sickle cell disease sickle cell disease updates sickle... · complications of sickle cell disease...
TRANSCRIPT
Pediatrics Grand Rounds 26 March 2010
University of Texas Health Science Center at San Antonio
1
SICKLE CELL DISEASESICKLE CELL DISEASEUPDATESUPDATES
Reginald Moore M.DReginald Moore M.DAssociate ProfessorAssociate Professor
Pediatric Hematology OncologyPediatric Hematology OncologyUTHSCSAUTHSCSA
Sickle Cell DiseaseSickle Cell Disease
IntroductionIntroductionHistorical ReviewHistorical ReviewOverview of Sickle Cell DiseaseOverview of Sickle Cell DiseaseClinical PresentationClinical PresentationDisease PathogenesisDisease PathogenesisComplications of Sickle Cell DiseaseComplications of Sickle Cell DiseaseTreatment Options and UpdatesTreatment Options and Updates
IntroductionIntroductionMany advances in both basic science and Many advances in both basic science and treatment have come about in sickle cell disease treatment have come about in sickle cell disease over the last 20 years.over the last 20 years.We recognize sickle cell disease as a group of We recognize sickle cell disease as a group of complex genetic disorders leading to potentially complex genetic disorders leading to potentially life threatening multilife threatening multi--organ damage. organ damage. Understanding the genetics and pathogenesis of Understanding the genetics and pathogenesis of the disease has lead to many treatment the disease has lead to many treatment approaches and decreased both morbidity and approaches and decreased both morbidity and mortality.mortality.
Historical ReviewHistorical Review
Sickle cell disease was known long before Sickle cell disease was known long before the medical profession recognized it in the medical profession recognized it in 1904 ( red cells of a sick dental student 1904 ( red cells of a sick dental student from Grenada).from Grenada).James Herrick described red cell as James Herrick described red cell as ““sickledsickled shapedshaped”” in 1910in 19101927: Hahn and Gillespie correlated 1927: Hahn and Gillespie correlated sicklingsickling with low oxygenwith low oxygen
Historical ReviewHistorical Review
1940: Deoxygenated cell altered 1940: Deoxygenated cell altered hemoglobin structure (Sherman)hemoglobin structure (Sherman)1948: Janet Watson noted few sickle cell 1948: Janet Watson noted few sickle cell in newborns/ fetal hemoglobinin newborns/ fetal hemoglobin1948: Pauling and 1948: Pauling and ItanoItano noted sickle noted sickle hemoglobin was different and SCD was hemoglobin was different and SCD was first disorder related to a protein first disorder related to a protein abnormalityabnormality
Historical ReviewHistorical Review
1956: Ingram and Hunt sequenced 1956: Ingram and Hunt sequenced HbgHbg S S ((glutamicglutamic acid to acid to valinevaline) and thus predict ) and thus predict SCD (first genetic disorder whose SCD (first genetic disorder whose molecular basis was known)molecular basis was known)1984: BMT cured the disease1984: BMT cured the disease1995: 1995: HydroxyureaHydroxyurea proven to prevent proven to prevent complications complications The Human GenomeThe Human Genome
Pediatrics Grand Rounds 26 March 2010
University of Texas Health Science Center at San Antonio
2
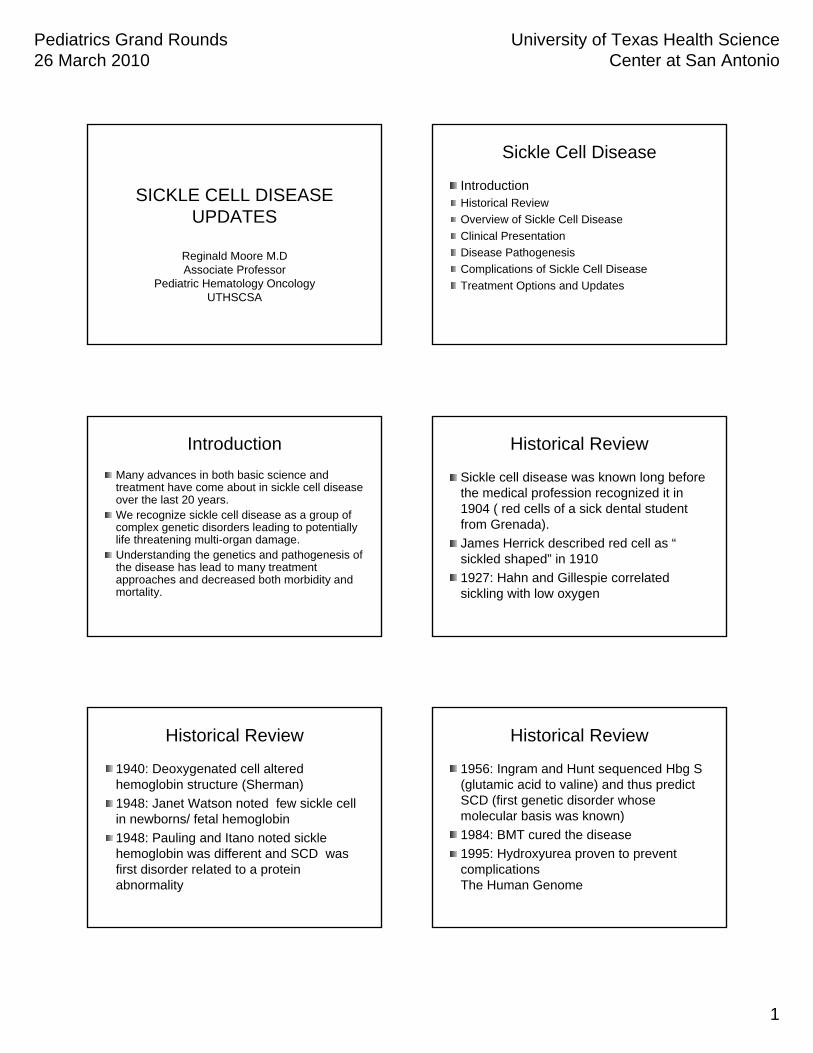
Normal Vs. Sickle Red CellsNormal Vs. Sickle Red CellsNormalNormal
DiscDisc--ShapedShapedDeformableDeformableLife span of 120 daysLife span of 120 days
SickleSickleSickleSickle--ShapedShapedRigid Rigid Lives for 20 days or Lives for 20 days or lessless
What Is Sickle Cell Disease?What Is Sickle Cell Disease?
