smoking and alcohol consumption in relation to risk of thyroid cancer in postmenopausal women
TRANSCRIPT
Cancer Epidemiology 36 (2012) 335–340
Smoking and alcohol consumption in relation to risk of thyroid cancer inpostmenopausal women
Geoffrey C. Kabat a,*, Mimi Y. Kim a, Jean Wactawski-Wende b, Thomas E. Rohan a
a Department of Epidemiology and Population Health, Albert Einstein College of Medicine, Bronx, NY, United Statesb Department of Social and Preventive Medicine, School of Public Health and Health Professions, University at Buffalo, Buffalo, NY, United States
A R T I C L E I N F O
Article history:
Received 23 November 2011
Received in revised form 29 February 2012
Accepted 21 March 2012
Available online 22 April 2012
Keywords:
Thyroid carcinoma
Papillary type
Smoking
Alcohol consumption
Postmenopausal women
A B S T R A C T
Background: Few cohort studies have examined smoking and alcohol consumption in relation to risk of
thyroid cancer, and their findings are conflicting. Methods: We therefore assessed the association of
smoking and alcohol intake with risk of thyroid cancer in a cohort of 159,340 women enrolled in the
Women’s Health Initiative. Over 12.7 years of follow-up 331 cases of thyroid cancer, of which 276 were
papillary thyroid cancer, were identified. Cox proportional hazards models were used to estimate hazard
ratios (HR) and 95% confidence intervals (CI). Results: Compared to never smokers, ever smokers did not
have altered risk. Current smokers had reduced risk for all thyroid cancer (HR 0.54, 95% CI 0.29–1.00) and
for papillary thyroid cancer (HR 0.34, 95% CI 0.15–0.78); however, the number of current smokers among
cases was small. No associations or trends were seen for amount smoked, age of starting smoking, or age
at quitting. Smokers of �40 pack-years had a significantly reduced risk of papillary thyroid cancer (HR
0.44, 95% CI 0.21–0.89). In contrast, women who had smoked for < 20 years had increased risk of thyroid
cancer (HR 1.35, 95% CI 1.05–1.74) and papillary cancer (HR 1.43, 95% CI 1.09–1.89). Alcohol intake was
not associated with risk. Conclusion: Our findings suggest that current smoking and having higher pack-
years of exposure are associated with a modestly reduced risk of thyroid cancer, whereas alcohol
consumption does not appear to affect risk.
� 2012 Elsevier Ltd. All rights reserved.
Contents lists available at SciVerse ScienceDirect
Cancer EpidemiologyThe International Journal of Cancer Epidemiology, Detection, and Prevention
jou r nal h o mep age: w ww.c an cer ep idem io log y.n et
Although relatively rare, thyroid cancer is the most commoncancer of the endocrine system and is the eighth most commoncancer in women [1]. Little is known about the causes of thismalignancy, aside from the well-established association withexposure to ionizing radiation [1]. While there is a strong andconsistent association between benign thyroid conditions (goiterand nodules) and risk of thyroid cancer [1–4], it is unclear whetherthis reflects a true causal relationship, an effect of treatment for thebenign disease, common risk factors for the benign conditions andfor cancer, more intense medical surveillance for those with benignconditions, or misdiagnosis of the benign condition [1].
A number of studies have examined cigarette smoking andalcohol consumption in relation to risk of thyroid cancer. Many ofthese studies have provided some evidence of inverse associationswith smoking [5–9]. However, others have shown either norelationship [4,10–13] or a positive association with smoking[3,14]. Most of the studies to date have been case–control studies
* Corresponding author at: Department of Epidemiology and Population Health,
Albert Einstein College of Medicine, 1300 Morris Park Avenue, Bronx, NY 10461,
United States. Tel.: +1 718 430 3038; fax: +1 718 430 8653.
E-mail addresses: [email protected], [email protected]
(G.C. Kabat).
1877-7821/$ – see front matter � 2012 Elsevier Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.canep.2012.03.013
[3–10,12,14,15], some of which had limited information onexposure to cigarette smoke [3,4,14]. Of the three cohort studies[2,11,13], only one provided evidence of an inverse relationship[2], whereas the remaining two found no association [11,13]. Aninverse association of alcohol consumption has also been reported[9,16,17], but most studies have found no association [2,4,10–13],and there is some question as to whether the associations withalcohol that have been observed were due to confounding bysmoking [8].
In several cohort studies that examined the role of cigarettesmoking or alcohol consumption in relation to risk of thyroidcancer the range of ages at enrollment was narrow (only 15–20years [13,16,17]). We therefore examined these associations in aprospective study in the 161,808 postmenopausal women with a30-year age range enrolled in the Women’s Health Initiative (WHI).
1. Methods
The Women’s Health Initiative (WHI) is a large, multi-center,multi-faceted study designed to advance understanding of thedeterminants of major chronic diseases in postmenopausal women.It is composed of a Clinical Trial component (CT, N = 68,132) and anObservational Study component (OS, N = 93,676) [18]. The clinicaltrial component included three randomized controlled intervention

G.C. Kabat et al. / Cancer Epidemiology 36 (2012) 335–340336
studies: hormone therapy, low-fat diet modification and cal-cium + vitamin D supplementation. Women between the ages of50 and 79 and representing major racial/ethnic groups wererecruited from the general population at 40 clinical centersthroughout the United States between 1993 and 1998. Details ofthe design and reliability of the baseline measures have beenpublished [18,19].
