situation analysis for managing diabetic retinopathy · situation analysis for managing diabetic...
TRANSCRIPT
SITUATION ANALYSIS FOR MANAGING DIABETIC RETINOPATHY
IN TAKEO PROVINCE, CAMBODIA
Dec 2012 Caritas Takeo Regional Eye Hospital
Page 2 of 26
ACKNOWLEDGEMENTS
The evaluation team expresses their sincere appreciation to the National Eye Health Program
team, Professor Ngy Meng, Director of NPEH; Professor Do Seiha, Vice Director and Coordinator
for NPEH; and Professor Kong Piseth, a member of NPEH, Deputy Director and Chairman of the
Department of Ophthalmology, Preah Ang Duong Hospital, Phnom Penh, Cambodia. Additionally,
Dr Hem Saret, Director Takeo Provincial Health Department; and Dr.Kheav Samros, Deputy
Director of Provincial Health Department in charge of Dunkeo Referral Hospital (General Hospital)
who also participated in the evaluation.
Special thanks is also expressed toward the Caritas Takeo Eye Hospital management team and
staff, for helping to make the necessary arrangements for appointments and visits to the Kiri Vong
Referral Hospital Vision Centre. Particular acknowledgement to Dr Neang Mao, Mr Te Serey Bonn,
Mr El Nimeth, Sr Myrna Porto, Sr Evangeline Dunton.
The evaluation team also would like to thank the team at the Kiri Vong Referral Hospital and Kiri
Vong Referral Hospital Vision Centre, and Dr Sambo (Director of the Kiri Vong Operational
District).
Funding for this program was provided by the Australia Agency for International Development
(AusAID), Avoidable Blindness Initiative to CBM Australia / Caritas Takeo Eye Hospital.
EVALUATION TEAM
Rahul Chakrabarti1, Gail M Ormsby1, Mufarriq Shah1, Manfred Mörchen2, Jill E Keeffe3
1 PhD candidate, Population Health Unit, Centre for Eye Research Australia, The University of Melbourne,
Royal Victorian Eye and Ear Hospital
2 Caritas Takeo Eye Hospital, Takeo, Cambodia; CBM
3 Head of Population Health Unit, Centre for Eye Research Australia, The University of Melbourne, Royal
Victorian Eye and Ear Hospital
Page 3 of 26
TABLE OF CONTENTS
Background ......................................................................................................................................... 5
Aim ...................................................................................................................................................... 7
Objectives ............................................................................................................................................ 7
Methods .............................................................................................................................................. 8
Results ............................................................................................................................................... 10
The Need: Current Estimates of Diabetic Retinopathy ................................................................. 10
Health Service Delivery ................................................................................................................. 11
Linkages and Networks ................................................................................................................. 13
Health Workforce and Strengthening Capacity ............................................................................ 15
Health Technologies and Infrastructure ....................................................................................... 17
Health Information Systems and Management ............................................................................ 20
Health Financing and Sustainability .............................................................................................. 20
Governance and Leadership .......................................................................................................... 21
Key Outcomes ................................................................................................................................... 22
References......................................................................................................................................... 24
Page 4 of 26
ACRONYMS
AusAID Australian Agency for International Development
ABI Avoidable Blindness Initiative
CBMA CBM Australia
CBR Community Based Rehabilitation
CDMD Cambodian Development Mission for Disability
CERA Centre for Eye Research Australia
CTEH Caritas Takeo Eye Hospital
DM Diabetes Mellitus
DR Diabetic Retinopathy
HIMS Health Information Management System
KAP Knowledge, Attitude and Practice
KVRHVC Kiri Vong Referral Hospital Vision Centre
MoH Ministry of Health
MOU Memorandum of Understanding
NGO Non-Government Organisation
NPEH National Program for Eye Health
RAAB Rapid Assessment of Avoidable Blindness
URE Uncorrected Refractive Error
VA Visual Acuity
WHO World Health Organization

Page 5 of 26
EXECUTIVE SUMMARY
Background and context
Diabetic retinopathy (DR) is a microvascular complication of diabetes. Worldwide, the global
burden of diabetes is estimated at 346 million.1 This is projected to increase to 438 million by the
year 2030 (4.4% of the estimated world population). In Cambodia, it is estimated that the
prevalence of any DR amongst people with diabetes is 30.3%.2 This is consistent with global meta-
analyses data that showed one-third of patients with diabetes will have evidence of any DR, and
one-third of those with DR will have vision threatening retinopathy (VTDR).3 Research has clearly
demonstrated that blindness from diabetes is almost entirely preventable with early diagnosis,
optimisation of risk factors, and timely photocoagulation where appropriate.4-6 Presently, 70 per
cent of diabetes occurs in lower and middle income countries, where systematic screening for
retinopathy is rare.7
The growth of diabetes and diabetic retinopathy is a concern for developing countries. According
to the World Health Organization (WHO) in 2012, the age-standardised estimate of prevalence of
diagnosed diabetes amongst adults (age 20-79) in Cambodia was 5.1%.8 King et al in 2005
estimated the prevalence of diabetes in a community-based survey of 5% in the Siem Riep
province, and 11% in the Kampong Cham province, of which two-thirds of all cases of diabetes
were undiagnosed prior to the survey.9 The WHO estimates the population with diabetes in
Cambodia will increase to 317,000 by the year 2030.10 This will therefore impact upon the burden
of vision impairment secondary to diabetes.
Presently in Cambodia there is no systematic screening for DR. However, there is interest in using
an evidence-based approach to guide future planning. This report will assess the existing
infrastructure and the potential for the Kiri Vong Referral Hospital Vision Centre and Takeo Eye
Hospital to screen, refer and manage patients with diabetes and diabetic retinopathy. At present,
the Cambodian Government has expressed interest in addressing the issue of how to approach
management of diabetic retinopathy. The NPEH committee has requested AusAID to fund the
establishment of twelve diabetes clinics in 2013. It is intended that this preliminary report will
provide insight into the current strengths and limitations of the health system to manage DR. This
work will contribute to future research for the development of an evidence-based framework to
guide the management of diabetic retinopathy as part of systemic approach to care for the
patient with diabetes.
Page 6 of 26
Summary of Findings
The situational analysis was conducted using themes adapted from the WHO Health System
‘Building Blocks’ that together constitute a complete system.
1. Health Service Delivery and Performance
2. Linkages and Networks
3. Health Workforce and Strengthening Capacity
4. Health information Systems and Management
5. Health Financing and Sustainability
6. Governance and Leadership
The situation analysis showed that the CTEH is the only facility in the Takeo Province with the
capacity to examine and provide laser treatment of patients with diabetes for DR. Preliminary
data suggests that DR accounts for 12% of all retinal pathology diagnosed at the CTEH. Eight of
thirteen patients diagnosed with DR had mild non-proliferative retinopathy.
People with diabetes access multiple sources of health care in the Takeo Province including health
centres, general hospitals, community vision screening, and private medical practitioners.
However, the CTEH is the only health care facility in the province with the capacity to perform
retinal examination. Patients with diabetes can be referred for eye examinations from the
KVRHVC, community outreach screening and the local NGO, Mo Po Tsyo to the CTEH. However,
there is no referral of patients with diabetes from general hospitals, and currently it is estimated
that only a small proportion patients are referred from KVRHVC or community outreach. Most
patients with diabetes present to the CTEH as “walk-ins”.
The health information management system for recording details of patients with diabetes can be
improved. The CTEH health information system has recently started to record pertinent clinical
information related to the eye examination for the patient with diabetes. However, the data
entered at the KVRHVC is non-specific, and there is no established procedure for recording
outcomes of patient follow-up.
The cost recovery methods of the CTEH and KVRHVC involve sales of spectacles and nominal fees
for cost-recovery. At the CTEH, approximately 30% of retinal examination fees are out-of-pocket
for the patient. The KVRHVC continues to receive technical advice as required from the CTEH.
There are no current national guidelines for diabetic retinopathy in Cambodia. There is no routine
referral system for eye examination amongst patients with diabetes.
Page 7 of 26
AIM
The aim is to perform a situation analysis of existing infrastructure at the Kiri Vong Referral
Hospital Vision Centre (KVRHVC) and the Caritas Takeo Eye Hospital (CTEH) to examine and
manage patients with diabetes mellitus for diabetic retinopathy.