An inherited disease of red blood cellsAn inherited disease of red blood cellsAffects hemoglobinAffects hemoglobinPolymerization of hemoglobin leads to a Polymerization of hemoglobin leads to a cascade of effects decreasing blood flowcascade of effects decreasing blood flowTissue hypoxia causes acute and chronic Tissue hypoxia causes acute and chronic damagedamage
Overview of Sickle Cell DiseaseOverview of Sickle Cell Disease
SCD due to hemoglobin SS presenting SCD due to hemoglobin SS presenting with hemolytic anemia and with hemolytic anemia and vasovaso--occlusion.occlusion.Affects 1 in 500 African AmericansAffects 1 in 500 African AmericansHispanic (Caribbean, Hispanic (Caribbean, C.AmericaC.America and S. and S. America) have 1 in 2000America) have 1 in 20008 % of African American with trait8 % of African American with traitEndemic malariaEndemic malariaFound worldwideFound worldwide
Pediatrics Grand Rounds 26 March 2010
University of Texas Health Science Center at San Antonio
3
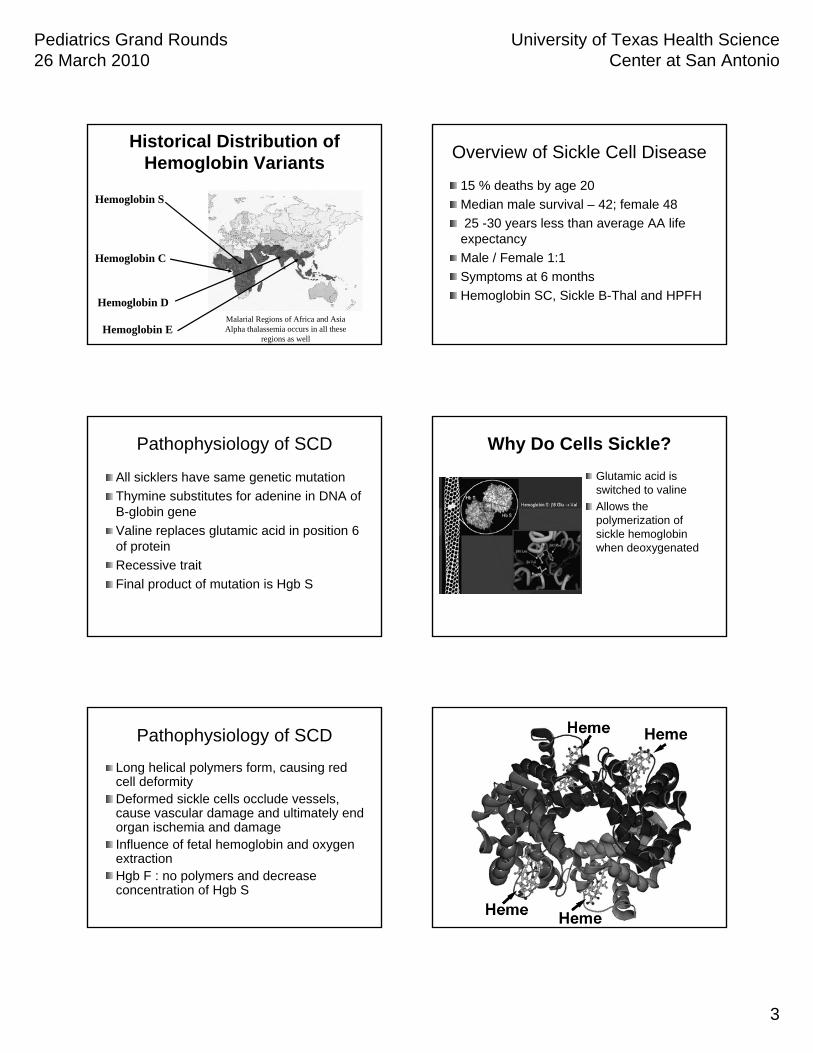
Historical Distribution of Historical Distribution of Hemoglobin VariantsHemoglobin Variants
Hemoglobin SHemoglobin S
Hemoglobin CHemoglobin C
Hemoglobin EHemoglobin E
Hemoglobin DHemoglobin DMalarial Regions of Africa and AsiaAlpha thalassemia occurs in all these
regions as well
Overview of Sickle Cell DiseaseOverview of Sickle Cell Disease
15 % deaths by age 2015 % deaths by age 20Median male survival Median male survival –– 42; female 4842; female 4825 25 --30 years less than average AA life 30 years less than average AA life
expectancyexpectancyMale / Female 1:1Male / Female 1:1Symptoms at 6 monthsSymptoms at 6 monthsHemoglobin SC, Sickle BHemoglobin SC, Sickle B--ThalThal and HPFHand HPFH
Pathophysiology of SCDPathophysiology of SCD
All All sicklerssicklers have same genetic mutationhave same genetic mutationThymine substitutes for adenine in DNA of Thymine substitutes for adenine in DNA of BB--globinglobin genegeneValineValine replaces replaces glutamicglutamic acid in position 6 acid in position 6 of proteinof proteinRecessive traitRecessive traitFinal product of mutation is Final product of mutation is HgbHgb SS
Why Do Cells Sickle?Why Do Cells Sickle?GlutamicGlutamic acid is acid is switched to switched to valinevalineAllows the Allows the polymerization of polymerization of sickle hemoglobin sickle hemoglobin when deoxygenatedwhen deoxygenated
Pathophysiology of SCDPathophysiology of SCD
Long helical polymers form, causing red Long helical polymers form, causing red cell deformitycell deformityDeformed sickle cells occlude vessels, Deformed sickle cells occlude vessels, cause vascular damage and ultimately end cause vascular damage and ultimately end organ ischemia and damageorgan ischemia and damageInfluence of fetal hemoglobin and oxygen Influence of fetal hemoglobin and oxygen extractionextractionHgbHgb F : no polymers and decrease F : no polymers and decrease concentration of concentration of HgbHgb SS
Pediatrics Grand Rounds 26 March 2010
University of Texas Health Science Center at San Antonio
4
HemolysisHemolysis and and VasoVaso--occlusion occlusion
VasoVaso--occlusion:occlusion:Occurs when the rigid sickle Occurs when the rigid sickle shaped cells fail to move shaped cells fail to move through the small blood through the small blood vessels, blocking local blood vessels, blocking local blood flow to a microscopic region of flow to a microscopic region of tissue. Amplified many times, tissue. Amplified many times, these episodes produce tissue these episodes produce tissue hypoxia. The result is pain, and hypoxia. The result is pain, and often damage to organs.often damage to organs.
