sodium channel blockers (full coverage)
TRANSCRIPT

Sodium Channel Blockers
Jacinto, Adrien Kyle M.(Our Lady of Fatima University)
Adrien Kyle M. Jacinto, RPh (Confidential File)

Adrien Kyle M. Jacinto, RPh (Confidential File)
Sodium(Na+)
• Major Extracellular Cation• Function: Excitatory/Activator

Adrien Kyle M. Jacinto, RPh (Confidential File)
Channels/Transport
• Regulatory proteins that take part in trans- membrane signaling and regulates ionic composition.

Adrien Kyle M. Jacinto, RPh (Confidential File)
Sodium Channel
Function:• Play a central role in the transmission of action potentials along a
nerve

Adrien Kyle M. Jacinto, RPh (Confidential File)
Types Of Na+ Channels
• Voltage gatedThere’s a regulation of channels depending on charges (Ions) approaching to cell membranes (either open or close the channel).• Ligand gated (nicotinic acetylcholine receptor) Ligand binding alters
channel/receptor conformation and opens the pore

Adrien Kyle M. Jacinto, RPh (Confidential File)
Physiology of the Nerve Impulse
Resting potential• Na (3 ions) outside the cell.• K (2 ions) inside the cell.• -70mvolts

Adrien Kyle M. Jacinto, RPh (Confidential File)
Physiology of the Nerve Impulse
Action potential• All or none response

Adrien Kyle M. Jacinto, RPh (Confidential File)
Action potential’s 5 distinct phases
Phase 0: • Depolarization phase• Opening of Na Channel (influx of Na into the cell)Phase 1:• (Partial) repolarization• Closure of Na ChannelPhase 2:• Plateau• Opening of K and Ca ChannelsPhase 3:• Repolarization• Closure of Ca Channel, efflux of K Phase 4:Stabilization phase (Membrane is stable)• Resting potential• Established when movement of K out of cell is equal to their movement into the cell• All channels are closed

Adrien Kyle M. Jacinto, RPh (Confidential File)
Class I: Sodium Channel Blockers
MOA:• Blockade of the Sodium ChannelsSub classification of SCBs:• Antiarrhythmic/Antidysrhythmics • Local Anesthetics• Antiseizure/Anticonvulsants

Adrien Kyle M. Jacinto, RPh (Confidential File)
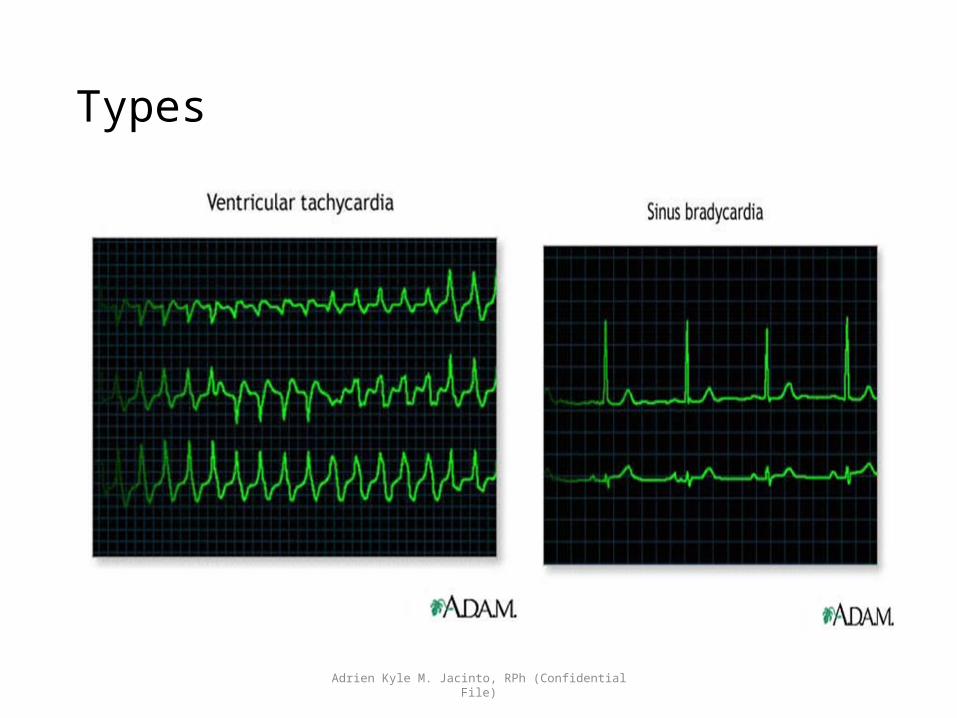
Dysrythmia/Arrhythmia
•An abnormality in the rhythm of the heartbeat• Two basic types of dysrhythmias• Tachydysrhythmias: heart rate is increased• Bradydysrhythmias: heart rate is slowed