1.1. Data collection and variable definition
At study entry, self-administered questionnaires were used tocollect information on demographics, medical, reproductive andfamily history, and on dietary and lifestyle factors, includingsmoking history and alcohol consumption. Information onsmoking habits at baseline included whether subjects had eversmoked (at least 100 cigarettes) and, for those who had eversmoked, age at starting to smoke regularly (9 categories), whetheror not they were current smokers (yes/no), age at quitting (formersmokers—11 categories), number of cigarettes smoked per day(both current and former smokers—7 categories), and number ofyears of smoking (7 categories).
In order to characterize alcohol consumption, informationobtained from two different questionnaires was combined. In ahealth habits questionnaire administered at baseline, womenwere asked whether they had ever consumed at least 12 drinksof any alcoholic beverage over their lifetime and whether theystill drank alcohol. In addition, in the food frequency question-naire (FFQ) completed at baseline, women were asked abouttheir intake of beer, wine, and hard liquor during the past 3months. Frequency categories for number of servings were asfollows: never or less than once per month, 1–3 per month, 1 perweek, 2–4 per week, 5–6 per week, 1 per day, 2–3 per day, 4–5per day, and 6 per day. Serving size was also queried. A mediumserving was defined as a 12-oz can or bottle of beer, 6-oz glass ofwine, or 1 shot (1.5 oz) of hard liquor. In a validation studycarried out in a subsample of 113 participants, the Pearsoncorrelation coefficient between alcohol intake assessed by theFFQ versus an 8-day dietary intake diary (four 24-h recalls and a4-day food record) was 0.89 [20]. Based on information from thetwo questionnaires, two variables were created to describe totalalcohol intake: frequency of intake (nondrinker [never-drinker,past drinker, or <1 drink per month]; <1 drink per week, 1–7drinks per week, and �7 drinks per week) and level of alcoholintake in grams per day (nondrinker: >0–<1; 1–<4; �4). Inaddition, we examined the frequency and quantity of intake ofspecific alcoholic beverages.
Clinical outcomes (including new cancer diagnoses) wereupdated semi-annually in the CT and annually in the OS usingin-person, mailed, or telephone questionnaires. Self-reports ofthyroid cancer were verified by centralized review of medicalrecords and pathology reports by trained physician adjudicators[21]. As of 30 September 2010, a total of 343 incident cases ofthyroid cancer had been diagnosed among the 161,808 partici-pants in the OS and CT after a median of 12.7 years of follow-up.The proportion of the cohort that was lost to follow-up was lessthan 1%.
For the analyses reported here, we excluded women withmissing information on smoking status (N = 2126, including 8cases) or alcohol intake (N = 342, including 4 cases), leaving 331cases and 159,009 non-cases for analysis. Histology was catego-rized according to the ICD-O-3 as follows: papillary (8050/3, 8260/3, 8340/3), follicular (8290/3, 8330/3, 8331/3, 8332/3), medullary(8510/3), anaplastic (8021/3), carcinoma NOS (8010/3), and other(8030/3, 8032/3). The breakdown of cases by histologic type was asfollows: papillary 276, follicular 36, anaplastic 6, medullary 10,other 3.
1.2. Statistical analysis
Cox proportional hazards models were used to estimate hazardratios (HRs) and 95% confidence intervals (95% CI) for theassociations of smoking and alcohol intake with risk of all thyroidcases (N = 331) and papillary thyroid tumors (N = 276) with days toevent as the time scale (from date of enrollment to date ofdiagnosis (for cases), or death, withdrawal from the study, or end offollow-up (for non-cases)). We computed both age-adjusted andmultivariable adjusted HRs and 95% confidence intervals. Each of 6smoking variables (smoking status, number of cigarettes smokedper day, age at starting smoking, duration of smoking, pack-years,and years since quitting) was assessed in separate models. Becausethe number of cases who were current smokers was small, we tooknever smokers as the reference category for years since quittingand ordered subjects by decreasing years since quitting in order tocompute a trend statistic. Lifetime pack-years of cigarette smokingwere computed by multiplying the midpoint of the smokingfrequency interval by the midpoint of the duration interval anddividing the product by 20.
Variables were selected for inclusion in the multivariablemodels based on whether their inclusion altered the parameterestimate for the exposure of interest by >10%, or if, based on theliterature, they were established risk factors (history of benignthyroid conditions). The following variables were considered forinclusion as covariates: age, education, ethnicity, age at menarche,body mass index, height, age at first live birth, parity, age atmenopause, oral contraceptive use, hormone therapy, physicalactivity, and history of benign thyroid conditions. The followingcovariates were included in the final multivariable models: age(continuous), age at first live birth (<20, 20–29, �30, missing),education (less than high school graduate, high school graduate/some college, college graduate, post-college), height (continuous),history of benign thyroid disease (goiter, nodules – yes, no), andenrollment in the OS/treatment arm assignment in each of the 3CTs (hormone therapy, calcium plus vitamin D, and dietarymodification). Models assessing smoking parameters additionallyincluded alcohol as a covariate and models assessing alcoholincluded pack-years of smoking as a covariate. For alcohol, weexamined the associations of both total alcohol intake and intake ofbeer, wine, and hard liquor separately with risk of thyroid cancer.For categorical variables, tests for trend were performed byassigning the median value to each category and modeling thisvariable as a continuous variable. We tested for departure fromlinearity for smoking variables using a likelihood ratio test tocompare the model with the categorical variable and that with thecontinuous variable. We formally tested for interactions betweenalcohol intake (nondrinker, >0–<4 g/day, �4 g/day) and smoking(never, >0–20 pack-years, �20 pack-years) and thyroid cancer riskby comparing the fit of models with and without the product termsrepresenting the variables of interest using a likelihood ratio test.We also carried out four sensitivity analyses: (1) excluding the first3 years of follow-up of the entire cohort; (2) excluding women whoreported any cancer diagnosis prior to enrollment; (3) excludingwomen with a history of nodules/goiter; and (4) repeating themain analyses for localized thyroid cancer to take into accountpossible bias due to screening. All analyses were performing usingSAS (version 9.1, Cary, NC). All P values are two-sided.
