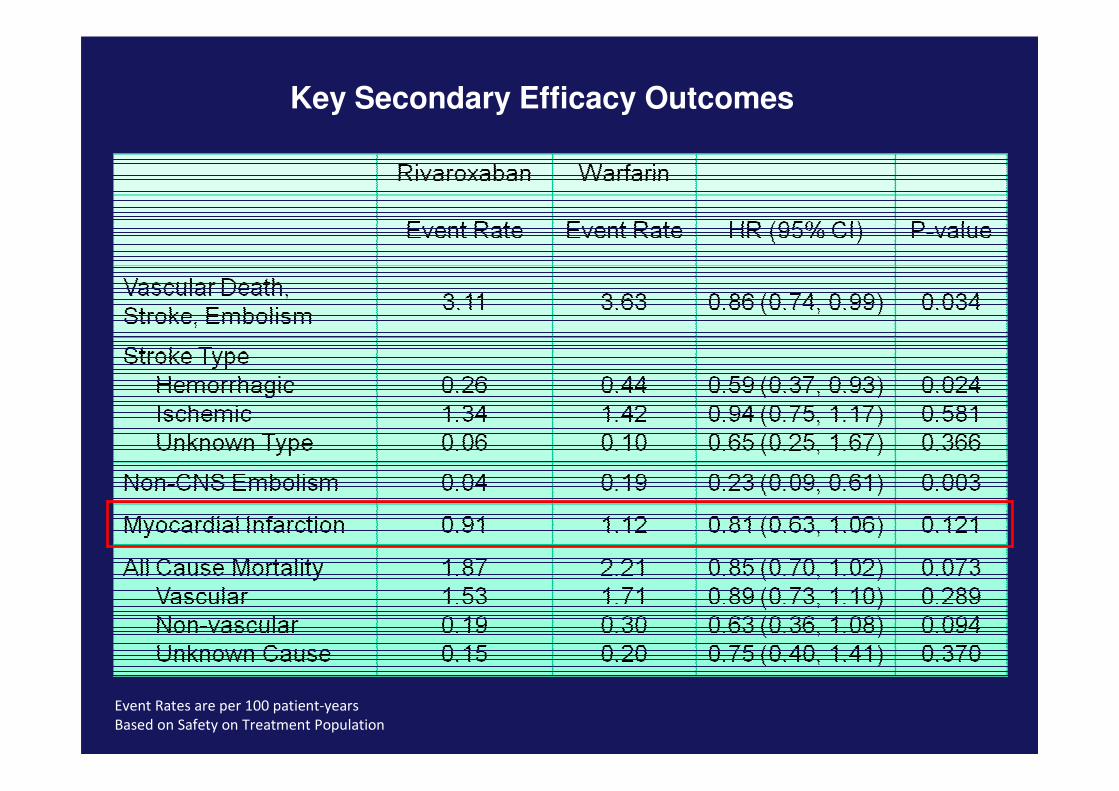
Key Secondary Efficacy Outcomes
Event Rates are per 100 patient-years
Based on Safety on Treatment Population
A Comparison of RE-LY and ROCKET AFTrial Designs and Outcomes

Drug Rivaroxaban Dabigatran
Site of action Xa (direct) Thrombin
Pro-drug No Yes
Frequency of
administration
OD BD
Tmax 2-4 h 0.5 -2 h
Half-Life 9-13 h 14-17 h
Interactions CyP3A4 Inhibitors GpP
Protein Binding 90% 35%
Renal excretion 66% 85%
Antidote none none
HIT frequency No effects on platelets

Double-Blind vs. Open-Label Studies
Differences in Primary efficacy Outcome in SPORTIF V and SPORTIF III
1. JAMA 2005;293(6): 690-698
2. Lancet 2003;362: 1691-1698
0
1
2
3
Eve
nt
rate
/ye
ar
1.2
1.6
Non-inferior efficacy demonstrated with ximelagatran vs. warfarin
1.6
2.3
SPORTIF V1
Double-blind design
N=3922, p=0.13
SPORTIF III2
Open-label design.