OBJECTIVES
The objectives of this research were guided by the National Strategic Plan for Blindness
Prevention and Control, 2008-2015 (Cambodian Ministry for Health). The situation analysis
assessed the possible role of the KVRHVC, CTEH and linkages with district hospitals in the care of
patients with diabetes, and assessment and timely referral of people with diabetic retinopathy.
The World Health Organization framework for health systems evaluation has guided the
development of specific research themes to be used in this study. The objectives were:
1. Service Delivery and Performance in managing DR
a. Describe and quantify the spectrum of functions performed by the CTEH to manage DR
including:
I. Diagnosis, treatment, referral, follow-up, and rehabilitation.
II. Role of the CTEH and other health facilities in providing health promotion
(information, education and communication) about diabetes and DR.
2. Linkages and Networks
a. Describe linkages and referral pathways for patients with diabetes and DR between Vision
Centres and primary health centres, CDMD, outreach services, public hospitals and the
Caritas Takeo Eye Hospital.
b. Identify service-related barriers to the delivery and utilisation of linkages and referral
pathways.
c. Describe what and how information is provided to patients with diabetes regarding DR,
referral, the follow-up process, and reminders for screening.
3. Health Workforce and Strengthening Capacity
a. Define the current roles and tasks performed by the workforce.
b. Identify the capacity for training of the workforce and continuing medical education
specifically for management of DR.
Page 8 of 26
4. Health Information Systems and Management
a. Examine the content of health records, as to how diabetes and diabetic retinopathy and
recorded.
b. Describe the health information systems for patient record collection, storage, follow-up,
and to show compliance with services.
5. Health Technologies and Infrastructure
a. List the equipment at KVRHVC and CTEH to perform eye examinations for patients with
diabetes and treatment of patients with retinopathy.
6. Health Financing and Sustainability
a. For eye care services provided to the patients with diabetes, describe and quantify who
pays (patient, government, NGO, private health insurance)
7. Governance and Leadership
a. Describe the role and involvement of key stakeholders in the operation and overseeing
diabetic retinopathy management at the CTEH and the KVRHVC.
b. Describe the presence and rationale for clinical preferred practice statements or national
guidelines.
METHODS
Setting
The situation analysis assessed the existing system for eye care management at the KVRHVC and
Caritas Takeo Eye Hospital and their referral sources.
Participants
Key stakeholders consulted in the data collection phase included:
(a) Policy level personnel (NPEH, Country directors for NGOs, Ministry of Health, Director of
Takeo Operational District),
(b) Workers at the Vision Centres and hospitals (Medical director, ophthalmologists,
refractionists, ophthalmic nurse manager and educator, medical records personnel).
Time frame of the Evaluation
Data were collected over a two week period in mid December, 2012.
Page 9 of 26
Data collection
Data were acquired from two main sources.
1. Existing information available in medical records and databases at Caritas Takeo Eye
Hospital and the Kiri Vong Referral Hospital Vision Centre.
2. Semi-structured interviews and observational data from site visits and consultation with
relevant stakeholders.
Evaluation study questionnaires
The evaluation study questionnaires were developed by the Population Health Unit at the Centre
for Eye Research Australia (CERA). The questionnaires were designed to assess the specific
objectives listed. Each questionnaire included items relevant to the particular health care setting
and stakeholders (KVRHVC, CTEH, and NPEH). The 15 page questionnaire is obtainable from CERA
on request. The questionnaires were divided into the nine themes as listed in the objectives.
Informed consent was obtained from all participants in the evaluation.
Page 10 of 26
RESULTS
THE NEED: CURRENT ESTIMATES OF DIABETIC RETINOPATHY
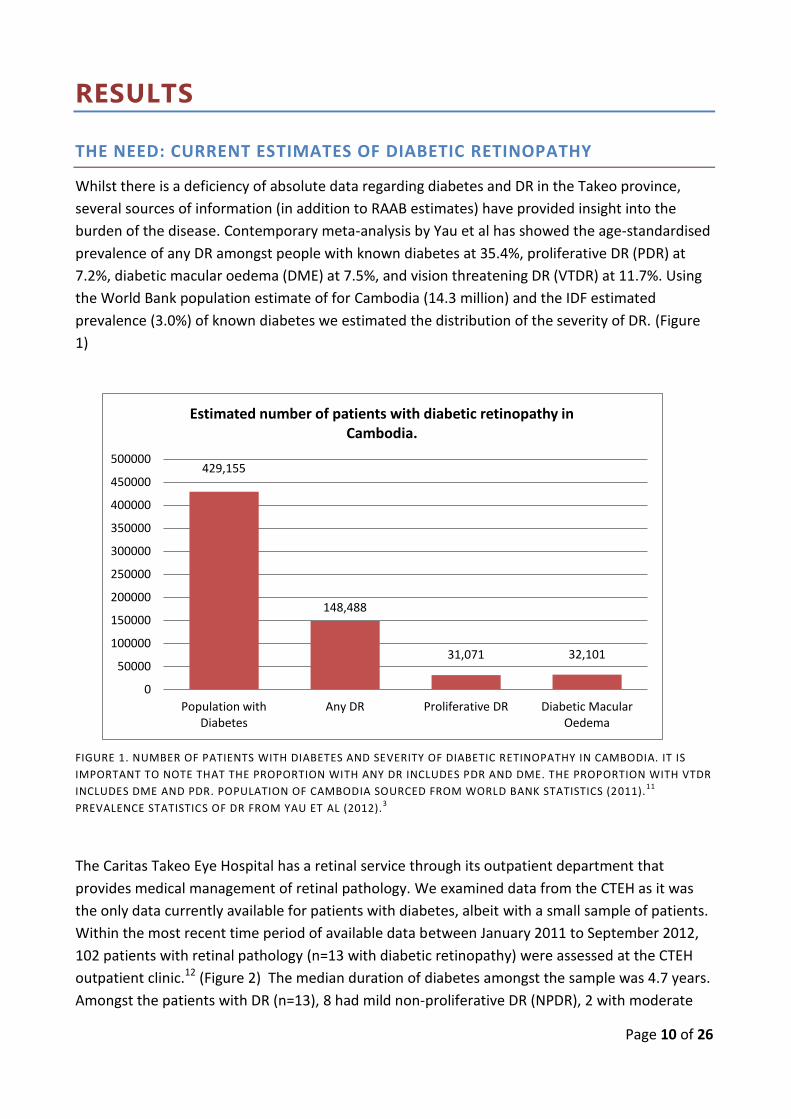
Whilst there is a deficiency of absolute data regarding diabetes and DR in the Takeo province,
several sources of information (in addition to RAAB estimates) have provided insight into the
burden of the disease. Contemporary meta-analysis by Yau et al has showed the age-standardised
prevalence of any DR amongst people with known diabetes at 35.4%, proliferative DR (PDR) at
7.2%, diabetic macular oedema (DME) at 7.5%, and vision threatening DR (VTDR) at 11.7%. Using
the World Bank population estimate of for Cambodia (14.3 million) and the IDF estimated
prevalence (3.0%) of known diabetes we estimated the distribution of the severity of DR. (Figure
1)
FIGURE 1. NUMBER OF PATIENTS WITH DIABETES AND SEVERITY OF DIABETIC RETINOPATHY IN CAMBODIA. IT IS
IMPORTANT TO NOTE THAT THE PROPORTION WITH ANY DR INCLUDES PDR AND DME. THE PROPORTION WITH VTDR
INCLUDES DME AND PDR. POPULATION OF CAMBODIA SOURCED FROM WORLD BANK STATISTICS (2011).11
PREVALENCE STATISTICS OF DR FROM YAU ET AL (2012).3
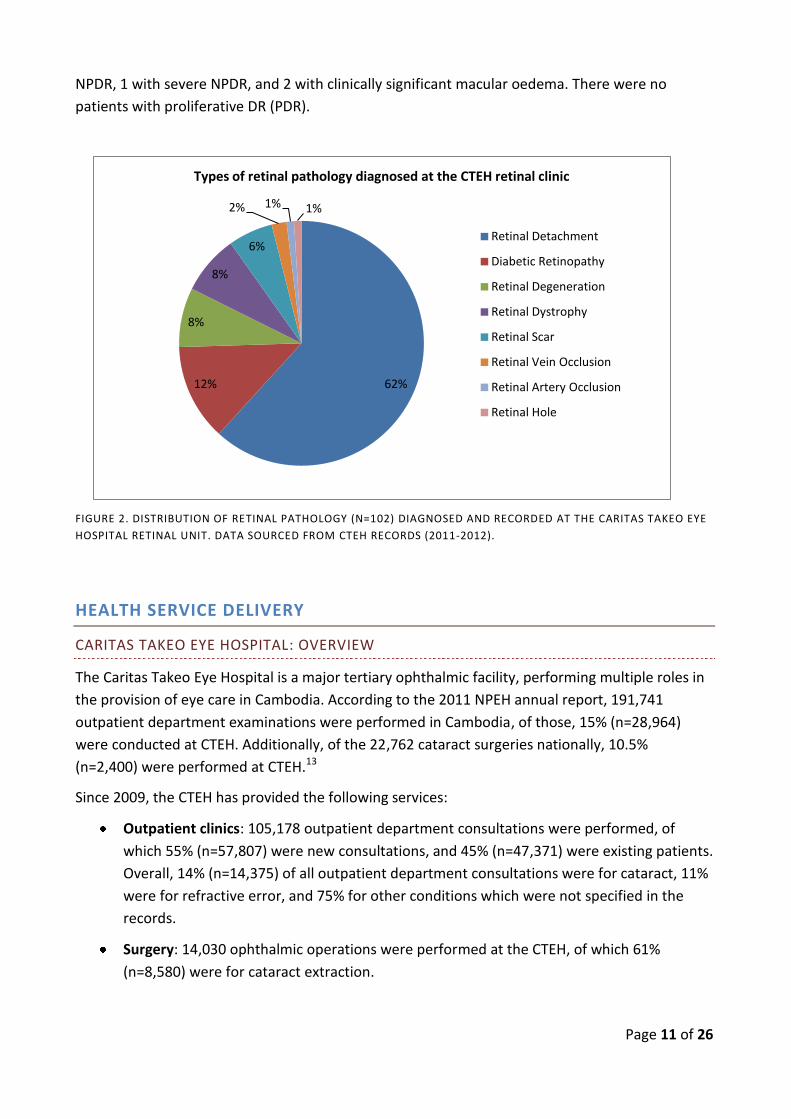
The Caritas Takeo Eye Hospital has a retinal service through its outpatient department that
provides medical management of retinal pathology. We examined data from the CTEH as it was
the only data currently available for patients with diabetes, albeit with a small sample of patients.
Within the most recent time period of available data between January 2011 to September 2012,
102 patients with retinal pathology (n=13 with diabetic retinopathy) were assessed at the CTEH