2. Results
At baseline, compared to non-cases, thyroid cancer cases weresignificantly younger, taller, had lower alcohol intake, and greaterfrequency of thyroid nodules and goiter (Table 1). Other factorsdiffered little between the two groups. The distribution of cases by
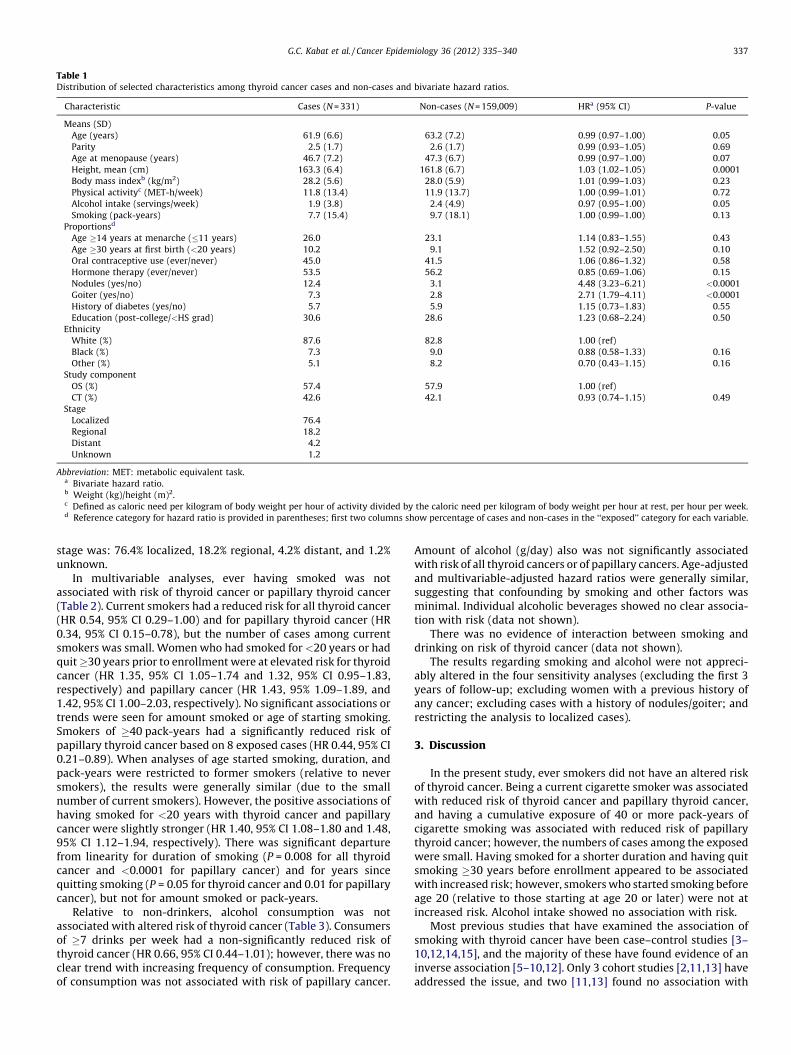
Table 1Distribution of selected characteristics among thyroid cancer cases and non-cases and bivariate hazard ratios.
Characteristic Cases (N = 331) Non-cases (N = 159,009) HRa (95% CI) P-value
Means (SD)
Age (years) 61.9 (6.6) 63.2 (7.2) 0.99 (0.97–1.00) 0.05
Parity 2.5 (1.7) 2.6 (1.7) 0.99 (0.93–1.05) 0.69
Age at menopause (years) 46.7 (7.2) 47.3 (6.7) 0.99 (0.97–1.00) 0.07
Height, mean (cm) 163.3 (6.4) 161.8 (6.7) 1.03 (1.02–1.05) 0.0001
Body mass indexb (kg/m2) 28.2 (5.6) 28.0 (5.9) 1.01 (0.99–1.03) 0.23
Physical activityc (MET-h/week) 11.8 (13.4) 11.9 (13.7) 1.00 (0.99–1.01) 0.72
Alcohol intake (servings/week) 1.9 (3.8) 2.4 (4.9) 0.97 (0.95–1.00) 0.05
Smoking (pack-years) 7.7 (15.4) 9.7 (18.1) 1.00 (0.99–1.00) 0.13
Proportionsd
Age �14 years at menarche (�11 years) 26.0 23.1 1.14 (0.83–1.55) 0.43
Age �30 years at first birth (<20 years) 10.2 9.1 1.52 (0.92–2.50) 0.10
Oral contraceptive use (ever/never) 45.0 41.5 1.06 (0.86–1.32) 0.58
Hormone therapy (ever/never) 53.5 56.2 0.85 (0.69–1.06) 0.15
Nodules (yes/no) 12.4 3.1 4.48 (3.23–6.21) <0.0001
Goiter (yes/no) 7.3 2.8 2.71 (1.79–4.11) <0.0001
History of diabetes (yes/no) 5.7 5.9 1.15 (0.73–1.83) 0.55
Education (post-college/<HS grad) 30.6 28.6 1.23 (0.68–2.24) 0.50
Ethnicity
White (%) 87.6 82.8 1.00 (ref)
Black (%) 7.3 9.0 0.88 (0.58–1.33) 0.16
Other (%) 5.1 8.2 0.70 (0.43–1.15) 0.16
Study component
OS (%) 57.4 57.9 1.00 (ref)
CT (%) 42.6 42.1 0.93 (0.74–1.15) 0.49
Stage
Localized 76.4
Regional 18.2
Distant 4.2
Unknown 1.2
Abbreviation: MET: metabolic equivalent task.a Bivariate hazard ratio.b Weight (kg)/height (m)2.c Defined as caloric need per kilogram of body weight per hour of activity divided by the caloric need per kilogram of body weight per hour at rest, per hour per week.d Reference category for hazard ratio is provided in parentheses; first two columns show percentage of cases and non-cases in the ‘‘exposed’’ category for each variable.