HemolysisHemolysis::The anemia in SCD is caused The anemia in SCD is caused by red cell destruction, or by red cell destruction, or hemolysishemolysis, and, and the degree of the degree of anemia varies widely between anemia varies widely between patients. The production of patients. The production of red cells by the bone marrow red cells by the bone marrow increases dramatically, but is increases dramatically, but is unable to keep pace with the unable to keep pace with the destruction.destruction.
Complications of Sickle Cell Complications of Sickle Cell DiseaseDisease
Anemia associated with Anemia associated with hemolysishemolysis, , splenicsplenicsequestration and sequestration and aplasticaplastic crisiscrisisInfections with encapsulated organisms Infections with encapsulated organisms (10(10--30% mortality)30% mortality)Acute Chest Syndrome ( fluids and Acute Chest Syndrome ( fluids and sedation)sedation)VasoVaso--occlusive /Pain crises / occlusive /Pain crises / dactylitisdactylitisStrokes in 11% of Strokes in 11% of sicklerssicklers, TIA and silent , TIA and silent infarctsinfarcts
Clinical PresentationClinical Presentation
Fever / infectionFever / infectionChest painChest painFatigue and anemiaFatigue and anemiaHeadaches / weakness / sensation Headaches / weakness / sensation changeschangesPriapismPriapismAbdominal and bone pain / muscle achesAbdominal and bone pain / muscle aches
Fever and InfectionFever and InfectionFever > 38.5Fever > 38.5°° C (101C (101°°F) F) is an is an EMERGENCYEMERGENCYBasic laboratory Basic laboratory evaluation:evaluation:–– CBC with differential and CBC with differential and
reticulocytereticulocyte count, blood, count, blood, urine, and throat cultures, urine, and throat cultures, urinalysis, chest xurinalysis, chest x--rayray
ParenteralParenteral broadbroad--spectrum spectrum antibiotic (e.g. antibiotic (e.g. ceftriaxoneceftriaxone) ) IMMEDIATELYIMMEDIATELY after blood after blood draw and before other draw and before other procedures such as chest procedures such as chest xx--rayrayObserve after antibiotics Observe after antibiotics with repeat vital signswith repeat vital signs
Indications for hospitalization Indications for hospitalization & continued IV antibiotics:& continued IV antibiotics:Child appears illChild appears illAge < 1 yearAge < 1 yearAny temperature > 40Any temperature > 40°°CCLaboratory values:Laboratory values:
WBC >30,000/WBC >30,000/µµLL or < or < 5,000/5,000/µµLL
Platelet <100,000/Platelet <100,000/µµLLHbHb < 5g/dL< 5g/dL
Other complications such Other complications such as as splenicsplenic sequestration sequestration or acute chest syndromeor acute chest syndrome
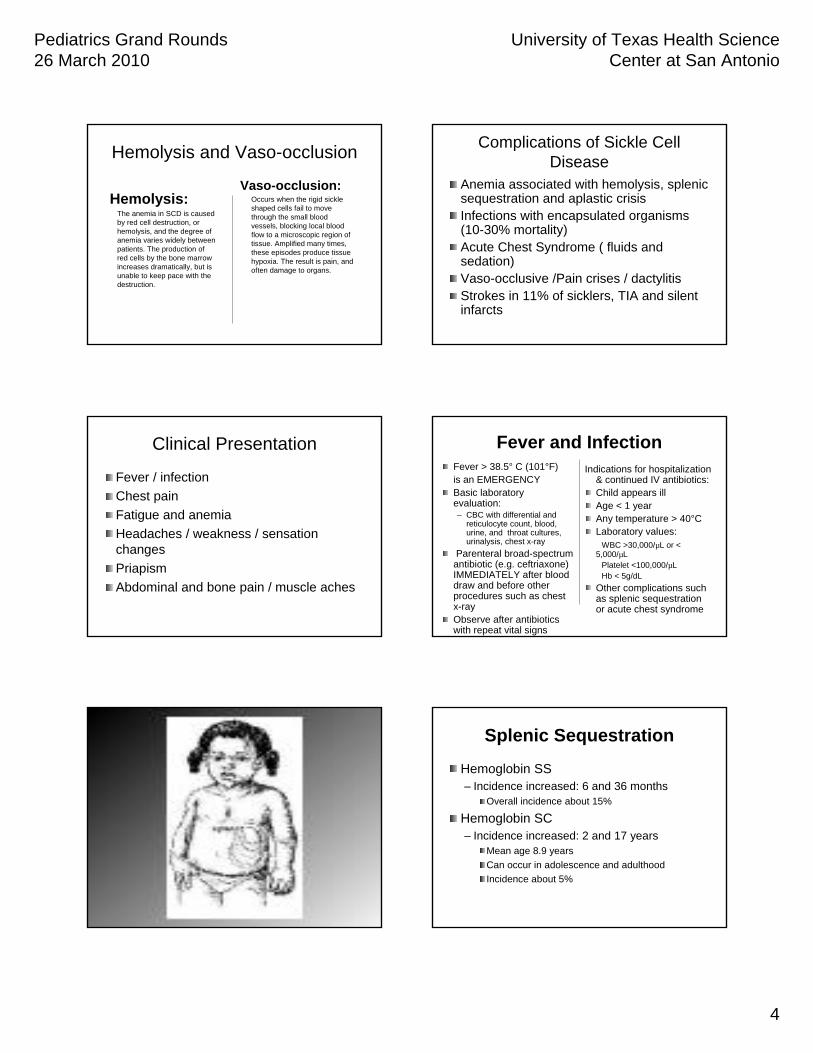
SplenicSplenic SequestrationSequestration
Hemoglobin SSHemoglobin SS–– Incidence increased: 6 and 36 monthsIncidence increased: 6 and 36 months
Overall incidence about 15% Overall incidence about 15%
Hemoglobin SCHemoglobin SC–– Incidence increased: 2 and 17 yearsIncidence increased: 2 and 17 years
Mean age 8.9 yearsMean age 8.9 yearsCan occur in adolescence and adulthoodCan occur in adolescence and adulthoodIncidence about 5%Incidence about 5%
Pediatrics Grand Rounds 26 March 2010
University of Texas Health Science Center at San Antonio
5
SplenicSplenic SequestrationSequestration
Sudden trapping of blood Sudden trapping of blood within the spleenwithin the spleenUsually occurs in infants Usually occurs in infants under 2 years of age with SSunder 2 years of age with SSSpleen enlarged on physical Spleen enlarged on physical exam, may not be exam, may not be associated with fever, pain, associated with fever, pain, or other symptomsor other symptomsHemoglobin more than 2 Hemoglobin more than 2 g/dLg/dL below baseline, often below baseline, often with relative with relative thrombocytopeniathrombocytopeniaSevere sequestration crisis Severe sequestration crisis can be fatal within a few can be fatal within a few hours.hours. •Recurrence very common (50%)
