some points on spasm in the alimentary tract
TRANSCRIPT
361
Some PointsON
SPASM IN THE ALIMENTARYTRACT.
Presidential Address delivered on Jan. 12th, 1922,before the Harveian Society.
BY G. DE BEC TURTLE, M.D. DURH.,M.R.C.P. LOND.
IN choosing a subject upon which to deliver thisvaledictory address I have selected that of spasm asit may occur in various parts of the alimentary tract.
DILATATION OF THE ŒSOPHAGUS.
Commencing with the oesophagus :-Idiopathicdilatation of the gullet has been recognised for sometime, but until fairly recently very little has beenwritten on the subject. It may occur during infantor adult life, but before describing the actual condi-tions present I want to remind you of certain physio-
_ logical facts, which I think have some bearing on thesubject. Deglutition has been divided into fourstages. The first stage is when the masticated food,having been collected into a bolus in the mouth, isforced back by the act of swallowing past the anteriorpillars of the fauces. The second stage is the passageof the food through the pharynx and past the aper-tures of the nose and larynx. The third stage is thepassage of the bolus down the oesophagus to thecardiac end of the stomach. The fourth or last stageis the passage of the food through the cardiac ringinto the stomach. The ring is formed by the cardiacsphincter muscle, and is normally in a state of con-traction. If the bolus is small or the food liquid itmay pass immediately into the stomach. On theother hand, food may stop at the cardiac orifice until
’
the peristaltic wave which follows each act of degluti-tion reaches the orifice, when the sphincter muscleis expanded and the food shot into the stomach.
In certain animals the food remains much longerin the gullet, and may be returned to the mouth forfurther mastication, a process known as chewing thecud or rumination. This is due to reverse peristalsisin the oesophagus, and may occasionally occur inhuman beings.
The Cardiac Sphincter.The cardiac sphincter is a circular band of plain
muscle fibre situated at the junction of the oesophagusand the stomach. Its function is to prevent thepassage of food back from the stomach into theoesophagus. It has two distinct activities : (1) a
persistent contracted state or tonus ; (2) rhythmicactivity of contraction and relaxation. It is probablethat the presence of free acid in the stomach influencesthe tonicity of the cardiac sphincter, for it has beenshown that if acid be injected continuously into theduodenum just beyond the pylorus, the pyloricsphincter can be kept closed for an unlimited period.This response of the pylorus to the acid illustrates ageneral law of the alimentary tract that a stimuluscauses a contraction above -the stimulated spot. Ithink an example of this is the spasm that occurs atthe ileocaecal valve when inflammatory changes aretaking place in the appendix. I have already men-tioned that the contraction of the cardiac sphincterundergoes rhythmic oscillation, allowing of slightregurgitation of fluid material from the stomach intothe oesophagus. Each regurgitation, however, isfollowed immediately by a peristaltic wave, whichcauses the escaped material to re-enter the stomach.I shall mention this point again later in referring tocertain types of vomiting.
(Esophageal Obstruction in Young Children.This condition has been well described by Dr. Hugh
Ashby, of Manchester, who showed several cases
of the condition at the provincial meeting of the
Section for the Study of Disease in Children ofthe Royal Society of Medicine, held in Manchesterin June, 1920. Dr. Bellingham Smith has alsorecently shown cases at meetings of the same
section, one of which had been relieved by thepassage of bougies. The history is usually thatthe child above a year old begins to vomit all solidfood at frequent intervals. Before this age liquidsare taken well without any inconvenience ; andvomiting only commences when solid food is begun.The condition of the gullet can be demonstratedquite easily with the assistance of the X rays and ashadow meal, and can be confirmed by the passageof bougies if necessary. In one fatal case the lumenof the oesophagus at the point of the stricture wasjust sufficient to admit of a fine probe being passed,and a microscopical section showed much hypertrophyof the circular muscle fibres and some excess offibrous tissue. Whether this latter was due to thepassage of bougies which had been used in the attemptto dilate the stricture, or to overgrowth of muscle, itis difficult to say.As regards the treatment of this class of case in
infants, it has been suggested that the regular passageof bougies of increasing size dilates the stricture, andby this means a certain number are alleviated andpossibly cured. If, however, the infants are left, orthe parents neglect to bring them for treatment,strictures may become so tight that an anaestheticis needed to enable a bougie to be passed at all. Insome cases it is found that under deep anaesthesia agreat deal of the spasm is relaxed. It has also beensuggested that in well-marked cases with tight stric-tures a gastrostomy might be performed, and thechild fed entirely in this way in order to give theoesophagus complete rest for some weeks from theirritation of food.