G.C. Kabat et al. / Cancer Epidemiology 36 (2012) 335–340 337
stage was: 76.4% localized, 18.2% regional, 4.2% distant, and 1.2%unknown.
In multivariable analyses, ever having smoked was notassociated with risk of thyroid cancer or papillary thyroid cancer(Table 2). Current smokers had a reduced risk for all thyroid cancer(HR 0.54, 95% CI 0.29–1.00) and for papillary thyroid cancer (HR0.34, 95% CI 0.15–0.78), but the number of cases among currentsmokers was small. Women who had smoked for <20 years or hadquit �30 years prior to enrollment were at elevated risk for thyroidcancer (HR 1.35, 95% CI 1.05–1.74 and 1.32, 95% CI 0.95–1.83,respectively) and papillary cancer (HR 1.43, 95% 1.09–1.89, and1.42, 95% CI 1.00–2.03, respectively). No significant associations ortrends were seen for amount smoked or age of starting smoking.Smokers of �40 pack-years had a significantly reduced risk ofpapillary thyroid cancer based on 8 exposed cases (HR 0.44, 95% CI0.21–0.89). When analyses of age started smoking, duration, andpack-years were restricted to former smokers (relative to neversmokers), the results were generally similar (due to the smallnumber of current smokers). However, the positive associations ofhaving smoked for <20 years with thyroid cancer and papillarycancer were slightly stronger (HR 1.40, 95% CI 1.08–1.80 and 1.48,95% CI 1.12–1.94, respectively). There was significant departurefrom linearity for duration of smoking (P = 0.008 for all thyroidcancer and <0.0001 for papillary cancer) and for years sincequitting smoking (P = 0.05 for thyroid cancer and 0.01 for papillarycancer), but not for amount smoked or pack-years.
Relative to non-drinkers, alcohol consumption was notassociated with altered risk of thyroid cancer (Table 3). Consumersof �7 drinks per week had a non-significantly reduced risk ofthyroid cancer (HR 0.66, 95% CI 0.44–1.01); however, there was noclear trend with increasing frequency of consumption. Frequencyof consumption was not associated with risk of papillary cancer.
Amount of alcohol (g/day) also was not significantly associatedwith risk of all thyroid cancers or of papillary cancers. Age-adjustedand multivariable-adjusted hazard ratios were generally similar,suggesting that confounding by smoking and other factors wasminimal. Individual alcoholic beverages showed no clear associa-tion with risk (data not shown).
There was no evidence of interaction between smoking anddrinking on risk of thyroid cancer (data not shown).
The results regarding smoking and alcohol were not appreci-ably altered in the four sensitivity analyses (excluding the first 3years of follow-up; excluding women with a previous history ofany cancer; excluding cases with a history of nodules/goiter; andrestricting the analysis to localized cases).
3. Discussion
In the present study, ever smokers did not have an altered riskof thyroid cancer. Being a current cigarette smoker was associatedwith reduced risk of thyroid cancer and papillary thyroid cancer,and having a cumulative exposure of 40 or more pack-years ofcigarette smoking was associated with reduced risk of papillarythyroid cancer; however, the numbers of cases among the exposedwere small. Having smoked for a shorter duration and having quitsmoking �30 years before enrollment appeared to be associatedwith increased risk; however, smokers who started smoking beforeage 20 (relative to those starting at age 20 or later) were not atincreased risk. Alcohol intake showed no association with risk.