Adrien Kyle M. Jacinto, RPh (Confidential File)
Types
Adrien Kyle M. Jacinto, RPh (Confidential File)
Types

Adrien Kyle M. Jacinto, RPh (Confidential File)
Atrial fibrillation

Adrien Kyle M. Jacinto, RPh (Confidential File)
Generation of Dysrhythmias
Two fundamental causes•Disturbances of automaticity•Disturbances of conduction•Atrioventricular block• Reentry (recirculating activation)

Adrien Kyle M. Jacinto, RPh (Confidential File)
Cardiac Conduction Pathways

Adrien Kyle M. Jacinto, RPh (Confidential File)
Electrical Properties of the Heart
• Impulse Conduction: pathways and timing• SA node—pacemaker of heart•AV node•His-Purkinje system
Adrien Kyle M. Jacinto, RPh (Confidential File)
The Electrocardiogram
•Major components of an ECG• P wave
• Depolarization in the atria
• QRS complex• Depolarization of the ventricles
• T wave• Repolarization of the ventricles
• Three other components• PR interval• QT interval• ST segment

Adrien Kyle M. Jacinto, RPh (Confidential File)

Adrien Kyle M. Jacinto, RPh (Confidential File)
Common Dysrhythmiasand Their Treatment
• Supraventricular• Impulse arises above the ventricle•Atrial flutter •Atrial fibrillation• Sustained supraventricular tachycardia (SVT)
•Ventricular• Sustained ventricular tachycardia• Ventricular fibrillation• Ventricular premature beats•Digoxin-induced ventricular dysrhythmias• Torsades de pointes

Adrien Kyle M. Jacinto, RPh (Confidential File)
Most antidysrhythmic drugs act by blocking ion channels in myocardial cells.

Adrien Kyle M. Jacinto, RPh (Confidential File)
The flow of ions through ion channels in myocardial cells

Adrien Kyle M. Jacinto, RPh (Confidential File)
Classification ofAntidysrhythmic Drugs• Vaughan Williams classification• Class I: sodium channels blockers• Class II: beta blockers• Class III: potassium channel blockers• Class IV: calcium channel blockers•Other: adenosine, digoxin, and ibutilide

Adrien Kyle M. Jacinto, RPh (Confidential File)
Class I: Sodium Channel Blockers
Membrane stabilizing agents• Class IA agents Quinidine, procainamide (Procanbid), dysopyramide (Norpace)• Class IB agentsTocainide, Mexiletine (Mexitil), Lidocaine (Xylocaine), Phenytoin (Dilantin)• Class IC agentsEncainide, Flecainide (Tambocor), Propafenone (Rythmol)• Other class I: Moricizine

Adrien Kyle M. Jacinto, RPh (Confidential File)
Class IA Agents
Quinidine, procainamide, Dysopyramide• Effects on the heart• Blocks sodium channels• Slows impulse conduction• Delays repolarization• Blocks vagal input to the heart
• Effects on the ECG•Widens the QRS complex• Prolongs the QT interval
• Therapeutic uses• Used against supraventricular and ventricular dysrhythmias

Adrien Kyle M. Jacinto, RPh (Confidential File)
Class IA Agents
• Adverse effects• Diarrhea• Cinchonism• Cardiotoxicity• Arterial embolism• Alpha-adrenergic blockade, resulting in hypotension• Hypersensitivity reactions
• Drug interactions• Digoxin