Œsophageal Dilatation in Adults.Cardiospasm with dilatation of the oesophagus may
occur in adults. Plummer has reported 40 cases
seen in the Mayo Clinic in 3¼ years. The patientcomplains of food sticking, causing discomfortat the lower end of the sternum ; later there isregurgitation of food, unmixed with acid fluid,the bolus never having reached the stomach. Thediagnosis can be made as before by means ofthe X ray and shadow meal, or by use of thecesophagoscope.
Dr. Arthur F. Hurst, in the Quarterly Journal ofMedicine, 1914, described this condition in adultsas achalasia of the cardia (deriving the term fromthe Greek a negative, &khgr;&agr;&lgr;&agr;&ohgr;, to relax). X rayobservations have shown that when each successiveperistaltic wave passing down the normal oesophagusreaches its lowest extremity the cardia relaxes, justas later the pyloric sphincter also relaxes when thewave reaches it. But in this condition of achalasia,for some reason due no doubt to a reflex inhibitionof relaxation, the cardia does not relax, and in-con-sequence food collects and stagnates in the oesophagus,which becomes dilated and hypertrophied from re-peated but fruitless peristaltic action. Dr. Hurstalso demonstrated that this condition of achalasiacan be quite readily overcome by an indiarubber tubefilled with mercury, which passes without the slightestdifficulty into the stomach, demonstrating the absenceof spasm at the cardia. In the majority of cases noobvious cause for this spasm or failure of relaxationcan be ascertained either during life or post mortem ;in a few an ulcer or carcinoma of the stomach hasbeen present.
Quite recently there appeared 1 an excellent descrip-tion by Dr. N. Mutch of the treatment of the conditionby means of a hydrostatic dilator, which apparentlyacts by forcibly overstretching the cardiac sphincter.The best records, as before mentioned, are those ofPlummer, who followed up the subsequent historiesof over a hundred cases treated by this method, andreported success in 81 per cent.
1 The Practitioner, November, 1921, p. 339.
362
SPASM OF TUB PYLORUS.
Probably the commonest point in the intestinaltract for spasm to occur is at the pylorus. It isfrequently present in infants, and has to be distin-guished from stenosis (a point I shall refer to again),and it is quite usual to meet it in adult life, generallysecondary to some condition such as ulcer or newgrowth in the stomach or duodenum ; but it mayoccur without any primary cause being discoverable.The principal symptom is vomiting, and I want hereto say something about certain types of vomiting.
Types of Vomiting.I have already mentioned rumination or regurgita-
tion of the surplus food. It occurs in strong, vigorous,and healthy babies ; it appears, in fact, to be nature’sway of getting rid of the excess quantity which thechild cannot digest. The habit, for such it is, isassociated with a hyper-excitability of the involuntarymuscles, and in some cases pylorospasm has beenfound. This is what might be described as thesimple type of vomiting, and merely depends uponan over-distended hollow viscus emptying itself in thereverse way because, the pylorus being closed,nothing can escape down the intestinal tract.Take next the vomiting of pregnancy. This has
always been looked upon as, and undoubtedly is, areflex act, but this does not explain how and why itoccurs. As is well known, it is most frequent whenthe patient first assumes the erect posture in themorning, and the vomited material as a rule is littlein quantity, and consists generally of a small amountof mucus and possibly a portion of the previousevening’s meal, but generally only mucus. It is, Ithink, a well-known fact that one of the ways tocheck this regurgitation is to put a small quantity offood into the patient’s stomach while she is still inthe recumbent posture ; if this rule is carefully carriedout a surprisingly large number of these cases yieldto this very simple method of treatment. Theregurgitation of the mucus, &c., is obviously due toan abnormal inhibition of the contraction at thecardiac ring, and this abnormality is overcome byputting the distal part of the alimentary tract intoaction-viz., by giving it some work to do.Another type met with during the late war was of
particular interest. I refer to the slightly shell-shocked and neurasthenic case, whose chief andperhaps only symptom was persistent vomiting. Isaw quite half a dozen of such cases, and I believe Iwas responsible for coining the term " professionalvomiter." No medicinal or dietary treatment seemedto have the slightest effect on checking the condition.In some cases one could obtain a definite history ofits commencing from a bad stench in the trenches ora gas attack, and in others there was a negativehistory. Those were, I am sure, cases of spasm,either cardiospasm or pylorospasm, more probablythe latter, due to some derangement of the neuro-muscular mechanism of the stomach.