N=3410, p=0.10
Warfarin Ximelagatran
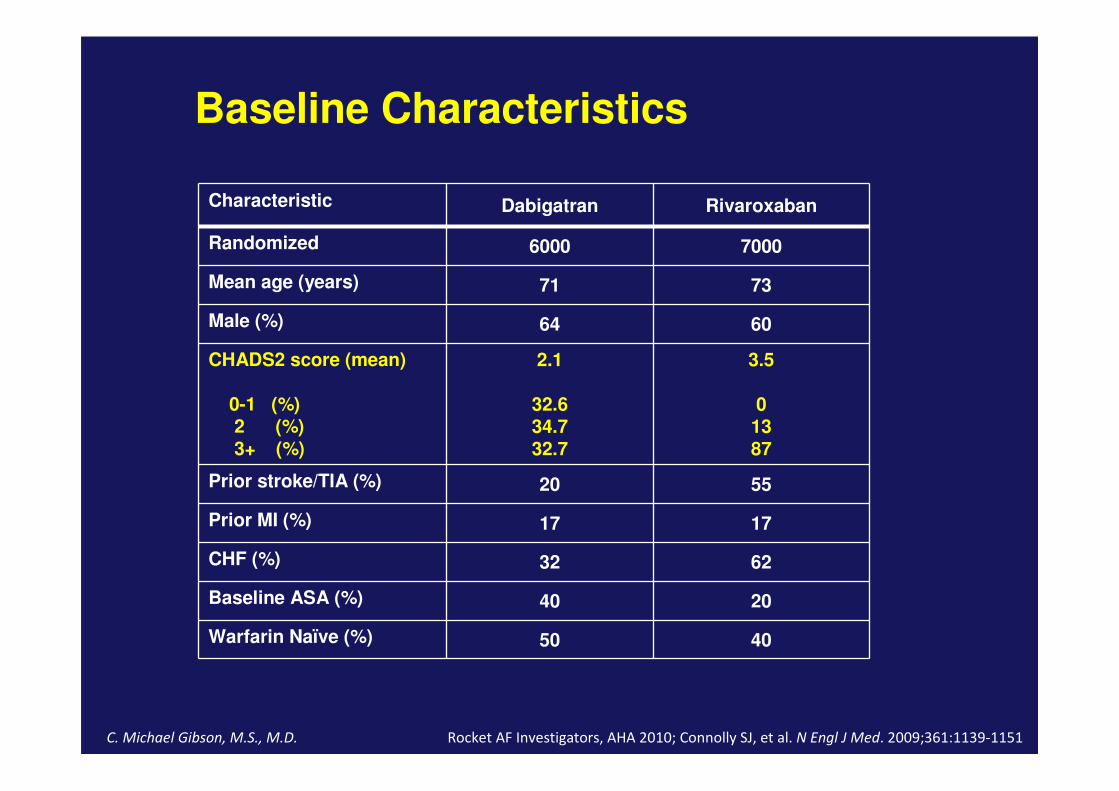
Baseline Characteristics
Characteristic Dabigatran Rivaroxaban
Randomized 6000 7000
Mean age (years) 71 73
Male (%) 64 60
CHADS2 score (mean)
0-1 (%)2 (%)3+ (%)
2.1
32.634.732.7
3.5
01387
Prior stroke/TIA (%) 20 55
Prior MI (%) 17 17
CHF (%) 32 62
Baseline ASA (%) 40 20
Warfarin Naïve (%) 50 40
C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
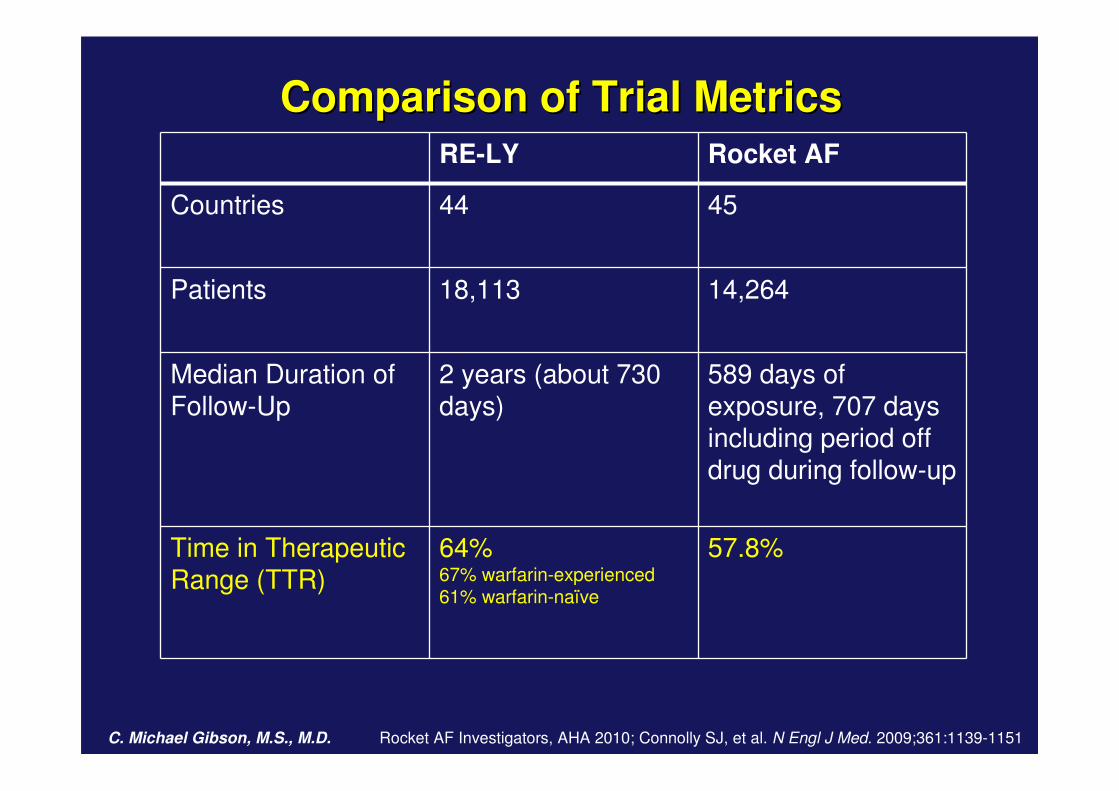
Comparison of Trial MetricsComparison of Trial Metrics
RE-LY Rocket AF
Countries 44 45
Patients 18,113 14,264
Median Duration of Follow-Up
2 years (about 730 days)
589 days of exposure, 707 days including period off drug during follow-up
Time in Therapeutic Range (TTR)
64%67% warfarin-experienced61% warfarin-naïve
57.8%
C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Impact of Enrolling Higher CHADs Score Patients
Higher CHADs scores are associated with:
1.Higher rates of major bleeding
2.Lower TTRs3.Greater risk of stroke or SE
C. Michael Gibson, M.S., M.D. Personal communication RE-LY Investigators. Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151