outpatient clinic.12 (Figure 2) The median duration of diabetes amongst the sample was 4.7 years.
Amongst the patients with DR (n=13), 8 had mild non-proliferative DR (NPDR), 2 with moderate
429,155
148,488
31,071 32,101
0
50000
100000
150000
200000
250000
300000
350000
400000
450000
500000
Population with Diabetes
Any DR Proliferative DR Diabetic Macular Oedema
Estimated number of patients with diabetic retinopathy in Cambodia.
Page 11 of 26
NPDR, 1 with severe NPDR, and 2 with clinically significant macular oedema. There were no
patients with proliferative DR (PDR).
FIGURE 2. DISTRIBUTION OF RETINAL PATHOLOGY (N=102) DIAGNOSED AND RECORDED AT THE CARITAS TAKEO EYE
HOSPITAL RETINAL UNIT. DATA SOURCED FROM CTEH RECORDS (2011-2012).
HEALTH SERVICE DELIVERY
CARITAS TAKEO EYE HOSPITAL: OVERVIEW
The Caritas Takeo Eye Hospital is a major tertiary ophthalmic facility, performing multiple roles in
the provision of eye care in Cambodia. According to the 2011 NPEH annual report, 191,741
outpatient department examinations were performed in Cambodia, of those, 15% (n=28,964)
were conducted at CTEH. Additionally, of the 22,762 cataract surgeries nationally, 10.5%
(n=2,400) were performed at CTEH.13
Since 2009, the CTEH has provided the following services:
Outpatient clinics: 105,178 outpatient department consultations were performed, of
which 55% (n=57,807) were new consultations, and 45% (n=47,371) were existing patients.
Overall, 14% (n=14,375) of all outpatient department consultations were for cataract, 11%
were for refractive error, and 75% for other conditions which were not specified in the
records.
Surgery: 14,030 ophthalmic operations were performed at the CTEH, of which 61%
(n=8,580) were for cataract extraction.
62% 12%
8%
8%
6%
2% 1% 1%
Types of retinal pathology diagnosed at the CTEH retinal clinic
Retinal Detachment
Diabetic Retinopathy
Retinal Degeneration
Retinal Dystrophy
Retinal Scar
Retinal Vein Occlusion
Retinal Artery Occlusion
Retinal Hole
Page 12 of 26
Vision screening in the Takeo province: 8,828 people were screened for vision loss. 11% of
the screened population had “normal” eyes. Amongst the population with ophthalmic
pathology, 44% were diagnosed with cataract, of which 67% (n=2,198) were referred for
surgery at the CTEH.
Refractive Services and Optical workshop: Since 2009, the CTEH has performed 11,802
refractions and dispensed 6419 spectacles.
Training: In 2011, the CTEH provided training of 9 resident doctors in the national
ophthalmology training program, an additional 3 doctors in the diploma of ophthalmology
program, 18 nurses in diploma of ophthalmic nursing, and training of one paediatric nurse
and one orthoptic nurse. The diploma of ophthalmology program has since ceased.
Diploma qualified and Basic Eye Doctors are now receiving training to be upgraded to
ophthalmologists.
CARITAS TAKEO EYE HOSPITAL AND DIABETIC RETINOPATHY
Screening patients with diabetes for diabetic retinopathy has been a recent addition to the
services of the outpatient department at the CTEH. The screening examination involves
assessment of the patient’s visual acuity, measurement of intraocular pressure (IOP), and dilated
fundoscopy which is performed by ophthalmologists. Patients with suspected refractive error are
assessed by ophthalmic nurses trained in refraction; and those requiring spectacles are referred
to the optical workshop. The CTEH currently does not provide pathology services for patients
with diabetes as such services are located nearby in Provincial Regional Hospital (general
hospital). The typical examination interval for patients with varying severity of DR attending the
CTEH outpatient clinic is shown in the table below. Interestingly, for patients with nil to mild NPDR
the current practised examination interval is 12 months. However, it was shown in the small
cohort from CTEH that patients with diabetes had short duration from the diabetes diagnosis
(median 4.7 years), and had mild DR. Further longitudinal data will provide insight into the true
distribution of DR severity at CTEH. However, evidence has shown that extending the screening
interval to two years for the majority of patients with diabetes who have nil-mild NPDR is a safe
and practical approach to meet the demands of screening.14
TABLE 1. EXAMINATION INTERVAL FOR PATIENTS AT VARYING SEVERITY OF DR. SOURCED FROM CORRESPONDENCE
WITH OPHTHALMOLOGIST AT THE CTEH, 2012.
Severity of DR Examination interval
Nil-Mild Non Proliferative DR 12 months
Moderate Non Proliferative DR 6 months
Severe Non Proliferative DR 3 months
Clinically significant Macular Oedema 1 month
Page 13 of 26
The CTEH also has the capacity for non-surgical treatment of retinopathy. It is estimated that two
patients with diabetes referred to the CTEH outpatient department have been treated with retinal
laser. The CTEH does not have vitreoretinal surgical expertise or equipment. Those requiring
surgery for vitreous haemorrhage or vitreoretinal traction related issues are referred to the
National Eye Hospital in Phnom Penh; the number of patients referred was not available.
Beyond screening, the retinal unit is also involved in health promotion for patients with diabetes.
Through the CTEH vision screening program, health education is provided during the screening
days. Additionally, most patients referred for surgical assessment at the outpatient department
are routinely asked of their diabetes status, but are not usually asked whether they have had a
previous examination to the back of their eye. For all patients with diabetes, the CTEH provides
general advice on diabetes control, and education about blindness from diabetes and treatment.