Nervous illechaiiism of the Stomach.To turn for a moment to this mechanism, the
centres which cause constriction are in the medullaoblongata and the fibres run almost entirely inthe vagi. In the medulla also are fibres causingthe pylorus to relax or gape; apparently thepath for these is down the cord and by the splanchnicnerves. It is in this way possible to trace theinfluence of the nervous system upon the move-ments of the stomach, which is well shown bythe fact that psychical conditions, such as anger orpain, may at once stop, or at any rate partiallyinhibit, any gastric movements. The closure of thepylorus is reflex, and the stimulus for this movementis the action of the hydrochloric acid on the mucousmembrane of the duodenum. Pylorospasm, therefore,may result from central impulses or local causes, andthe latter may be either an abnormal amount of oran altered gastric secretion such as hyperacidity, or an ulcer or new growth in the vicinity.
’
DIFFERENTIAL DIAONOSIS OF SPASM AND STEN0SIS.
I mentioned just now that the condition may occurin infants, and has to be distinguished from caseswhere definite stenosis at the pylorus exists, and Ihave drawn out a short table indicating the maindifferences which enable one to arrive at a diagnosis.
STENOSIS. SPASM.1. Boy. I Either sex.2. No evidence of pain. 2. Evidence of pain, crying,
&c.3. Vomiting some time after 3. Vomiting soon after meal,
food, very forcible, through and whole stomach con.
nose, &c., part of contents tents returned.retained.
4. Much dilatation and hyper- 4. No evidence of gastric dfla-trophy. tation or hypertrophy.
5. Typical peristaltic waves 5. Before the vomiting com-precede vomiting. mences the stomach may
stand out distinctly, butno definite peristalticwaves.
6. Definite pyloric tumour. 6. No pyloric tumour.7. Constipation. 7. Motions scanty, but slight
diarrhoea sometimes.
As regards the aetiology of hypertrophic pylorusthere are two schools of thought: (1) Those whohold that the condition is a primary congenital hyper-plasia, and that the abnormal functions are theresult and not the cause of the muscular enlargement ;(2) those who say it is always the result of some ante-cedent overaction, and who account for the presenceof the hypertrophy by assuming that there has beenmuscular overaction, such as incoordination of thestomach and pylorus for some time, and that thisincoordination may have begun during intra-uterinelife when fluids are passing through the foetalintestinal tract.
ENTEROSPASM.
Coming now to enterospasm, it may be defined asa tonic contraction of the muscular coats of theintestine leading to narrowing or complete occlusionof the intestinal lumen. It is probable that theintestine behaves like this in acute and violententeritis, and may only involve certain parts. Rigidintestinal contraction is also met with in lead colic,and-combined with it-tetanic contraction of themuscular wall of the abdomen (this may be cited asan example of enterospasm due to toxic origin).Colic is in general merely the result of violent localtetanus of the intestine. Enterospasm never occursas an independent neurosis in subjects otherwisenormal and healthy ; if it appears to be so, rememberthat the patient may be in a preataxic stage of tabesdorsalis. The colon is more often affected than thesmall bowel, and of the colon the first and last portionsare most liable to spasm-that is to say, the caecumand the rectum. Even the appendix itself may bea defaulter in this respect, for a small foreign body,such as a grape stone or fæcal concretion, is quitesufficient to set up violent appendicular colic, whichis nothing more than spasm or contraction of themuscular coat of the appendix in its endeavour toexpel the intruder.