•Associated with high mortality (20%)
Treatments For Treatments For SplenicSplenicSequestionSequestion
Intravenous fluidsIntravenous fluids–– Maintain vascular volume Maintain vascular volume
Cautious blood Cautious blood transfusiontransfusion–– Treat anemia, sequestered Treat anemia, sequestered
blood can be released from blood can be released from spleen spleen
Spleen removal or Spleen removal or splenectomysplenectomy–– If indicatedIf indicated
Health MaintenanceHealth MaintenanceSpecial studiesSpecial studies
BrainBrain-- TranscranialTranscranial dopplerdoppler ultrasonographyultrasonography, , MRI/MRAMRI/MRALungsLungs-- Pulmonary function tests, Echo Pulmonary function tests, Echo cardiogram for pulmonary hypertensioncardiogram for pulmonary hypertensionNeurologicNeurologic-- neuropsychological testingneuropsychological testing
Pulmonary complications in SCDPulmonary complications in SCD
Primary pathologic processes are Primary pathologic processes are infection, bone marrow infarction, fat infection, bone marrow infarction, fat emboli as well as rib and emboli as well as rib and sternalsternal infarcts infarcts and pulmonary edemaand pulmonary edemaACS most common pulmonary problemACS most common pulmonary problem
Acute Chest SyndromeAcute Chest Syndrome
Clinically:Clinically:Acute onset of fever, respiratory symptoms, new infiltrate on chAcute onset of fever, respiratory symptoms, new infiltrate on chest xest x--rayray
CausesCauses-- InfectionInfection-- Fat emboliFat emboli-- Lung infarctLung infarct
TreatmentTreatment-- HospitalizeHospitalize-- Antibiotics Antibiotics
(broad spectrum plus (broad spectrum plus macrolidemacrolide))-- OxygenOxygen-- AnalgesicsAnalgesics-- BronchodilatorsBronchodilators-- Simple or exchange transfusionSimple or exchange transfusion
A leading cause of death in sickle cell diseasePulmonary hypertensionPulmonary hypertension
Retrospective studies estimate prevalence of pulmonary Retrospective studies estimate prevalence of pulmonary hypertension in SCD patients to be 20hypertension in SCD patients to be 20--40 %40 %HemolysisHemolysis, chronic anemia and transfusion were , chronic anemia and transfusion were predictivepredictiveProspective study: elevated TR jet velocity> 2.5 m/sec Prospective study: elevated TR jet velocity> 2.5 m/sec on ECHO in 30% of 62 children > 6 years with on ECHO in 30% of 62 children > 6 years with HgbHgb SS SS and SBTand SBTRisk factors: increase Risk factors: increase reticulocytereticulocyte count, count, low O2 saturation and high plateletslow O2 saturation and high plateletsRight heart Right heart catherizationcatherization is now required for definitive is now required for definitive diagnosis of pulmonary hypertensiondiagnosis of pulmonary hypertension
Pediatrics Grand Rounds 26 March 2010
University of Texas Health Science Center at San Antonio
6
Pulmonary hypertensionPulmonary hypertensionDefinitive diagnosis require right heart cath, but Definitive diagnosis require right heart cath, but plasma level of brain plasma level of brain natriureticnatriuretic peptide (BNP) peptide (BNP) and sixand six--minute walk test may help identify minute walk test may help identify BNP> 160pg/ml was sensitive, specific and had BNP> 160pg/ml was sensitive, specific and had positive predictive value in positive predictive value in ddetectingddetecting pulmonary pulmonary hypertensionhypertensionSupportive care with transfusions to maintain Supportive care with transfusions to maintain HgbHgb S < 20 % and Oxygen therapyS < 20 % and Oxygen therapyClinical trial with Clinical trial with prostacyclinprostacyclin and agents to and agents to reduce PA pressure are neededreduce PA pressure are neededSildenafilSildenafil stopped in July due to increased sickle stopped in July due to increased sickle cell crisiscell crisis