Adrien Kyle M. Jacinto, RPh (Confidential File)
Class IB Agents
Tocainide, Mexiletine, Lidocaine, Phenytoin
• Effects on the heart and ECG• Blocks cardiac sodium channels
• Slows conduction in the atria, ventricles, and His-Purkinje system
• Reduces automaticity in the ventricles and His-Purkinje system• Accelerates repolarization
• Adverse Effects• CNS effects• Drowsiness• Confusion• Paresthesias

Adrien Kyle M. Jacinto, RPh (Confidential File)
Class IC Agents
• Block cardiac sodium channels•Delay ventricular repolarization•All class IC agents can exacerbate existing dysrhythmias
and create new ones• 3 class IC agents• Encainide• Flecainide• Propafenone

Adrien Kyle M. Jacinto, RPh (Confidential File)
Moricizine
• General Class I agent• Has characteristics of all three subclasses• Used for symptomatic ventricular and life-threatening dysrhythmias

Adrien Kyle M. Jacinto, RPh (Confidential File)
Local Anesthetics (-Caine)
• Reversibly block impulse conduction along nerve axons and other excitable membranes that utilize sodium channels • Affect permeability of nerve membranes to Na ions- prevent Na ions
from entering the nerve- Cannot depolarize- particular section of the nerve cannot be stimulated

Adrien Kyle M. Jacinto, RPh (Confidential File)
Basic Pharmacology of Local AnestheticsChemistry• Lipophilic group (aromatic ring)• Intermediate chain (ester or amide)• Ionizable group (tertiary amine)

Adrien Kyle M. Jacinto, RPh (Confidential File)

Adrien Kyle M. Jacinto, RPh (Confidential File)
Basic Pharmacology of Local Anesthetics
Chemistry• Increase lipophilic character= Increase potency= Decrease metabolism= Increase toxicity

Adrien Kyle M. Jacinto, RPh (Confidential File)
2 classes
• Ester • More prone to hydrolysis• Short duration of action• Cocaine (prototype)
• Amide• More stable• Lidocaine (prototype)

Adrien Kyle M. Jacinto, RPh (Confidential File)
Specific agents
• The choice of local anesthetic for a specific procedure usually based on duration of action

Adrien Kyle M. Jacinto, RPh (Confidential File)
• Addition of a vasoconstrictor epinephrine or phenylephrine3 purpose
• Retards the removal of drug from the injection site• Prolongs the duration of action of short and intermediate action local
anesthetics• Prevent systemic toxicity
Adrien Kyle M. Jacinto, RPh (Confidential File)
Onset of action
• Can be accelerated by the use of solutions saturated with CO2 (carbonated)

Adrien Kyle M. Jacinto, RPh (Confidential File)
Repeated injection
• Can result in loss of effectiveness (e.g. tachyphylaxis) due to extracellular acidosis. • Local anesthetics are commonly marketed as hydrochloride salts (PH
4.0-6.0)

Adrien Kyle M. Jacinto, RPh (Confidential File)
Use/s
• Since local anesthetics are membrane-stabilizing drugs they are used to treat patients with neuropathic pain syndromes.• Parenteral (e.g. IV Lidocaine) and Oral (e.g. Mexiletine, Tocainide)

Adrien Kyle M. Jacinto, RPh (Confidential File)
Use/s
• Topical local anesthesia is often used for eye, ear, nose, and throat procedures and for cosmetic surgery.

Adrien Kyle M. Jacinto, RPh (Confidential File)
2 major forms of toxicity
• Direct neurotoxicity• When administered around the cord or other major nerve trunks
• Systemic effects• When absorbed from the site of administration

Adrien Kyle M. Jacinto, RPh (Confidential File)
Effects on other organs
• CNS effectsLow doses: Sleepiness, light-headedness, visual and auditory disturbances and restlessnessEarly symptoms: tongue numbness and metallic tasteHigher conc.: Nystagmus and muscular twitching, Overt tonic-clonic convulsions followed by CNS depression and death.(to avoid: premedication with benzodiazepine, e.g. oral diazepam or midazolam parenterally