Specifically, patients are educated on the complications of diabetes and the importance of regular
eye examination. At present, there are no data regarding the quality of these services provided,
and the impact of their effect on change in knowledge, attitudes and practice.
LINKAGES AND NETWORKS
The CTEH is the only facility in the province that has the capacity to perform dilated retinal
examinations for patients with diabetes. People with diabetes are referred the CTEH outpatient
department for examination and management from several sources including the Kiri Vong
Referral Hospital Vision Centre (KVRHVC), outreach vision screening clinics, general medical
hospitals, private clinics, and from Mo Po Tsyo (a local NGO involved in screening for diabetes in
the community).
Kiri Vong Referral Hospital Vision Centre
The KVRHVC has been in operation since April 2010. The primary functions of the KVRHVC are
provision of primary eye care, refraction, provision of ready-made spectacles and sunglasses, and
participation in community eye screening. The staff at the KVRHVC cannot perform dilated retinal
examinations so patients with diabetes are referred for eye examination at the CTEH.
Review of the KVRHVC records between April 2010 and November 2012 documented 7,858
consultations of which 1,774 patients were referred to the CTEH. Amongst the patients referred
from the KVRHVC to the CTEH, 47% (n=826) were for management of cataract, 44% (n=788) for
“other” conditions, 8% (n=153) refractive error, and <1% (n=7) for glaucoma. However, there
were no records to estimate the proportion of patients with diabetes seen at the KVRHVC or the
proportion of those that were referred to the CTEH.
Outreach vision screening
The community outreach vision screening programs conducted by the KVRHVC and the CTEH are
important sources of referral of patients to the CTEH outpatient department. Between January
2010 to October 2012, 8,828 patients were screened through the CTEH outreach program, of
which 3,534 people were referred for examination at the CTEH. From the proportion of patients
referred to the CTEH, 62% (n=2,198) were for cataract, and the remainder were for “other”
Page 14 of 26
conditions. As patients with diabetes were not identified specifically at screening, it was reported
that few patients with DR were referred from outreach screening for eye examination.
Vision screening is conducted by the Kiri Vong Referral Hospital Vision Centre outreach program in
the Kiri Vong District. From data obtained of referrals made from screening in the Kiri Vong
District (2010-2011, n=2,997), it was estimated that cataract accounted for 39% (n=1158),
refractive error 15% (n=439), and 46% (n=1,396) were recorded as “other” conditions. Analysis of
the sources for patient referral to the KVRHVC showed that 82% of consultations were from
“walk-in” patients. This opens the opportunity to enquire about the known diagnosis of diabetes
or previous eye examination amongst patients with diabetes during the consultation as a simple
method to facilitate early identification of people needing follow-up eye examination for diabetes
related ocular complications.
General Medical Hospital (Chronic Disease Clinic of Dunkeo Referral Hospital)
General hospitals are a potential source of referral of patients with diabetes for an eye
examination.
The Dunkeo Referral Hospital is a general hospital in close proximity to the CTEH was staffed by
three medical officers (doctors), and six nurses. Typically, patients with diabetes are asked by
attending clinicians about their diabetes type, duration since diagnosis, and current treatment
(oral medication, insulin). General hospitals have the facilities to perform and record a basic
examination (weight and blood pressure measurement), and simple pathology tests for patients
with diabetes. Patients with diabetes are provided general advice on diabetes control and
informed about the complications of diabetes (including vision threatening disease). However,
patients are not routinely asked if they have ever had an eye examination.
Data on the proportion of patients with diabetes attending general hospital and those referred to
CTEH were not available. There is no eye care provided at general hospitals, or referral protocol
for patients with diabetes attending a general hospital to have an eye examination.
Consequently, very few patients are referred to CTEH for eye examination. If required, patients
with diabetes reporting or found to have deterioration in their vision are provided a verbal
referral to attend the CTEH.
Local Non-Government Organisation – Mo Po Tsyo
The close network between CTEH and the local NGO, Mo Po Tsyo, offers an insight into how DR
can be approached in low-resource settings. The Mo Po Tsyo program performs a screening for
diabetes amongst the population at high risk across five provinces of Cambodia. In their referral
pathway, a research assistant visits households and those with evidence of an abnormal urinalysis
(urine dipstick test for glucose, protein) are requested to have further blood tests and are advised
to visit a referral hospital in their district on a particular date. That particular hospital is visited by
a diabetologist (who is employed by Mo Po Tsyo) who performs the examination and investigation
of these patients. Whilst this method may only capture the proportion of patients with diabetes
with renal impairment, through interview with Mo Po Tsyo staff it was explained that this is a
relatively inexpensive tool in a setting where glucometers (and their random blood sugar sampling
Page 15 of 26
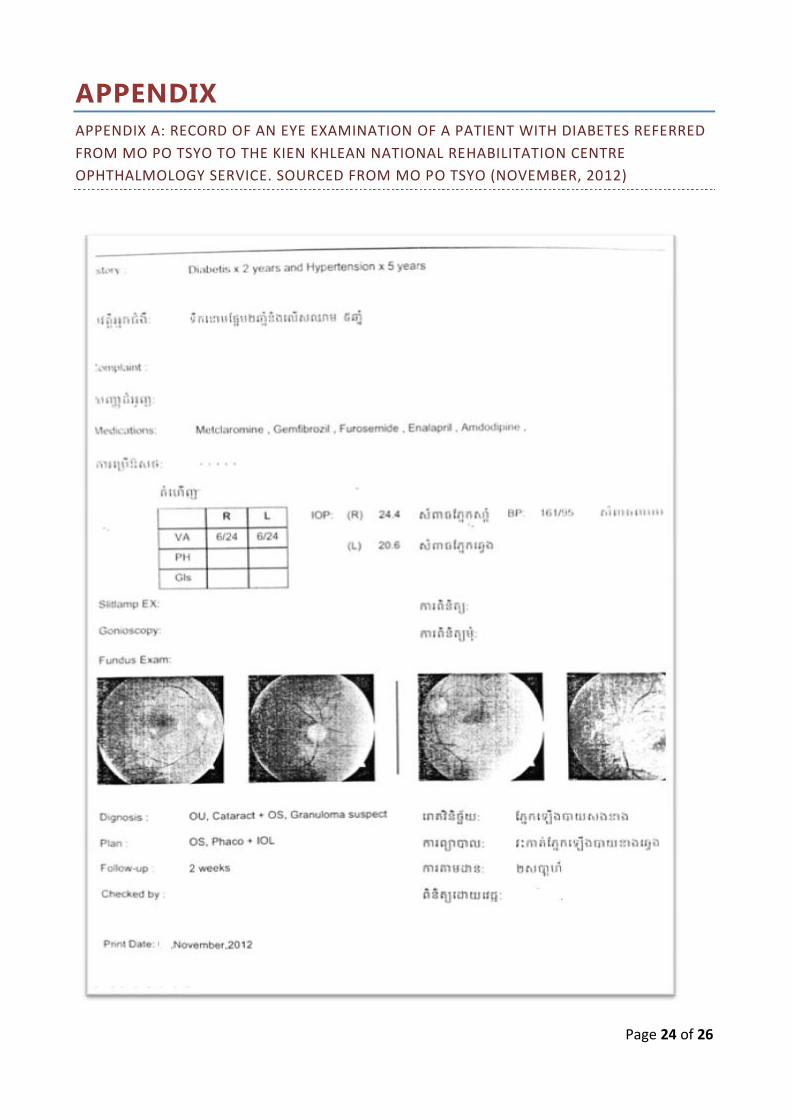
strips) are not readily affordable. After consultation with the endocrinologist, patients with high
risk factors (duration since diagnosis of diabetes, hypertension, poor glycaemic control) are
referred for a retinal examination at CTEH and the Kien Khleang National Rehabilitation Centre
Ophthalmology Service (Phnom Penh). The Kien Khleang ophthalmology service has the capacity
to measure visual acuity, slit-lamp examination and retinal photography. Findings are recorded in
a computerised health information system, and reported back to Mo Po Tsyo. (Appendix) The
strength of collaboration between the Mo Po Tsyo clinic and the CTEH is evidenced by the
increased numbers of referrals of patients with diabetes to the retina clinic from 44 patients in
2011, to 136 patients in 2012.