Pulmonary complicationsPulmonary complicationsRecurrent vascular and lung Recurrent vascular and lung parenchymalparenchymal insult insult are greatest risk for sickle cell chronic lung are greatest risk for sickle cell chronic lung diseasediseaseSCCLD develop as early as age 20,lung SCCLD develop as early as age 20,lung dysfunction can be rapid and death within 7 dysfunction can be rapid and death within 7 yearsyearsStart with chest pain and mild reductions in FVC Start with chest pain and mild reductions in FVC and TLC, progress to diffuse interstitial fibrosis and TLC, progress to diffuse interstitial fibrosis and poor O2 saturation, finally to prolonged and poor O2 saturation, finally to prolonged chest pain, severe pulmonary fibrosis, chest pain, severe pulmonary fibrosis, hypoxemia at rest and elevated pulmonary hypoxemia at rest and elevated pulmonary artery pressure at restartery pressure at rest
Pulmonary HypertensionPulmonary HypertensionHydroxyureaHydroxyurea to reduce red cell to reduce red cell hemolysishemolysis may may be of benefit.be of benefit.10 children with elevated TRV on echo treated 10 children with elevated TRV on echo treated with HU decreased TRV, improved hemoglobin with HU decreased TRV, improved hemoglobin concentration and O2 saturationconcentration and O2 saturationSurvival decreased in children and adults with Survival decreased in children and adults with SCD and pulmonary hypertension, SCD and pulmonary hypertension, each10mmHg rise in each10mmHg rise in mPaPmPaP associated with1.7associated with1.7--fold increase in mortality, median survival 26 fold increase in mortality, median survival 26 monthsmonths
Obstructive Sleep ApneaObstructive Sleep Apnea
Upper airway obstruction during sleep due Upper airway obstruction during sleep due to adenoid and to adenoid and tonsillartonsillar enlargementenlargement1/3 of SCD patients/ snoring1/3 of SCD patients/ snoringHypoxemia on sleep studies and improve Hypoxemia on sleep studies and improve with T & Awith T & ACompliance poor with CPAPCompliance poor with CPAP
Pediatrics Grand Rounds 26 March 2010
University of Texas Health Science Center at San Antonio
7
Pain ManagementPain Management
Morphine Sulfate now being used in higher Morphine Sulfate now being used in higher dosing IV, IT and as a dosing IV, IT and as a nebulizednebulized agentagentToradolToradolDilaudidDilaudidFentanylFentanyl patchpatchNonNon--pharmacologic adjunctive therapypharmacologic adjunctive therapy
Chronic PainChronic Pain
Pain lasting >3 to 6 monthsPain lasting >3 to 6 monthsPatients should receive comprehensive Patients should receive comprehensive psychologicpsychologic and clinical assessmentand clinical assessmentTreatmentTreatment–– AnalgesicsAnalgesics–– HydroxyureaHydroxyurea–– TENS unitsTENS units–– Relaxation techniquesRelaxation techniques–– Physical and occupational therapyPhysical and occupational therapy
Bone Disease Diagnosis and Bone Disease Diagnosis and TreatmentTreatment
AvascularAvascular necrosis of hips and shouldersnecrosis of hips and shoulders–– Index of suspicion Index of suspicion
Persistent hip or shoulder painPersistent hip or shoulder painPlain film or MRIPlain film or MRI
TreatmentTreatment–– ConservativeConservative
NSAIDNSAID’’ss and 6 weeks of rest off affected limband 6 weeks of rest off affected limbPhysical therapyPhysical therapy
Screening AVNScreening AVNAvascularAvascular Necrosis Necrosis –– Hip FilmsHip Films–– Hip MRIHip MRI–– Grading of AVNGrading of AVN