Most previous studies that have examined the association ofsmoking with thyroid cancer have been case–control studies [3–10,12,14,15], and the majority of these have found evidence of aninverse association [5–10,12]. Only 3 cohort studies [2,11,13] haveaddressed the issue, and two [11,13] found no association with
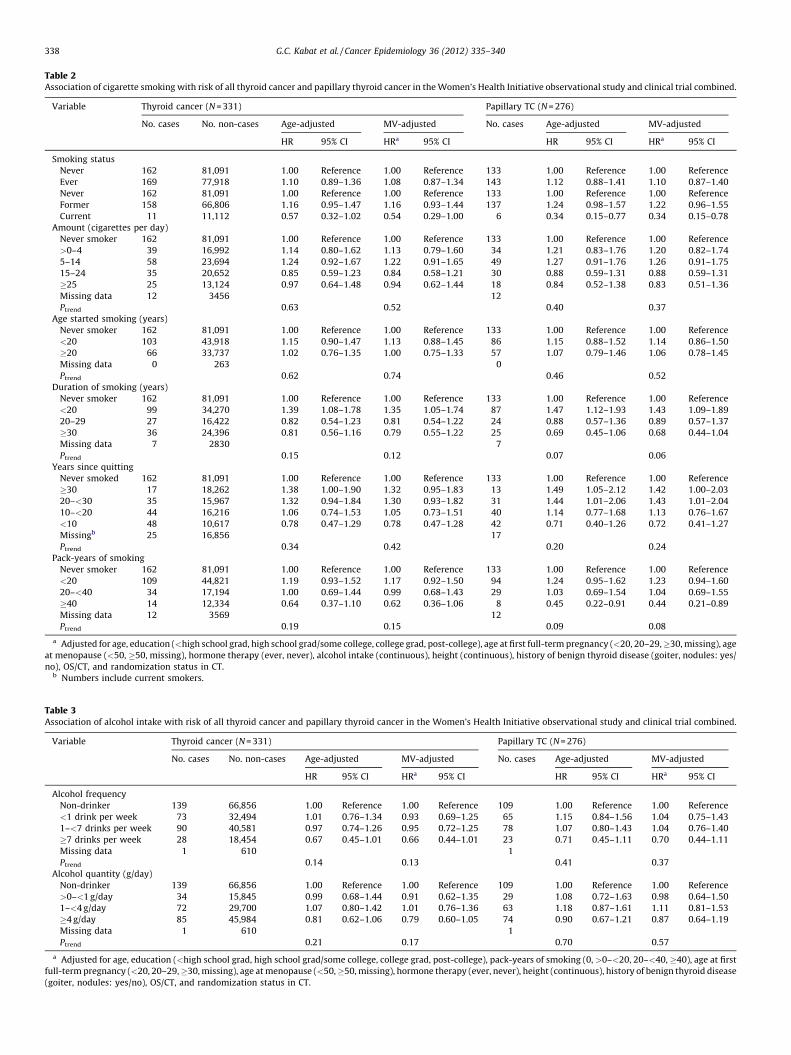
Table 2Association of cigarette smoking with risk of all thyroid cancer and papillary thyroid cancer in the Women’s Health Initiative observational study and clinical trial combined.
Variable Thyroid cancer (N = 331) Papillary TC (N = 276)
No. cases No. non-cases Age-adjusted MV-adjusted No. cases Age-adjusted MV-adjusted
HR 95% CI HRa 95% CI HR 95% CI HRa 95% CI
Smoking status
Never 162 81,091 1.00 Reference 1.00 Reference 133 1.00 Reference 1.00 Reference
Ever 169 77,918 1.10 0.89–1.36 1.08 0.87–1.34 143 1.12 0.88–1.41 1.10 0.87–1.40
Never 162 81,091 1.00 Reference 1.00 Reference 133 1.00 Reference 1.00 Reference
Former 158 66,806 1.16 0.95–1.47 1.16 0.93–1.44 137 1.24 0.98–1.57 1.22 0.96–1.55
Current 11 11,112 0.57 0.32–1.02 0.54 0.29–1.00 6 0.34 0.15–0.77 0.34 0.15–0.78
Amount (cigarettes per day)
Never smoker 162 81,091 1.00 Reference 1.00 Reference 133 1.00 Reference 1.00 Reference
>0–4 39 16,992 1.14 0.80–1.62 1.13 0.79–1.60 34 1.21 0.83–1.76 1.20 0.82–1.74
5–14 58 23,694 1.24 0.92–1.67 1.22 0.91–1.65 49 1.27 0.91–1.76 1.26 0.91–1.75
15–24 35 20,652 0.85 0.59–1.23 0.84 0.58–1.21 30 0.88 0.59–1.31 0.88 0.59–1.31
�25 25 13,124 0.97 0.64–1.48 0.94 0.62–1.44 18 0.84 0.52–1.38 0.83 0.51–1.36
Missing data 12 3456 12
Ptrend 0.63 0.52 0.40 0.37
Age started smoking (years)
Never smoker 162 81,091 1.00 Reference 1.00 Reference 133 1.00 Reference 1.00 Reference
<20 103 43,918 1.15 0.90–1.47 1.13 0.88–1.45 86 1.15 0.88–1.52 1.14 0.86–1.50
�20 66 33,737 1.02 0.76–1.35 1.00 0.75–1.33 57 1.07 0.79–1.46 1.06 0.78–1.45
Missing data 0 263 0
Ptrend 0.62 0.74 0.46 0.52
Duration of smoking (years)
Never smoker 162 81,091 1.00 Reference 1.00 Reference 133 1.00 Reference 1.00 Reference
<20 99 34,270 1.39 1.08–1.78 1.35 1.05–1.74 87 1.47 1.12–1.93 1.43 1.09–1.89
20–29 27 16,422 0.82 0.54–1.23 0.81 0.54–1.22 24 0.88 0.57–1.36 0.89 0.57–1.37
�30 36 24,396 0.81 0.56–1.16 0.79 0.55–1.22 25 0.69 0.45–1.06 0.68 0.44–1.04
Missing data 7 2830 7
Ptrend 0.15 0.12 0.07 0.06
Years since quitting
Never smoked 162 81,091 1.00 Reference 1.00 Reference 133 1.00 Reference 1.00 Reference
�30 17 18,262 1.38 1.00–1.90 1.32 0.95–1.83 13 1.49 1.05–2.12 1.42 1.00–2.03
20–<30 35 15,967 1.32 0.94–1.84 1.30 0.93–1.82 31 1.44 1.01–2.06 1.43 1.01–2.04
10–<20 44 16,216 1.06 0.74–1.53 1.05 0.73–1.51 40 1.14 0.77–1.68 1.13 0.76–1.67
<10 48 10,617 0.78 0.47–1.29 0.78 0.47–1.28 42 0.71 0.40–1.26 0.72 0.41–1.27
Missingb 25 16,856 17
Ptrend 0.34 0.42 0.20 0.24
Pack-years of smoking
Never smoker 162 81,091 1.00 Reference 1.00 Reference 133 1.00 Reference 1.00 Reference
<20 109 44,821 1.19 0.93–1.52 1.17 0.92–1.50 94 1.24 0.95–1.62 1.23 0.94–1.60
20–<40 34 17,194 1.00 0.69–1.44 0.99 0.68–1.43 29 1.03 0.69–1.54 1.04 0.69–1.55
�40 14 12,334 0.64 0.37–1.10 0.62 0.36–1.06 8 0.45 0.22–0.91 0.44 0.21–0.89
Missing data 12 3569 12
Ptrend 0.19 0.15 0.09 0.08
a Adjusted for age, education (<high school grad, high school grad/some college, college grad, post-college), age at first full-term pregnancy (<20, 20–29, �30, missing), age
at menopause (<50, �50, missing), hormone therapy (ever, never), alcohol intake (continuous), height (continuous), history of benign thyroid disease (goiter, nodules: yes/
no), OS/CT, and randomization status in CT.b Numbers include current smokers.