Dr. H. P. Hawkins some years ago drew attentionto the fact that spasm occurring in the neighbourhoodof the ileocæcal valve might simulate an attackof appendicitis. I am quite sure many of us
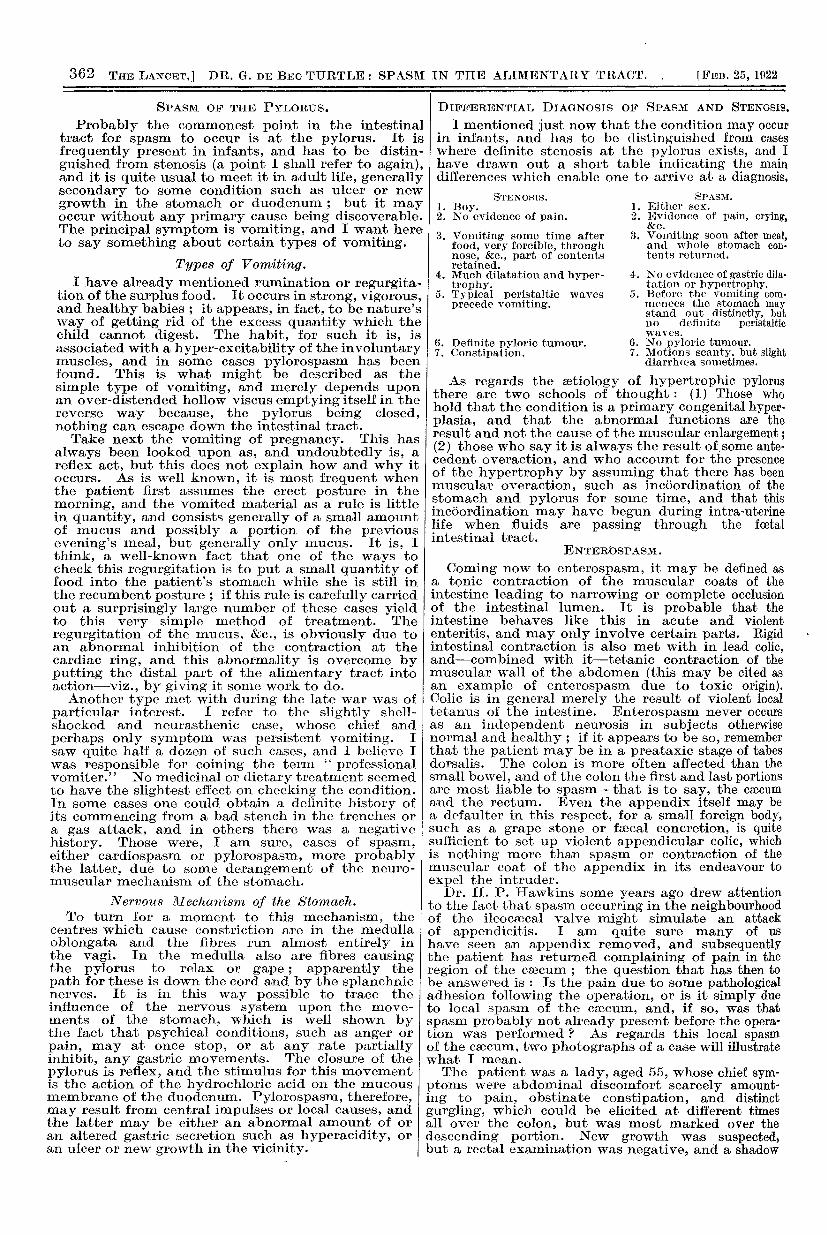
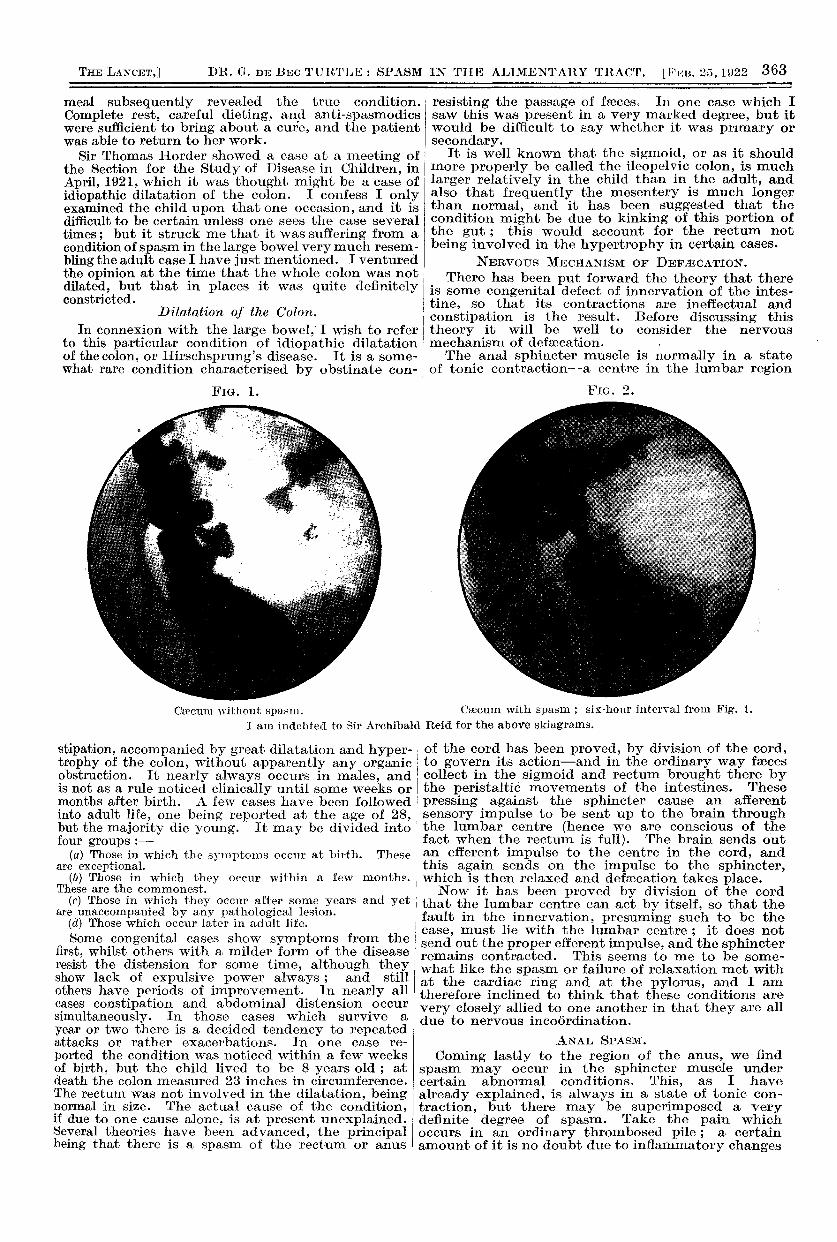
have seen an appendix removed, and subsequentlythe patient has returnea complaining of pain in theregion of the caecum ; the question that has then tobe answered is : Is the pain due to some pathologicaladhesion following the operation, or is it simply dueto local spasm of the caecum, and, if so, was thatspasm probably not already present before the opera-tion was performed ? As regards this local spasmof the caecum, two photographs of a case will illustratewhat I mean.The patient was a lady, aged 55, whose chief sym-
ptoms were abdominal discomfort scarcely amount-ing to pain, obstinate constipation, and distinctgurgling, which could be elicited at different timesall over the colon, but was most marked over thedescending portion. New growth was suspected,but a rectal examination was negative, and a shadow
363
meal subsequently revealed the true condition. Complete rest, careful dieting, and anti-spasmodicswere sufficient to bring about a cure, and the patientwas able to return to her work.