Grade I: MRIGrade I: MRIGrade II: Film/MRIGrade II: Film/MRIGrade III: FilmGrade III: FilmGrade IV: FilmGrade IV: FilmGrade V: FilmGrade V: Film
–– No grade for AVN of the shoulderNo grade for AVN of the shoulder
Pediatrics Grand Rounds 26 March 2010
University of Texas Health Science Center at San Antonio
8
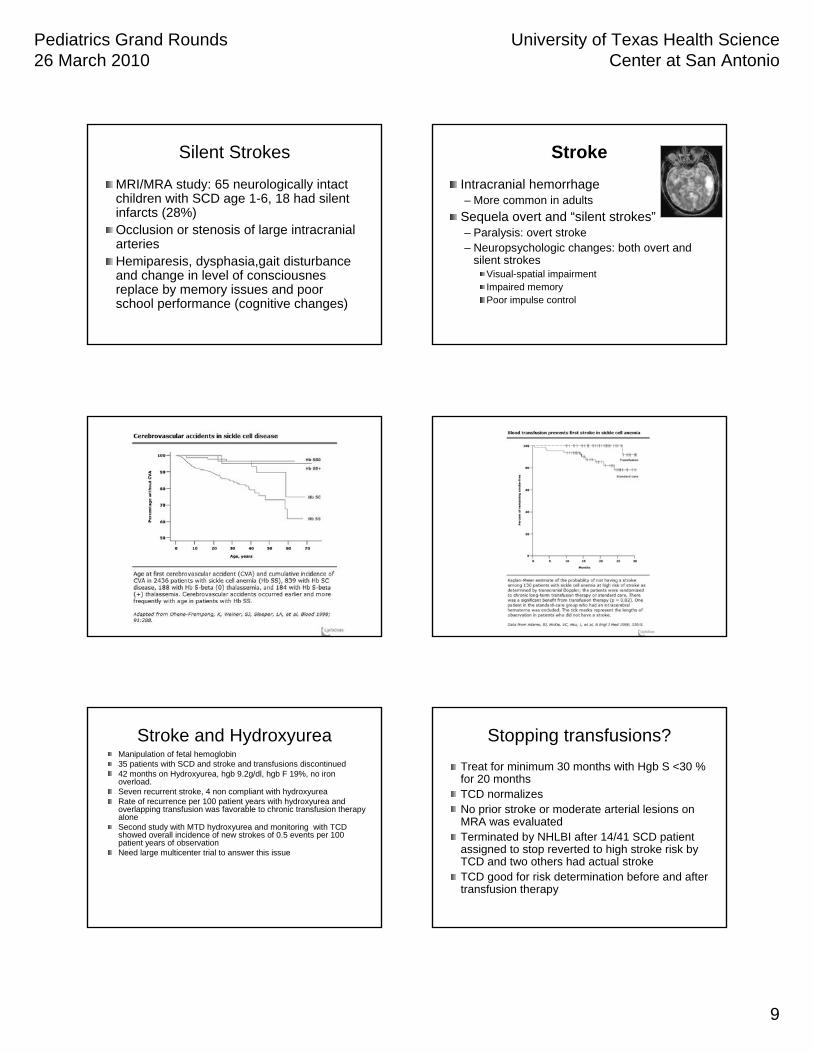
StrokesStrokes
Leading cause of death in children and Leading cause of death in children and adultsadults0.6 to 0.76 per 100 patient years during 0.6 to 0.76 per 100 patient years during first 20 years of life, mostly first 20 years of life, mostly HgbHgb SSSS300 times higher than children without 300 times higher than children without SCDSCDIschemic strokes in children 2Ischemic strokes in children 2--9 years old9 years old
StrokeStroke
Historically 8 to 10% of Historically 8 to 10% of children with SSchildren with SS
““Silent StrokeSilent Stroke”” in 22% of in 22% of children with hemoglobin children with hemoglobin SSSS
Any acute neurologic symptom other than mild headache, even if transient, requires urgent evaluation.
Treatment: Chronic transfusion therapy to maintain sickle hemoglobin at or below 30%
StrokesStrokes
Risk factors include prior Risk factors include prior TIATIA’’ss, low steady , low steady state Hemoglobin, ACS (recent or state Hemoglobin, ACS (recent or recurrent), elevated systolic BPrecurrent), elevated systolic BPTCD: time averaged mean velocity in large TCD: time averaged mean velocity in large intracranial vesselsintracranial vessels> 170cm/sec worrisome> 170cm/sec worrisome>200 cm/sec high risk even before MRA >200 cm/sec high risk even before MRA lesions notedlesions noted
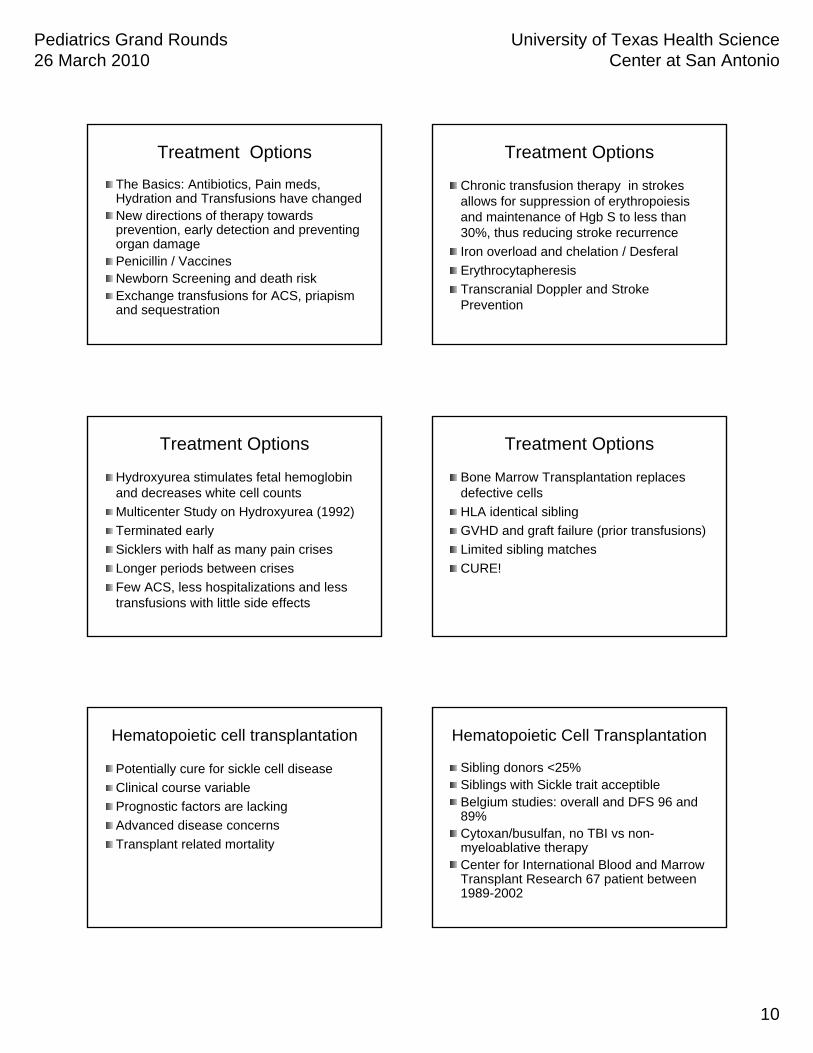
STOP 1 TrialSTOP 1 Trial
130 children ,all > 200cm/sec on at least 130 children ,all > 200cm/sec on at least two studiestwo studiesObservation vs prophylactic transfusion (< Observation vs prophylactic transfusion (< 30 % 30 % HgbHgb S)S)Early termination with 1 to 10 infarction Early termination with 1 to 10 infarction rate in transfusion grouprate in transfusion groupAlso reduced risk of silent strokesAlso reduced risk of silent strokesTCD between age 2TCD between age 2--4 is effective for 4 is effective for screening stroke risk (AA Neurology)screening stroke risk (AA Neurology)
Pediatrics Grand Rounds 26 March 2010
University of Texas Health Science Center at San Antonio
9
Silent StrokesSilent Strokes
MRI/MRA study: 65 neurologically intact MRI/MRA study: 65 neurologically intact children with SCD age 1children with SCD age 1--6, 18 had silent 6, 18 had silent infarcts (28%)infarcts (28%)Occlusion or Occlusion or stenosisstenosis of large intracranial of large intracranial arteriesarteriesHemiparesisHemiparesis, , dysphasia,gaitdysphasia,gait disturbance disturbance and change in level of and change in level of consciousnesconsciousnesreplace by memory issues and poor replace by memory issues and poor school performance (cognitive changes) school performance (cognitive changes)
StrokeStrokeIntracranial hemorrhageIntracranial hemorrhage–– More common in adultsMore common in adults
SequelaSequela overt and overt and ““silent strokessilent strokes””–– Paralysis: overt strokeParalysis: overt stroke–– NeuropsychologicNeuropsychologic changes: both overt and changes: both overt and
silent strokes silent strokes VisualVisual--spatial impairmentspatial impairmentImpaired memoryImpaired memoryPoor impulse controlPoor impulse control