Rates of Drug Discontinuation
RE-LY
1 Year:
Dabigatran 110 mg: 14.5%
Dabigatran 150 mg: 15.5%
Warfarin: 10.2%
2 Years:
Dabigatran 110 mg: 20.7%
Dabigatran 150 mg: 21.2%,
Warfarin: 16.6%
Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Most common adverse events
Dabigatran 110 mgDabigatran 110 mg%%
Dabigatran 150 mgDabigatran 150 mg%%
WarfarinWarfarin%%
Dyspepsia* 11.8 11.3 5.8
Dyspnea 9.3 9.5 9.7
Dizziness 8.1 8.3 9.4
Peripheral edema 7.9 7.9 7.8
Fatigue 6.6 6.6 6.2
Cough 5.7 5.7 6.0
Chest pain 5.2 6.2 5.9
Arthralgia 4.5 5.5 5.7
Back pain 5.3 5.2 5.6
Nasopharyngitis 5.6 5.4 5.6
Diarrhea 6.3 6.5 5.7
Urinary tract infection 4.5 4.8 5.6
Upper respiratory tract infection 4.8 4.7 5.2
*Occurred more commonly on dabigatran p<0.001
Connolly SJ., et al. NEJM 2009.DOI 10.1056/NEJMoa0905561
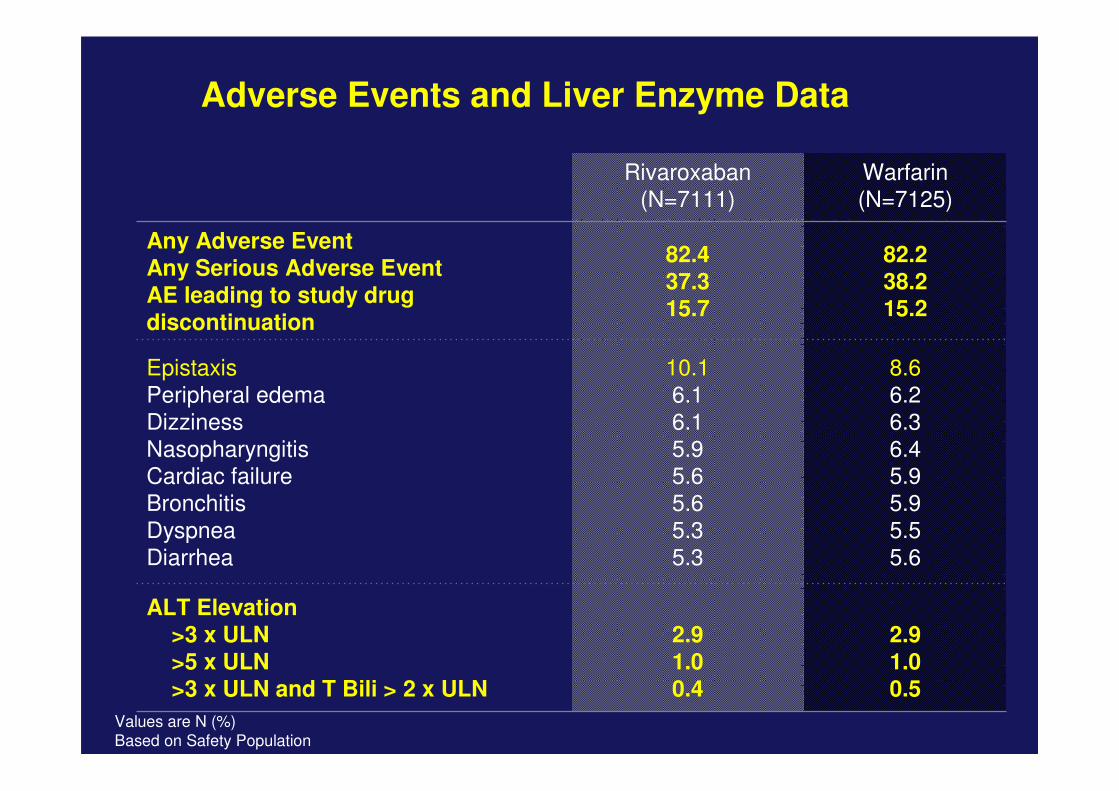
Adverse Events and Liver Enzyme Data
Values are N (%)
Based on Safety Population
Rivaroxaban (N=7111)
Warfarin (N=7125)
Any Adverse EventAny Serious Adverse EventAE leading to study drug discontinuation