Adrien Kyle M. Jacinto, RPh (Confidential File)
Seizure
• Can also be treated with small doses of thiopental, propofol, midazolam, or diazepam• The muscular manifestations of seizures can be suppressed by short
acting neuromuscular blocking agents e.g succinylcholine

Adrien Kyle M. Jacinto, RPh (Confidential File)
Neurotoxicity
• At high conc., all local anesthetics can be toxic to nerve tissue.Chlorprocaine and lidocaine• Neurotoxic when used for spinal anesthesia, producing so called
transient radicular irritation

Adrien Kyle M. Jacinto, RPh (Confidential File)
Transient radicular irritation
• This toxicity results from pooling of high conc. Of local anesthetics in the cauda equina

Adrien Kyle M. Jacinto, RPh (Confidential File)
Cardiovascular system
• Block cardiac Na channels = depress abnormal cardiac pacemaker activity, excitability and conduction• At very high concentration = blockade of Ca channels
• Severe hypotension
• Cardiovascular collapse and death• Usually occur only after large doses of 0.75% bupivacaine (most cardiotoxic)

Adrien Kyle M. Jacinto, RPh (Confidential File)
Levobupivacaine
• (S)-isomer• Appears to have lower propensity for cardiovascular toxicity than the
racemic mixture or (R)- isomer and has recently approved for clinical use

Adrien Kyle M. Jacinto, RPh (Confidential File)
Ropivacaine
• Another newer local anesthetic• Similar to bupivacaine• Available only as (s)-stereoisomer, which has inherently less affinity
for cardiac Na channel
Adrien Kyle M. Jacinto, RPh (Confidential File)
Hematologic effects
• Prilocaine (> 10mg/kg)• Metabolite = o-toluidine (oxidizing agent)
• Patients appears cyanotic and the blood chocolate colored.• Treatment:• IV administration of methylene blue or ascorbic acid

Adrien Kyle M. Jacinto, RPh (Confidential File)
Allergic reactions
• Butyrylcholinesterase/Pseudocholinesterase• Enzyme responsible for the metabolism of the ester type local anesthetics in
plasma (also in liver and glia)

Adrien Kyle M. Jacinto, RPh (Confidential File)
Local anesthetics: Ester
• Procaine HCl (Novocaine)• Used for dental procedures
• Tetracaine HCl (Pontocaine)• For spinal anesthesia
• Benzocaine• Topical for wounds and ulcers
• Dibucaine• 15-20X more potent and 15X more toxic than procaine
Adrien Kyle M. Jacinto, RPh (Confidential File)
Cocaine
• From coca leaves. “The divine plant of incas”• Sympathomimetic• Blockade of norepinephrine reuptake results in vasoconstriction and
Hypertension• May precipitate cardiac arrhythmias• Lead to ischemia

Adrien Kyle M. Jacinto, RPh (Confidential File)
Local anesthetics: Amide
• Lidocaine (Xylocaine)• Rapid and long duration of action• Causes fever and hypersensitivity reactions more than procaine• With anti-arrhythmic activity• Most neurotoxic when given as spinal anesthesia causing transient radicular
irritation

Adrien Kyle M. Jacinto, RPh (Confidential File)
Bupivacaine
• For peripheral nerve block, caudal and epidural anesthesia

Adrien Kyle M. Jacinto, RPh (Confidential File)
Seizures
• Characterized by excessive, hypersynchronous discharge of cortical neuron activity, which can be measured by electroencephalogram (EEG).

Adrien Kyle M. Jacinto, RPh (Confidential File)
Convulsions
• Violent, involuntary contractions of voluntary muscles.*A patient may have epilepsy or a seizure disorder without convulsions

Adrien Kyle M. Jacinto, RPh (Confidential File)
3 major phases of seizure:
• Prodrome- precede the seizure by hours or days. Changes in mood/behavior typically occur. Include aura subjective sensation (unusual smell, flashing light..)• Ictal phase- seizure itself. Its onset is heralded by scream or cry.• Postictal phase- after seizure. The patient typically exhibits lethargy,
confusion and behavioral changes.