Stroke and Stroke and HydroxyureaHydroxyureaManipulation of fetal hemoglobinManipulation of fetal hemoglobin35 patients with SCD and stroke and transfusions discontinued35 patients with SCD and stroke and transfusions discontinued42 months on 42 months on HydroxyureaHydroxyurea, , hgbhgb 9.2g/dl, 9.2g/dl, hgbhgb F 19%, no iron F 19%, no iron overload.overload.Seven recurrent stroke, 4 non compliant with Seven recurrent stroke, 4 non compliant with hydroxyureahydroxyureaRate of recurrence per 100 patient years with Rate of recurrence per 100 patient years with hydroxyureahydroxyurea and and overlapping transfusion was favorable to chronic transfusion theoverlapping transfusion was favorable to chronic transfusion therapy rapy alonealoneSecond study with MTD Second study with MTD hydroxyureahydroxyurea and monitoring with TCD and monitoring with TCD showed overall incidence of new strokes of 0.5 events per 100 showed overall incidence of new strokes of 0.5 events per 100 patient years of observationpatient years of observationNeed large multicenter trial to answer this issueNeed large multicenter trial to answer this issue
Stopping transfusions?Stopping transfusions?Treat for minimum 30 months with Treat for minimum 30 months with HgbHgb S <30 % S <30 % for 20 monthsfor 20 monthsTCD normalizesTCD normalizesNo prior stroke or moderate arterial lesions on No prior stroke or moderate arterial lesions on MRA was evaluatedMRA was evaluatedTerminated by NHLBI after 14/41 SCD patient Terminated by NHLBI after 14/41 SCD patient assigned to stop reverted to high stroke risk by assigned to stop reverted to high stroke risk by TCD and two others had actual strokeTCD and two others had actual strokeTCD good for risk determination before and after TCD good for risk determination before and after transfusion therapytransfusion therapy
Pediatrics Grand Rounds 26 March 2010
University of Texas Health Science Center at San Antonio
10
Treatment OptionsTreatment Options
The Basics: Antibiotics, Pain meds, The Basics: Antibiotics, Pain meds, Hydration and Transfusions have changedHydration and Transfusions have changedNew directions of therapy towards New directions of therapy towards prevention, early detection and preventing prevention, early detection and preventing organ damage organ damage Penicillin / VaccinesPenicillin / VaccinesNewborn Screening and death riskNewborn Screening and death riskExchange transfusions for ACS, Exchange transfusions for ACS, priapismpriapismand sequestrationand sequestration
Treatment OptionsTreatment Options
Chronic transfusion therapy in strokes Chronic transfusion therapy in strokes allows for suppression of allows for suppression of erythropoiesiserythropoiesisand maintenance of and maintenance of HgbHgb S to less than S to less than 30%, thus reducing stroke recurrence30%, thus reducing stroke recurrenceIron overload and Iron overload and chelationchelation / / DesferalDesferalErythrocytapheresisErythrocytapheresisTranscranialTranscranial Doppler and Stroke Doppler and Stroke PreventionPrevention
Treatment OptionsTreatment Options
HydroxyureaHydroxyurea stimulates fetal hemoglobin stimulates fetal hemoglobin and decreases white cell countsand decreases white cell countsMulticenter Study on Multicenter Study on HydroxyureaHydroxyurea (1992)(1992)Terminated earlyTerminated earlySicklersSicklers with half as many pain criseswith half as many pain crisesLonger periods between crisesLonger periods between crisesFew ACS, less hospitalizations and less Few ACS, less hospitalizations and less transfusions with little side effectstransfusions with little side effects
Treatment OptionsTreatment Options
Bone Marrow Transplantation replaces Bone Marrow Transplantation replaces defective cellsdefective cellsHLA identical siblingHLA identical siblingGVHD and graft failure (prior transfusions)GVHD and graft failure (prior transfusions)Limited sibling matchesLimited sibling matchesCURE!CURE!