Table 3Association of alcohol intake with risk of all thyroid cancer and papillary thyroid cancer in the Women’s Health Initiative observational study and clinical trial combined.
Variable Thyroid cancer (N = 331) Papillary TC (N = 276)
No. cases No. non-cases Age-adjusted MV-adjusted No. cases Age-adjusted MV-adjusted
HR 95% CI HRa 95% CI HR 95% CI HRa 95% CI
Alcohol frequency
Non-drinker 139 66,856 1.00 Reference 1.00 Reference 109 1.00 Reference 1.00 Reference
<1 drink per week 73 32,494 1.01 0.76–1.34 0.93 0.69–1.25 65 1.15 0.84–1.56 1.04 0.75–1.43
1–<7 drinks per week 90 40,581 0.97 0.74–1.26 0.95 0.72–1.25 78 1.07 0.80–1.43 1.04 0.76–1.40
�7 drinks per week 28 18,454 0.67 0.45–1.01 0.66 0.44–1.01 23 0.71 0.45–1.11 0.70 0.44–1.11
Missing data 1 610 1
Ptrend 0.14 0.13 0.41 0.37
Alcohol quantity (g/day)
Non-drinker 139 66,856 1.00 Reference 1.00 Reference 109 1.00 Reference 1.00 Reference
>0–<1 g/day 34 15,845 0.99 0.68–1.44 0.91 0.62–1.35 29 1.08 0.72–1.63 0.98 0.64–1.50
1–<4 g/day 72 29,700 1.07 0.80–1.42 1.01 0.76–1.36 63 1.18 0.87–1.61 1.11 0.81–1.53
�4 g/day 85 45,984 0.81 0.62–1.06 0.79 0.60–1.05 74 0.90 0.67–1.21 0.87 0.64–1.19
Missing data 1 610 1
Ptrend 0.21 0.17 0.70 0.57
a Adjusted for age, education (<high school grad, high school grad/some college, college grad, post-college), pack-years of smoking (0, >0–<20, 20–<40, �40), age at first
full-term pregnancy (<20, 20–29, �30, missing), age at menopause (<50, �50, missing), hormone therapy (ever, never), height (continuous), history of benign thyroid disease
(goiter, nodules: yes/no), OS/CT, and randomization status in CT.
G.C. Kabat et al. / Cancer Epidemiology 36 (2012) 335–340338

G.C. Kabat et al. / Cancer Epidemiology 36 (2012) 335–340 339
cigarette smoking. Consistent with the results of most case–control studies and with those of the cohort study of Meinholdet al. [2], we observed an inverse association of being a currentsmoker with risk, with a suggestion that greater duration ofsmoking or greater pack-years were associated with reduced risk.However, these associations were based on small numbers ofexposed women and may be chance findings. There was evidenceof significant departure from linearity for duration of smoking andyears since quitting but not for amount smoked or pack-years.Interpretation of the smoking results is challenging in view of theinconsistency among different variables. Although there was asuggestion of an increased risk among smokers of <20 yearsduration and smokers who had quit �30 years prior to enrollment,an early age of starting smoking did not confer increased risk.Previous studies are not suggestive of an increased risk amongformer smokers or smokers who quit at a relatively early age[2,7–10,12,13].
Although smoking has mostly been associated with anincrease in risk of various diseases, inverse associations ofsmoking have been consistently observed with risk of endome-trial cancer [22] and Parkinson’s disease [23]. The inverseassociation of smoking with thyroid cancer, if real, may beexplained by the lower levels of thyroid stimulating hormone(TSH) among current smokers compared to never or formersmokers [24,25], since TSH is involved in the regulation ofgrowth and differentiation of thyroid cells [26]. However, theroles of TSH in thyroid carcinogenesis have not been establishedin prospective studies.
Two recent cohort studies [16,17] have reported that alcoholintake is associated with reduced risk of thyroid cancer, with riskestimates for thyroid cancer of 0.55 (95% CI 0.31–0.95) for womenconsuming �1 drink per day [17] and of 0.54 (95% CI 0.31–0.92) forwomen consuming �15 drinks per week [16] relative tonondrinkers, after adjustment for smoking. Two case–controlstudies [9,10] showed suggestive evidence that drinkers were atdecreased risk; however, there was no evidence of a trend withincreasing consumption. In contrast, three cohort studies [2,11,13]and two other case–control studies [4,12] showed no association.In a pooled analysis of 10 case–control studies [8], alcohol showedan inverse association with risk of thyroid cancer beforeadjustment for smoking; however, after adjustment the associa-tion was attenuated and no longer statistically significant. It shouldbe pointed out that, even in the two large cohort studies [16,17] thenumber of cases in the highest drinking category was small (Nconsuming �1 drink per day = 16 [17] and N consuming �15drinks per week = 13 [16]).