HEALTH WORKFORCE AND STRENGTHENING CAPACITY
CARITAS TAKEO EYE HOSPITAL
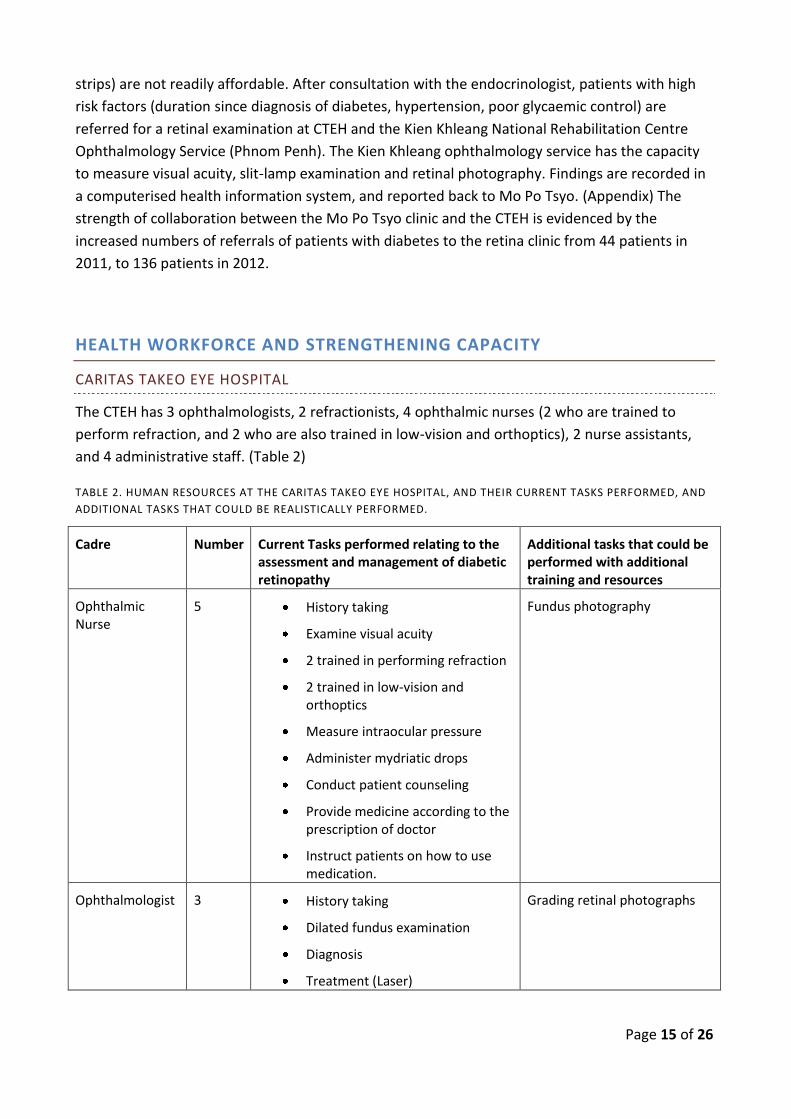
The CTEH has 3 ophthalmologists, 2 refractionists, 4 ophthalmic nurses (2 who are trained to
perform refraction, and 2 who are also trained in low-vision and orthoptics), 2 nurse assistants,
and 4 administrative staff. (Table 2)
TABLE 2. HUMAN RESOURCES AT THE CARITAS TAKEO EYE HOSPITAL, AND THEIR CURRENT TASKS PERFORMED, AND
ADDITIONAL TASKS THAT COULD BE REALISTICALLY PERFORMED.
Cadre Number Current Tasks performed relating to the assessment and management of diabetic retinopathy
Additional tasks that could be performed with additional training and resources
Ophthalmic Nurse
5
History taking
Examine visual acuity
2 trained in performing refraction
2 trained in low-vision and orthoptics
Measure intraocular pressure
Administer mydriatic drops
Conduct patient counseling
Provide medicine according to the prescription of doctor
Instruct patients on how to use medication.
Fundus photography
Ophthalmologist 3 History taking
Dilated fundus examination
Diagnosis
Treatment (Laser)
Grading retinal photographs
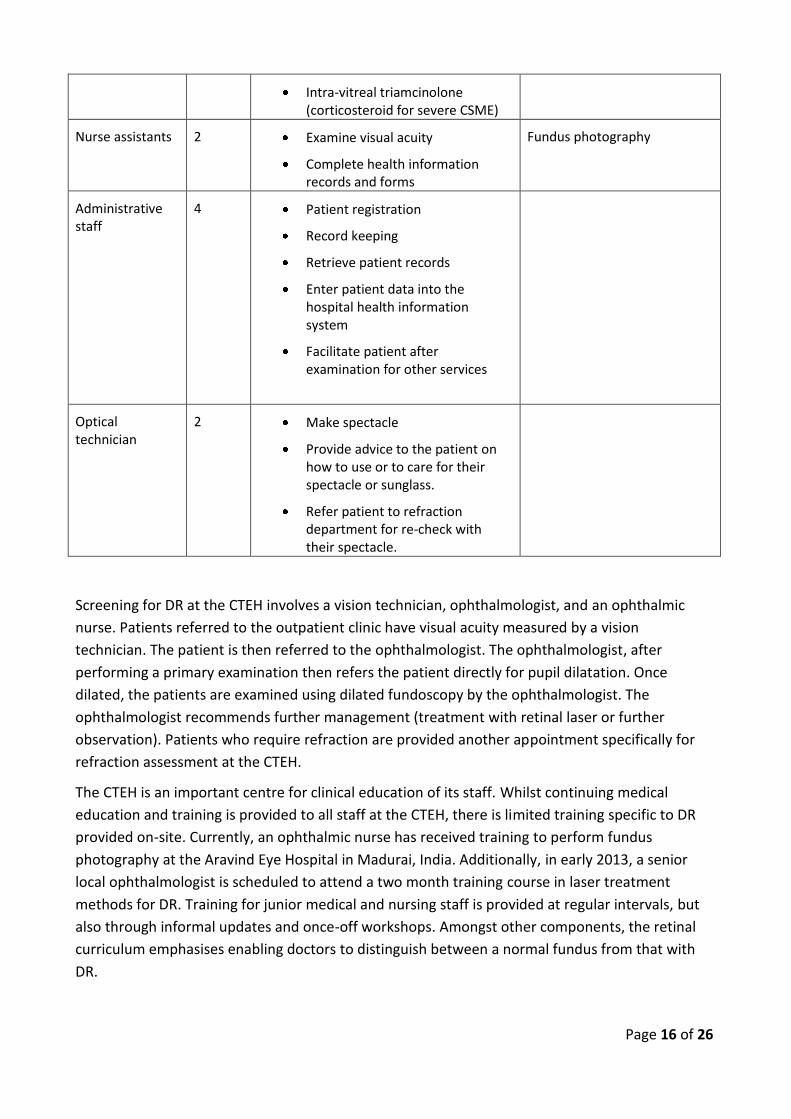
Page 16 of 26
Intra-vitreal triamcinolone (corticosteroid for severe CSME)
Nurse assistants 2 Examine visual acuity
Complete health information records and forms
Fundus photography
Administrative staff
4 Patient registration
Record keeping
Retrieve patient records
Enter patient data into the hospital health information system
Facilitate patient after examination for other services
Optical technician
2 Make spectacle
Provide advice to the patient on how to use or to care for their spectacle or sunglass.
Refer patient to refraction department for re-check with their spectacle.
Screening for DR at the CTEH involves a vision technician, ophthalmologist, and an ophthalmic
nurse. Patients referred to the outpatient clinic have visual acuity measured by a vision
technician. The patient is then referred to the ophthalmologist. The ophthalmologist, after
performing a primary examination then refers the patient directly for pupil dilatation. Once
dilated, the patients are examined using dilated fundoscopy by the ophthalmologist. The
ophthalmologist recommends further management (treatment with retinal laser or further
observation). Patients who require refraction are provided another appointment specifically for
refraction assessment at the CTEH.