Adrien Kyle M. Jacinto, RPh (Confidential File)
Epilepsy
• A chronic seizure disorder, usually recur unpredictably in the absence of consistent provoking factor.• Intermitent derangement of nervous system due to sudden,
excessive, disorderly discharge of cerebral neurons.

Adrien Kyle M. Jacinto, RPh (Confidential File)
International classification of epileptic seizures

Adrien Kyle M. Jacinto, RPh (Confidential File)
Classification based on etiology
• Primary seizure• Idiopathic. Have no identifiable cause
• Secondary seizure• Symptomatic/Acquired seizure• Occurs secondary to an identifiable cause• Intracranial neoplasms, Infectious diseases(Meningitis, measles, mumps,
syphillis, influenza, toxoplasmosis), high fever (children), congenital diseases, Metabolic disorder(hypoglycemia, hypocalcemia), Alcohol or drug withdrawal, lipid storage disorders, and developmental abnormalities.

Adrien Kyle M. Jacinto, RPh (Confidential File)
Treatment
• Therapy is aimed at control (drugs do not cure)Notable Adverse effects:• Nausea and vomiting• Drowsiness-Sedation• Ataxia• Rash• Hyponatremia• Weight gain or weight loss• Teratogenicity• osteoporosis

Adrien Kyle M. Jacinto, RPh (Confidential File)
Mechanism of Action
• Inhibition of voltage gated Na channels to slow neuron firing• Enhancement of the inhibitory effects of the neurotransmitter GABA• Inhibition of Ca channel (T-type)• Block NMDA glutamate receptors• Enhance/facilitate K channel

Adrien Kyle M. Jacinto, RPh (Confidential File)
Na Channel blockers
• Blocks voltage gated Na channel by selectively binding to the channel in the inactive state and slowing its rate of recovery• Phenytoin (Dilantin)• Fosphenytoin (Cerebyx)• Carbamazepine (Tegretol)• Oxcarbamazine (Trileptal)• Valproic acid (Valproate, Depakene, Depakote)• Lamotrigine (Lamictal)• Topiramate (Topamax)• Zonisamide (Zonegran)

Adrien Kyle M. Jacinto, RPh (Confidential File)
Phenytoin (Dilantin)
• Oldest non-sedative antiepileptic drug• DOC for partial and generalize tonic-clonic seizure• Elimination converts from 1st order elimination (proportional to its
concentration) to zero order elimination (fixed amount per unit time), usually at high therapeutic levels

Adrien Kyle M. Jacinto, RPh (Confidential File)
Phenytoin (Dilantin)
Drug interaction• Enzyme inducer
• Decrease blood levels of many medications, but increases blood levels of phenobarbital and warfarin
• Adverse effects• Dermatological: Maculopapular rash sometimes with fever, SJS, and
lupus erythematosus• Hirsutism• Acne• Gingival hyperplasia

Adrien Kyle M. Jacinto, RPh (Confidential File)
Gingival hyperplasia

Adrien Kyle M. Jacinto, RPh (Confidential File)
Phenytoin (Dilantin)
• CNS side effect: Ataxia, Dysarthria, Insomnia, Transient hyperkinesia• Decreased folic acid, thyroxine and vitamin K with long term use• Fetal Hydantoin syndrome
• Growth retardation, microencephaly, and craniofacial abnormalities (e.g. cleft palate) possibly due to epoxide metabolite of phenytoin

Adrien Kyle M. Jacinto, RPh (Confidential File)
Fosphenytoin (Cerebyx)
• Prodrug• Converted to phenytoin in blood• Administered IM/IV
Phenytoin Na never given IM= can cause tissue damage and necrosis

Adrien Kyle M. Jacinto, RPh (Confidential File)
Congeners of Phenytoin
• Mephenytoin (Mesantoin)• Norvanol – Metabolite that contributes most of antiseizure activity of
mephenytoin
• Ethotoin (Peganone)• Phenacemide
Adrien Kyle M. Jacinto, RPh (Confidential File)
Carbamazepine (Tegretol)
• TCA (Bipolar)• First choice for complex partial and generalized tonic clonic seizuresContraindicatiobs:• May exacerbate absence or myoclonic seizureAdverse effects:• Common: Diplopia and ataxia, GI disturbances, sedation