In the present study, there was a non-significant reduction inrisk of thyroid cancer among consumers of �7 drinks per week;however, there was no clear trend with increasing frequency orwith increasing amount consumed. The results were not materiallydifferent before and after adjustment for pack-years of smoking.The proportion of women in WHI consuming �7 drinks per week isonly 12%, and therefore this study is not informative about theeffects of heavy drinking. Furthermore, we only had informationabout alcohol consumption at baseline, and drinking habits mayhave changed over the follow-up period, resulting in misclassifi-cation of exposure. The association was unchanged in thesensitivity analyses.
There was only a weak correlation between smoking (numberof cigarettes smoked per day) and drinking (either number ofdrinks per week or grams of alcohol per day): r = 0.165 and 0.167,respectively. This low correlation is likely due in part to the smallproportion of current smokers and to the small proportion of heavydrinkers in this population.
The lack of consistency in the results of different studiesregarding the associations of smoking and drinking with risk of
thyroid cancer may be due to a number of factors, including studydesign, differences in the age distribution of the study populations,adjustment for different covariates, and under-reporting ofexposure, particularly of alcohol intake [27,28].
The present study has a number of strengths, including itsprospective nature, the central adjudication of thyroid cancerdiagnoses, a substantial number of cases, information on cell type,relatively detailed information on smoking and drinking, avail-ability of information on wide range of potential confoundingvariables (including a history of benign thyroid conditions), andthe high degree of completeness of follow-up. Based on oursensitivity analyses, the observed associations did not appear to bedue to the inclusion of cases who may have developed disease priorto enrollment; to the inclusion of women with a prior history ofcancer; to a history of nodules/goiter; or to differences in stage ofdisease by smoking status.
Among the limitations of our study is the fact that it wasrestricted to postmenopausal women, and for this reason is notrepresentative of all thyroid cancers among women, which have amedian age at diagnosis of 46 years [1] and whose distribution byhistology differs by age: cases of papillary thyroid cancer tend tobe younger and cases of follicular carcinoma tend to be somewhatolder [1]. Thus, our results are only pertinent to thyroid canceroccurring in postmenopausal women. In addition, the numbers ofcurrent smokers and heavy alcohol consumers among cases weresmall. Finally, due to the small number of cases of follicularthyroid cancer, we were unable to examine associations with thiscell type.
In conclusion, in this prospective cohort study of postmeno-pausal women, ever smoking was not associated with risk ofthyroid cancer in postmenopausal women. Being a current smokerand/or having high pack-years of exposure was associated withmodestly reduced risk of thyroid cancer; however the numbers inthese categories were small and estimates may be unstable.Alcohol consumption was not associated with risk.
Conflict of interest statement
All authors state that they have no conflicts-of-interest that arepertinent to this work.
Acknowledgments
Short list of WHI investigatorsProgram Office: (National Heart, Lung, and Blood Institute,
Bethesda, Maryland) Jacques Rossouw, Shari Ludlam, Dale Burwen,Joan McGowan, Leslie Ford, and Nancy Geller.
Clinical Coordinating Center: (Fred Hutchinson Cancer ResearchCenter, Seattle, WA) Garnet Anderson, Ross Prentice, AndreaLaCroix, and Charles Kooperberg.
Investigators and Academic Centers: (Brigham and Women’sHospital, Harvard Medical School, Boston, MA) JoAnn E. Manson;(MedStar Health Research Institute/Howard University,Washington, DC) Barbara V. Howard; (Stanford PreventionResearch Center, Stanford, CA) Marcia L. Stefanick; (The OhioState University, Columbus, OH) Rebecca Jackson; (University ofArizona, Tucson/Phoenix, AZ) Cynthia A. Thomson; (Universityat Buffalo, Buffalo, NY) Jean Wactawski-Wende; (University ofFlorida, Gainesville/Jacksonville, FL) Marian Limacher; (Univer-sity of Iowa, Iowa City/Davenport, IA) Robert Wallace; (Univer-sity of Pittsburgh, Pittsburgh, PA) Lewis Kuller; (Wake ForestUniversity School of Medicine, Winston-Salem, NC) Sally Shu-maker.
Women’s Health Initiative Memory Study: (Wake Forest Univer-sity School of Medicine, Winston-Salem, NC) Sally Shumaker.
G.C. Kabat et al. / Cancer Epidemiology 36 (2012) 335–340340
References
[1] Ron E, Schneider AB. Thyroid cancer. In: Schottenfeld D, Fraumeni Jr JF, eds.Cancer epidemiology and preventioned. New York: Oxford University Press,2006: 975–94.
[2] Meinhold CL, Ron E, Schonfeld SJ, Alexander BH, Freedman DM, Linet MS, et al.Nonradiation risk factors for thyroid cancer in the US Radiologic TechnologistsStudy. Am J Epidemiol 2010;171:242–52.
[3] Memon A, Varghese A, Suresh A. Benign thyroid disease and dietary factors inthyroid cancer: a case–control study in Kuwait. Br J Cancer 2002;86:1745–50.