The CTEH is an important centre for clinical education of its staff. Whilst continuing medical
education and training is provided to all staff at the CTEH, there is limited training specific to DR
provided on-site. Currently, an ophthalmic nurse has received training to perform fundus
photography at the Aravind Eye Hospital in Madurai, India. Additionally, in early 2013, a senior
local ophthalmologist is scheduled to attend a two month training course in laser treatment
methods for DR. Training for junior medical and nursing staff is provided at regular intervals, but
also through informal updates and once-off workshops. Amongst other components, the retinal
curriculum emphasises enabling doctors to distinguish between a normal fundus from that with
DR.
Page 17 of 26
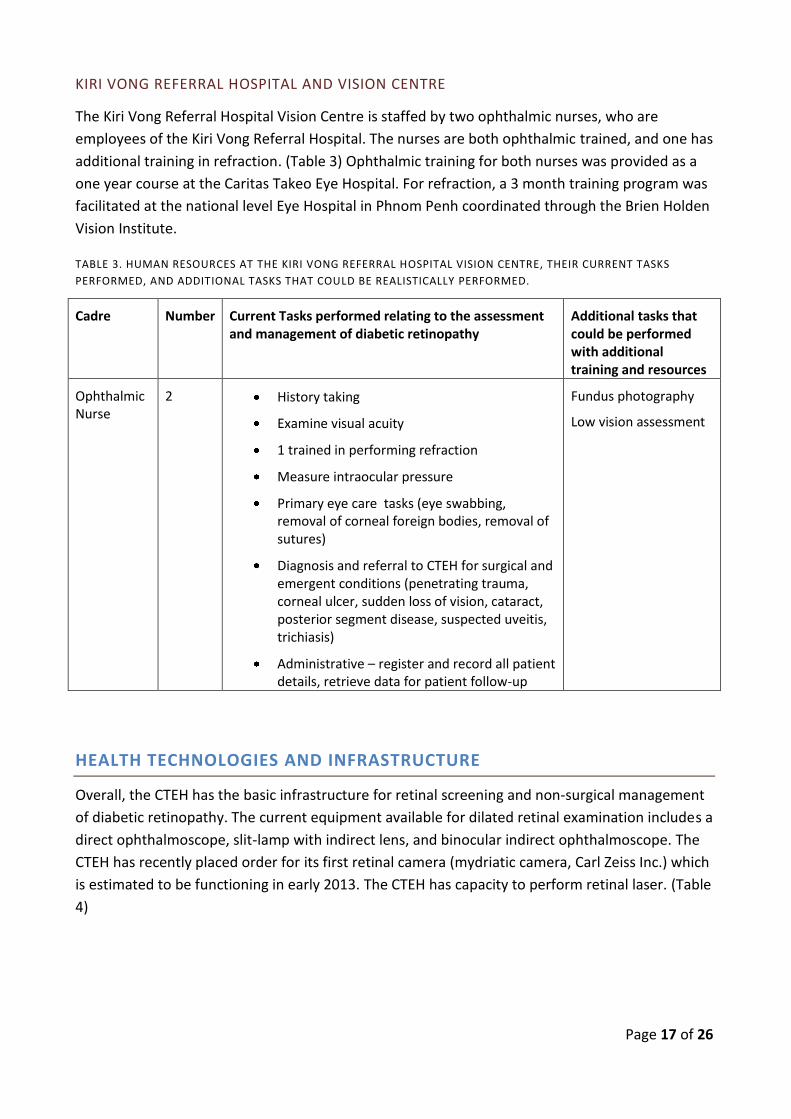
KIRI VONG REFERRAL HOSPITAL AND VISION CENTRE
The Kiri Vong Referral Hospital Vision Centre is staffed by two ophthalmic nurses, who are
employees of the Kiri Vong Referral Hospital. The nurses are both ophthalmic trained, and one has
additional training in refraction. (Table 3) Ophthalmic training for both nurses was provided as a
one year course at the Caritas Takeo Eye Hospital. For refraction, a 3 month training program was
facilitated at the national level Eye Hospital in Phnom Penh coordinated through the Brien Holden
Vision Institute.
TABLE 3. HUMAN RESOURCES AT THE KIRI VONG REFERRAL HOSPITAL VISION CENTRE, THEIR CURRENT TASKS
PERFORMED, AND ADDITIONAL TASKS THAT COULD BE REALISTICALLY PERFORMED.
Cadre Number Current Tasks performed relating to the assessment and management of diabetic retinopathy
Additional tasks that could be performed with additional training and resources
Ophthalmic Nurse
2
History taking
Examine visual acuity
1 trained in performing refraction
Measure intraocular pressure
Primary eye care tasks (eye swabbing, removal of corneal foreign bodies, removal of sutures)
Diagnosis and referral to CTEH for surgical and emergent conditions (penetrating trauma, corneal ulcer, sudden loss of vision, cataract, posterior segment disease, suspected uveitis, trichiasis)
Administrative – register and record all patient details, retrieve data for patient follow-up
Fundus photography
Low vision assessment
HEALTH TECHNOLOGIES AND INFRASTRUCTURE
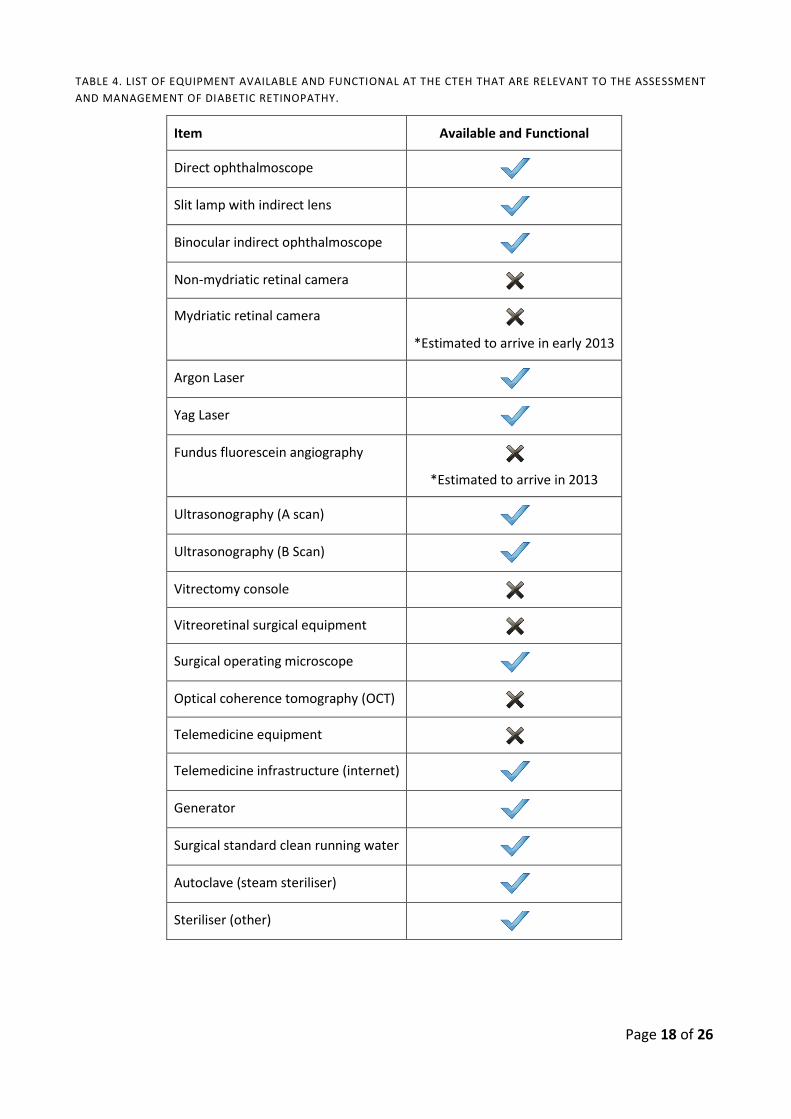
Overall, the CTEH has the basic infrastructure for retinal screening and non-surgical management
of diabetic retinopathy. The current equipment available for dilated retinal examination includes a
direct ophthalmoscope, slit-lamp with indirect lens, and binocular indirect ophthalmoscope. The
CTEH has recently placed order for its first retinal camera (mydriatic camera, Carl Zeiss Inc.) which
is estimated to be functioning in early 2013. The CTEH has capacity to perform retinal laser. (Table
4)
Page 18 of 26
TABLE 4. LIST OF EQUIPMENT AVAILABLE AND FUNCTIONAL AT THE CTEH THAT ARE RELEVANT TO THE ASSESSMENT
AND MANAGEMENT OF DIABETIC RETINOPATHY.