Adrien Kyle M. Jacinto, RPh (Confidential File)
Carbamazepine (Tegretol)
• Drug interactions:• Enzyme inducer• Exhibits autoinduction (It Metabolize itself)

Adrien Kyle M. Jacinto, RPh (Confidential File)
Oxcarbazepine (Trileptal)
• For primary and secondarily generalize tonic clonic seizure• Prodrug.• Half life: 1-2 hour• Fewer adverse effects than CBZ, Phenytoin

Adrien Kyle M. Jacinto, RPh (Confidential File)
Eslicarbazine (Stedesa)
• Prodrug• Advantage: Once daily dosing regimen

Adrien Kyle M. Jacinto, RPh (Confidential File)
Valproic acid (Depakote)• Other MOA:
• Inhibition of T-type Ca channel• Increases GABA production and Decreases GABA metabolism (Inhibition of GABA
transaminase)
• Indication:• Simple or complex partial, and primary generalize tonic clonic.• Highly effective for photosensitive epilepsy and juvenile myoclonic epilepsy
• Contraindication:• Liver disease

Adrien Kyle M. Jacinto, RPh (Confidential File)
Valproic acid (Depakote)
• Drug interaction:• Enzyme inhibitor
• Adverse effects:• Weight gain• Hair loss• Ankle swelling

Adrien Kyle M. Jacinto, RPh (Confidential File)
Lamotrigine (Lamictal)
Other MOA:• Inhibits voltage gated Ca channel (N and P/Q type)• May inhibit release glutamateIndications:• Adjunct therapy
• for simple and complex partial seizure• Generalized seizures of Lennox- Gestaut syndrome
• Contraindications:• Make myoclonic seizure worse

Adrien Kyle M. Jacinto, RPh (Confidential File)
Lennox Gestaut syndrome
• Most distressing childhood epilepsy (Movement disorder)• Frequent fits and gradual mental retardationAdverse effects:• Rash (10%)• Increased alertness

Adrien Kyle M. Jacinto, RPh (Confidential File)
Topiramate (Topamax)
• Other MOA:• Ebhances post-synaptic GABAA Receptor currents• Kainate receptor antagonists (blocks certain type of glutamate channel)
• Indications:• Adjunct therapy for partial and primary generalized.• Decreases tonic and atonic seizures in children with Lennox Gestaut
syndrome

Adrien Kyle M. Jacinto, RPh (Confidential File)
Topiramate (Topamax)
• Adverse effects:Weight lossMetabolic acidosisKidney stone formation• Contraindication:History of kidney stone• Drug interaction
• Enzyme inducer interact with it.

Adrien Kyle M. Jacinto, RPh (Confidential File)
Zonisamide (Sonegran)
• Sulfonamide derivative. Broad spectrum• Other MOA:
• Inhibits T-type Ca channels• Binds to GABA receptor• Facilitates dopaminergic and serotonergic neurotransmission
• Indications:• Adjunct treatment of partial seizure in adults• Broad spectrum:
• Myoclonic seizure• Infantile spasm• Generalized and atypycal absense seizure• Lennox Gestaut seizure

Adrien Kyle M. Jacinto, RPh (Confidential File)
Zonisamide (Sonegran)
Drug interactions:• Phenytoin and Carbamazepine decrease its half life by halfAdverse effects:• Weight loss (Inc. serotonin levels)

Adrien Kyle M. Jacinto, RPh (Confidential File)
Lacosamide (Vimpat)
• Amino acid related compound• Also binds to collapsin-response mediator protein (CRMP) thereby
blocking the effect of neurotropic factors such as BDNF and NT3 on axonal and dendritic growth

Adrien Kyle M. Jacinto, RPh (Confidential File)
Rufinamide (Banzel)
• Triazole derivative• Prolong the inactive state of Na channel• Adjunct for Lennox Gestaut syndrome

Adrien Kyle M. Jacinto, RPh (Confidential File)
Others
Tetrodotoxin• From Puffer fishBetrachotoxin • From Colombian frog
MOA: Block the Na channelResponse: Hyperpolarization (Inactivation of neurons)