[4] Ron E, Kleinerman RA, Boice Jr JD, LiVolsi VA, Flannery JT, Fraumeni Jr JF. Apopulation-based case–control study of thyroid cancer. J Natl Cancer Inst1987;79:1–12.
[5] Galanti MR, Hansson L, Lund E, Bergstrom R, Grimelius L, Stalsberg H, et al.Reproductive history and cigarette smoking as risk factors for thyroid cancer inwomen: a population-based case–control study. Cancer Epidemiol BiomarkersPrev 1996;5:425–31.
[6] Hallquist A, Hardell L, Degerman A, Boquist L. Occupational exposures andthyroid cancer: results of a case–control study. Eur J Cancer Prev 1993;2:345–9.
[7] Kreiger N, Parkes R. Cigarette smoking and the risk of thyroid cancer. Eur JCancer 2000;36:1969–73.
[8] Mack WJ, Preston-Martin S, Dal Maso L, Galanti R, Xiang M, Franceschi S, et al. Apooled analysis of case–control studies of thyroid cancer: cigarette smokingand consumption of alcohol, coffee, and tea. Cancer Causes Control2003;14:773–85.
[9] Rossing MA, Cushing KL, Voigt LF, Wicklund KG, Daling JR. Risk of papillarythyroid cancer in women in relation to smoking and alcohol consumption.Epidemiology 2000;11:49–54.
[10] Guignard R, Truong T, Rougier Y, Baron-Dubourdieu D, Guenel P. Alcoholdrinking, tobacco smoking, and anthropometric characteristics as risk factorsfor thyroid cancer: a countrywide case–control study in New Caledonia. Am JEpidemiol 2007;166:1140–9.
[11] Iribarren C, Haselkorn T, Tekawa IS, Friedman GD. Cohort study of thyroidcancer in a San Francisco Bay area population. Int J Cancer 2001;93:745–50.
[12] Mack WJ, Preston-Martin S, Bernstein L, Qian D. Lifestyle and other risk factorsfor thyroid cancer in Los Angeles County females. Ann Epidemiol2002;12:395–401.
[13] Navarro Silvera SA, Miller AB, Rohan TE. Risk factors for thyroid cancer: aprospective cohort study. Int J Cancer 2005;116:433–8.
[14] Sokic SI, Adanja BJ, Vlajinac HD, Jankovic RR, Marinkovic JP, Zivaljevic VR. Riskfactors for thyroid cancer. Neoplasma 1994;41:371–4.
[15] Zivaljevic V, Vlajinac H, Marinkovic J, Paunovic I, Diklic A, Dzodic R. Cigarettesmoking as a risk factor for cancer of the thyroid in women. Tumori2004;90:273–5.
[16] Allen NE, Beral V, Casabonne D, Kan SW, Reeves GK, Brown A, et al. Moderatealcohol intake and cancer incidence in women. J Natl Cancer Inst 2009;101:296–305.
[17] Meinhold CL, Park Y, Stolzenberg-Solomon RZ, Hollenbeck AR, Schatzkin A,Berrington de Gonzalez A. Alcohol intake and risk of thyroid cancer in the NIH-AARP Diet and Health Study. Br J Cancer 2009;101:1630–4.
[18] Design of the Women’s Health Initiative clinical trial and observational study.The Women’s Health Initiative Study Group. Control Clin Trials 1998;19:61–109.
[19] Langer RD, White E, Lewis CE, Kotchen JM, Hendrix SL, Trevisan M. TheWomen’s Health Initiative Observational Study: baseline characteristics ofparticipants and reliability of baseline measures. Ann Epidemiol 2003;13:S107–21.
[20] Patterson RE, Kristal AR, Tinker LF, Carter RA, Bolton MP, Agurs-Collins T.Measurement characteristics of the Women’s Health Initiative food frequencyquestionnaire. Ann Epidemiol 1999;9:178–87.
[21] Curb JD, McTiernan A, Heckbert SR, Kooperberg C, Stanford J, Nevitt M, et al.Outcomes ascertainment and adjudication methods in the Women’s HealthInitiative. Ann Epidemiol 2003;13:S122–8.
[22] Kuper H, Boffetta P, Adami HO. Tobacco use and cancer causation: associationby tumour type. J Intern Med 2002;252:206–24.
[23] Wirdefeldt K, Adami HO, Cole P, Trichopoulos D, Mandel J. Epidemiology andetiology of Parkinson’s disease: a review of the evidence. Eur J Epidemiol2011;26(Suppl. 1):S1–58.
[24] Asvold BO, Bjoro T, Nilsen TI, Vatten LJ. Tobacco smoking and thyroid function:a population-based study. Arch Intern Med 2007;167:1428–32.
[25] Belin RM, Astor BC, Powe NR, Ladenson PW. Smoke exposure is associated witha lower prevalence of serum thyroid autoantibodies and thyrotropin concen-tration elevation and a higher prevalence of mild thyrotropin concentrationsuppression in the third National Health and Nutrition Examination Survey(NHANES III). J Clin Endocrinol Metab 2004;89:6077–86.
[26] Hard GC. Recent developments in the investigation of thyroid regulation andthyroid carcinogenesis. Environ Health Perspect 1998;106:427–36.
[27] Klatsky AL. Invited commentary: never, or hardly ever? It could make adifference. Am J Epidemiol 2008;168:872–5 [discussion 6–7].
[28] Rehm J, Irving H, Ye Y, Kerr WC, Bond J, Greenfield TK. Are lifetime abstainersthe best control group in alcohol epidemiology? On the stability and validity ofreported lifetime abstention. Am J Epidemiol 2008;168:866–71.