Item Available and Functional
Direct ophthalmoscope
Slit lamp with indirect lens
Binocular indirect ophthalmoscope
Non-mydriatic retinal camera
Mydriatic retinal camera
*Estimated to arrive in early 2013
Argon Laser
Yag Laser
Fundus fluorescein angiography
*Estimated to arrive in 2013
Ultrasonography (A scan)
Ultrasonography (B Scan)
Vitrectomy console
Vitreoretinal surgical equipment
Surgical operating microscope
Optical coherence tomography (OCT)
Telemedicine equipment
Telemedicine infrastructure (internet)
Generator
Surgical standard clean running water
Autoclave (steam steriliser)
Steriliser (other)
Page 19 of 26
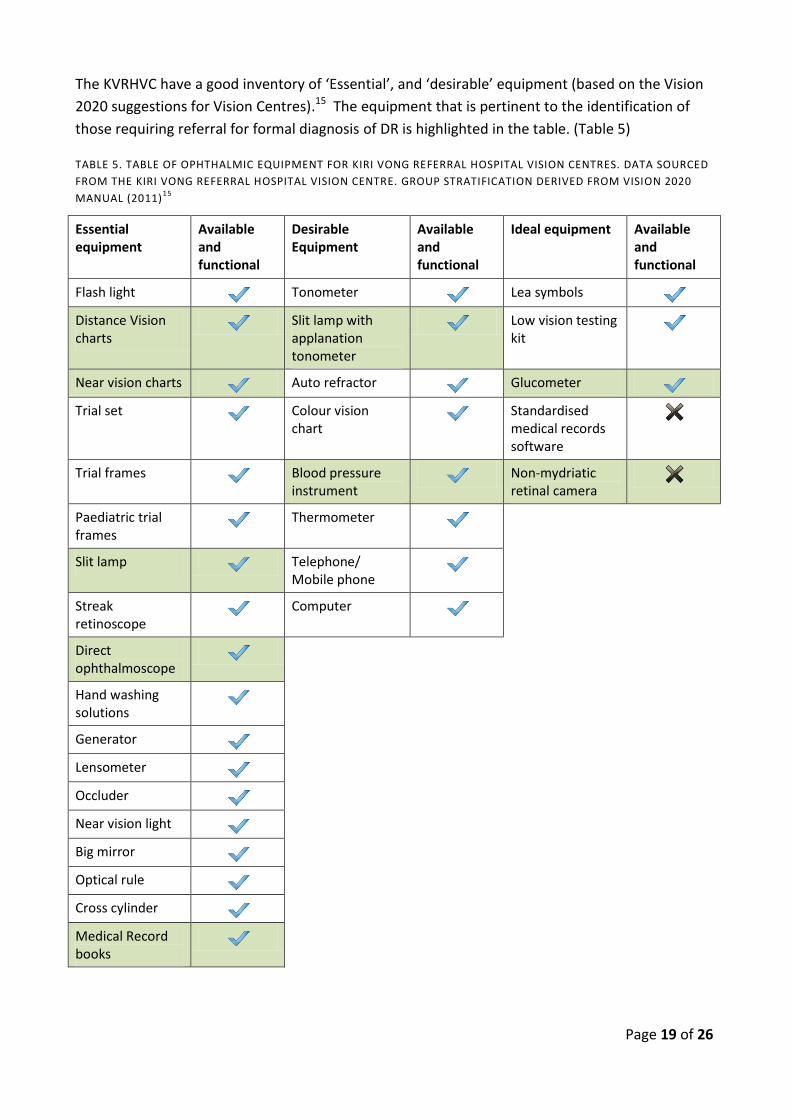
The KVRHVC have a good inventory of ‘Essential’, and ‘desirable’ equipment (based on the Vision
2020 suggestions for Vision Centres).15 The equipment that is pertinent to the identification of
those requiring referral for formal diagnosis of DR is highlighted in the table. (Table 5)
TABLE 5. TABLE OF OPHTHALMIC EQUIPMENT FOR KIRI VONG REFERRAL HOSPITAL VISION CENTRES. DATA SOURCED
FROM THE KIRI VONG REFERRAL HOSPITAL VISION CENTRE. GROUP STRATIFICATION DERIVED FROM VISION 2020
MANUAL (2011)15
Essential equipment
Available and functional
Desirable Equipment
Available and functional
Ideal equipment Available and functional
Flash light Tonometer Lea symbols
Distance Vision charts
Slit lamp with applanation tonometer
Low vision testing kit
Near vision charts Auto refractor Glucometer
Trial set Colour vision chart
Standardised medical records software
Trial frames Blood pressure instrument
Non-mydriatic retinal camera
Paediatric trial frames
Thermometer
Slit lamp Telephone/ Mobile phone
Streak retinoscope
Computer
Direct ophthalmoscope
Hand washing solutions
Generator
Lensometer
Occluder
Near vision light
Big mirror
Optical rule
Cross cylinder
Medical Record books
Page 20 of 26
HEALTH INFORMATION SYSTEMS AND MANAGEMENT
Health records of patients attending the CTEH are hand-written and then entered into a computer
database. The basic parameters that are routinely documented in the clinical notes for a patient
with diabetes are demographics (age, gender, address), type of diabetes, presence of
hypertension and hyperlipidaemia, presence and severity of retinopathy, current treatment
regimen for diabetes, previous treatment of DR (laser, vitreoretinal surgery), and the
management plan. For patients referred to the CTEH from Mo Po Tsyo, clinical parameters
including duration of diabetes, presence and severity of DR, additional health co-morbidities and
follow-up schedule are entered as a separate entity in the computer database. For ongoing follow
up patients are provided with a card which states the date of their next appointment.
The KVRHVC uses a similar combination to the CTEH of hand-written and computerised database
methods for recording patient details. For all patients, standard recorded information includes:
demographics (name, address, age, gender, socio-economic status, presence of self-reported
disability), relevant brief general medical history, relevant family history, probable diagnosis,
visual acuity, and a management plan. However, when clinical notes are entered into the
database, there is omission of ophthalmic-relevant patient co-morbidities (such as diabetes). The
referral system from KVRHVC to CTEH typically involves a referral note or letter. However, the
KVRHVC does not receive notification if the patient has attended their appointment unless they
are referred back from CTEH for follow-up. The KVRHVC does not have a system to enable
accurate recording from periodic assessments of the same patient. In this context, it is
foreseeable that the introduction of the non-mydriatic camera will be beneficial for diagnostic
accuracy, teaching, and to facilitate monitoring the quality of services and follow-up for patients
with diabetes.
HEALTH FINANCING AND SUSTAINABILITY
There were limited data regarding out-of-pocket expenditure for patients with diabetes attending
outpatient department at the CTEH for management of DR. The cost recovery strategy at the
CTEH has set the platform for its expansion of services. The hospital estimates that approximately
30% of costs for retinal examinations are paid for by patients and 70% from NGO funding.
According to the CTEH Annual Report in 2011, the hospital has three private rooms designated for
full-fee paying patients. The optical workshop based at the CTEH estimates 49% of spectacles
dispensed are paid the full price (ranging from US$2 to $6).16 Furthermore, according to the
memorandum of understanding between Mo Po Tsyo and CTEH, patients referred from Mo Po
Tsyo to CTEH are required to pay a registration fee of 4,000 Riel (US$1), which includes the fee for
the first consultation. The fee for follow-up consultations is 2,000 Riel (US$0.5). For patients
referred from Mo Po Tsyo, transport costs are incurred by the CTEH, and any laser treatment for
DR is provided free of charge.