Sir Thomas Horder showed a case at a meeting ofthe Section for the Study of Disease in Children, inApril, 1921, which it was thought might be a case ofidiopathic dilatation of the colon. I confess I onlyexamined the child upon that one occasion, and it is difficult to be certain unless one sees the case severaltimes; but it struck me that it was suffering from acondition of spasm in the large bowel very much resem-bling the adult case I have just mentioned. I venturedthe opinion at the time that the whole colon was notdilated, but that in places it was quite definitelyconstricted.
Dilatation of the Colon. !Dilatation of the Colon.In connexion with the large bowel,’ I wish to refer I
to this particular condition of idiopathic dilatationof the colon, or Hirschsprung’s disease. It is a some-what rare condition characterised by obstinate con- ;
FiG. 1.
stipation, accompanied by great dilatation and hyper-trophy of the colon, without apparently any organicobstruction. It nearly always occurs in males, andis not as a rule noticed clinically until some weeks ormonths after birth. A few cases have been followedinto adult life, one being reported at the age of 28,but the majority die young. It may be divided intofour groups :-
(a) Those in which the symptoms occur at birth. Theseare exceptional.
(b) Those in which they occur within a few months.These are the commonest.
(c) Those in which they occur after some years and yetare unaccompanied by any pathological lesion.