Hematopoietic cell transplantationHematopoietic cell transplantation
Potentially cure for sickle cell diseasePotentially cure for sickle cell diseaseClinical course variableClinical course variablePrognostic factors are lackingPrognostic factors are lackingAdvanced disease concernsAdvanced disease concernsTransplant related mortalityTransplant related mortality
Hematopoietic Cell TransplantationHematopoietic Cell Transplantation
Sibling donors <25%Sibling donors <25%Siblings with Sickle trait Siblings with Sickle trait acceptibleacceptibleBelgium studies: overall and DFS 96 and Belgium studies: overall and DFS 96 and 89%89%Cytoxan/busulfanCytoxan/busulfan, no TBI vs non, no TBI vs non--myeloablativemyeloablative therapytherapyCenter for International Blood and Marrow Center for International Blood and Marrow Transplant Research 67 patient between Transplant Research 67 patient between 19891989--20022002
Pediatrics Grand Rounds 26 March 2010
University of Texas Health Science Center at San Antonio
11
Hematopoietic Cell Hematopoietic Cell TranplantationTranplantation
Average age 10 years(2Average age 10 years(2--27) stable or 27) stable or improved MRI of brainimproved MRI of brainLinear growth improvedLinear growth improved3 of 26 developed GVHD3 of 26 developed GVHD81 % bone marrow was source for stem 81 % bone marrow was source for stem cellscellsFive year Overall and DFS were 97% and Five year Overall and DFS were 97% and 85%85%Only 9 patients (13 %) recurrence of SCD Only 9 patients (13 %) recurrence of SCD
Hematopoietic Cell TransplantationHematopoietic Cell Transplantation
Early Transplants better overall survival Early Transplants better overall survival and DFS and DFS Lower rates of death, engraftment Lower rates of death, engraftment failure,mixedfailure,mixed chimerismchimerism and relapse (7/36)and relapse (7/36)Goal of alternative donors, non Goal of alternative donors, non --myeloblativemyeloblative conditioning and umbilical conditioning and umbilical cord offer potential improvementcord offer potential improvement
Treatment OptionsTreatment Options
New and perhaps experimental New and perhaps experimental approaches are many.approaches are many.Erythropoietin (EPO) stimulates red cell Erythropoietin (EPO) stimulates red cell production and fetal hemoglobin synthesis production and fetal hemoglobin synthesis (Livingston,1994) delivered via adenovirus (Livingston,1994) delivered via adenovirus vector.vector.ArginineArginine butyrate stimulate fetal butyrate stimulate fetal hemoglobin, side effects, IV and short halfhemoglobin, side effects, IV and short half--lifelife
Treatment OptionsTreatment Options
Gene TherapyGene TherapyProof exist that it is possible to correct Proof exist that it is possible to correct genetic defects in the blood by correcting genetic defects in the blood by correcting damaged RNAdamaged RNACorrecting RNA will allow for the removal Correcting RNA will allow for the removal of the sickle defect from patients born with of the sickle defect from patients born with the diseasethe diseaseHow this can be accomplished is still very How this can be accomplished is still very much experimentalmuch experimental
Adolescents and Transition of Adolescents and Transition of CareCare
Young adults (>20 years) with frequent pain Young adults (>20 years) with frequent pain crises at greatest risk for early deathcrises at greatest risk for early deathBarriers to care for young adultsBarriers to care for young adults–– Lack of adult SCD providersLack of adult SCD providers–– Loss of medical coverage Loss of medical coverage –– Developmental (level of independence, denial of Developmental (level of independence, denial of
chronic illness)chronic illness)–– Ineffective coping skills (passive versus active)Ineffective coping skills (passive versus active)
Adolescents and Transition of Adolescents and Transition of CareCare
Develop explicit plan for transitionDevelop explicit plan for transition
Team approachTeam approach-- pediatric and adult providers, pediatric and adult providers, social work, school/vocational staff, support social work, school/vocational staff, support groupsgroups
Plan gradual transition (start 1 year before)Plan gradual transition (start 1 year before)
Continue communication between pediatric & Continue communication between pediatric & adult providers after transitionadult providers after transition

Pediatrics Grand Rounds 26 March 2010
University of Texas Health Science Center at San Antonio
12
ConclusionsConclusions
While our knowledge of the genetics of While our knowledge of the genetics of sickle cell disease is extensive, more is sickle cell disease is extensive, more is need to reach our goal of curing this need to reach our goal of curing this terrible disease.terrible disease.These are exciting times and the sky truly These are exciting times and the sky truly
is the limit!!!is the limit!!!