82.437.315.7
82.238.215.2
EpistaxisPeripheral edemaDizzinessNasopharyngitisCardiac failureBronchitisDyspneaDiarrhea
10.16.16.15.95.65.65.35.3
8.66.26.36.45.95.95.55.6
ALT Elevation>3 x ULN>5 x ULN>3 x ULN and T Bili > 2 x ULN
2.91.00.4
2.91.00.5

Conclusions
� New agents may make risk reduction in AF easier.
� Newer agents are equally effective at reducing stoke risk with lower bleeding risk, or
� More effective with equal bleeding risk
� New agents bring new side effects
� Economic analysis yet to be considered
� 1st patient to go into A&E with a bleed!!
� Unknown benefit/risk with triple therapy
Pending Questions
� Interactions: drugs and food?
� Association with antiplatelet agents?
� Sub group of patients - Elderly patients?
� Renal insufficiency?
� Liver toxicity?
� Other indications? Valvular prosthesis?
� Lack of Monitoring/adherence – BD vs OD?
� How to deal with bleed?
� Cost may be deciding factor for choice!!
RE-LY vs ROCKET AF
Sotiris Antoniou
Consultant Pharmacist, Cardiovascular Medicine
Barts and the London NHS Trust &
North East London Cardiovascular & Stroke Network