(d) Those which occur later in adult life.Some congenital cases show symptoms from the
first, whilst others with a milder form of the diseaseresist the distension for some time, although theyshow lack of expulsive power always ; and stillothers have periods of improvement. In nearly allcases constipation and abdominal distension occursimultaneously. In those cases which survive a
year or two there is a decided tendency to repeatedattacks or rather exacerbations. In one case re-
ported the condition was noticed within a few weeksof birth, but the child lived to be 8 years old ; atdeath the colon measured 23 inches in circumference.The rectum was not involved in the dilatation, beingnormal in size. The actual cause of the condition,if due to one cause alone, is at present unexplained.Several theories have been advanced, the principalbeing that there is a spasm of the rectum or anus
resisting the passage of faeces. In one case which Isaw this was present in a very marked degree, but itwould be difficult to say whether it was primary orsecondary.
It is well known that the sigmoid, or as it shouldmore properly be called the ileopelvic colon, is muchlarger relatively in the child than in the adult, andalso that frequently the mesentery is much longerthan normal, and it has been suggested that thecondition might be due to kinking of this portion ofthe gut ; this would account for the rectum notbeing involved in the hypertrophy in certain cases.
NERVOUS MECHANISM OF DEFÆCATION.There has been put forward the theory that there
is some congenital defect of innervation of the intes-tine, so that its contractions are ineffectual and
constipation is the result. Before discussing thistheory it will be well to consider the nervous
mechanism of defæcation. ’
The anal sphincter muscle is normally in a stateof tonic contraction-a centre in the lumbar region
FIG. 2.
of the cord has been proved, by division of the cord,to govern its action-and in the ordinary way faecescollect in the sigmoid and rectum brought there bythe peristaltic movements of the intestines. Thesepressing against the sphincter cause an afferentsensory impulse to be sent up to the brain throughthe lumbar centre (hence we are conscious of thefact when the rectum is full). The brain sends outan efferent impulse to the centre in the cord, andthis again sends on the impulse to the sphincter,which is then relaxed and defaecation takes place.
.
Now it has been proved by division of the cordi that the lumbar centre can act by itself, so that the! fault in the innervation, presuming such to be the! case, must lie with the lumbar centre ; it does notsend out the proper efferent impulse, and the sphincterremains contracted. This seems to me to be some-what like the spasm or failure of relaxation met withat the cardiac ring and at the pylorus, and I amtherefore inclined to think that these conditions arevery closely allied to one another in that they are alldue to nervous incoordination.
ANAL SPASM.
Coming lastly to the region of the anus, we findspasm may occur in the sphincter muscle undercertain abnormal conditions. This, as I havealready explained, is always in a state of tonic con-traction, but there may be superimposed a verydefinite degree of spasm. Take the pain whichoccurs in an ordinary thrombosed pile ; a certainamount of it is no doubt due to inflammatory changes
Cæcum without spasm. Cæcum with spasm ; six-hour interval from Fig. 1.
I am indebted to Sir Archibald Reid for the above skiagrams.
364
taking place in the vessels, but a good deal is, Ibelieve, due to the overaction of the external sphinctermuscle, more especially if the pile is just beingextruded through that muscular ring. The samestate applies to a fissure. Anybody who has attemptedto make a rectal examination under either of these
conditions will, I am sure, have realised this super-imposed spasm as I have called it upon the normaltonically contracted sphincter muscle, and if werelieve this spasm we cure at least 50 per cent. ofthe patient’s pain.
In this short address I have not touched upon thequestion of treatment-all I have done is to try toindicate where in the alimentary tract one may lookfor, and expect at times to find, abnormal spasm ;and, secondly, to try to point out why this abnormalspasm may occur. ,
GAMMA RAYS AND MALIGNANT DISEASE.
BY REGINALD MORTON, M.D.C.M. TORONTO, F.R.C.S. EDIN., D.P.H.,
PHYSICIAN, X RAY DEPARTMENT, WEST LONDON HOSPITAL.