Page 21 of 26
In the case at the KVRHVC, records specific to the out-of-pocket expenditure for patients with
diabetes were not available. Previously, the KVRHVC had an ‘Equity fund’ for patients from lower
socioeconomic backgrounds with limited resources to obtain their spectacles. This funding now
comes from the Government. The KVRHVC also accepts a nominal user fee from patients who can
afford a certain percentage but not the full cost of their care. The KVRHVC has generated cost
recovery from the sale of glasses. This has made a positive contribution to the income of the Kiri
Vong Referral Hospital. It currently supports the cost of salaries and provides a sustainable supply
of glasses. Within the region is it stated that approximately 30% of the population is below the
poverty line. There are some patients who cannot afford the total cost of eye care and glasses.
Some patients have been subsidised by the hospital.
GOVERNANCE AND LEADERSHIP
The CTEH and the KVRHVC are the only providers of public eye care services in the Takeo
Province. The sustained performance of the CTEH and the KVRHVC can largely be attributed to the
strength of governance and stakeholder (Government and Non-Government Organisation)
contributions. Both these facilities have established themselves as trusted points of eye care
within the public health system. In addition to community outreach screening, the CTEH and
KVRHVC have engaged with local stakeholders (general hospitals, CDMD, health centres) to
conduct eye health promotion as an important component of the holistic approach to healthcare,
and to facilitate early referral of people with vision impairment.
In the context of DR, progression to blindness can almost always be prevented through early
detection of diabetes and timely referral for eye examination. Opportunistic referral of patients
with diabetes for eye examination occurs from KVRHVC and Mo Po Tsyo to the CTEH. However, at
present, the presence and use of clinical practice guidelines for screening and treatment of DR do
not exist in Cambodia. There is no process of routine referral of patients with diabetes who
attend other medical facilities.
Emphasis must also be placed upon data collection and reporting of diabetes and its
complications. This may be enhanced by the presence of guidelines for health management
information systems across all levels of health care. Accurate collection and reporting of data
pertaining to diabetes and DR will also enable essential key performance indicators to be
monitored for future planning of service delivery.17 (Table 6)
TABLE 6 KEY PERFORMANCE INDICATORS AT A NATIONAL LEVEL RELEVANT TO DIABETIC RETINOPATHY. SOURCED
FROM THE GLOBAL INDICATORS TO MONITOR ELIMINATION OF AVOIDABLE BLINDNESS REPORT, 2012.18
Prevalence of blindness and vision impairment due to diabetic retinopathy
Coverage of screening services: Percentage of patients with diabetes that undergo eye examination
Coverage of treatment services: Percentage of patients with diabetes that are treated with retinal laser

Page 22 of 26
KEY OUTCOMES
Health Services
The CTEH is the only facility in the Takeo Province with the capacity to examine and provide laser
treatment of patients with diabetes for diabetic retinopathy. People with diabetes access multiple
sources of health care including health centres, general hospitals, community vision screening,
and private medical practitioners. However, currently there is a paucity of information on the
quality of services provided for patients with diabetes due to health information management
systems.
Health Workforce and Training
Currently there is no capacity for posterior segment examination at the secondary (district
hospital) level. This could possibly be achieved with non-mydriatic retinal imaging and training
vision centre workers to use the technology.
Health Management Information Systems
Currently there is no accurate record of the number of people with diabetes who are presenting
to health care facilities or the proportion who are being referred for eye examination at the CTEH.
The CTEH health information system does record pertinent clinical information related to the eye
examination for the patient with diabetes. However, the data entered at the KVRHVC is non-
specific, thus not providing specific information on all important causes of vision impairment that
is required to estimate the need, monitor key performance indicators, and plan service
development. Additionally, there is no established procedure for recording of follow-up
management of patients.
Referral Pathways
Patients with diabetes can be referred for eye examinations from the KVRHVC, community
outreach screening and the local NGO, Mo Po Tsyo to the CTEH. However, there is no referral of
patients with diabetes from general hospitals, and currently it is estimated that only a small
proportion patients are referred from KVRHVC or community outreach. Most patients with
diabetes present to the CTEH as “walk-ins”. Although it is at early stages, the collaboration
between CTEH and Mo Po Tsyo has demonstrated that such a partnership can be a successful
approach to conduct a DR screening program in Cambodia.
The large proportion of “walk-in” patients attending the KVRHVC and community outreach
presents the opportunity at these sites of primary care to increase community awareness of
diabetes, identify patients at risk of DR, and facilitate early referral for eye examination.
Page 23 of 26
Sustainability
The sustainability of the CTEH and KVRHVC has been demonstrated through their successful
integration into the public health care system. Both facilities have used sales of spectacles and
nominal fees for cost-recovery. At the CTEH, approximately 30% of retinal examination fees are
out-of-pocket for the patient. The KVRHVC continues to receive technical advice as required from
the CTEH.
Governance
There are no current national guidelines for diabetic retinopathy in Cambodia. There is no routine
referral system for eye examination amongst patients with diabetes.
Page 24 of 26
APPENDIX
APPENDIX A: RECORD OF AN EYE EXAMINATION OF A PATIENT WITH DIABETES REFERRED
FROM MO PO TSYO TO THE KIEN KHLEAN NATIONAL REHABILITATION CENTRE
OPHTHALMOLOGY SERVICE. SOURCED FROM MO PO TSYO (NOVEMBER, 2012)
Page 25 of 26
REFERENCES
1. WHO. Diabetes fact sheet. 2011; http://www.who.int/mediacentre/factsheets/fs312/en/index.html. Accessed 13/12/2011, 2011.
2. Ruamviboonsuk P, Wongcumchang N, Surawongsin P, Panyawatananukul E, Tiensuwan M. Screening for diabetic retinopathy in rural area using single-field, digital fundus images. J Med Assoc Thai. Feb 2005;88(2):176-180.
3. Yau JW, Rogers SL, Kawasaki R, et al. Global Prevalence and Major Risk Factors of Diabetic Retinopathy. Diabetes Care. Mar 2012;35(3):556-564.
4. Photocoagulation treatment of proliferative diabetic retinopathy. Clinical application of Diabetic Retinopathy Study (DRS) findings, DRS Report Number 8. The Diabetic Retinopathy Study Research Group. Ophthalmology. Jul 1981;88(7):583-600.
5. Early photocoagulation for diabetic retinopathy. ETDRS report number 9. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology. May 1991;98(5 Suppl):766-785.
6. Mohamed Q, Gillies MC, Wong TY. Management of diabetic retinopathy: a systematic review. JAMA. Aug 22 2007;298(8):902-916.
7. Friedman DS, Ali F, Kourgialis N. Diabetic retinopathy in the developing world: how to approach identifying and treating underserved populations. Am J Ophthalmol. Feb 2011;151(2):192-194 e191.
8. Global Health Observatory Data Repository: Blood glucose. In: WHO, ed. Geneva2012.
9. King H, Keuky L, Seng S, Khun T, Roglic G, Pinget M. Diabetes and associated disorders in Cambodia: two epidemiological surveys. Lancet. Nov 5 2005;366(9497):1633-1639.
10. WHO. Diabetes facts. 2010; http://www.who.int/diabetes/facts/world_figures/en/. Accessed 16/12/2012.
11. The World Bank Group: Total population of Cambodia. . 2012; http://data.worldbank.org/indicator/SP.POP.TOTL?cid=GPD_1. Accessed 20/12/2012.
12. Morchen M, Ang C, Mao N, Van Pelt M. Outcome of screening for diabetic retinopathy in collaboration with community based peer educators in Takeo province, Cambodia. Asia Pacific Ophthalmology Association (APAO), 2012. Busan, Korea.2012.
13. NPEH. Annual report of the National Committee for Prevention of Blindness, Cambodia. Phnom Penh2011.
14. Chakrabarti R, Harper C, Keeffe J. Diabetic retinopathy management guidelines. Expert Review of Ophthalmology. 2012;7(5):417-439.
15. Vision2020. Vision Centre Manual. New Delhi, India: VISION2020: The right to sight India;2011.
16. Annual Report: Caritas Takeo Eye Hospital 2011. http://www.caritascambodia.org/teh/tehdocs/annualreport/Annual%20Report%202011.pdf. Takeo: Caritas Cambodia;2011.

Page 26 of 26
17. WHO. Global initiative for the elimination of avoidable blindness. Action Plan 2006-2011. Geneva: WHO;2007.
18. CERA. Global Indicators to Monitor Elimination of Avoidable Blindness. Melbourne: Centre for Eye Research Australia;2012.