THE introduction of the Erlangen method of X raytreatment marks a definite advance in an importantbranch of professional work, and like most otheradvances of a similar nature, especially in the earlierstages, it has come in for a large amount of adversecomment. Few medical men have clear ideas on thegeneral principles governing the use and action ofX rays in therapeutics, but a common knowledge ofthese principles should serve as a useful correctiveto misunderstanding and inaccurate statement.Regarding the alleged dangers of the Erlangen technique it is generally admitted that, in all circum-stances depending on human control for their properapplication, accidents are liable to, and sometimes do,happen. Lives have been lost through error indispensing dangerous drugs. Apart from this risk theErlangen method is not dangerous in competent hands.Even if there were some appreciable danger it wouldneed to be very serious to be comparable to the graveplight of most of the patients who come to us forpossible relief. During the past year I have treatednot less than 300 cases by this method without seeingany severe X ray burn ; nor has there been a singleinstance of sloughing. It is largely owing tounfortunate antagonism that the method cannotyet be carried out in its full perfection here as it isat its place of origin. For want of skilled assistancedosage lacks that complete accuracy which constitutesthe chief feature of the system.
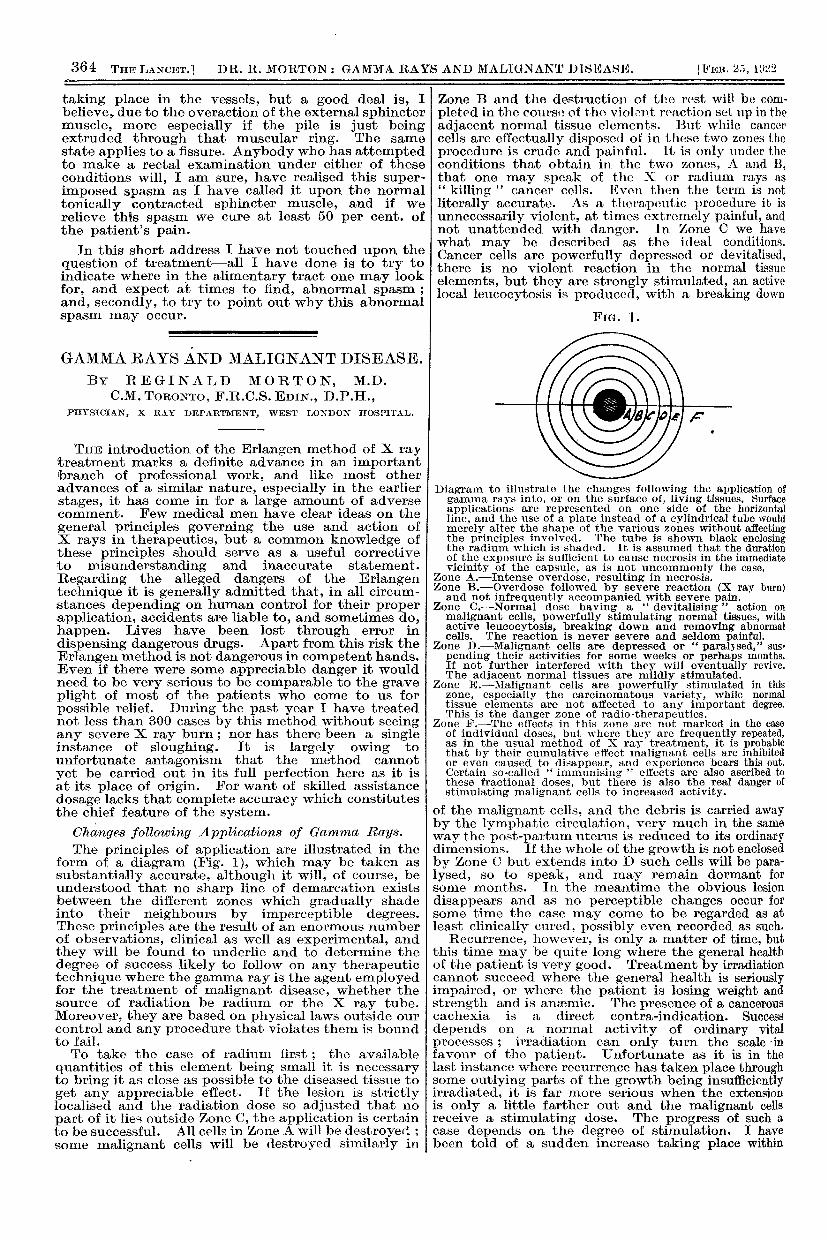
Changes following Applications of Gamma Rays.The principles of application are illustrated in the
form of a diagram (Fig. 1), which may be taken assubstantially accurate, although it will, of course, beunderstood that no sharp line of demarcation exists Ibetween the different zones which gradually shadeinto their neighbours by imperceptible degrees.These principles are the result of an enormous numberof observations, clinical as well as experimental, andthey will be found to underlie and to determine thedegree of success likely to follow on any therapeutictechnique where the gamma ray is the agent employedfor the treatment of malignant disease, whether thesource of radiation be radium or the X ray tube.Moreover, they are based on physical laws outside ourcontrol and any procedure that violates them is boundto fail.To take the case of radium first ; the available
quantities of this element being small it is necessaryto bring it as close as possible to the diseased tissue toget any appreciable effect. If the lesion is strictlylocalised and the radiation dose so adjusted that nopart of it lies outside Zone C, the application is certainto be successful. All cells in Zone A will be destroyed;some malignant cells will be destroyed similarly in
Zone B and the destruction of the rest will be com-pleted in the course of the viotr’nt reaction set up in theadjacent normal tissue elements. But while cancer
cells are effectually disposed of in these two zones theprocedure is crude and painful. It is only under theconditions that obtain in the two zones, A and B,that one may speak of the X or radium rays as" killing cancer cells. Even then the term is notliterally accurate. As a therapeutic procedure it isunnecessarily violent, at times extremely painful, andnot unattended with danger. In Zone C we havewhat may be described as the ideal conditions.Cancer cells are powerfully depressed or devitalised,there is no violent reaction in the normal tissueelements, but they are strongly stimulated, an activelocal leucocytosis is produced, with a breaking down
FIG. 1.
Diagram to illustrate the changes following the application ofgamma rays into, or on the surface of, living tissues. Surfaceapplications are represented on one side of the horizontalline, and the use of a plate instead of a cylindrical tube wouldmerely alter the shape of the various zones without affectingthe principles involved. The tube is shown black enclosingthe radium which is shaded. It is assumed that the durationof the exposure is sufficient to cause necrosis in the immediatevicinity of the capsule, as is not uncommonly the case.
Zone A.-Intense overdose, resulting in necrosis.Zone B.-Overdose followed by severe reaction (X ray burn)and not infrequently accompanied with severe pain.
Zone C.-Normal dose having a " devitalising
" action on
malignant cells, powerfully stimulating normal tissues, withactive leucocytosis, breaking down and removing abnormalcells. The reaction is never severe and seldom painful.
Zone D.—Malignant cells are depressed or " paralysed," sus’pending their activities for some weeks or perhaps months.If not further interfered with they will eventually revive.The adjacent normal tissues are mildly stimulated.
Zone E.-Malignant cells are powerfully stimulated in thiszone, especially the carcinomatous variety, while normal
, tissue elements are not affected to any important degree.I This is the danger zone of radio-therapeutics.
Zone F.-The effects in this zone are not marked in the caseof individual doses, but where they are frequently repeated,I as in the usual method of X ray treatment, it is probable
that by their cumulative effect malignant cells are inhibitedor even caused to disappear, and experience bears this out.Certain so-called " immunising " ettects are also ascribed tothese fractional doses, but there is also the real danger ofstimulating malignant cells to increased activity.
of the malignant cells, and the debris is carried awayby the lymphatic circulation, very much in the sameway the post-partum uterus is reduced to its ordinarydimensions. If the whole of the growth is not enclosedby Zone C but extends into D such cells will be para-lysed, so to speak, and may remain dormant forsome months. In the meantime the obvious lesiondisappears and as no perceptible changes occur forsome time the case may come to be regarded as atleast clinically cured, possibly even recorded as such.
Recurrence, however, is only a matter of time, butthis time may be quite long where the general healthof the patient is very good. Treatment by irradiationcannot succeed where the general health is seriouslyimpaired, or where the patient is losing weight andstrength and is anaemic. The presence of a cancerouscachexia is a direct contra-indication. Successdepends on a normal activity of ordinary vitalprocesses ; irradiation can only turn the scale -infavour of the patient. Unfortunate as it is in thelast instance where recurrence has taken place throughsome outlying parts of the growth being insufficientlyirradiated, it is far more serious when the extensionis only a little farther out and the malignant cellsreceive a stimulating dose. The progress of such acase depends on the degree of stimulation. I havebeen told of a sudden increase taking place within